
Abstract
Endometriosis is a chronic inflammatory condition that may cause pelvic pain, dysmenorrhea, and/or infertility in women of reproductive age. While treatments may include medical or surgical management, the majority of therapeutic options are non-curative, and women may experience longstanding pain and/or disability. In general, chronic diseases are believed to result from modifiable risk factors, including diet. In this review, we discuss recent data on evidence-based associations between diet and endometriosis and the mechanistic points of action of constituent dietary factors with emphasis on inflammatory events that may contribute to the promotion or inhibition of the disease. Understanding the convergence of diet and endometriosis may lead to the development of clinical strategies to improve the quality of life for symptomatic women.
Introduction
Endometriosis, a condition histologically characterized by the presence of viable endometrial glands and stroma in extrauterine locations such as in the peritoneum, ovary, and bowel, is a chronic disease that causes pelvic pain, dysmenorrhea, and/or infertility in up to 10% of women of reproductive age.1,2 Because the condition is latent at the very early stages and may remain undiagnosed for many years after onset of symptoms, it can significantly progress by the time of clinical diagnosis, with limited treatment options in advanced stages. 3 Surgical removal of lesions generally provides only temporary relief since the condition has a high incidence of recurrence. 3 In some cases, surgery may compromise ovarian function. 4 Moreover, a significant fraction of patients do not respond or develop resistance to hormonal treatments. 5 Thus, identifying preventative and alternative therapeutic strategies for management of endometriosis continues to be of high priority.
Chronic diseases have emerged as a considerable global health burden, in lieu of infectious diseases that have rapidly declined in the last 20 years. Risk factors for the majority of chronic diseases, including smoking, alcohol use, Western diet, and physical inactivity, are considered mostly preventable. 6 According to the Global Burden of Disease study, 7 diet is a leading risk factor for early death worldwide, second only to smoking. Indeed, approximately 60% of all cancer types may be attributed to metabolic syndrome and its accompanying components of obesity and Type 2 diabetes, which are due largely to over-nutrition. 8 In the United States, obesity has reached almost epidemic proportions with nearly 40% of adults and 19% of children categorized as metabolically compromised. Given the latter and the increasing incidence of obesity globally, it is reasonable to predict that in the absence of effective interventions, the incidence of chronic diseases will only escalate with accompanying personal and socioeconomic consequences. 9
In recent years, endometriosis has been increasingly linked to ovarian, endometrial, and breast cancers.10–12 A significant proportion of these steroid hormone-dependent cancers are tied to metabolic dysfunctions. A known trigger for metabolic syndrome is inflammation initiated by over-production and secretion of local- or systemic-acting pro-inflammatory cytokines. Given that women with endometriosis demonstrate a state of chronic inflammation, 13 treatments that reduce inflammation may mitigate the risk or severity of endometriosis. In this review, we discuss recent data on evidence-based associations between diet and endometriosis and the mechanistic points of action of constituent dietary factors that may contribute to promotion or inhibition of the disease.
Diet and endometriosis—the linkages
Population studies to date support an inverse association of endometriosis with body mass index (BMI). 14 Interestingly, endometriosis is associated with lean body size during childhood, adolescence, and adulthood. 15 This relationship between BMI and endometriosis appears counter-intuitive, but can be explained to some extent by the fact that obese women may suffer from anovulation, fewer menstrual cycles and hence, decreased menstrual tissue reflux, the latter being the most accepted etiology for endometriosis. 16 However, there are sporadic reports on a positive association between increasing BMI and advancing-stage endometriosis 17 and between prepubertal obesity and endometriosis recurrence risk. 18 Given these conflicting findings, the question on whether obesity results in endometriosis or whether the presence of endometriosis leads to obesity remains unresolved.
