
Abstract
We present a case report of a patient with laparoscopic surgery of a deep infiltrating endometriosis with a complicative course. In addition to a postoperatively diagnosed ureteral fistula with local inflammation, acute perforation and ultimately lethal bleeding from the adjacent external iliac artery occurred more than 3 weeks after surgery. To the best of our knowledge, a case with the same constellation has not yet been published. A literature review on the rare and comparable complication of a ureteroarterial fistula is discussed in connection with the case.
Introduction
For the surgical treatment of endometriosis, the minimally invasive approach has largely established itself as the primary approach in trained hands. 1 Resections of deep infiltrating endometriosis (DIE) of the uterosacral ligament (USL) in particular significantly increase the risk of injury to the ureter. 2
Coagulation of surrounding so called vasa vasorum – as they are present in ureters or arterial vessels, for example – increase the risk of necrosis. Secondary severe bleeding events in the sense of a ureteroarterial fistula with high mortality are described whereby this is mostly in connection with large oncological operations, radiotherapy and ureteral stents. 3 To the best of our knowledge, however, no case has been published where lethal bleeding of an iliac vessel occurred after ureteral injury without the aforementioned risk factors. An institutional review board was not required in the present case.
Case
A 47-year-old patient presented herself to our clinic because of increasing, periodic pain in the left lower abdomen. The patient had already undergone several laparoscopies due to pain and ovarian cysts; a caesarean section and an abdominal total hysterectomy were performed, one of which resulted in urinary bladder perforation, with intraoperative suturing. The patient was slightly obese (body mass index (BMI): 27.5) but otherwise healthy. The rectovaginal palpation resulted in a very painful thickening, starting at the left vaginal angle and extending into the left pelvic wall. A 25-mm large, bland cyst was visible in the left ovarian fossa by sonography. Lab results (blood count, C-reactive protein (CRP), and creatinine) were normal. The suspected diagnosis was a deeply infiltrating endometriosis of the left USL and superficial extrinsic infiltration of the ureter. Hydronephrosis had been preoperatively excluded by sonography.
The patient stated a strong desire for a surgical solution due to unbearable side effects or lack of effect of previous hormonal and pain medication. In a long consultation with two specialists and weighing the benefits and risks of surgical intervention, the patient wished to have the left ovary removed, including the deeply infiltrating endometriosis in this area. Minimally invasive surgery was performed by an experienced surgeon in the field of endometriosis. Operating time was 234 min with a blood loss of about 200 mL; the vital parameters during the operation were all in the normal range. A single-shot antibiotic with a third-generation cephalosporin was administered. After extensive adhesiolysis and exposure of the ureter, starting cranially of the crossing of the ureter and the left common iliac artery to just before confluence into the bladder, the ovary could be deposited at the infundibulopelvic ligament including the ovarian cyst. The sacrouterine ligament and the left ovary (which was to be removed) were located in a conglomerate with the ureter at the left vaginal margin, so that dissection of the individual structures was necessary in order to be able to safely remove the ovary and the sacrouterine ligament. For safe removal of the entire endometriotic nodule, a partial colpectomy of the left apex angle of approximately 20 mm was necessary. After a normal postoperative course, the patient could be discharged on the third day without any problems. A vaginal sonography and a sonography of the kidneys at discharge showed no abnormalities. Two weeks later, at postoperative day 14, the patient presented herself again to our clinic due to fluid in the vagina. Further diagnosis including computer tomography (CT) – performed on postoperative day 15 – revealed a ureterovaginal fistula with an inflammatory reaction along the dissected area. From the point of view of radiologists and urologists, further cross-sectional imaging (e.g. magnetic resonance imaging (MRI)) would not have yielded any further findings. Otherwise, the patient was without any symptoms. The patient was examined by urologists at postoperative day 15. Since the patient was asymptomatic except for the urine loss, and no larger urinoma was described in the imaging, the revision was planned electively as reimplantation of the ureter for the postoperative day 46. A few days later, the patient presented herself again to our clinic with vaginal bleeding. The examination showed a slight vaginal bleeding, most likely due to a small erosion in the area of the vaginal fistula. A mild hydronephrosis of the left side was visible by sonography, so the patient was recommended to see the urologist promptly – which she had not done directly at her own request. On the following day, the patient called the emergency doctor due to massive bleeding from the vagina. The patient was resuscitated and intubated on site and immediately admitted to the emergency department of the university hospital, where an interdisciplinary team of anaesthesists, radiologists, vascular surgeons, gynaecologists, urologists and internists was on standby. Nevertheless, due to the massive blood loss, all further resuscitation activities were frustrating and the patient died. The subsequent autopsy showed macroscopically a haemorrhagic soft tissue defect that was situated in direct proximity to the known ureterovaginal fistula and to the left external iliac artery (see Figure 1). A perforation of the left external iliac artery measuring a few millimetres was found to be the causative factor for the massive bleeding. Histology revealed an inflammatory soft tissue reaction along the course of the ureterovaginal fistula that lead to an inflammatory necrosis and subsequent perforation of the vascular wall.
