
Abstract
Background/Purpose
To compare outcomes of minimally invasive screw fixation (MIS) versus conservative management for fragility fractures of the pelvis (FFP).
Methods
Sixty-five patients aged 70–95 years with FFP Type II-IV were retrospectively reviewed (30 MIS, 35 conservative). Functional status was assessed via Modified Functional Ambulatory Categories (MFAC). Rehabilitation duration was defined as postoperative length of stay (LOS) for the MIS group and total LOS for the conservative group.
Results
The conservative group was older (P = 0.007), while MIS had more complex fractures (P = 0.0254). Despite a 15.1-day surgical delay in MIS, rehabilitation duration was comparable (26.1 vs 27.6 days; P = 0.76). Mortality and MFAC decline showed no significant differences. No major complications occurred in the MIS group. Upon discharge, 78.6% (MIS) and 71.0% (conservative) of home-dwellers returned home.
Conclusion
MIS is a safe and effective option for unstable FFP. It achieved functional outcomes and rehabilitation efficiency comparable to conservative management despite higher fracture complexity and operative delays.
Keywords
Introduction
Geriatric pelvic fractures, or fragility fractures of the pelvis (FFP), present an escalating public health challenge due to osteoporosis.1,2 Unlike high-energy fractures, FFP often involve lower instability as ligamentous structures remain intact. While immediate haemodynamic instability is uncommon, continued monitoring for progressive bleeding is essential. Diminished physiological reserves render these seemingly minor injuries in elderly patients prone to marked functional decline and elevated mortality (one-year mortality rates of 8–27%) due to prolonged immobilization, highlighting the compounded effects of frailty, comorbidities, and injury severity.3–8
Common classifications designed for high-energy pelvic fracture patterns in younger adults are not applicable to FFP. The classification by Rommens and Hofmann (Table 1) in 2013 is now widely adopted, 9 providing a framework for clinical decision-making.