Metabolic dysfunction and obesity usually co-exist but disrupted metabolic status can also arise independent of body weight. Indeed, metabolic syndrome rather than BMI better predicts cardiovascular risk in women and inflammatory activity is more closely associated with metabolic status than body weight. 19 In a study of women with and without endometriosis, differing plasma metabolite profiles were associated with and predictive of disease occurrence. 20 A recent study addressed the causal relationship involving BMI, metabolic status, and endometriosis in a mouse model of the disease. 21 Mice with experimentally induced endometriosis were found to display lower body weights than sham controls after 21 weeks of ad libitum feeding, leading to the conclusion that endometriosis is causal to loss of body weight and body fat. The lower BMI consequent to endometriosis was attributed to disruption of hepatic liver metabolism, providing a mechanistic link to the poorly understood metabolic component of endometriosis. While these findings offer support for the negative correlation between BMI and endometriosis, they challenge the long-held view that lower BMI is a risk factor for endometriosis and a predictive factor for severe endometriosis. Further assessment of the systemic and local (lesion, peritoneal) inflammatory phenotypes in these mice will provide important insight on the link between metabolic perturbations and inflammation in women with endometriosis.
Our own study implicated a causal link between diet and endometriosis in an immune-competent mouse model of the disease. 22 We found that diets which differed only in fat content (high-fat diet, HFD: 45% fat kcal vs control diet, CD: 17% fat kcal) and provided ad libitum to recipient mice beginning at weaning (5 weeks prior to intraperitoneal lesion administration) and for an additional 4 weeks after endometrial tissue i.p. administration, elicited significant differences in lesion number (HFD > CD), lesion inflammatory and redox status (HFD > CD), and systemic/peritoneal fluid redox levels (HFD > CD). No differences in body weights and in serum levels of estrogen, progesterone, and insulin were noted between the two groups. These results indicate that diets promoting systemic inflammation and oxidative stress can enhance endometriosis progression. Furthermore, they lend support to the notion that adiposity is not a major contributor to endometriosis risk.
Table 1 summarizes recent studies (2000 to present) that have experimentally evaluated dietary effects on endometriosis progression using animal models of endometriosis and women with diagnosed endometriosis. Manuscripts reporting prospective data wherein diets were assessed via food frequency questionnaires and hence, maybe subject to recall bias, are not included in this review. Several important points are worth-noting from these collective studies. First, dietary factors with known anti-inflammatory effects can mitigate disease progression, assessed as lesion size in mouse models and/or decreased risk for advanced endometriosis stage and/or reduction in pain symptoms in afflicted patients. The various dietary factors evaluated (e.g. green tea, resveratrol, fish oil, soy isoflavones) have shown health benefits in many previous experimental animal and human studies, and thus, their ability to alleviate endometriosis is not entirely surprising. Second, women with endometriosis (and their lesion stromal cells) and mouse models of the condition respond similarly to dietary factors with anti-inflammatory effects, consistent with chronic inflammation as an underlying driver in endometriosis establishment and progression. Third, polyunsaturated fatty acids, fish oils, vitamins, and flavonoids as candidate molecules in the management of endometriosis pain and in reducing lesion size are in keeping with previous reports from dietary recall questionnaires suggesting a negative association between consumption of fish oils, green vegetables, fruits and dairy products, and endometriosis risk.23–25
Dietary factors and endometriosis risk.