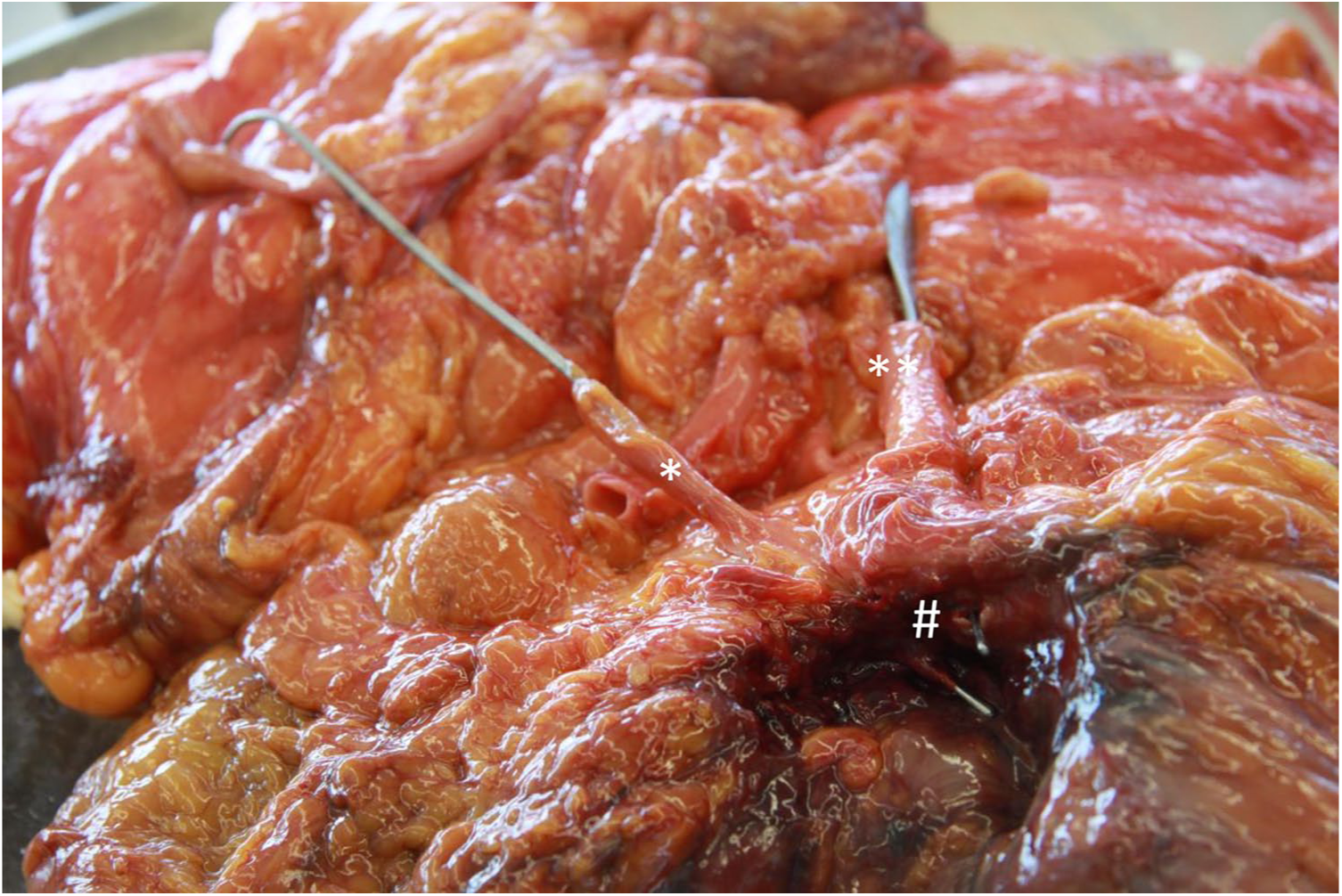
The two probes pass through the ureter (*) and the external iliac artery (**) and leave the respective organ through the perforation site (#).
Discussion
The preoperatively assumed cause of pain in our patient was a thickened residual left USL due to DIE and an endometrioma stuck – after previous hysterectomy – at the vaginal stump.
