
Abstract
Introduction: Abdominal wall endometriosis (AWE) is the presence of ectopic endometrial tissue in abdominal wall and is most frequently encountered in women with previous cesarean section (CS). The aim of this study is to evaluate the possible risk factors of AWE development. Methods: Women with previous CS and pathologically confirmed AWE were included into the study (n = 33). Controls (n = 127) were randomly selected among women who had previous CS and absence of AWE were confirmed by physical examination. Clinical characteristics of the patient and the CS operation preceding AWE were recorded. Results: CS was performed before onset of labor in 87.9% in AWE and in 59.1% of control group (p = 0.002). The antenatal BMI and weight gain during pregnancy were significantly higher in AWE patients (p < 0.0001; p = 0.002, respectively). In logistic regression model procedure duration (p = 0.039; OR = 1083), antenatal BMI (p = 0.003; OR = 1254), weight gain (p = 0.002; OR = 1171), and CS before spontaneous labor (p = 0.021; OR = 5169) were significant parameters for predicting AWE. Discussion: High antenatal BMI, weight gain during pregnancy, and longer duration of operation are all factors effecting subsequent AWE development. However, CS before spontaneous labor is by far the most powerful risk factor for AWE development.
Keywords
Introduction
Endometriosis is the presence of implants of endometrial tissues, including glands and stroma, outside the uterine cavity. 1 Abdominal wall endometriosis (AWE), on the other hand, is the presence of embedded ectopic endometrial tissue between the muscles and adipose tissue of the abdominal wall. It is the most frequent type of extra pelvic endometriosis. 2 AWE consists of a wide range of pathologic conditions. All kinds of scars related to abdominal surgical conditions may give rise to AWE. 3 Although women with no prior abdominal operation might also rarely develop AWE, it is most frequently encountered in women with previous cesarean section (CS).4–6 Despite the frequent utilization of CS, the prevalence of AWE is 0.03%–0.45%. 7 This certainly suggests the presence of a complex etiopathogenesis and multiple risk factors. 8 Various risk factors like age at CS, menorrhagia, CS before the onset of labor, duration of CS, high body mass index (BMI), parity, number of previous CS, and duration of lactation were studied in limited number of case controlled studies.6,9 The results, on the other hand, are inconclusive.
The prerequisite for AWE following a CS is the presence of a CS operation. From this point of view, the aim of this study is to evaluate and determine the possible risk factors involving the characteristics of the patient as well as the CS operation preceding the development of AWE.
Methods
This is a case-controlled, cross-sectional study and was methodologically designed and conducted according to the checklist of items according to STROBE Statement. 10 All the procedures in this study were in compliance with the institutional and national research committee ethical standards and the 1964 Helsinki Declaration and its later amendments. Approval for the study was granted by Niğde Ömer Halisdemir University Ethics Committee (23.07.2020; 2020/16).
The electronic medical records of 11,439 women who had undergone CS in Niğde Ömer Halisdemir University Training and Research Hospital were analyzed retrospectively between January 2010 and January 2021 and 39 anonymous records with histopathology proven AWE were detected. The flowchart of the study population was demonstrated in Figure 1. Thirty-three women who had CS with Pfannenstiel incision and developed histopathologically proven AWE at the site of the cutaneous incision constituted the AWE group.