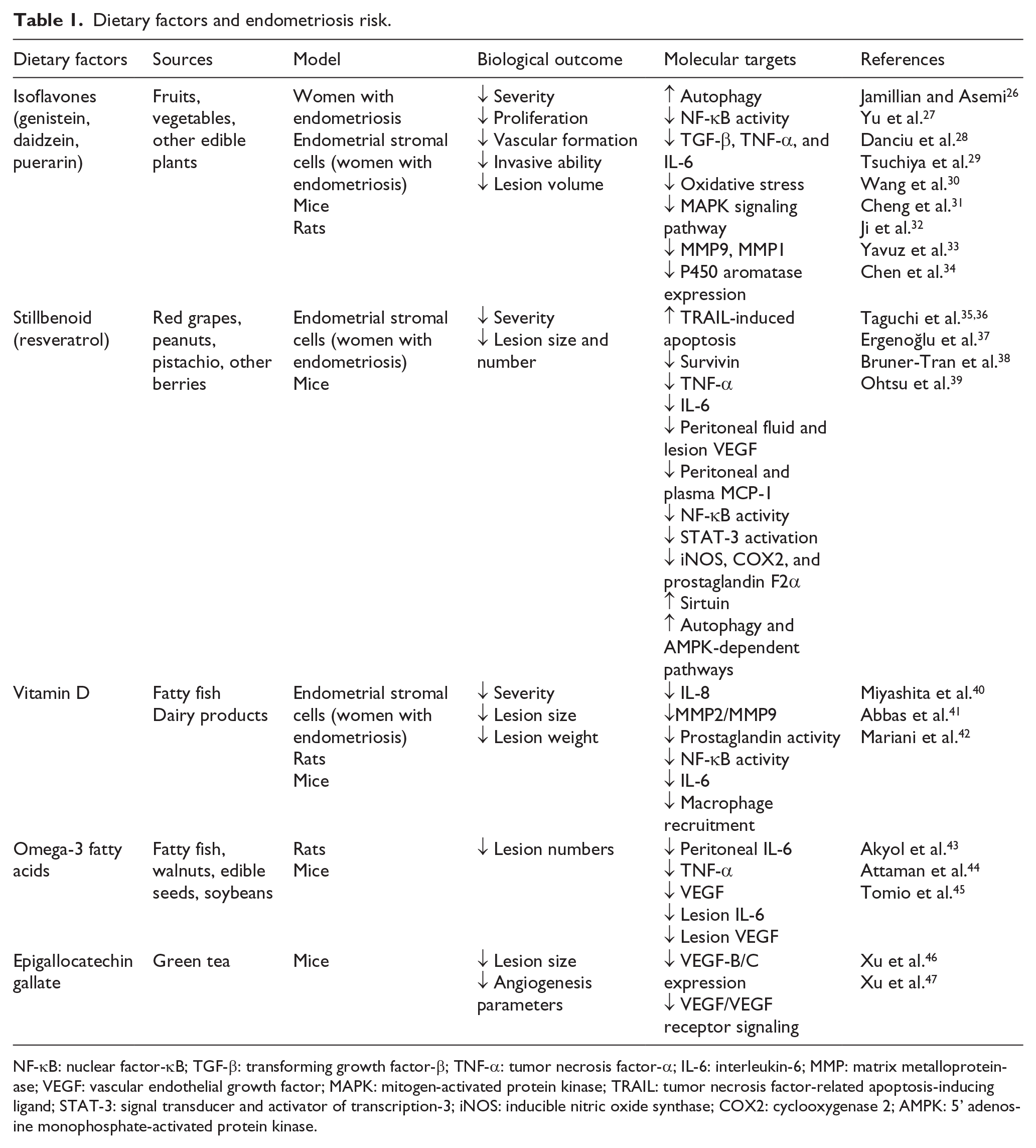
NF-κB: nuclear factor-κB; TGF-β: transforming growth factor-β; TNF-α: tumor necrosis factor-α; IL-6: interleukin-6; MMP: matrix metalloproteinase; VEGF: vascular endothelial growth factor; MAPK: mitogen-activated protein kinase; TRAIL: tumor necrosis factor-related apoptosis-inducing ligand; STAT-3: signal transducer and activator of transcription-3; iNOS: inducible nitric oxide synthase; COX2: cyclooxygenase 2; AMPK: 5’ adenosine monophosphate-activated protein kinase.
In a recent study, gluten-free diet showed a significant positive effect in reducing pain symptoms in endometriosis patients. 48 The retrospective study involving 150 women in each of two groups (group 1 = gluten-free diet + dienogest; group 2 = dienogest alone) is a single report that requires additional follow-up investigation. However, gluten-free diet is prescribed for patients with celiac disease caused by an overactive cytokine network.49,50 Moreover, women with celiac disease demonstrated increased risk for endometriosis 51 and infertility. 52 Thus, this dietary regimen may be equally useful in tempering the heightened inflammatory status associated with endometriosis.
