
Abstract
Background:
Ovarian endometriosis cysts (OEC) are common chronic diseases occurring in women of reproductive age. Hormone therapy, including the use of oral contraceptives (COCs) and progestins, is widely employed in the treatment of endometriosis and OEC.
Objective:
This study aims to compare therapeutic effects of long-term daily use of dienogest (DNG, 2 mg) versus drospirenone (DRSP, 3 mg)/ethinyl estradiol (EE, 20 μg) daily on ovarian endometrial cysts, particularly focusing on cysts suppression.
Methods:
A retrospective analysis was conducted on 84 patients diagnosed with OEC, with 42 receiving DNG and 42 treated with DRSP/EE. After 6 months, assessments were made regarding pain symptoms, size of OEC, tumor markers, and adverse reactions.
Results:
After 6 months of treatment, both DNG and DRSP/EE effectively alleviated pain in patients with ovarian endometriotic cysts. DNG demonstrated more significant improvements than DRSP/EE in reducing tumor size, mainly in terms of higher drug efficacy and greater percentage of tumor shrinkage. However, DRSP/EE significantly reduced the expression of the tumor markers CA125 and CA199 in our study. Patients taking DNG had a higher likelihood of experiencing side effects than those on DRSP/EE, mainly vaginal bleeding and irregular menstrual periods.
Conclusions:
Both DNG and DRSP/EE are effective in treating ovarian endometrial cysts. DNG appears to be superior in terms of tumor reduction, while DRSP/EE more significantly decreases the expression of the tumor markers and has fewer side effects.
Keywords
Introduction
Ovarian endometriosis cysts (OEC) represent a chronic estrogen-dependent disorder that affects approximately 10% of women of reproductive age globally, with the peak incidence typically observed during gestational age. 1 The characteristic feature of endometriosis involves the development of endometrial lesions in ovaries. 2 OEC poses potential risks to women, including infertility, pain, and possible malignant transformation.
Symptoms commonly experienced by women with OEC encompass dysmenorrhea, premenstrual pain, dyspareunia, and chronic fatigue, significantly impacting patients’ quality of life, fertility, and emotional well-being.3,4 Studies have indicated that women with OEC often report decreased work efficiency attributed to reduced productivity in the presence of pelvic pain. 5 Moreover, it was documented that individuals with OEC suffer from depression and anxiety, with anxiety severity showing correlation with pain intensity. 6
In recent years, tumor markers have emerged as potential diagnostic tools for OEC, such as carbohydrate antigen 125 and 19-9 (CA125 and CA199),7,8 human epididymis protein 4 (HE4), 9 carcinoembryonic antigen (CEA), 10 and alpha-fetoprotein (AFP). 11 However, these markers exhibit low diagnostic specificity and sensitivity, as elevated concentrations can be found in malignancies of various origins including non-ovarian gynecological cancer.12,13 Nevertheless, combining use of these markers has shown improved sensitivity and specificity in OEC diagnosis, presenting a promising adjunctive approach for the early detection of OEC.14,15
The primary goals of treating ovarian endometrial cysts involve pain relief, fertility enhancement, reduction of endometrial lesions, and improvement in patients’ quality of life. 16 Hormone therapy is one of the common treatment options for OEC, encompassing the use of oral contraceptives and progestogen-only pills. 17 These treatments work by regulating hormone levels and can alleviate the severity of pain and prevent the progression of OEC. Surgery intervention may be necessary when medication fails to provide relief or when severe damage is caused by OEC. In comparison to drug therapy, surgery is invasive, costly, and carries a risk of recurrence. 18
Combined oral contraceptives (COC), considered the first-line medical option, have been extensively studied and consistently demonstrated to be safe, well-tolerated, cost-effective, and effective in the long-term treatment of endometriosis.19,20 Drospirenone (DRSP)/ethinyl estradiol (EE) are recognized for possessing properties akin to natural progesterone, including anti-androgenic activities and anti-mineralocorticoid effects. 21 DRSP blocks the mineralocorticoid receptor to offset EE-related water and sodium retention. Clinical experience has shown that a common issue with long-term continuous oral contraceptive regimens is breakthrough bleeding, and an increased risk of venous and arterial thrombosis. 22 Dienogest (DNG) is regarded as an alternative for managing endometriosis symptoms, exerting a localized effect on endometriotic lesions with minimal hormonal activity and metabolic impact.23,24 Although research indicates DNG’s effectiveness in endometriosis therapy, side effects like vaginal bleeding, headache, breast pain, and weight gain have been reported. 25 Previous studies comparing Dienogest with COC have demonstrated their efficacy in reducing endometriosis-related discomfort and enhancing quality of life in women with severe endometriosis.26,27
However, there exists a scarcity of comparative studies on the efficacy of dienogest versus drospirenone/ethinyl estradiol in treating ovarian endometrial cysts and tumor markers. This study aims to compare the effectiveness of DNG and DRSP/EE in terms of pain relief and side effects among patients with ovarian endometriosis cysts, with a specific focus on evaluating their inhibitory effects on cyst volume and tumor marker expression.