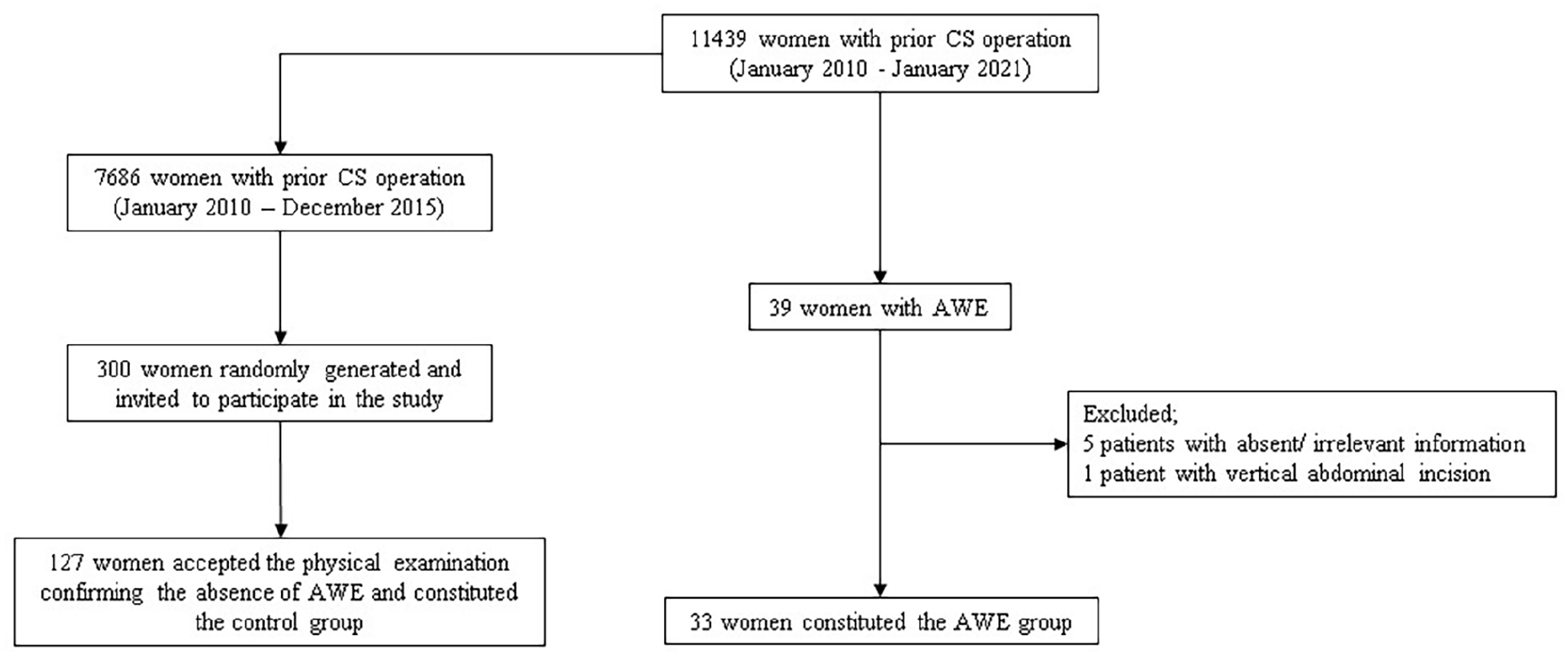
Flowchart of the study population.
AWE following CS is a clinic condition with long latent period and in a meta-analysis the mean interval from the original surgery to presentation of AWE was reported as 3.6 years. 11 Therefore, women for control group were randomly selected among 7686 patients who had undergone CS in our hospital between January 2010 and December 2015. The minimum number of women needed for the control group was calculated by power analysis calculations using G*Power 3.1.12,13 A priori analysis using a two-tailed test, a strong effect size (d = 0.8), and an alpha of 0.05, showed that an allocation ratio of at least 1:3 (patient:control) was required to achieve a power of 0.97 with 33 AWE patients. Therefore, at least 102 women without AWE were required for the control group. In total, 300 women were randomly assigned using SPSS 22 version. Each woman was contacted by telephone or e-mail and invited for participation in the study. Out of these, 127 women who responded to the invitation were informed in detail about the study and a written consent was obtained. Subsequently, the medical history was taken and physical examination were performed in each volunteer and the absence of AWE was confirmed medically.
The dataset for the present study was constituted by using hospital’s computer based database system for both AWE patients and controls. Clinical characteristics (age, height, weight at the first antenatal visit, weight at the time of CS, presence of menstrual irregularities and medically diagnosed pelvic endometriosis or infertility), obstetric history (number of previous CS operations, presence of spontaneous onset of labor before CS and lactation period), and characteristics of the CS operation (length of hospital stay, duration of surgery, and amount of blood loss) were recorded for each patient. Weight at the first antenatal visit was accepted as valid and recorded if the aforementioned visit occurred before the completion of 12th gestational week. Blood loss was referred to the difference in Hb levels (g/dL) in the complete blood count studied before and after CS operation. The onset of spontaneous labor before CS was referred to the presence of labor and was defined as the presence of cervical dilatation of at least 3 cm with regular uterine contractions before the CS operation was performed.
For statistical analysis IBM SPSS Statistics 22 version (IBM, Chicago) was used. p values <0.05 was accepted as statistically significant. The descriptive statistics were expressed as mean ± SD for continuous variables and as % (range) for categorical variables. The continous variables were compared with Student’s t test. The categorical variables were compared with either Pearson χ2 test or Fisher Exact test where appropriate. Logistic regression analysis was featured to determine the most relevant factors and the predictivity of the factors were expressed in terms of odds ratio (OR).