Molecular targets of dietary components in endometriosis
The link between endometriosis and systemic/local immune dysfunctions, while well-established,13,53 remains a “chicken or egg” dilemma. In effect, it is not known whether endometriosis predisposes to an inflammatory state or whether chronic inflammation leads to the development of endometriosis. Nevertheless, the inflammatory environment caused by endometriosis is considered to contribute to infertility due to effects of pro-inflammatory cytokines on endometrial receptivity and embryo implantation54,55 and to other pregnancy complications in women with the disease. 56 In a recent review, Alderman et al. 57 described how systemic effects associated with endometriosis may underlie its co-morbidities including cancers, cardiovascular and autoimmune diseases, and pain. Several signaling molecules including cytokines, chemokines, and micro-RNAs, and the recruitment of bone marrow-derived stem cells into endometriotic lesions were discussed as contributory to systemic pathogenesis in endometriosis. Readers are referred to this review for more details. 57
Since inflammation is potentially at the top of the regulatory loop leading to endometriosis, maintaining a systemic non-inflammatory state or targeting low-level inflammation may conceivably alleviate endometriosis development and/or recurrence. Studies from our own group in conjunction with findings from other laboratories suggest a plausible mechanism by which inflammation may initiate the process of endometriosis at the level of the endometrium (Figure 1). This model invokes the loss of expression of certain regulatory molecules (e.g. Krüppel-like factor 9 (KLF9), progesterone receptor) and the over-expression of others (estrogen receptor-β, interleukin-6 (IL-6), Notch-1 activation) leading to compromised uterine glands and stroma with unique molecular defects that foster their residence in ectopic sites. 58 The loss of KLF9 promoted lesion establishment in a mouse model of endometriosis, 59 consistent with the lower abundance of KLF9 transcripts found in eutopic endometria of women with endometriosis relative to endometria of women without disease. 60 Resistance to progestin is a well-established feature of eutopic endometria and ectopic lesions of women with endometriosis due in part, to loss of progesterone receptor expression. 61 The over-expression of estrogen receptor-β leads to inflammation in endometriosis, 62 and interestingly, lesions lacking KLF9 from experimentally induced endometriosis in mice were associated with increased levels of this estrogen receptor isoform. 59 Additionally, Notch-1 signaling activation promotes 63 and is promoted 64 by inflammation, is linked to endometriosis in a mouse model, 59 and is shown to downregulate progesterone receptor expression via increased promoter methylation in uterine endometrial cells. 65 Finally, the pro-inflammatory molecule IL-6, an inhibitor of progesterone receptor expression, 66 is up-regulated in endometriotic lesions,59,67 whereas progesterone inhibits inflammatory response pathways in uterine endometriotic stromal cells. 68 While there are gaps in this model given the current unknowns and the multi-factorial and polygenic nature of endometriosis, it is reasonable to predict that diets and dietary factors that can significantly impact inflammation-initiated events may influence endometriosis progression and recurrence.