Rommens and Hofmann classification of fragility fracture of the pelvis (FFP).
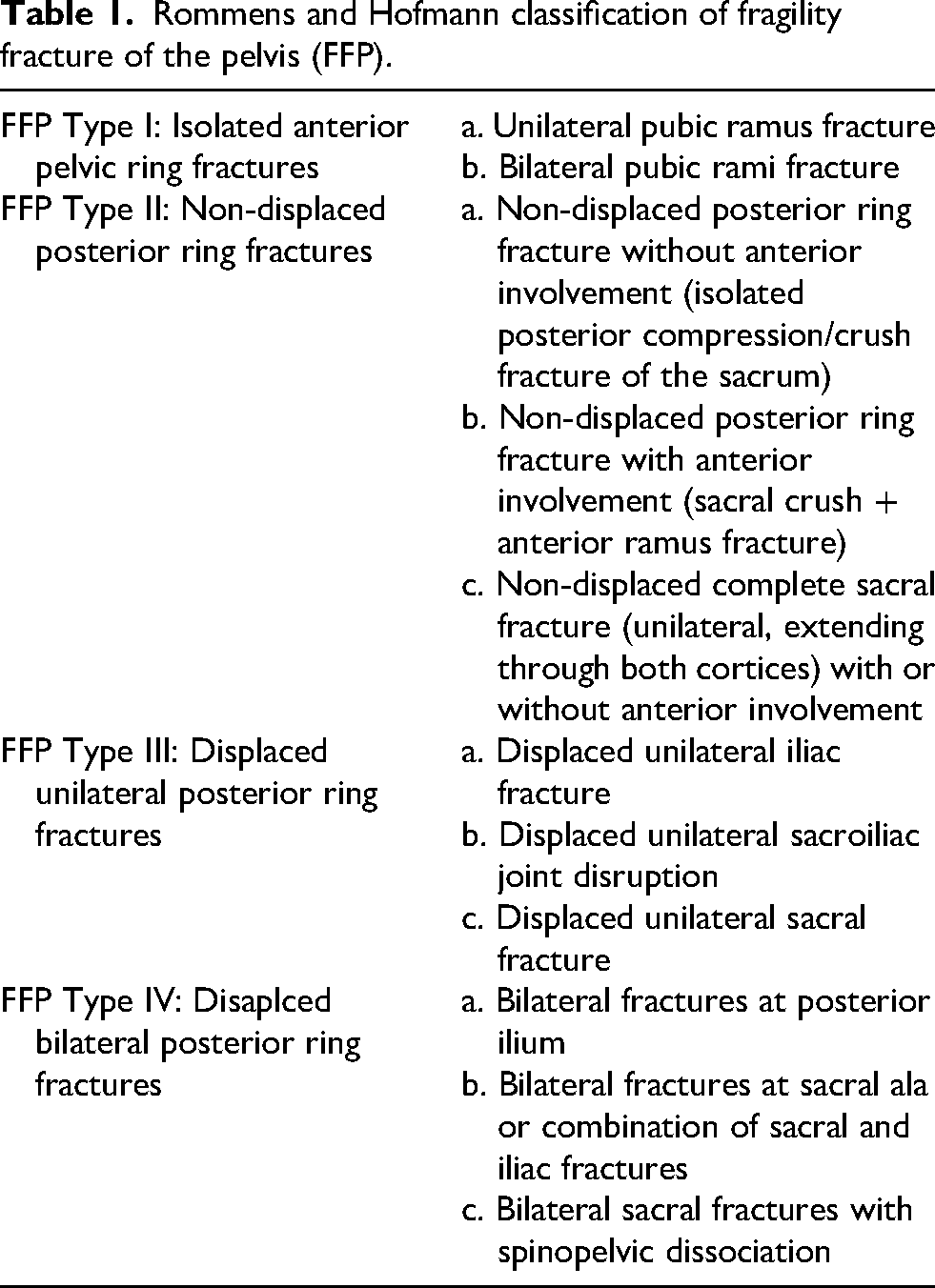
While Type I fractures are typically managed conservatively, consensus is lacking for Type II fractures. Traditionally, Type III-IV fractures require open reduction and internal fixation, which is associated with high complication rates in geriatric populations.4,9,10
This has led to a shift toward minimally invasive techniques aimed at restoring stability while minimizing physiological burden. Image-guided percutaneous minimally invasive screw fixation (MIS) offers a potential balance: mechanical stabilization with reduced soft-tissue trauma, shorter operative times, and earlier mobilization.11,12 Traditional 2D intraoperative imaging is limited in accurately assessing complex 3D pelvic anatomy. With advances in 3D imaging, integrating intraoperative 3D imaging with high-resolution preoperative CT and surgical navigation optimizes surgical planning and enhances screw placement precision.13–15 Despite these theoretical advantages, evidence directly comparing MIS with conservative care in elderly patients remains limited, particularly regarding short-term functional outcomes, early mobility, and healthcare resource utilization.
To address this gap, this retrospective cohort compared the outcomes of MIS and conservative management in geriatric unstable FFP. It was hypothesized that MIS would enable earlier mobilization and improved short-term functional recovery without increasing perioperative risk.
Methods
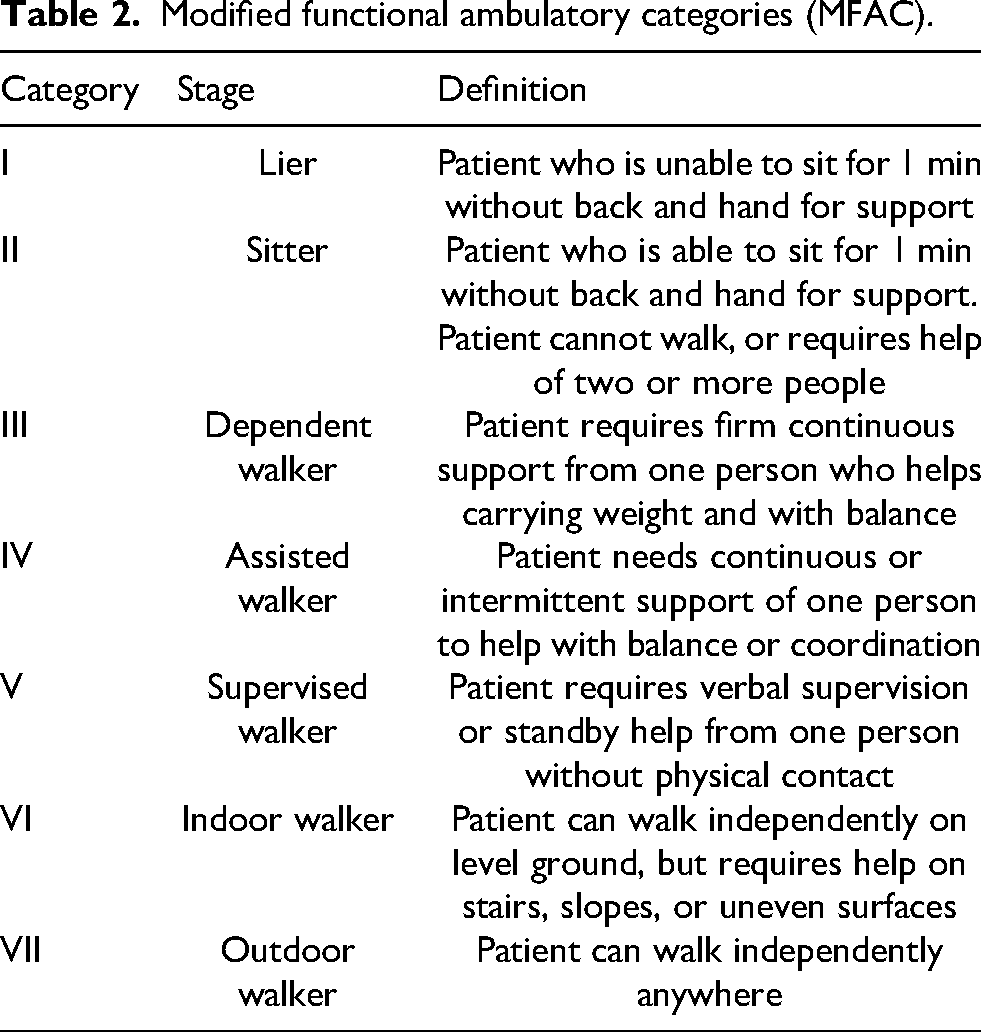
This retrospective study (January 2020–November 2023) was conducted at a regional acute tertiary general hospital in Hong Kong, serving a district of more than 600,000 population. Sixty-five patients aged 70–95 years with CT-confirmed FFP Type II-IV fractures, and a premorbid Modified Functional Ambulatory Category (MFAC) score ≥ IV was included (Table 2). The MFAC is a modification of the well-established Functional Ambulation Classification, which is