Materials and methods
Patients
To determine the effects of dienogest and drospirone/ethinyl estradiol on women with ovarian endometriosis cysts, a retrospective analysis was conducted at Xiamen Women and Children’s Hospital (XWCH). This study was approved by research ethics committee (REC) of Xiamen Women and Children’s Hospital in accordance with the World Medical Association Declaration of Helsinki.
Patient data were collected from the period between January 2020 and June 2023 for individuals with endometriosis and ovarian endometrial cysts based on ultrasonography imaging. 28 Inclusion criteria comprised females aged 18–45 years with a clinical diagnosis of ovarian endometriosis cysts, while exclusion criteria included menopause, hormone therapy contraindications, chronic diseases or metabolic disorders, and pregnancy preparation. A total of 84 patients participated in this retrospective analysis, with 42 receiving Dienogest (DNG, 2 mg) treatment and 42 receiving drospirenone (DRSP, 3 mg)/ethinyl estradiol (EE, 20 μg) treatment using a 24/4 regimen.
Data analysis
Baseline information such as age, BMI, childbearing history, and treatment history of patients in both groups was collected for initial analysis.
Pain intensity was measured by a 10-point Visual Analog Scale (VAS score) consisting of a 10-cm line with 0 representing no pain and 10 representing the worst possible pain. The scores were recorded before and after the treatment period. Accompanying symptoms and side effects were documented through a specialized questionnaire.
Transvaginal pelvic ultrasound scanning (TVUS) was performed by the same operator before and after treatment to evaluate the presence and size of OEC. Cyst volumes were calculated using the prolate ellipsoid formula: (pi/6 × a × b 2 ), where a and b represented the maximum diameter in the transverse and longitudinal axes. Tumor marker quantification was conducted for absolute measurement.
Adverse reactions during treatment, such as vaginal bleeding, headache, breast tenderness, insomnia, irregular menstrual periods, and skin itching, were recorded, and the occurrence percentage was counted.
Statistical analyses were performed using IBM SPSS version 24.0 software (IBM Corp., Armonk, NY, USA). Descriptive analyses were used to determine average values and standard error of mean (SEM) of patients’ characteristics. Matched samples t-test (normally distributed) or Mann-Whitney U test (Wilcoxon rank sum test; non-normally distributed) were conducted to compare differences between the two treatment groups. Data are presented as mean ± SEM. A difference of p-value <0.05 was deemed as statistically significant, and p value was also provided in table notes for reference.
Results
Basic clinical information of OEC patients
Comparing patients’ initial clinical information in clinical research is crucial to ensure that subsequent comparative analyses are not influenced by confounding factors, thereby enabling more accurate and reliable comparisons between different groups or interventions. This helps control for variables that could introduce bias or affect results interpretation. Our results showed that patients in the DNG and DRSP/EE groups were comparable in age, BMI, reproductive history, previous treatments, surgical history, and clinical condition. There were no statistically significant differences between the two groups at baseline (Table 1).