The risk of complications is substantially dependent on the location of the resection of the endometriosis site, for example, nodules on the USL or pelvic wall significantly increase the risk of injury to the ureter. 4 , 5 In our patient, the surgical strategy was to remove the left ovary and the endometriotic nodule at the USL as this was the reproducible area of the patient’s pain. Due to the physiological adhesion of the sigmoid colon to the left pelvic side wall, the dissection of the ureter is more difficult compared to the right side. It could also be shown that injuries of the left ureter are more frequent than injuries of the right ureter. 6 Furthermore – as in our case – this procedure was complicated by destruction of the anatomy because of previous operations and DIE. In a large review on the basis of 18 studies with a total of 700 patients and DIE of the ureter, Cavaco-Gomes and colleagues could also show that the rate of intraoperative diagnosed injuries of the ureter was very low, while in 2.1% (14/682) postoperatively a ureteral fistula or stenosis was diagnosed. 6
In a comparison of four different coagulation instruments (monopolar, bipolar, ultrasonic scalpel and CO2 laser), Tulikangas et al. were able to demonstrate in female pigs that the macroscopically perceived extent of thermal tissue damage differed significantly from the extent measured on the histological specimen. While a length of 0.4 ± 0.2 cm was measured intraoperatively after bipolar coagulation at the ureter, the damage was 1.5 ± 1.4 cm in length at the same site in the histologic preparation. In addition, five out of six samples showed an injury of the urothelium. 7
Nevertheless, the question remains as to what extent the external iliac artery was damaged thermally or by laceration during the first operation so that it could open 5 weeks later? And, to what extent did the ureteral fistula and the leaking urine cause an inflammation that could contribute to the perforation of the external iliac artery?
In regard to histological standpoints, perforation of the external iliac artery was most likely due to an inflammation in the surrounding tissue encroaching on the arterial wall and leading to a circumscribed necrosis of the arterial wall. No signs of a preexisting vessel abnormality or a vasculitis were found. The examined vasa vasorum was found to be open. The etiology of the inflammation remains ambiguous. We discussed an (ascending) infection caused by the ureterovaginal fistula, as well as soft tissue necrosis caused by the leaking urine or by ischaemia. Special conspicuous features favouring an ischaemic etiology included thrombosed blood vessels, extensive fibrosis and scar tissue surrounding the wound cavity, which was attributed to previous operations and most likely negatively influencing tissue repair and wound healing.
There are a number of case reports with ureteroarterial fistula and consecutive massive macrohaematuria with a reported mortality rate of up to 58%. 8 There are slightly more than 150 cases described so far in the literature. 9 Although the actual underlying pathophysiology for fistula formation has not yet been fully understood, major surgical interventions in the pelvis with damage to the vasa vasorum on the ureter and artery as well as radiation appear to play an important role due to local damage and necrosis. 9 In addition, the constant pulsation of the artery seems to have an influence on the formation of a fistula between ureter – mostly with a double J catheter in it – and artery where the two organs are in contact. 9 While primary ureteroarterial fistulas are always caused by an abnormality of the arterial vessel (e.g. aneurysm or vascular surgery), secondary fistulas, which are much more common, develop mainly in connection with large gynaecological or urological cancer surgeries, insertion of ureteral stents and devascularisation of the ureter. 3 Surgery alone without further therapeutic interventions has not yet been described in connection with the development of a ureteroarterial fistula. So, the question is whether the patient had any change in the arterial wall (primary or secondary) that favoured perforation and thus lethal bleeding? As described above, no systemic vascular diseases were known in the patient’s anamnesis and were not diagnosed in the histological examination.
Finally, the therapeutic options for acute haemorrhage from a large arterial vessel are limited and made more difficult by the enormous loss of blood within a very short time. In our case, the patient was found at home (about 30 min away from the clinic) unconscious and with massive bleeding from the vagina. Emergency laparotomy and suturing of the perforation site or endovascular insertion of a stent are the therapy of choice, but still have a mortality rate of up to 58%. 8 However, the aforementioned reviews also included patients who have already been in hospital, but whose rapid blood loss due to arterial bleeding ended lethally. The limitations to transfuse blood products and the time delay until arrival at the emergency unit were additional factors in our case that reduced the patient’s probability of survival to a minimum from the outset. Whether the course would have been more favourable in an inpatient setting must nevertheless be doubted, since it is ultimately an extremely rare and potentially life-threatening bleeding because it progresses rapidly.
Conclusion
In the patient information on major surgical procedures for endometriosis with a clearly anticipated high degree of difficulty, the patient must also be made aware of extremely rare life-threatening complications. The risk of complications increases especially if the patient had already undergone several operations before. When a postoperative complication occurs, an immediate management should be required. For the future, we have, together with our colleagues in urology, adapted the treatment in similar cases and treat this complication exclusively as inpatient and emergency cases.
Footnotes
Author contributions
P.W. and N.d.G. contributed to the study conception and design. P.W. and W.J. contributed to the data collection. P.W., J.B. and N.d.G. contributed to the data analysis and interpretation. P.W. was the responsible surgeon or imager. P.W. and W.J. contributed to the manuscript preparation. P.W., W.J., J.B. and N.d.G. contributed to the patient recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not sought for this study because of its retrospective, non-experimental nature.
Informed consent
Written patient informed consent was not possible to obtain in this particular case, since the patient died after treatment.