a 6-point scale (0–5) with excellent reliability validated in stroke and hip fracture populations.16–18 The MFAC is a regionally validated instrument used in Hong Kong public hospital settings.19,20 This represented a patient group with sufficient injury severity and reasonable function within a suitable age range which could be offered both conservative and surgical options. Patients younger than 70 years have a substantially high propensity for operative treatment, while those older than 95 years rarely receive surgical intervention. Exclusion criteria included major cognitive impairment or psychiatric illness, major concomitant injuries (e.g. hip fracture, abdominal or thoracic trauma requiring intervention), or inpatient cerebrovascular accident. Of 65 eligible patients, 35 were managed conservatively, and 30 received MIS.
Modified functional ambulatory categories (MFAC).
Treatment protocols
Conservative management entailed 8–12 weeks of protected weight-bearing to a varying degree, analgesia and physiotherapy.
The MIS group underwent navigated screw fixation under general anaesthesia. Surgical planning was performed according to preoperative CT, which provided superior resolution compared to intraoperative 3D fluoroscopy. Depending on fracture patterns, screw tracts were positioned commonly across the sacroiliac joint (SI screw), long intramedullary corridors of anterior and posterior columns of the acetabulum (AC and PC screws), or along the ilium (LC screw), or in combination. Intraoperative 3D fluoroscopy images were merged with preoperative CT scans to verify the accuracy of the preoperative plan. In occasional cases where fracture alignment had changed since the preoperative CT scan, intraoperative 3D fluoroscopy was used for intra-operative planning. The surgical plan was executed by inserting guide pins under real-time navigation, followed by the placement of 6.5 or 5.0 mm cannulated screws. Postoperatively, patients were instructed to commence full weight-bearing mobilization, supplemented by analgesia and physiotherapy.