Comparison of general characteristics at baseline between DNG and DRSP/EE group.
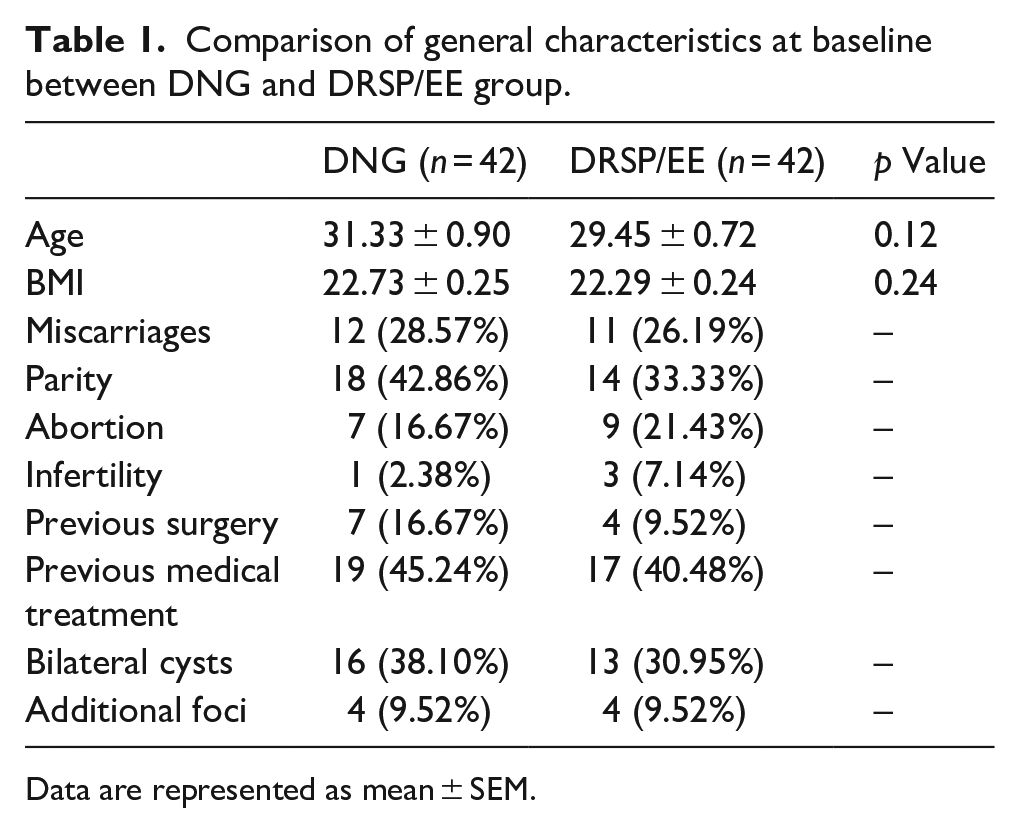
Data are represented as mean ± SEM.
Pain relief
Ovarian endometrial cysts are commonly found with associated symptoms of chronic pelvic pain.29,30 Chronic pain was recorded before treatment in 17 patients of DNG group and 20 patients of DRSP/EE treatment group. The remaining patients were either asymptomatic or below the VAS cutoff used in this study. Symptomatic patients were reassessed with the VAS after 6 months treatment. Significant improvements were observed in both two treatments. In the Dienogest group, the average VAS score decreased from 2.83 at baseline to 0.33 after 6 months of treatment, indicating an elimination of pain symptoms. Similarly, in the drospirenone/ethinyl estradiol group, the average VAS score decreased from 2.75 at baseline to 0.20 after 6 months of treatment, indicating an overall reduction in pain intensity (Table 2).
VAS changes after DNG or DRSP/EE treatment for 6 months.