Results
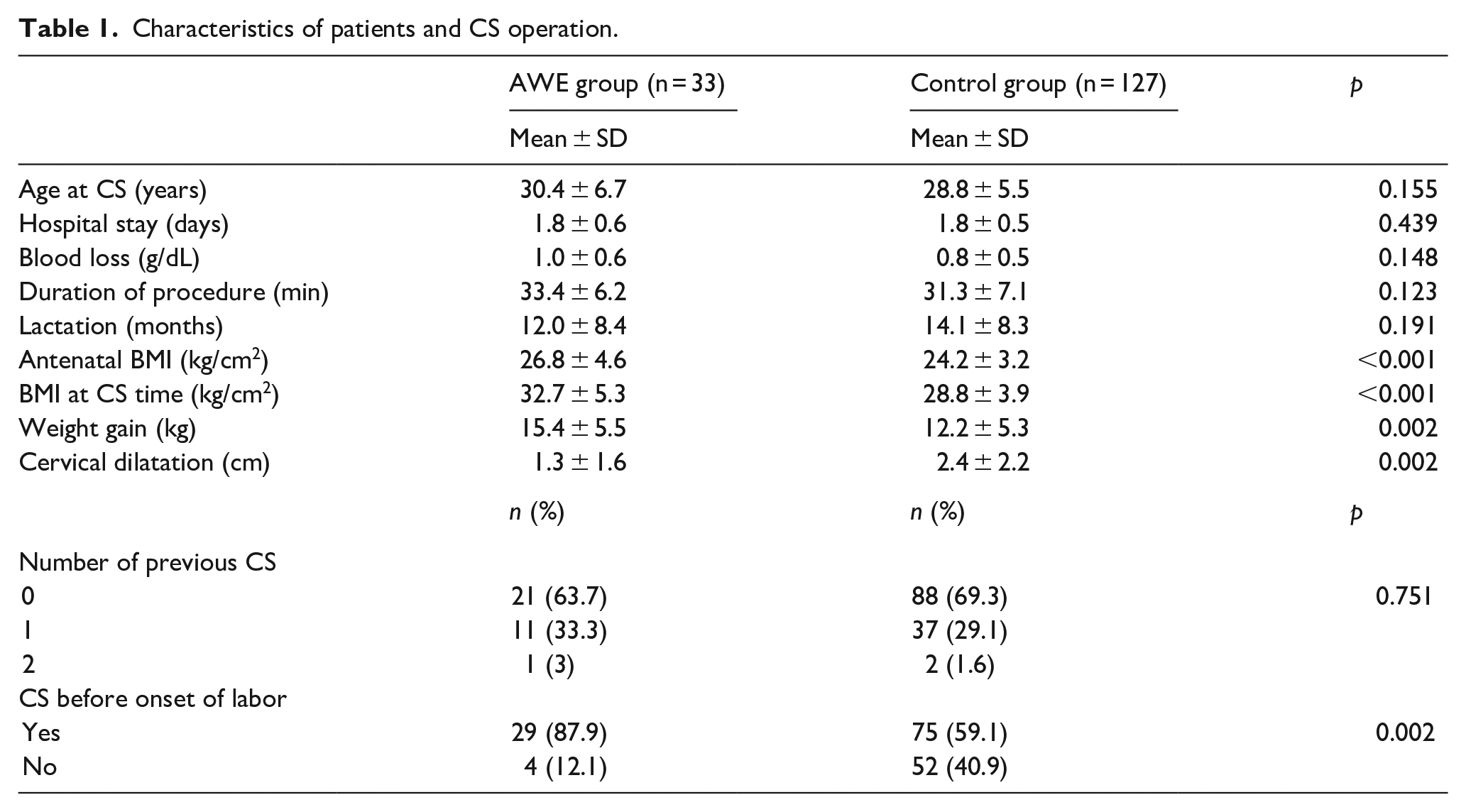
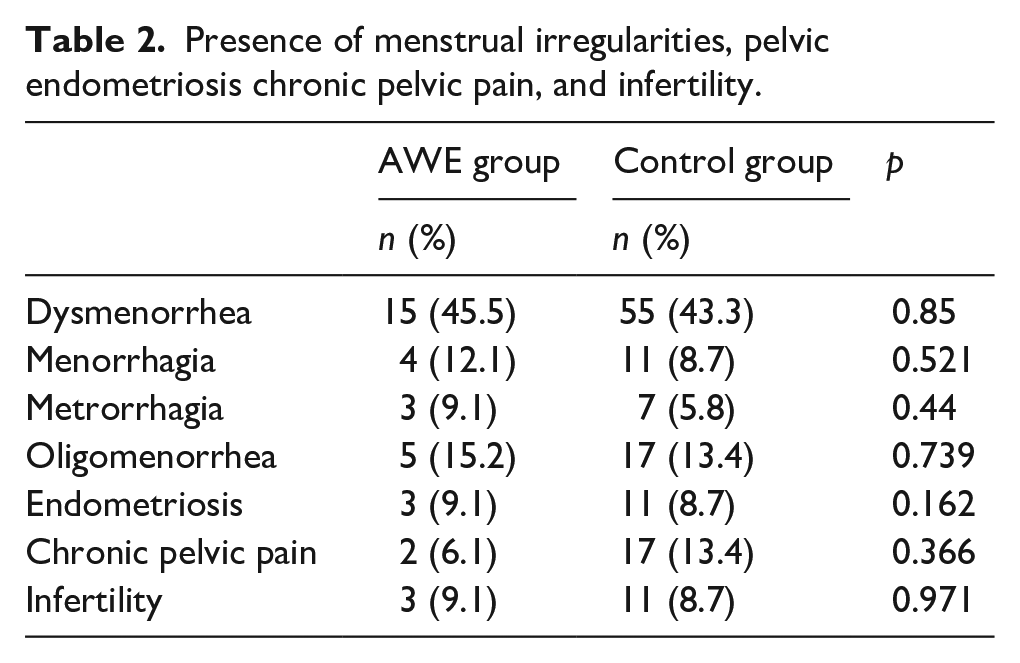
The number of patients included into the study was 33 for AWE group and 127 for control group. The clinical characteristics of the patients and the CS operation were listed in Table 1. The average antenatal BMI and BMI at the time of CS were significantly higher on the AWE group (26.8 ± 4.6 vs 24.2 ± 3.2; p < 0.0001 and 32.7 ± 5.3 vs 28.8 ± 3.9; p < 0.0001, respectively). Weight gain was also significantly higher in the AWE group (15.4 ± 5.5 and 12.2 ± 5.3; p = 0.002). In AWE group significantly higher percentage of women had CS before onset of labor (87.9% and 59.1%; p = 0.002). Accordingly, the average cervical dilatation was significantly higher in the control group (2.4 ± 2.2 and 1.3 ± 1.6; p = 0.002). The menstrual characteristics of the AWE and control groups were listed in Table 2. These characteristics were similar between study groups.
Characteristics of patients and CS operation.
Presence of menstrual irregularities, pelvic endometriosis chronic pelvic pain, and infertility.
The logistic regression model of the dataset was presented in Table 3. In the equation, procedure duration (p = 0.039; OR = 1.083), antenatal BMI (p = 0.003; OR = 1.254), weight gain (p = 0.002; OR = 1.171), and CS before spontaneous labor (p = 0.021; OR = 5.169) were significant parameters for predicting AWE. It is of note that out of the independent risk factors of AWE, only CS before the onset of labor had an OR of high predictivity, the remaining factors demonstrated rather weak predictivity (Table 3).
Logistic regression model for predicting the development of AWE after CS.