Both groups of patients were followed up for at least 1 year after discharge with serial X-rays. CT scan was used as an adjunct to assessment whenever necessary for better anatomical assessment.
Data collection
Data extracted from electronic medical records included age, premorbid mobility and residence, length of stay (LOS), mortality (during inpatient, at 6 and 12 months after discharge), post-injury mobility status (upon discharge, at 6 and 12 months after discharge) and post-injury residence (upon discharge, at 6 and 12 months after discharge). Mobility was assessed using the MFAC. 16 Only patients who had lived at home before injury were assessed for changes in residence after injury. Patients discharged to a temporary respite care facility before returning home would be classified as discharged to residential care home and home at later time points if they returned to their homes. Post-injury mobility and residence at any particular time point included only patients who survived up to that specific time.
MIS-specific variables included time from admission to surgery, postoperative LOS, operative time, blood loss, and operative complications.
Regarding resource utilization, total LOS was compared, acknowledging distinct care models: conservative care focused on immediate multidisciplinary rehabilitation, whereas the MIS group required preoperative and operative phases before rehabilitation commenced. To ensure a fair comparison of recovery efficiency, ‘inpatient rehabilitation duration’ was analyzed, defined as total LOS for the conservative group and postoperative LOS for the MIS group.
Recorded complications included venous thromboembolic events, anaemia requiring blood transfusion, wound infection, severe pneumonia, and severe urinary tract infection.
Statistical analysis
Continuous variables (e.g. age, LOS) were reported as means ± standard deviation and compared using Student's t-test. Paired t-test was used to assess longitudinal mobility changes within each group, while unpaired t-test compared mobility changes between groups. Fisher's exact test or the Chi-square test was used to compare categorical variables between groups as appropriate. A P-value <0.05 was considered statistically significant.
Results
Baseline characteristics
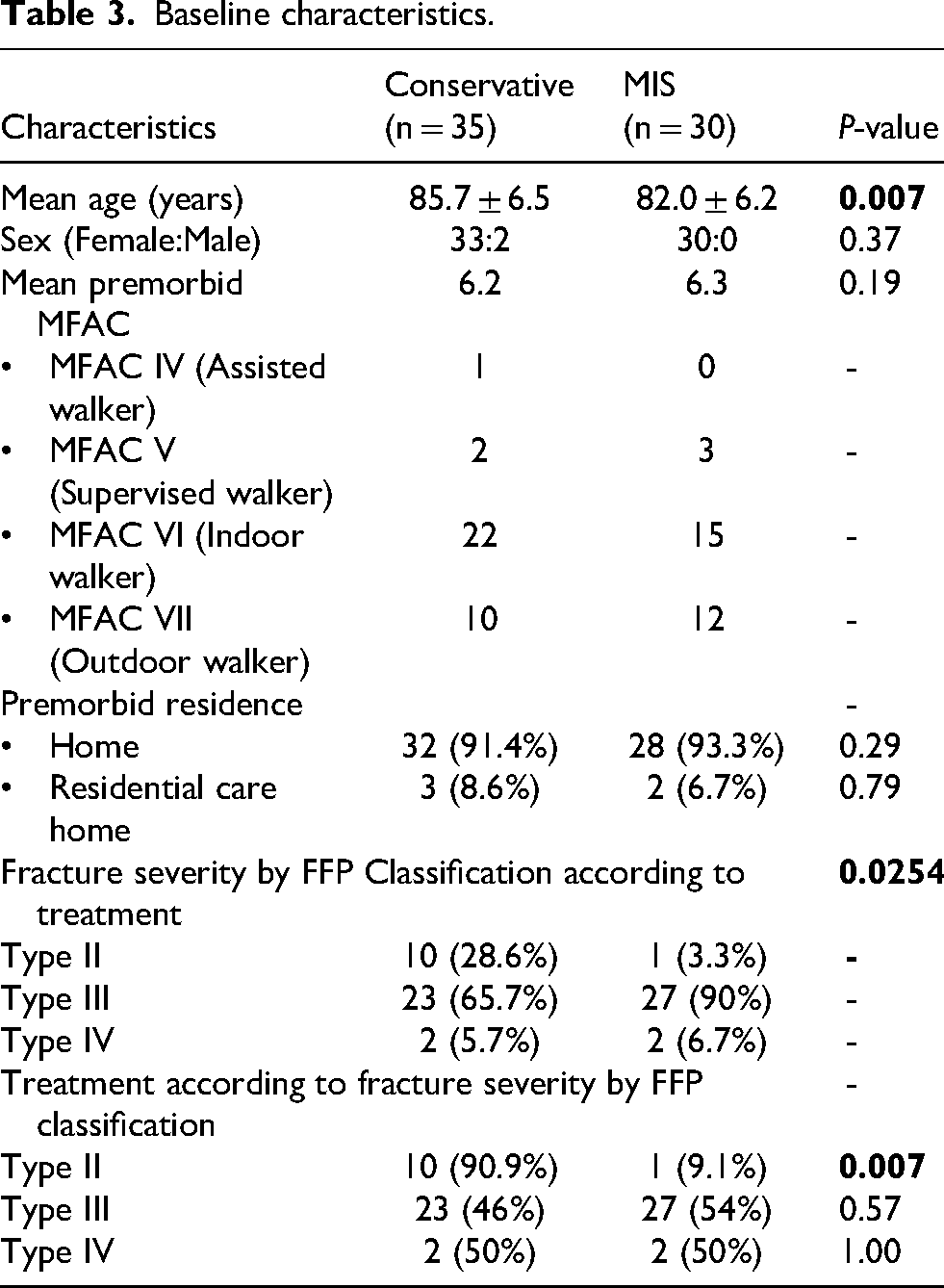
