
Abstract
Introduction:
Recent studies have proposed that advanced endometriosis might harbor histopathological, molecular, and genetic properties of malignant lesion. Thus we aimed to investigate the presence of Ki-67 staining index (KSI) and BRAF mutation in patients with and without recurrent endometriosis of stage III and IV.
Materials and methods:
Cross sectional study on 50 consecutive patients with endometriosis of stage III and IV was performed. Tissue specimens collected during laparoscopic surgery were used for the evaluation of presence of KSI and BRAF mutation. Also, serum levels of tumor markers including CA-125, CA19-9, AMH and αFP were gathered.
Results:
The mean ± SD of KSI was 12.18 ± 16.58. Forty-one out of 50 (82%) patients had a non-recurrent disease. KSI ⩾ 10% was found in 20 patients (40%). Furthermore, 29 patients (58%) and 13 patients (26%) had high levels of CA-125 and CA19-9, respectively. No evidence of significant correlation was observed between the KSI and CA-125 and CA19-9 (all p values > 0.05). However, a positive correlation was observed between CA-125 and CA19-9 (r = 0.55, p-value = 0.02). KSI level was insignificantly lower in recurrent patients compared with non-recurrent patients (9.78 ± 6.24 vs 12.71 ± 18.09, p-value = 0.33). Other tumor markers did not show any statistically significant difference (all p values > 0.05). None of the participants had BRAF V600E mutation.
Conclusion:
Endometriosis manifests malignant behavioral of rapid proliferation but the exact genetic alteration causing this phenomenon is not understood.
Introduction
Endometriosis is defined as the presence of endometrial glands and stromal tissue outside the uterus cavity which may be associated with infertility and pelvic pain. 1 Various genetic, environmental, and immunological factors along with hormonal profile alterations have been proposed to be the underlying etiological factor. However, the exact cause of endometriosis is still unknown.
Although endometriosis is known to be a benign disease, recent studies have suggested that endometriosis should be considered a neoplastic process, because of histopathological, molecular, and genetic similarities between endometriosis and malignancy. The recurrence rate of endometriosis is high, and it is estimated to be around 40%−50% in 5-year follow ups. 1 Similar to a neoplastic process, it is unclear why endometriosis behaves progressively and aggressively in some patients. It seems that the recurrent lesions may originate from the residual structures or de novo cells.2,3 A recent review study discussed the malignant transformation of endometriosis to neoplasia and different carcinoma over the time. They found an ectopic endometrium attached to the tumor, which proves the link between endometriosis and malignant processes. 4 Adequate information and knowledge about the risk factors of recurrent endometriosis could be useful to prevent it. Moreover, identifying related biomarkers could help develop targeted therapies. Despite the importance of clinical findings in predicting disease recurrence, obtained biochemical markers of patients are also very valuable for the assessment of recurrence.
The clinical course of endometriosis which usually begins with an attack, continues with proliferation and, eventually destroys the organ mimicking a tumor-like behavior. In this regard, the evaluation of tumor-related biomarkers has considerable interest. Ki-67 is a nuclear non-histone protein found in all active phases of cell division. It shows various morphological features of cell proliferation. 5 The expression of Ki-67 is strongly associated with tumor cell growth and proliferation. It is also commonly used in clinical practice for cancer management and tumor grading. The high Ki-67 staining index (KSI) in tumors such as breast, lung, and lymphoma indicates a poor prognosis and advanced disease. 6
On the other hand, activating mutations in the BRAF oncogene which encodes a type of RAF protein is known to play a role in the pathogenesis of a few cancers including colorectal, melanoma, breast, and endometrial cancer.7–9 Mutations in the BRAF gene have been found in low-grade ovarian serous carcinoma, in which it provides an alternative route for activating the RAS signaling pathway. 10 There is limited evidence about the presence of BRAF gene mutation in gynecological non-malignant disorders and the role of this mutation is still unclear.7,10,11
Therefore, in this study, the first objective was to evaluate the presence of two non-invasive and inexpensive biomarkers of KSI and BRAF mutation in patients with endometriosis of stage III and IV. The second objective was to assess and compare other common gynecological biomarkers in patients with recurrent disease and those without recurrence.