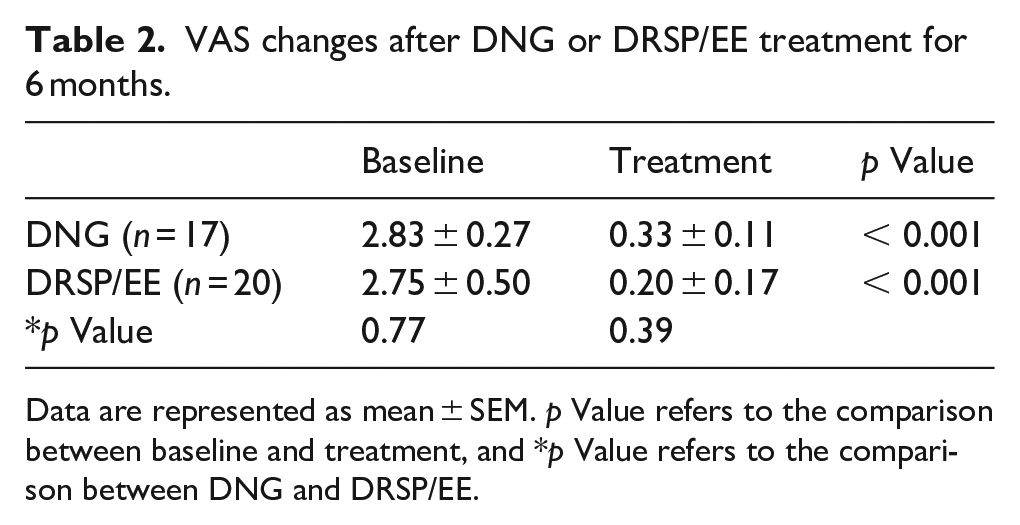
Data are represented as mean ± SEM. p Value refers to the comparison between baseline and treatment, and *p Value refers to the comparison between DNG and DRSP/EE.
Cyst size changes
The reduction in cyst size was assessed through transvaginal pelvic ultrasound scanning before and after the treatment period. Cyst volumes were calculated using obtained transverse and longitudinal axes. Among the patients treated with DNG, 36 out of 42 were effective (85.7%), while only 28 out of 42 showed a positive response in the DRSP/EE group (66.7%), indicating a lower effectiveness in reducing cyst size compared to DNG. Furthermore, the relative volumes of cysts before and after medication were analyzed among the effective patients. The cyst size in the DNG-positive response group significantly decreased to 39.80% of the pre-medication size, while it was 56.30% for DRSP/EE (Table 3).
Comparison of cyst volume changes under treatment of DNG or DRSP/EE for 6 months.
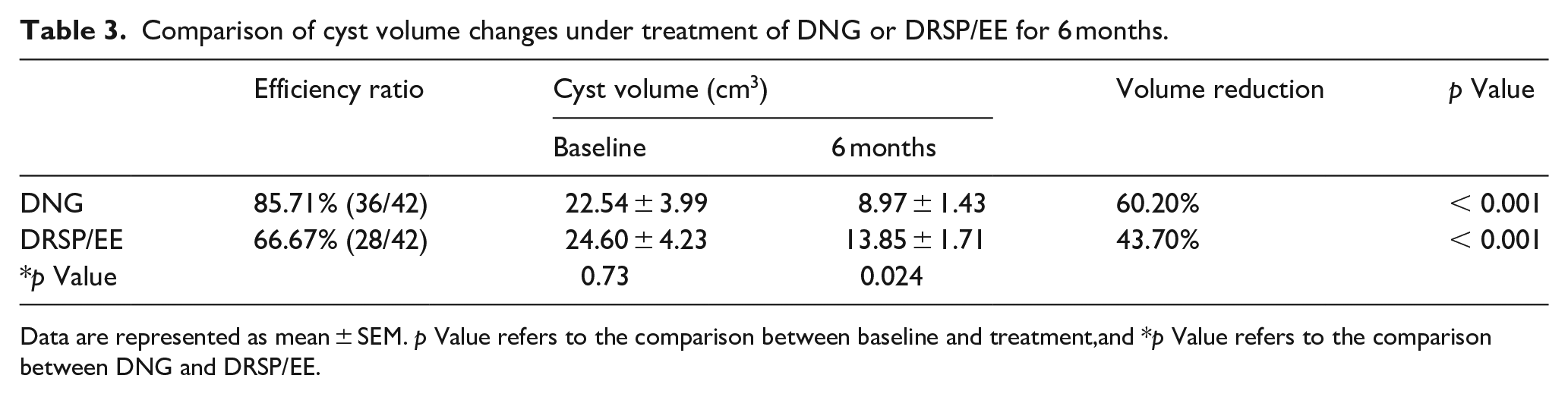
Data are represented as mean ± SEM. p Value refers to the comparison between baseline and treatment,and *p Value refers to the comparison between DNG and DRSP/EE.