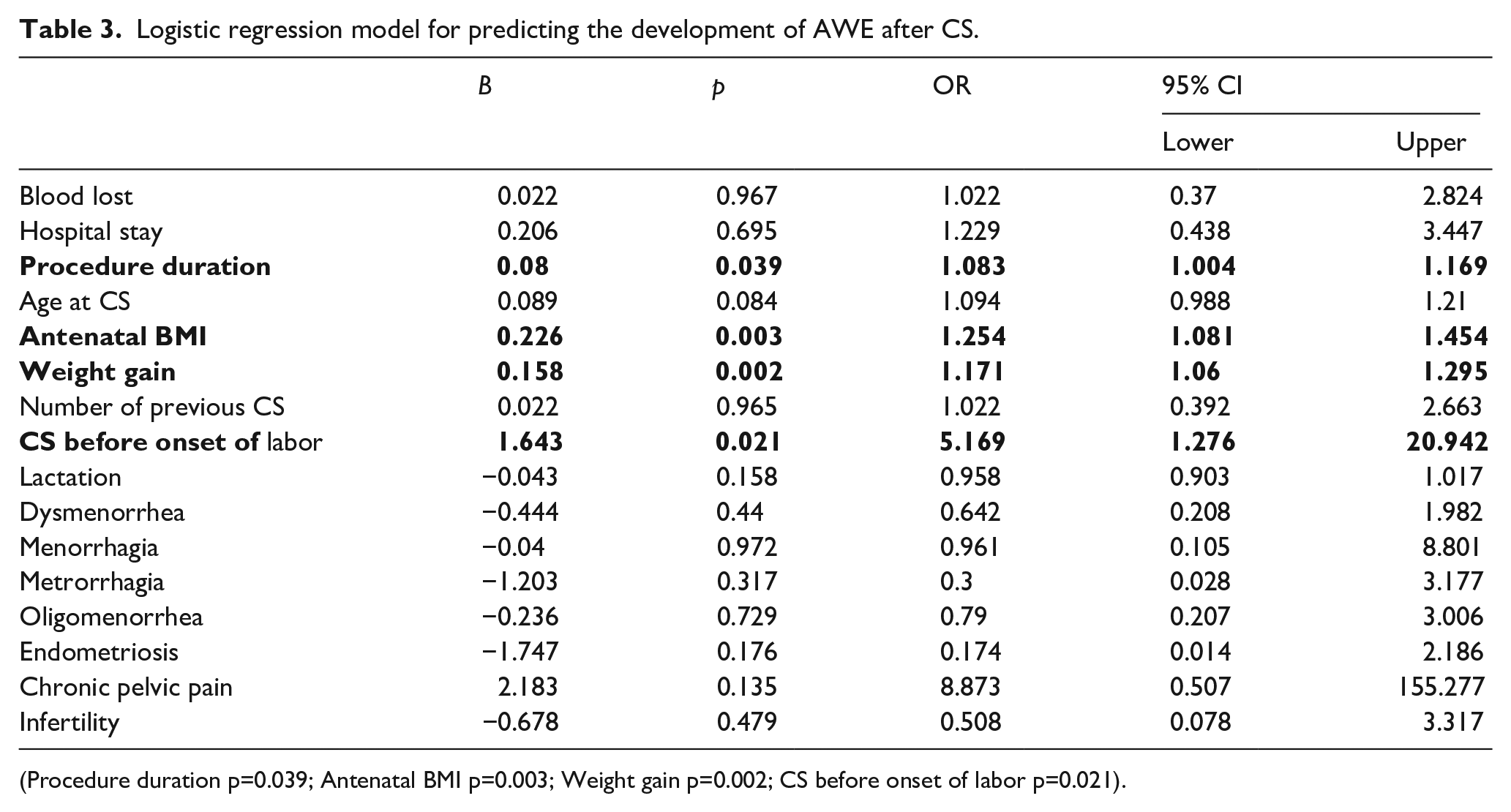
(Procedure duration p = 0.039; Antenatal BMI p = 0.003; Weight gain p = 0.002; CS before onset of labor p = 0.021).
Discussion
The results of the present study demonstrate that CS operation performed before the onset of labor has the highest OR for predicting AWE development. Besides, antenatal BMI, gestational weight gain, and duration of CS operation were additional independent risk factors. However, all these latter parameters bear an OR of rather weak strength. Although, previously, case-controlled studies investigating the risk factors for AWE were reported, the present study is the first study investigating the risk factors for AWE specifically following a CS operation.6,9 In the case-controlled study of De Olivera, the authors applied multivariate analysis for various factors and concluded that CS operation before the onset of labor is the main risk factor for AWE and that menorrhagia and alcohol consumption were also risk factors. 9 Khan et al. 6 in the final multivariate model concluded that history of a previous laparotomy was an independent risk factor for AWE.
The etiopathogenesis of AWE is not clear, however, different mechanisms are blamed for different types of AWE. 14 For development of AWE following a CS operation, primarily implantation theory and immunologic theory were held responsible.15–17 The transportation of viable endometrial cells from uterus to the cutaneous wound via surgical tools, sponges or gloves is the central pillar of the implantation theory.14,18 The immunologic theory, on the other hand, is mainly explained by the physiologic suppression of the cellular immunity for survival of the fetus during pregnancy. 19 Accordingly, this mechanism facilitates the implantation and survival of the foreign endometrial cells as well. 17 Therefore, the assumption in the present study was that some characteristics of the CS operation and/or the pregnant woman might as well contribute to AWE development.