Materials & methods
This cross-sectional study was performed under the approval of the ethics committee of Tehran University of Medical Sciences (IR.TUMS.IKHC.REC.1399.094) on patients referring to Arash Women’s Hospital, Tehran University of Medical Sciences, Tehran, Iran during January 2019 and October 2020. The study population included all consecutive patients with stage III and IV endometriosis based on the revised American Fertility Society classification 12 who underwent laparoscopic surgery for endometriosis. Those patients who were treated medically and those who did not consent to participate in the study were excluded. The diagnosis of endometriosis was confirmed pathologically based on the specimen obtained during surgery.
The archived pathology slides which were previously stained with hematoxylin-eosin Figure 1 were obtained for reevaluation. In each case, the clearest block of endometrioma tissue was selected for immunohistochemical analysis Figure 2. For each case, new slices with 4–5 μm-thickness were cut and placed on poly-L-lysine-coated slides; then these tissue samples were kept at 58°C in an incubator for 30 min. The tissues were subjected to antigen-retrieval at 95°C for 20 min on a Dako PT Link Envision Flex-Target retrieval solution (50x) low pH liquid. The slides were then removed from the unit and incubated for 10 min in Envision Flex Washing buffer (20x). In the Dako Autostainer Link 48 automatic immunohistochemical staining device, sections were stained with Ki-67 (Clone MIB-1, Zeta Corporation, USA) antibodies which were prepared by dilution to 1/75. The slides were then passed through a series of alcohol-xylene for 2 min each. The Ki67 proliferation index was calculated by counting cells which showed nuclear staining in 500 epithelial cells using an ocular micrometer. All microscopies were carried out by two attending pathologists at Bahar Medical laboratory (Reference laboratory based in Tehran, Iran). In case of discrepancy in results, the third pathologist would take part and prepare the final report.
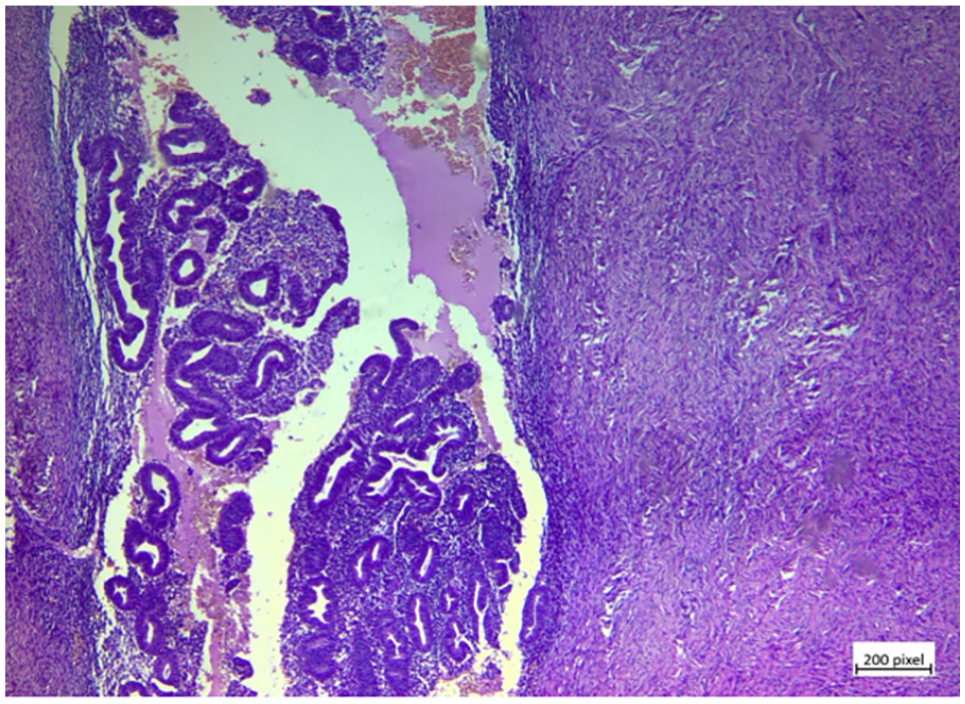
Histopathological image of endometriosis sample stained with hematoxylin-eosin (X100).