Tumor markers
Several tumor-related markers, including cancer antigen 125 (CA125), cancer antigen 129 (CA199), and human epididymal secretory protein 4 (HE4), were identified in the blood serum of patients with ovarian endometriotic cysts. To further compare the effectiveness of DNG and DRSP/EE, laboratory information on tumor markers, including CA125, CA199, HE4, AFP, and CEA, was collected from patients with ovarian endometriotic cysts. A significant proportion of patients with OEC exhibited elevated levels of CA125 and CA199, while no remarkable changes were observed in the other three markers, HE4, AFP, and CEA.
The therapeutic effects of DNG and DRSP/EE were compared based on their ability to lower CA125 and CA199 levels. Interestingly, DRSP/EE demonstrated superior efficacy in reducing the levels of CA125 and CA199 compared to Dienogest. After 6 months of treatment with DNG, a considerable proportion of patients still exhibited little to no improvement in terms of their CA125 and CA199 levels (30.4% and 20% respectively). Furthermore, for those patients who did exhibit reductions in these markers, a higher percentage of DRSP/EE-treated patients returned to normal levels than DNG (52.6% vs 26.1% in CA125, 100% vs 40% in CA199; Table 4). The effect of these two drugs on tumor marker reduction was not consistent with their results in reducing cyst size, which may be due to their different rationale for treating OEC.
Tumor markers changes after DNG or DRSP/EE treatment for 6 months.
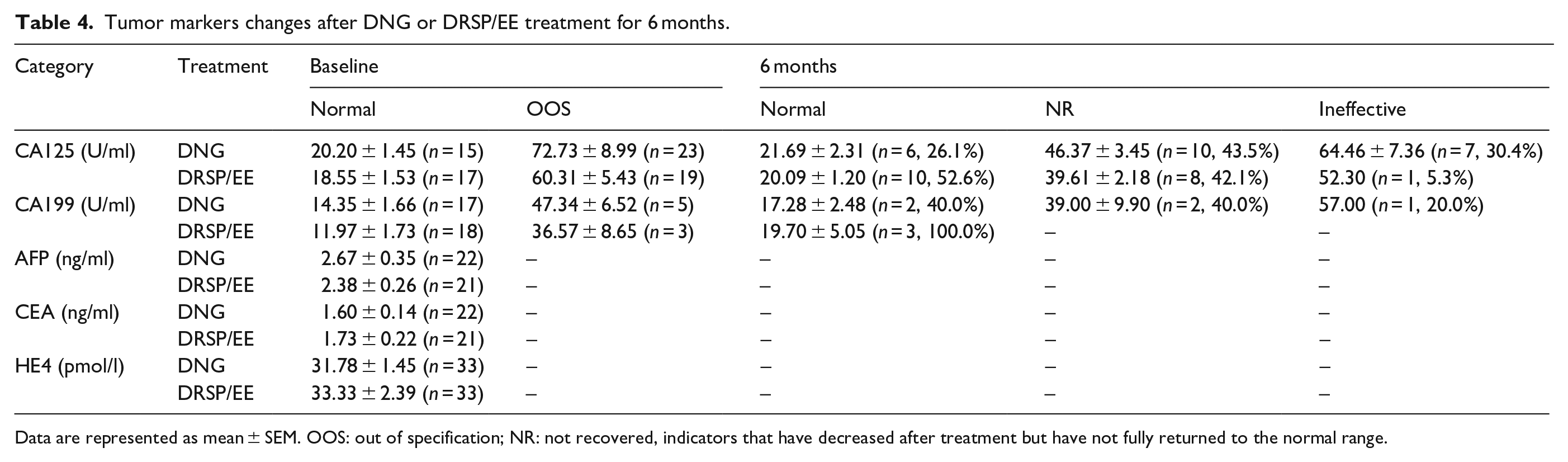
Data are represented as mean ± SEM. OOS: out of specification; NR: not recovered, indicators that have decreased after treatment but have not fully returned to the normal range.