The conservative group (n = 35) was significantly older than the MIS group (n = 30) (85.7 vs 82.0 years, P = 0.007). There were no differences in gender distribution (P = 0.37), mean premorbid MFAC score (6.2 vs 6.3; P = 0.19), or premorbid residence (P = 0.29). Fracture patterns differed significantly between the two groups (P = 0.0254). While FFP Type II fractures were predominantly treated conservatively (90.9%), conservative management and MIS were more evenly distributed in Type III fractures (46% vs 56%) and Type IV (50% vs 50%), resulting in a lower proportion of FFP Type II (3.3%) and a higher proportion of FFP Type III fractures (90%) in the MIS group as compared to the conservative group (28.6% Type II, 65.7% Type III) (Table 3).
Baseline characteristics.
Length of stay and operative details
The mean total LOS was significantly longer in the MIS group compared to the conservative group (41.2 vs 27.6 days, P = 0.014). However, inpatient rehabilitation duration – defined as the postoperative LOS for the MIS group (26.1 days) and total LOS of the conservative group – showed no significant difference (P = 0.76). For the MIS group, the mean time to surgery was 15.1 days, with a mean operative time of 136.0 min, and a mean blood loss of 15.7 mL.
Mortality and complications
Mortality rates in the two groups were comparable with no statistically significant differences observed at any time point: inpatient, 6 months and 12 months post-discharge (conservative: 2.9%, 5.7% and 17.1%, respectively; MIS: 0%, 6.7% and 16.7%, respectively). Causes of death for the conservative group included urosepsis accounting for 1 inpatient death, pneumonia for 1 death that happened within 6 months after discharge, and pneumonia and cerebrovascular accidents which resulted in 4 deaths between 6 and 12 months after discharge. For the MIS group, pneumonia and hepatic encephalopathy accounted for 1 death each in 6 months after the patient was discharged home, while pneumonia and congestive heart failure caused 3 more between 6 and 12 months after discharge.
Functional outcomes and home-dwelling ability
Functional outcomes, measured by MFAC scores and longitudinal changes from premorbid status, were comparable across all intervals (Table 4). MFAC scores, an ordinal categorical scale, were summarized using mean scores to illustrate trends across four time points: premorbid, hospital discharge, and 6- and 12-months post-discharge. To minimize attrition bias in the longitudinal comparison, analysis of premorbid MFAC was restricted to survivors at each specific time point.
Clinical and functional outcomes.