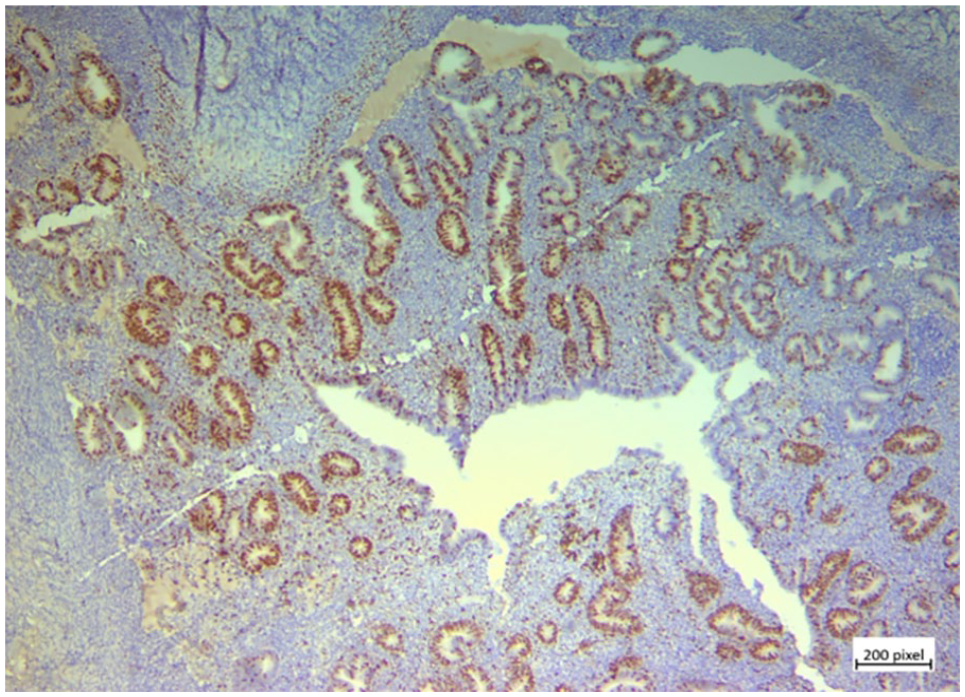
Histopathological image of endometriosis sample stained with Ki67 (X100).
Medical records were assessed to collect patients’ information including age, weight, height, parity, cyst size, and recurrence of the disease. Furthermore, tumor biomarker results including Cancer Antigen-125 (CA-125), Cancer Antigen 19-9 (CA19-9), Anti-Mullerian Hormone (AMH), and Alpha-FetoProtein (αFP) were extracted.
The cut-off values were set at 10% for KSI, 35 U/ml for CA-125, 37 U/ml for CA19-9, 1 ng/ml for AMH, and 10 ng/ml for αFP, as it was recommended in the user manual of the kits used. All patients were followed for at least 1 year in 3-month interval sessions, and were screened for the recurrence of clinical signs and symptoms. Also, patients who were highly suspicious of recurrent disease underwent abdominopelvic ultrasound imaging to confirm recurrence.
To investigate the presence of a mutation in the codon BRAF V600E gene, 10 μm slices of FFPE blocks were prepared and DNA was extracted using extraction columns (NucleoSpin DNA FFPE XS DNA, Macherey-Nagel, Germany). The quantity and quality of extracted DNA were checked by a Nanodrop spectrophotometer (Thermofisher, USA). The mutation status was evaluated using allele-specific Real-Time PCR method using MGB Taqman probes and Rotorgen Q device (QIAGEN, Germany).