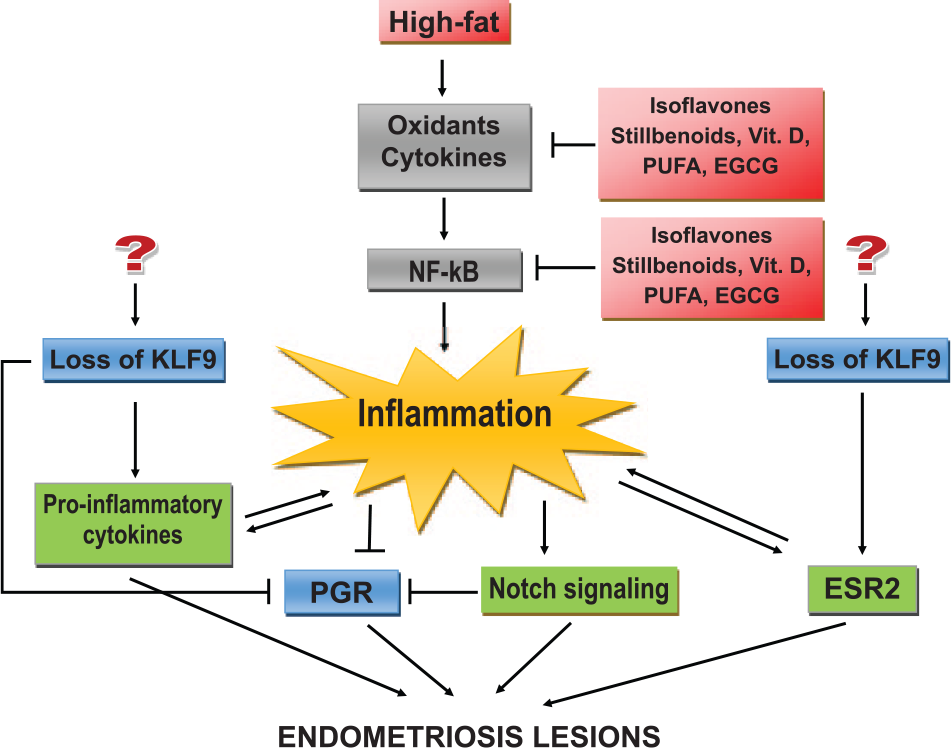
Schematic diagram of inflammation-mediated events in endometriosis and potential intervention points for diet/dietary factors. Inflammation can result in endometriosis lesion establishment through multiple pathways, which may be targeted by dietary factors (described in text).
The current literature highlights an abundance of anti-inflammatory foods recommended by nutrition experts, which consist of fruits and vegetables, whole grains, plant-based foods (beans, nuts), fatty fish, and spices. The molecular targets of the various dietary constituents present in these anti-inflammatory foods that may be useful to ameliorate endometriosis are presented in Table 1. Phytoestrogens present in many vegetables, fruits, and other edible plants include isoflavones, lignans, and stilbenoids. Isoflavones can influence inflammation through multiple mechanisms namely promotion of autophagy, down-regulation of transcription factor nuclear factor-κB (NF-κB) activity, reduction of inflammatory cytokine production (e.g. transforming growth factor-β (TGF-β), tumor necrosis factor-α (TNF-α), IL-6), and inhibition of oxidative stress.26–28 In line with the anti-inflammatory effects of isoflavones, women with endometriosis consuming isoflavones (measured by urinary levels of genistein and daidzein) showed decreased risk of advanced endometriosis (Stages III and IV) 29 and incorporation of soy isoflavone genistein in diets of mice with endometriotic implants resulted in regression of ectopic lesions relative to diets without genistein. 33
Another isoflavone found in arrowroots endemic to Japan and China is puerarin. Puerarin demonstrates inhibitory effects on estradiol-17β-induced proliferation, vascularization, and invasive ability of stromal cells isolated from women with endometriosis. Multiple mechanisms through which it is considered to exert its actions include the targeting of matrix metalloproteinase 9 (MMP9) and tissue inhibitor of metalloproteinase-1 expression, inhibiting the recruitment of nuclear receptor co-regulators to the estrogen receptor-α in promoter/regulatory regions of target genes, and suppressing the mitogen-activated protein kinase (MAPK) signaling pathway.30–32 In a rat model of endometriosis, orally administered puerarin reduced lesion estrogen production by inhibiting local aromatase expression, resulting in reduced lesion volume. 34 These collective data suggest the potential for puerarin as a therapeutic agent for disease management.