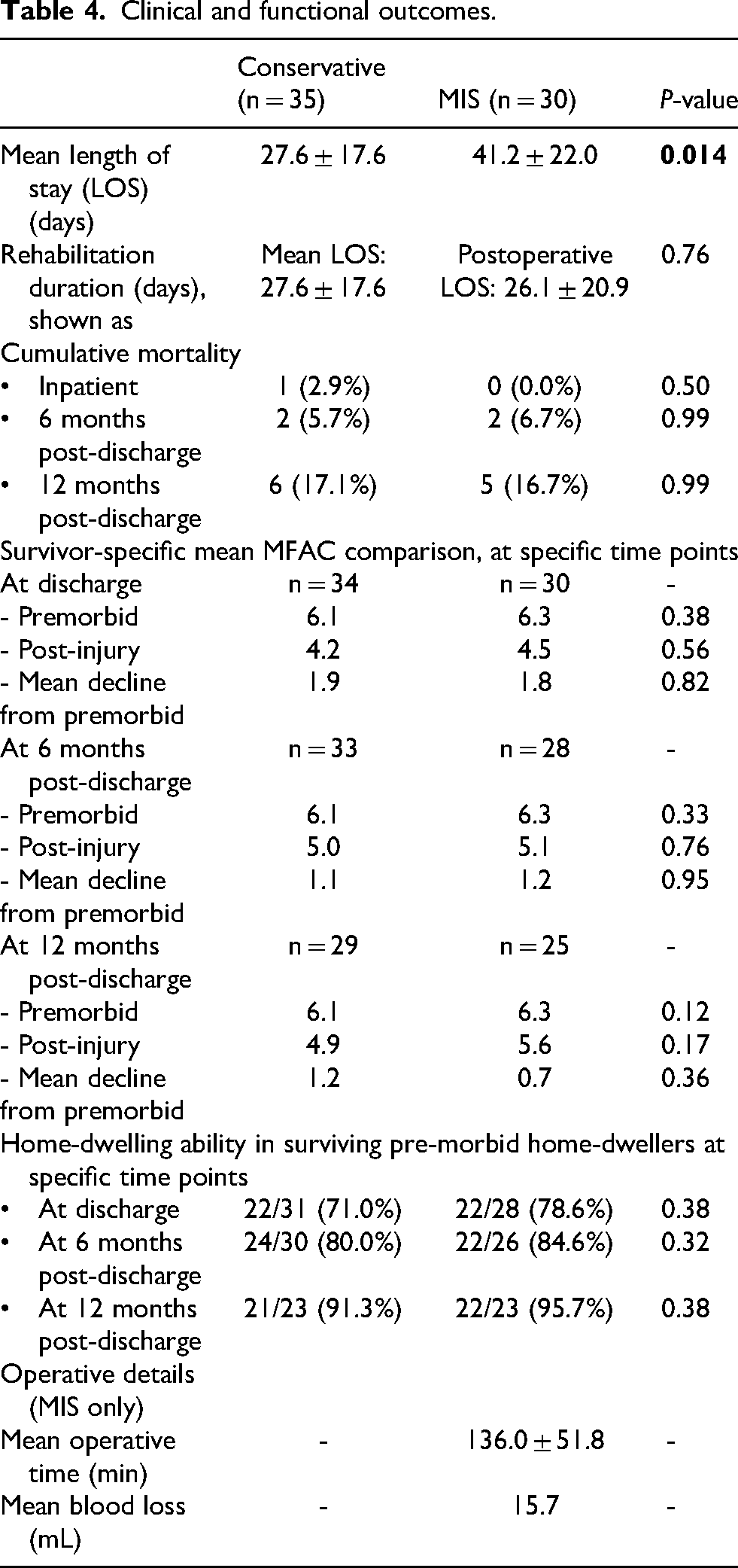
The two groups demonstrated comparable mean post-injury MFAC scores at discharge, 6 months, and 12 months post-discharge (4.2, 5.0 and 4.9 in the conservative group; 4.5, 5.1 and 5.6 in the MIS group). Functional decline from premorbid status was also comparable: changes at discharge, 6 months and 12 months post-discharge were 1.9, 1.1 and 1.2, respectively, in the conservative group, versus 1.8, 1.2 and 0.7, respectively, in the MIS group. Notably, two patients in the conservative group sustained hip fractures following falls within 12 months of discharge.