Statistical analysis
All statistical analysis was performed using the SPSS software (SPSS software, version 20, Chicago, IL, USA). Descriptive analysis was reported considering the types of variables. The normality of variables was checked using the Kolmogorov-Smirnov test. Correlation between tumor markers was assessed by Pearson’s or Spearman’s correlation coefficient. Student’s t-test or Mann-Whitney U-test were used to compare means of tumor markers between patients with and without recurrence. A two-sided p-value less than 0.05 was considered significant.
Results
Table 1 shows the demographic characteristics and tumor markers of 50 patients who entered the study with stage III and IV endometriosis. Forty-one out of 50 (82%) patients had a non-recurrent disease and the other nine patients (18%) had recurrent disease. The mean ± SD of KSI for endometrium epithelia was 12.18 ± 16.58 (range: 2–70, median: 6.50). KSI ⩾ 10% was found in 20 patients (40%). The Kolmogorov-Smirnov test shows that the CA-125, CA19-9, and KSI were not normally distributed (all p-values < 0.05).
Patients’ characteristics of the study population (n = 50).
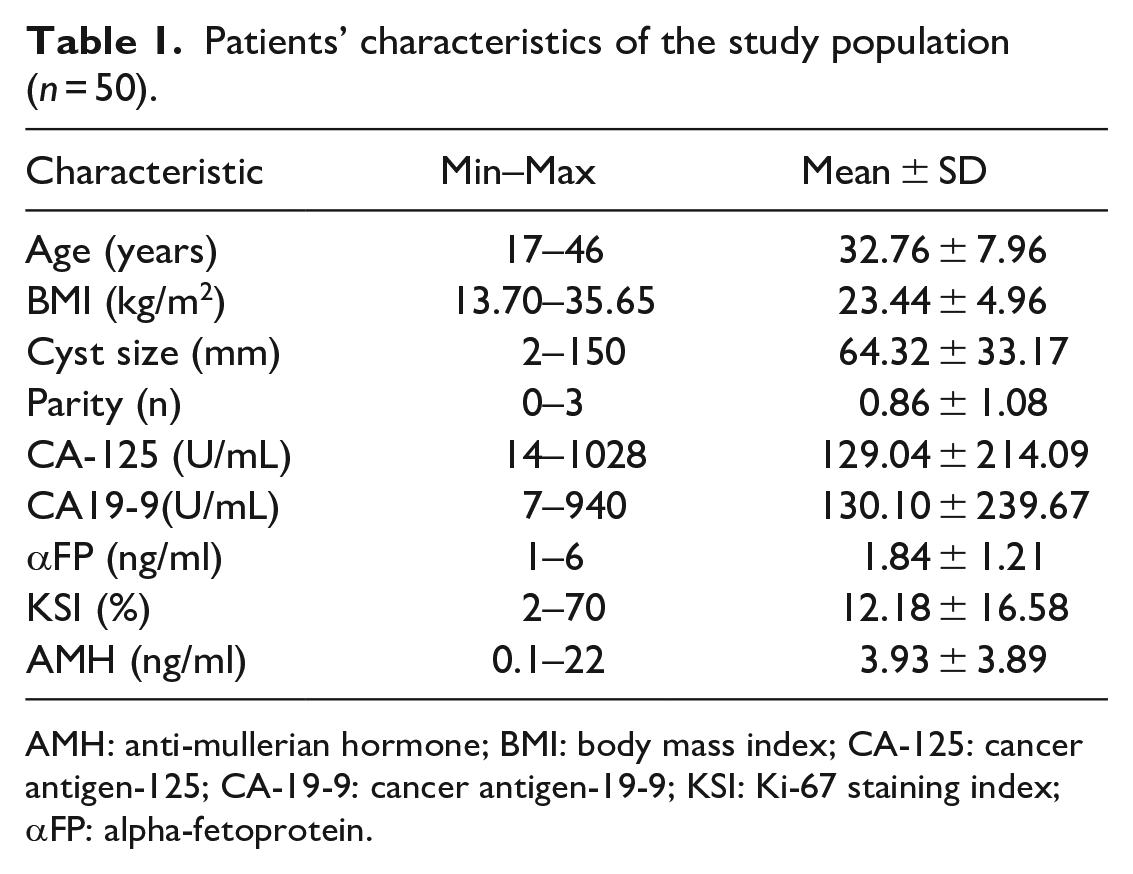
AMH: anti-mullerian hormone; BMI: body mass index; CA-125: cancer antigen-125; CA-19-9: cancer antigen-19-9; KSI: Ki-67 staining index; αFP: alpha-fetoprotein.