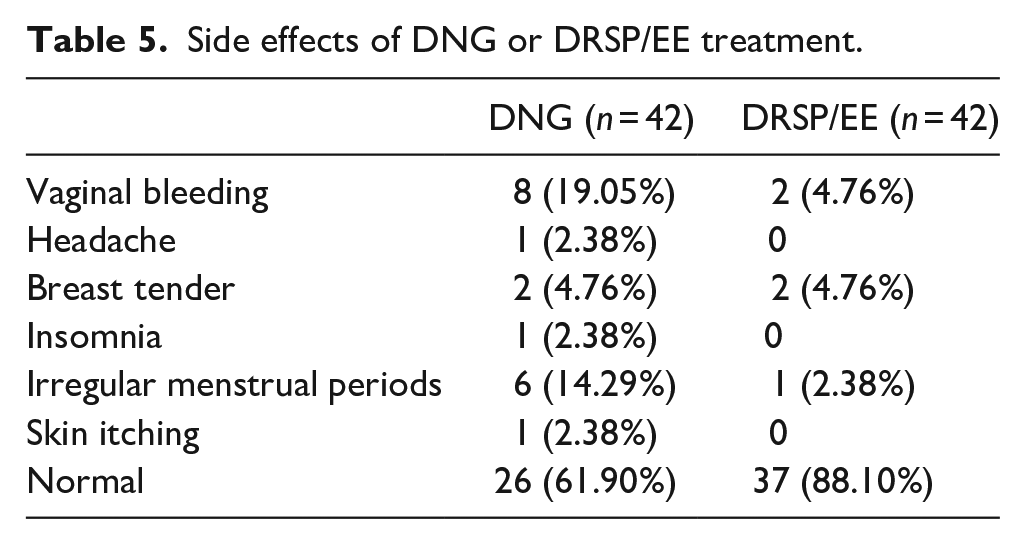
Side effects
An evaluation of the side effects of DNG and DRSP/EE was performed to assess their safety profiles and tolerability. The results revealed a higher proportion of patients (88.1%) in the DRSP/EE group who did not experience any side effects compared to the DNG group (61.9%). Specifically, in the DRSP/EE group, patients who took the medication for 6 months reported only occasional occurrences of vaginal bleeding, breast tenderness, and irregular menstrual cycles. In contrast, a significant proportion of patients in the DNG group reported vaginal bleeding and irregular menstrual cycles, along with occasional occurrences of headaches, breast tenderness, insomnia, and skin itching (Table 5). The side effects observed in the DRSP/EE group were relatively mild and occurred infrequently, whereas the DNG group had a higher incidence of side effects.
Side effects of DNG or DRSP/EE treatment.
Discussion
Many patients seek medical attention for ovarian endometriosis cysts primarily due to the presence of physical discomfort, with pain relief being their main concern. Researchers conducted studies on the pain relief effects of hormonal treatments, such as DNG and DRSP/EE.26,27,31 These studies indicate that DNG and COC have similar effects in pain relief, which is also supported by our data.