Among pre-morbid home-dwellers who survived hospitalization (n = 31 conservative; n = 28 MIS), the proportion of returning home upon discharge was 71.0% (22/31) in the conservative group versus 78.6% (22/28) in the MIS group. Four patients in the conservative group required temporary respite care before returning home. At 6 months post-discharge, 80.0% (24/30) of surviving pre-morbid home-dwellers in the conservative group remained at home compared to 84.6% (22/26) in the MIS group; at 12 months post-discharge, these rates were 91.3% (21/23) and 95.7% (22/23), respectively. No statistically significant differences were found regarding home-dwelling status at any measured time point.
MIS operative details included mean time to surgery of 15.1 ± 8.7 days, operative time of 136.0 ± 51.8 min, and mean blood loss of 15.7 mL.
No major intraoperative or postoperative complications (e.g. venous thromboembolic events, anaemia requiring transfusion or wound infections) occurred in the MIS group. Severe pneumonia and urinary tract infections contributing to mortality were captured in the available data, but information on pressure injuries was unavailable for analysis.
Discussion
Our study demonstrates that MIS is a viable and safe alternative to conservative management for unstable FFP. Notably, the MIS group comprised significantly more unstable fractures (90% Type III, 3.3% Type II vs 65.7% Type III, 28.6% Type II in the conservative group). Conversely, the conservative group was significantly older, likely carrying a higher comorbidity burden. While conservative treatment predominated in Type II fractures (90.9%) due to their relative stability, the relatively even distribution in Type III (46% conservative vs 54% MIS) and Type IV (50% vs 50%) was likely influenced by the age disparity; older patients often preferred conservative management despite having more unstable fracture patterns. Notwithstanding these baseline differences, MIS outcomes were comparable to conservative management, regarding mortality, rehabilitation duration and the rate of return home in premorbid home-dwellers.
Regarding the LOS, the MIS group experienced a longer total LOS, primarily driven by a protracted preoperative period. Unlike the conservative group, MIS patients required preoperative CT, anaesthetic assessments, medical optimization and surgical scheduling. Consequently, while patients in the conservative group began rehabilitation immediately, the MIS group experienced delayed mobilization, leading to a certain degree of deconditioning.
However, this delay in the MIS group did not translate into a longer rehabilitation period. The postoperative LOS for the MIS group (26.1 days) was comparable to the total LOS of the conservative group (27.6 days). This suggests that the mechanical stability provided by MIS may offset the ‘detrimental effects’ of delayed mobilization. We hypothesize that minimizing preoperative delays – similar to the protocols for hip fractures – could further shorten the rehabilitation process by mitigating early deconditioning.
The protective effect of MIS against deconditioning stems from its superior mechanical stability. Navigated MIS provides robust intraosseous fixation, reducing acute pain and enabling immediate postoperative full weight-bearing. Such stability is often unachievable with conservative treatment or traditional open plating, both of which require periods of protected weight-bearing, that are difficult for the frail elderly to maintain. Furthermore, minimal soft tissue trauma and blood loss associated with MIS minimize perioperative risks, as evidenced by our 0% inpatient mortality (2.9% in the conservative group) and absence of major complications in the MIS cohort.
The MFAC has been validated in patients with hip fracture, making it particularly relevant for assessing functional outcomes in elderly patients with fragility fractures. 19 Both groups showed comparable mean MFAC scores and functional declines at discharge, as well as at 6 months and 12 months. This reflects the high baseline morbidity and the profound long-term impact of geriatric FFP on physical function, regardless of the intervention chosen. 21 Given the significant delay in initiating mobilization within the MIS group, a more pronounced clinical advantage in mobility preservation may have been achieved had the operations been performed earlier. Furthermore, the occurrence of two subsequent hip fractures within one year in the conservative group – despite an earlier start of rehabilitation – suggests potentially less favourable independent mobility outcomes, although this remains partially attributable to the significantly more advanced age of the conservative cohort.