Obesity certainly facilitates the accumulation of transported endometrial cells in the pouches among subcutaneous layers. The association of obesity with AWE has been investigated previously. Yela et al. 20 reported an average BMI value of 26.5 in their case series of 52 patients with AWE. In the case series of Ecker et al., 21 70.8% of the 65 women with AWE were in overweight and obese category. Khan et al., 6 also investigated BMI in the previously mentioned case controlled study and reported that patients with AWE were significantly more overweight than controls (BMI levels 29.2 and 26.4 respectively).
However, it is important to emphasize that the BMI value investigated in all the previously mentioned studies is the BMI value of the women at the time of endometriosis excision operation. In the present study the BMI values of the patients at the time of CS preceding AWE development were investigated for the first time in literature and results demonstrated that BMI both at antenatal period and at the time of CS were weak, yet independent, risk factors for AWE development. Additionally, our findings indicate that the duration of surgery was also one of the independent factors with a weak strength in the development of AWE. It is not surprising that the procedure would take longer in obese patients and as a matter of course the duration of the procedure and obesity both directly effect the extent of exposure of cutaneous wound to endometrial cells. Therefore, changing tools, sutures, sponges, compresses, and abdominal dressings after suturing uterus as well as irrigating fascia, muscles, and subcutaneous tissues after closing the peritoneal layer are the main preventive measures for AWE development.4,8 Nevertheless, the spread of endometrial cells to the cutaneous wound to some extent is inevitable and is a matter of course during a CS procedure. The question is why only a minority of women undergoing CS, present with an ectopic endometriotic tissue in the cutaneous wound? Wicherek et al. 17 found that CS before onset of spontaneous labor is the main risk factor for scar endometrioma in their case series. The most effective predictor of AWE development, with a high strength, was the presence of CS before the onset of spontaneous labor in the present study as well and therefore the previously published results were validated.9,17
Endometriotic tissue is highly susceptible to hormonal stimulus and behaves like an expanding tumoral mass in an appropriate hormonal milieu. 19 Farland et al., 22 found a negative correlation between lactation and endometriosis development. In the present study the lactation period was similar between groups. Actually lactation is a temporary period and the mechanism underlying the correlation between lactation and endometriosis is partially, but not fully, influenced by postpartum amenorrhea. 22 Therefore, it is more likely that lactation does not protect against AWE but might prolong the latent period.
Another aspect of individual differences between women is the menstrual characteristics. Menorrhagia was defined as a possible risk factor previously. 9 Nevertheless, as an answer to this question in the present study the number of women with a history of menorrhagia, metrorrhagia, dysmenorrhea, and oligomenorrhea were similar between AWE and control groups and none of the menstrual characteristics were independent parameters of AWE prediction.
This is a relatively large dataset when compared to the similar reports in the literature. In most of the case series it is not possible to make the discrimination between different forms of AWE.6,9,19 Additionally case controlled design is the best method of studying chronic, rare conditions presenting with relatively long latent periods which exactly describes AWE. 23 Meanwhile the retrospective design is the main limitation of our study. First of all, in retrospective reviews information bias is mainly the result of missing or illegible data and/or errors in data collection. Additionally, AWE is a multifactorial condition and definitely some other factors absolutely would interfere with its development. The authors recorded the data available in retrospective records which limits the factors taken into consideration in the logistic regression model.
High antenatal BMI, weight gain during pregnancy, and longer duration of operation are all factors effecting subsequent AWE development. However, CS before spontaneous labor is by far the most powerful risk factor for AWE development. Clinicians need to think twice before making the CS decision in any case but especially in obese women. Also necessary intraoperative precautions must be taken and procedure needs to be completed as quick as possible in order to prevent contamination of endometrial tissues to surgical margins. Finally, in all women, but far more attentively and carefully in obese women the timing of elective and repeated CS needs to be considered and is better planned after the appearance of spontaneous uterine contractions.
Footnotes
Acknowledgements
There is no acknowledgments.
Authorship
PE and AE were responsible for study protocol. AE, HB, and CÖ were responsible for data collection. PE was responsible for data analysis and data interpretation. PE and AE were responsible for drafting the manuscript. All the authors contributed to the critical review of the manuscript and agreed on the final layout for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval for this study was obtained from Niğde Ömer Halisdemir University Ethics Committee (23.07.2020; 2020/16).
Informed consent to participate
Written informed consent was obtained from all subjects before the study.
Informed consent to publish
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Not applicable.