Regarding the occurrence of side effects, Lina El Taha’s study shows that DNG (2 mg) was associated with fewer side-effects than COC (YASMIN, 3 mg DRSP, and 30 μg EE). 32 In our study, DNG was found to have a higher incidence of adverse effects, such as vaginal bleeding and irregular menstrual cycles, compared to COC (YAZ, 3 mg DRSP, and 20 μg EE). This difference might be due to the different doses of EE used, as previous researches have shown that low-dose EE can reduce bleeding and cardiovascular side effects,33,34 although this conclusion is still controversial. Full disclosure of potential side effects, including vaginal bleeding, is essential for patients to make informed decisions about their treatment options. It is also vital to stress that the occurrence of side effects does not necessarily indicate the failure of the treatment. Such disclosure also helps to manage patients’ expectations and prepare them psychologically for any potential adverse effects. Patients should be encouraged to continue with the prescribed medication unless advised by their healthcare provider.
Our findings demonstrated variations in the treatment effects of the two medications on cysts. DNG exhibited better outcomes in reducing cyst size, whereas DRSP/EE showed superior effectiveness in decreasing tumor markers associated with the cysts. For patients, the size of the cysts is often a primary concern as it is closely associated with their symptoms. Small cysts may not manifest noticeable symptoms, while large cysts can lead to severe issues such as pain, irregular menstruation, pelvic pressure, and infertility. Therefore, the differential effects of DNG and DRSP/EE in reducing volume of ovarian endometriomas cysts may influence patients’ choices. It is also important to note that according to ESHRE guidelines, 35 tumor markers are generally not suggested for routine monitoring of ovarian endometriomas. Therefore, caution should be exercised in interpreting these conclusions, and further research is needed to explore the significance of these drugs in preventing malignant transformations.
Our results indicate that DNG and DRSP/EE are associated with approximately 14% and 33% of patients experiencing ineffectiveness along with certain side effects. This suggests that while conservative treatment plays a crucial role in the management of ovarian endometriomas, surgical intervention may be necessary in certain circumstances. 36 Among different surgical techniques, stripping is still considered the preferred procedure due to its lower recurrence rate compared to ablative techniques.37,38 New surgical technologies, such as CO2 fiber laser technique, 39 are purported to aid in ovarian preservation, maintaining pregnancy rates, and ensuring success in in vitro fertilization (IVF); however, further clinical data are needed to substantiate these claims. Physicians should select the appropriate treatment method based on patient preferences and the severity of the condition to achieve the best therapeutic outcomes.
When making clinical decisions, physicians prioritize patient considerations, including the ability to relieve symptoms and the cost of the medication. The high cost of DNG, which is typically three to four times higher than that of DRSP/EE, may have a negative impact on the promotion and adoption of this medication, as it poses financial challenges for patients.
In conclusion, our findings provide valuable insights into the comparative effects of DNG and DRSP/EE in the treatment of ovarian endometriotic cysts. Both medications demonstrated efficacy in pain relief, and DNG showed better results in reducing cyst size, while DRSP/EE exhibited superior effectiveness in reducing tumor markers associated with the cysts. These results could help in selecting the appropriate drug for better treatment outcomes, avoiding surgery, and preserving fertility.
However, it is important to acknowledge the limitations of our study, including the limited number of cases and treatment duration. Furthermore, being a retrospective study, it may introduce biases such as selection and information biases. Thus, further prospective cohort or randomized controlled studies with a larger sample size and long-term follow-up are needed to validate these results and gain a more comprehensive understanding of the clinical performance of these medications for ovarian endometriosis cysts.
Footnotes
Acknowledgements
Not applicable.
Author contributions
HL designed the research study. QX collected the data. QX, LH, and CL performed the analysis together. LH wrote the manuscript. SJ contributed to the revision of the manuscript. All authors contributed to editorial changes in the manuscript and interpreting data. All authors read and approved the final manuscript. QX, LH, CL, and SH have contributed equally to this work.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Xiamen Municipal Healthcare Guiding Project to Hongli Liu, grant number 3502Z20214ZD1230.
Ethical approval and consent to participate
This study was approved by Research Ethics Committee (REC) of Xiamen Women and Children’s Hospital. Written informed consent was obtained from a legally authorized representative for anonymised patient information to be published in this article.