Resveratrol, a stillbenoid, is a polyphenol found in foods such as red grapes, peanuts, pistachio, blueberry, and various other berries. This compound was found to decrease ectopic lesion size in a mouse model of endometriosis concurrent with reductions in peritoneal fluid vascular endothelial growth factor (VEGF) and peritoneal and plasma monocyte chemoattractant protein-1 levels, and in lesion VEGF expression. 37 In a nude mouse model implanted with human endometriotic tissues, systemic administration of resveratrol decreased lesion numbers (by 60%) and volume (by 80%); this was partly attributed to the reduction of the ability of endometriotic stromal cells to invade matrix in vitro with resveratrol treatment. 38 In endometriotic stromal cells derived from women with endometriosis, resveratrol inhibited survivin expression, enhanced tumor necrosis factor-related apoptosis-inducing ligand (TRAIL)-induced apoptosis, 36 and dose-dependently suppressed TNF-α-induced release of the pro-inflammatory cytokine IL-6. 35 Other potential mechanisms by which resveratrol may inhibit lesion establishment via its anti-inflammatory effects, based largely on its actions in other target systems, include inhibition of NF-κB activity, signal transducer and activator of transcription-3 (STAT-3) activation, and production of inducible nitric oxide synthase (iNOS), cyclooxygenase-2 (COX2), and prostaglandin F2α and conversely, promotion of autophagy, 5’ adenosine monophosphate-activated protein kinase (AMPK)-dependent pathways, and sirtuin expression. 39
Vitamin D is a fat-soluble sub-class of steroids with multiple endocrine effects. While vitamin D is naturally found at high levels in foods such as fatty fish (salmon, tuna, mackerel) and in smaller amounts in others (cheese, egg, liver), many foods consumed by the general population (milk, yogurt, orange juice) are fortified with vitamin D. The involvement of vitamin D in endometriosis has been studied in women and in experimental animal models. In a double-blind clinical trial involving women with diagnosed endometriosis, Vitamin D supplementation had no effect in reducing dysmenorrhea and/or pelvic pain, relative to those without supplementation. 69 However, in an observational study involving women with ovarian endometriosis, those with lower serum levels of vitamin D (considered hypovitaminosis D) were more prone to have endometriosis than women with normal serum vitamin D levels. Interestingly, a linear correlation between serum 1,25(OH)-D3 levels and diameter of ovarian endometriomas was reported. 70 Women with severe endometriosis were also found to have significantly lower serum 1,25(OH)-D3 levels than non-diseased women and women with mild endometriosis. 40 Furthermore, in endometrial stromal cells cultured from ovarian endometriomas, addition of 1,25(OH)-D3 elicited an anti-inflammatory response, manifested as reductions in IL-8 and MMP2/MMP9 expression, prostaglandin activity, and NF-κB activation, relative to non-treated cells. 40 In animal models of endometriosis, vitamin D3 significantly reduced endometriotic lesion sizes (by 48%) in rats. 41 In mice, injection of elocalcitol, a vitamin D agonist decreased lesion weight up to 70%, and this was associated with reduced peritoneal inflammation, inhibition of macrophage recruitment and diminished cytokine IL-6 secretion. 42
Epigallocatechin gallate (EGCG) from green tea has powerful anti-angiogenic and anti-oxidant properties and predictably, has been linked to inhibition of endometriosis-like lesion formation in mouse models. Transplanted eutopic endometria isolated from patients with endometriosis generated smaller lesions with significantly reduced microvessel size and density and lower VEGF-B/C expression in nude mice ip injected with EGCG than with vehicle alone. 46 The reduced macrovascular network in lesions was shown to be mediated by EGCG inhibition of VEGF/VEGF receptor signaling occurring through interferon-γ, MMP9, and chemokine ligand 3 pathways. 47 Interestingly, vitamin E (a non-angiogenic anti-oxidant) did not mimic EGCG-elicited effects on lesions, suggesting angiogenesis as a major target of EGCG actions. 46