Table 2 demonstrates the distribution of biomarkers based on the cut-off value of abnormality. 58% of patients (n = 29) had higher than normal CA-125 levels. Also, serum CA19-9 level was increased in 26% of patients (n = 13). Since the majority of patients were young adults with mean ± SD for age of 32.76 ± 7.96 years, 66% of patients (n = 33) had normal AMH levels. αFP was not elevated in any of the studied cases.
Distribution of tumor biomarkers based on abnormality cut off value.
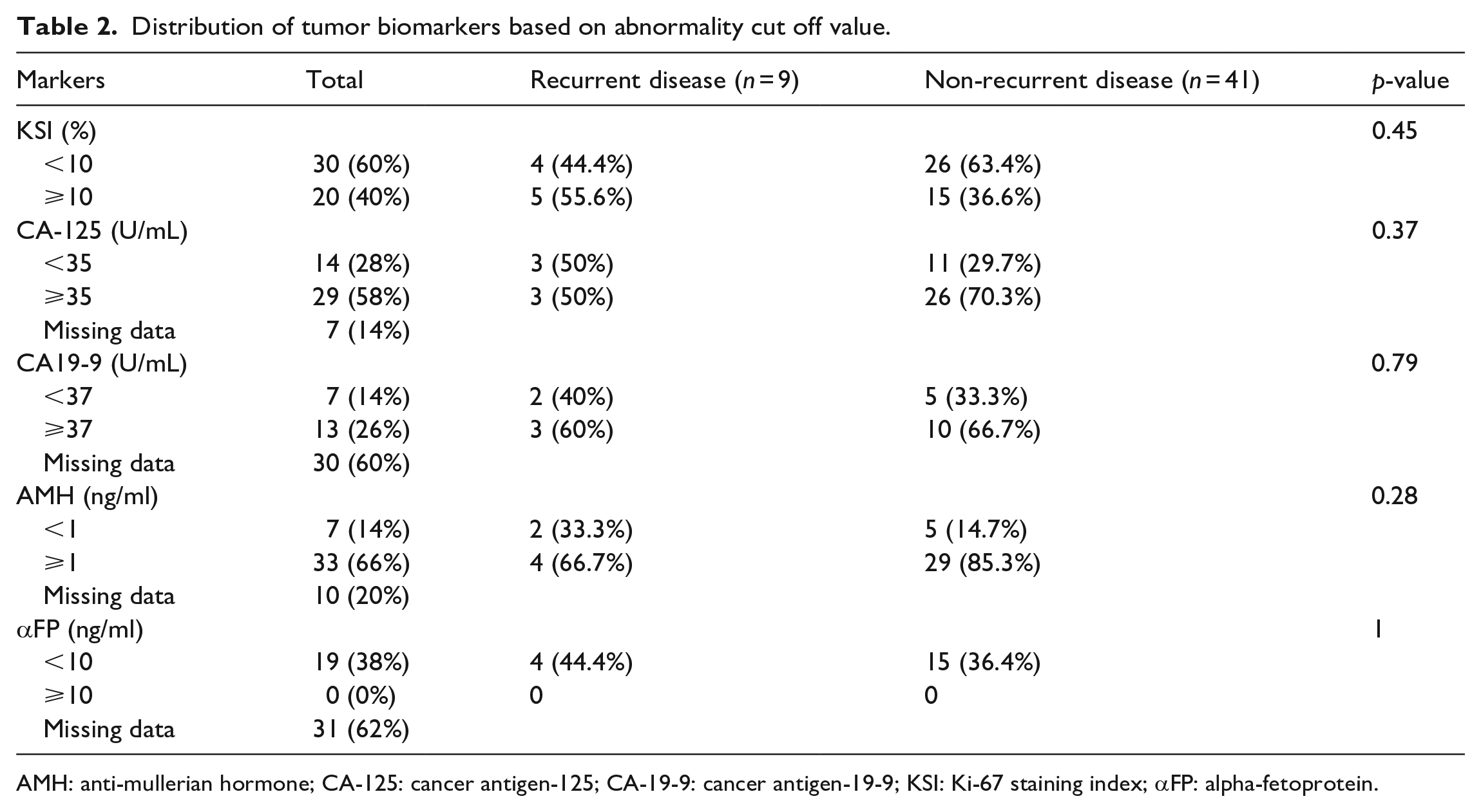
AMH: anti-mullerian hormone; CA-125: cancer antigen-125; CA-19-9: cancer antigen-19-9; KSI: Ki-67 staining index; αFP: alpha-fetoprotein.
No evidence of significant correlation was observed between the KSI and serum CA-125 (r = 0.01, p-value = 0.97) and serum CA19-9 (r = 0.07, p-value = 0.78). However, a positive correlation was observed between CA-125 and CA19-9 (r = 0.55, p-value = 0.02). Nevertheless, neither the serum level of CA-125 nor CA19-9 and KSI did show a significant correlation with tumor size (all p values > 0.05).
Table 3 compares the mean ± SD of study variables between patients who had recurrent disease and those who had not. As expected, the patients with recurrent disease were significantly older (p-value = 0.02) and more obese (p-value = 0.01) than patients with the non-recurrent disease. Mean KSI was insignificantly lower in recurrent patients compared with non-recurrent patients (9.78 ± 6.24 vs 12.71 ± 18.09, p-value = 0.33). Comparison of the other tumor markers (CA-125, CA-199, αFP, and AMH) between non-recurrent and recurrent groups did not show any statistically significant difference (all p values > 0.05). None of the samples harbored BRAF V600E mutation.