FFP has been recognized as a distinct clinical entity over the past decade with increasing international frequency. Unlike well-established management algorithms available for high-energy pelvic fractures in younger patients, clear-cut criteria for choosing between conservative and operative treatment in geriatric FFP do not yet exist. Management currently relies on a holistic assessment of various factors, including comorbidities, functional requirements and the mechanical instability of the fracture and its impact on early mobilization.5,22,23 Existing literature yields contradictory results regarding mortality, functional recovery, complications and indications for different management strategies (e.g. minimally invasive vs open surgery). It is important to note that many existing studies are retrospective with small sample sizes, and their designs are often subject to unavoidable selection bias.3,22,24–27 For instance, there is a general clinical tendency to favour conservative management for less severe fractures and operative treatment for more unstable patterns; a simple direct comparison of such groups would likely yield unfavourable results for operative treatment.
Additionally, many studies included different surgical techniques, such as open surgery, minimally invasive surgery, external fixation and cement augmentation, under a single ‘operative’ category.3,5,22,23 Larger prospective studies with more robust designs generally suggest that while conservative management (prioritizing early mobilization without weight-bearing limitations and optimal pain control) is appropriate for stable fractures, early MIS for unstable fracture patterns or intractable pain offers superior outcomes in terms of mortality and function. Surgical principles should be specifically adapted for geriatric patients: rather than aiming for anatomical reduction and rigid fixation required in younger populations, the goal should be acceptable functional reduction, stable minimally invasive fixation and immediate mobilization. Poor surgical outcomes are frequently associated with non-compliance with treatment algorithms and delayed operations.3,10,28
These points reinforce our findings that, despite significant operative delays and a high proportion of severe fracture patterns, the MIS group achieved outcomes – including rehabilitation duration, mobility preservation, community reintegration and mortality rates – that were at least comparable, if not slightly better than, those of the conservative group. With the emergence of higher-quality research, we anticipate that standardized clinical guidelines and treatment algorithms for FFP will be established in the near future, following the successful model of geriatric hip fractures.4,29
This study has several limitations that merit careful interpretation of the findings. The retrospective design is inherently susceptible to selection and information bias, as treatment allocation was based on clinical judgement regarding age, comorbidities and injury patterns rather than randomization. Although we excluded patients younger than 70 (who may be more inclined toward surgery) and those older than 95 (none of whom received surgery), age-related bias cannot be entirely eliminated. However, the influence of age may be partially balanced by disparities in fracture severity: while patients in the conservative group were significantly older, those in the MIS group presented with significantly more severe fracture patterns.
The relatively small sample size further limits the statistical power to detect subtle differences in clinical and functional endpoints. Furthermore, the single-centre design may constrain the generalizability of these findings to other healthcare settings with different logistical or rehabilitative resources. The absence of a standardized treatment algorithm led to significantly lengthened preoperative waiting time, which may have compromised outcomes in the operative group. Conversely, inconsistencies in rehabilitation protocols for the conservative group may have similarly affected their results. Regarding functional assessment, pain scores were not systematically recorded, and the use of MFAC alone may not fully capture the complexities of functional recovery. The quality of life in the elderly is multifaceted, encompassing physical mobility, activities of daily living, social roles, cognitive and emotional health, and the patient's self-perception of independence. These unmeasured factors collectively limit our ability to establish definitive causal relationships between treatment modality and outcome.
Nonetheless, this study represents one of the few investigations specifically addressing the role of MIS in elderly patients with unstable FFP. Given the increasing prevalence of such injuries in ageing populations, future multicentre, prospective studies employing standardized rehabilitation protocols, optimized surgical logistics and validated multimodal functional measures are warranted. Such research is essential to definitively evaluate the clinical efficacy and cost-effectiveness of minimally invasive fixation in this vulnerable patient population.
In summary, despite a significantly delayed start to mobilization due to preoperative waiting time, the MIS group demonstrated functional outcomes – including rehabilitation duration, the ability to return home and mortality rates – that were comparable to those of the conservative group. In contrast, the conservative group experienced higher mortality, and a greater incidence of complications, such as severe pneumonia, cerebrovascular accidents and subsequent hip fractures within one year of discharge. These findings suggest that MIS is a promising treatment option for appropriately selected older patients. Further prospective studies are required to confirm these findings and facilitate the establishment of clear treatment algorithms and clinical guidelines, ultimately improving outcomes for this increasingly common and debilitating fragility fracture in our ageing society.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.