Of high relevance to endometriosis is consumption of a HFD, given the latter’s known effects in promoting metabolic dysfunction. Studies on the consequences of fat consumption (e.g. saturated fat in red meat) on endometriosis progression in women have not yielded a clear consensus of an association. 23,25 By contrast, a negative association between HFD and endometriosis 22 was established in a relevant mouse model of the condition. Nevertheless, the benefits of certain dietary fats (e.g. omega-3 polyunsaturated fatty acid (omega-3 PUFA)) on reducing endometriosis risk in women, based on prospective data, 23 were consistent with those obtained from animal studies. In particular, intake of 3-PUFA in a rat model of experimentally induced endometriosis caused significant regression of endometriotic implants, concomitant with decreased peritoneal levels of IL-6, TNF-α, and VEGF. 43 Moreover, transgenic Fat-1 mice which express high levels of endogenous 3-PUFA also displayed smaller endometriosis-like lesions and lower lesion IL-6 and VEGF levels when used as an endometriosis model, relative to wild-type mice. 44 Furthermore, using the same Fat-1 endometriosis model, feeding with eicosapentaenoic acid (EPA), an omega-3-fatty acid found in cold-water fatty fish such as salmon and in fish oil supplements, caused the suppression of endometriotic lesion formation in the peritoneum, which was attributed to lower IL-6 levels mediated by the 12/15-lysyl oxidase-pathway products of EPA. 45 In women, the relevance of EPA to endometriosis risk was evaluated in a cross-sectional study wherein women undergoing in vitro fertilization were measured for specific serum and total PUFAs and surveyed for their history of endometriosis. Result indicated an inverse correlation between serum EPA levels and endometriosis risk, that is, women with high serum EPA levels had 82% lower risk of endometriosis compared to women with low EPA levels. 71
Conclusion and future directions
Diet and nutrition have come of age to be at the forefront in the fight against endometriosis, based on recent evidence-supported studies describing the ability of foods with anti-inflammatory actions to mitigate endometriosis progression in animal models and patients alike. Nevertheless, there are some caveats to consider with the very promising data generated thus far. First, studies conducted in animal models predominantly utilized purified dietary factors, and the doses and routes of administration (intraperitoneal, oral gavage) do not recapitulate standard consumption by the general population. Second, in studies using immune-deficient mouse models, the lack of normal systemic anti-defense mechanisms may be confounding to the actual elicited benefits; hence, there is a need to re-examine these reported effects in validated immune-competent experimental animal models of endometriosis.22,62 Third, the period and duration of dietary exposure/consumption may need to be carefully considered in the design of clinical interventions and in studies using animal models, given that systemic environments significantly differ in reproductively aged women (e.g. young vs middle-age adults; obese vs normal weight) and in those with varying severity of the disease. Fourth, rodent models and humans can significantly vary with respect to bioavailability of dietary factors and tissue uptake. Finally, while the value of epidemiological studies cannot be underestimated in developing health policies and system research to achieve health goals, the limitations of recall-based studies must be taken into account when designing personalized therapeutic interventions for afflicted patients.
More effective interventions are required to address endometriosis. Understanding the convergence of diet and endometriosis may generate integrated strategies in clinical practices to improve the quality of life for symptomatic women. Dietary modification as a complementary approach and a short-term recourse to reduce the effects of inflammation associated with endometriosis is feasible, practical and can be monitored under physician supervision. Nevertheless, due in part to the complex nature of the condition and the lack of reliable markers to detect disease initiation, scientific-based data are currently deficient to support the ability of anti-inflammatory foods and food components to prevent endometriosis. Thus, a long-term goal for endometriosis research is to achieve a clear appreciation of key mechanisms that underlie disease pathology that can be targeted by dietary factors to manage not only disease progression and recurrence but for disease prevention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part, by the University of Arkansas for Medical Sciences Translational Research Institute (RCMS) and the University of the Philippines Office of the Vice President for Academic Affairs—Emerging Interdisciplinary Research (OVPAA-EIDR-C08-006) (MCV, RCMS).