Comparison of mean ± SD of population characteristics.
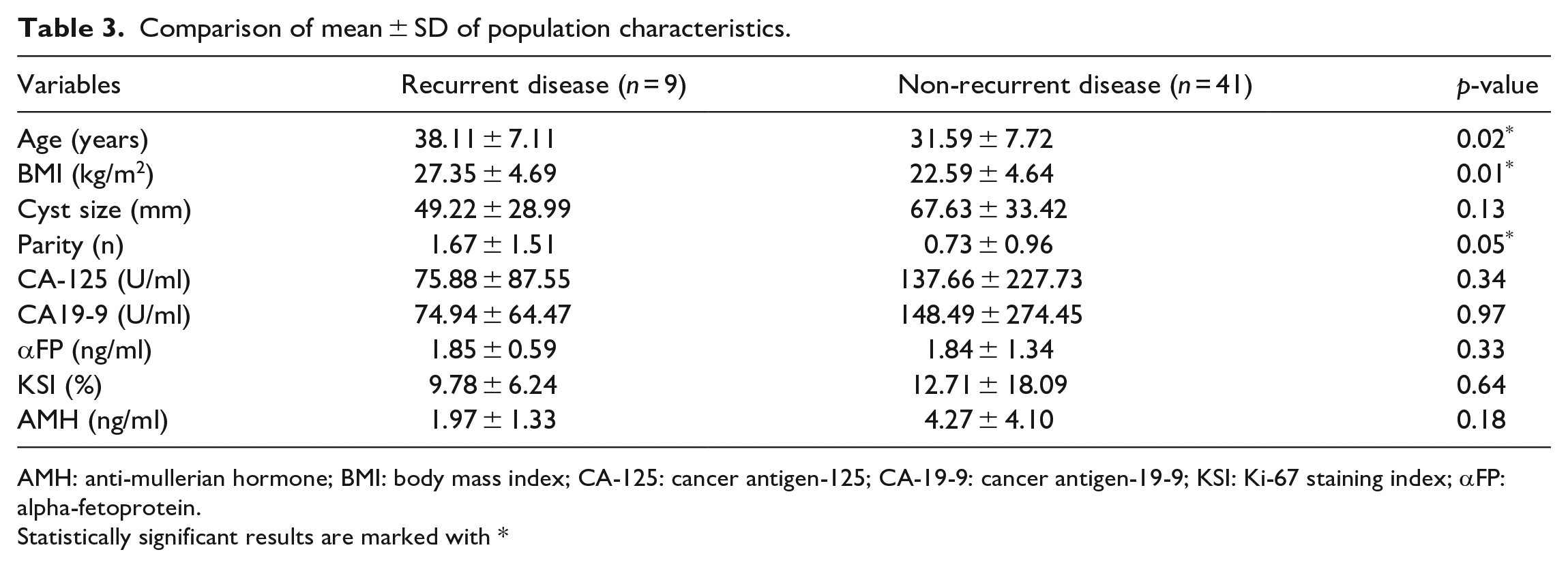
AMH: anti-mullerian hormone; BMI: body mass index; CA-125: cancer antigen-125; CA-19-9: cancer antigen-19-9; KSI: Ki-67 staining index; αFP: alpha-fetoprotein.
Statistically significant results are marked with *
Discussion
In the present study, KSI and the presence of BRAF mutation were evaluated in patients diagnosed with endometriosis of stage III and IV. Meanwhile, other tumor markers such as CA-125, CA19-9, αFP, and AMH were extracted from their medical records. We supposed the advanced endometriosis acts in a manner of a malignant process. It would, therefor be associated with a high index of proliferative activity and expression of higher levels of tumor markers, especially in patients with recurrent disease. In contrast, our results showed a higher level of KSI, CA-125, and CA19-9 in non-recurrent diseases. Differences in tumor marker levels between patients with recurrent disease and non-recurrent ones were not statistically significant.
However, higher levels of CA-125 (⩾35 U/ml) and CA19-9 (⩾37 U/ml) were revealed in non-recurrent endometriosis. These results may be due to the effect of medication taken by patients with recurrent disease, as it has been shown that danazol is associated with a reduction in CA-125 and CA19-9 levels. Furthermore, the effect of medication with danazol lasted even 3 months after cessation of treatment and the levels of antigens remained significantly low. 13
It should be considered while interpreting the results of the current study, that the small number of patients recruited in the recurrent disease group and our inability to control the probable effects of the medication on biomarker levels might have jeopardized the accuracy of the results. So, we cannot declare that endometriosis does not have an aggressive and malignant behavior.
Our study results were inconsistent with other studies that proposed a resemblance in the behavior of endometriosis and neoplastic processes.14–16 An investigation by Park et al. 15 showed that the endometrium of women with endometriosis has more proliferative activity based on increased expression of Ki-67, Bcl-2 proteins, and MTT assay results, compared with the control group. Another study conducted by Yalcin et al. evaluated different tumor markers, including Ki-67 and CA-125, in patients with recurrent and non-recurrent endometriosis and examined whether these factors could be considered as markers to predict recurrence. They found a positive relationship between serum levels of CA-125 and Ki-67 and the recurrence of endometriosis. 16 A cross-sectional study with 56 patients with stage III and IV endometriosis showed that Ki-67 expression was significantly associated with cyst size and stage of disease. 14 However, we could not find any correlation between cyst size and other tumor markers’ levels.
CA-125 marker is widely measured in gynecological malignancies including ovarian, tubal, endometrial, and cervical carcinomas. 17 It has been reported that the serum level of CA-125 is often elevated in endometriosis patients and the elevated level is correlated with the severity of the disease.18,19 In advanced endometriosis (stage III and IV) the elevated level of CA-125 was reported in 50%−100% of the study populations and in the present study, the percentage of cases above the cut-off value was 58%, which was consistent with previously reported studies.18,20
In our study, CA19-9 was measured in 20 patients and 13 patients (65%) had higher than normal serum levels of CA19-9. Few studies have reported an increased level of CA19-9 in patients with endometriosis.13,20 Since the CA-125 and CA19-9 were developed in different cancers, it seems the underlying mechanisms for the elevation of the serum level might be different. We found a positive correlation between CA-125 and CA19-9 (r = 0.55), which was confirmed in one study 21 and rejected by Toki et al. study. 20
The results of the current study were similar to several studies reporting no association between endometriosis and CA-125 and Ki-67.20,22–24 In a study conducted by Toki et al. they examined the relationship between CA-125 levels and epithelial cell proliferation rates in 45 patients with endometriosis of stage III and IV and reported no significant association between CA-125 level and Ki-67. These findings suggest that proliferative activated endometrial cells secrete significant amounts of CA-125, a factor that is an important marker for predicting recurrence in endometriosis. 21 The results of this study were confirmed by two other studies22,24 as well.
Another study looked at the Ki-67 in patients with endometrioma. The authors concluded that the index would increase as the disease progressed. They also showed that there was a relationship between CA-125 and Ki-67 and concluded that the Ki-67 could be used to predict the prognosis and to estimate the recurrence risk. 21
Scotti et al. utilized KSI to detect differences in proliferative activity between endometria and endometriotic lesions. Also, the presence of the adhesion complex E-cadherin was set as an indicator of dedifferentiation processes pointing to invasive properties of the uterine epithelium. Proliferation activity in uterine epithelium within the ectopic lesions was significantly reduced, but no difference was found between eutopic endometria of patients with and without endometriosis. Interestingly, the adhesion complex E-cadherin was slightly reduced in uterine epithelial cells of women with endometriosis and less expressed in endometriotic lesions. In conclusion, this study claimed that endometriotic lesions are not hyperproliferative, but exhibit properties of dedifferentiation and an invasive character. 25
RAS and RAF are proto-oncogenes controlling cell proliferation, transformation, differentiation, and apoptosis. 8 KRAS and BRAF gene mutations have been frequently detected in sporadic colorectal tumors. Different oncogenes provide cells with different transformation properties. BRAFV600E has greater potential in mediating tumor genesis effects than KRAS. 26 Despite the abundance of data on the role of BRAFV600E in gastrointestinal cancers, there are limited studies in gynecological cancers. According to our knowledge, there is no study on BRAF mutation status in endometriosis. In 2005, Feng et al. reported a 21% increase in BRAF mutations among 97 endometrial cancers (78 endometrioid and 19 non-endometrioid carcinomas). In addition, one of the nine cases of atypical endometrial hyperplasia had BRAF mutation. In this study, there was no clear difference between the prevalence of BRAF mutation among different stages of the disease, histological types, and different grades. 7
The main short-come of the present study is the limited number of participants and incomplete data around the level of tumor markers in the study population. It might have influenced the results and necessitates careful interpretation of them. However, the strength of this study is that we examined the whole population for BRAF mutation.
Conclusion
In conclusion, endometriosis manifests malignant behavior of rapid proliferation but the exact genetic alteration causing this phenomenon is not understood. It should be kept in mind that close follow-up of patients is mandatory to timely diagnosis of the recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.