
Abstract
Introduction:
Irritable Bowel Syndrome (IBS) is a prevalent digestive disorder characterized by abdominal pain and changes in bowel movements without any structural disorders. The present study aims to explore the impact of group Cognitive Behavioral Therapy (CBT) on resilience, functional anxiety, and the severity of IBS symptoms in patients from Hamadan, Iran.
Methods:
This study employed a semi-experimental, pre-test-post-test design with a control group. The participants were patients diagnosed with IBS referred to the gastroenterology clinic at Ibn Sina Hospital in Hamedan, Iran. A total of 40 patients were selected through simple random sampling and divided into experimental and control groups. The intervention consisted of CBT, based on the framework by Leahy et al. To measure the outcomes, this study used the Connor-Davidson Resilience Scale (CD-RISC) (2003), the Zung Self-Rating Anxiety Scale (SAS) (1970), and the Irritable Bowel Syndrome Severity Score (IBSSS). After completing the intervention, this research administered a post-test to both groups using the same questionnaires.
Results:
The study utilized multivariate and univariate covariance analyses to examine the data and test the research hypotheses. The results revealed that group CBT sessions led to notable differences between the experimental and control groups. Specifically, the subjects in the experimental group showed a significant reduction in functional anxiety, a decrease in the severity of IBS, and an increase in resilience compared to the control group.
Conclusion:
The results indicate that group CBT significantly reduces functional anxiety and the severity of IBS symptoms while boosting resilience.
Keywords
Introduction
Irritable bowel syndrome (IBS) is a common functional gastrointestinal disorder characterized by recurrent abdominal pain and altered bowel movements in the absence of identifiable structural abnormalities. 1 According to the Rome IV criteria, IBS symptoms are classified into constipation-predominant, diarrhea-predominant, or mixed types. For diagnosis, these symptoms must occur at least three days per month and have started at least 3 months prior to diagnosis. 2 Given the chronic nature of IBS, treatment goals have shifted from merely controlling symptoms to enhancing the quality of life (QoL) by reducing the disease’s impact on daily functioning.
The clinical presentation of IBS varies widely in both frequency and severity and may significantly impair daily functioning. Similar to other functional gastrointestinal disorders, psychological factors and the brain–gut axis play a pivotal role in the onset and progression of symptoms. In patients without substantial psychological distress and with adequate social support, minimal lifestyle and dietary adjustments combined with physician reassurance may be sufficient for symptom control. 3 In contrast, even mild gastrointestinal disturbances can persist in those with heightened psychological stress and inadequate support networks. 4 IBS frequently follows a cyclical course, with alternating periods of relapse and remission, accounting for approximately %50–%25 of gastroenterology referrals. 5 The prevalence of IBS is higher among women, and psychological and psychiatric factors can influence its onset, severity, and prognosis. 5
Recent evidence indicates that psychological symptoms—particularly anxiety—are highly prevalent among individuals with chronic pain. 6 Anxiety disorders are among the most prevalent psychiatric conditions across the lifespan. 7 Anxiety is a persistent feeling of unease accompanied by physical symptoms that, if untreated, may lead to further psychological problems. 8 IBS patients often present with functional anxiety and psychological distress, while individuals with anxiety or panic disorders frequently experience IBS-like gastrointestinal symptoms, suggesting a bidirectional relationship between psychological status and IBS progression. 9
Beyond anxiety, IBS can impair resilience—the capacity to adapt constructively to ongoing life challenges. Higher resilience has been linked to better coping strategies, improved pain tolerance, and reduced symptom catastrophizing, whereas prolonged illness duration may erode resilience, heightening susceptibility to maladaptive psychological responses and comorbid depression.5,10
Symptom severity in irritable bowel syndrome (IBS) encompasses the intensity, frequency, and duration of hallmark gastrointestinal complaints, commonly assessed using validated instruments such as the Irritable Bowel Syndrome Severity Scoring System (IBS‑SSS), which captures the combined physical, emotional, and functional burden of the disorder. 11 Over time, IBS management has incorporated pharmacological, biological, psychological, and social interventions, reflecting its multifactorial pathophysiology and impact on patients’ quality of life. 12 Given the impact of central nervous system dysregulation on psychosocial functioning in IBS, 13 combined pharmacological and psychological interventions are often beneficial. Cognitive behavioral therapy (CBT), a structured, time‑limited approach targeting maladaptive thoughts and behaviors, has demonstrated efficacy in improving gastrointestinal symptoms and related distress. 14
CBT applies cognitive strategies (identifying and restructuring distorted thoughts, building effective self‑talk) and behavioral strategies (exposure, relaxation training, and problem-solving). It also reinforces self‑control and self‑efficacy, thereby reducing anxiety, improving coping skills, and potentially decreasing symptom severity. 14
Recent research supports CBT’s efficacy in reducing anxiety and enhancing resilience.14–17 Limited evidence is available on the impact of group cognitive behavioral therapy (CBT) on resilience and functional anxiety in patients with irritable bowel syndrome (IBS). IBS is a global research priority due to its high prevalence and substantial quality‑of‑life burden. Given the side effects and costs of pharmacological treatments, demand is growing for effective, low‑risk, and accessible approaches. IBS symptoms, functional anxiety, and resilience are closely interconnected: anxiety may exacerbate gastrointestinal symptoms via increased visceral sensitivity and altered motility, while severe symptoms can diminish resilience by eroding coping confidence. Conversely, enhancing resilience may protect against stress‑induced symptom worsening and improve quality of life. Group CBT addresses these dynamics by modifying maladaptive thoughts and promoting adaptive behaviors through structured sessions incorporating cognitive restructuring, exposure, relaxation training, and problem‑solving. The present study investigates whether group CBT can improve resilience, decrease functional anxiety, and reduce IBS symptom severity.
Materials and methods
Study design and participants
This study employed a quasi‑experimental pre‑test–post‑test design with a control group. Participants were outpatients diagnosed with irritable bowel syndrome (IBS) according to the Rome IV diagnostic criteria 1 at the Ibn Sina Hospital gastroenterology clinic in Hamadan, Iran, during 2023. Forty eligible individuals were recruited using purposive sampling and then randomly allocated, via a random‑number table, to either the intervention group (n = 20) or the control group (n = 20).
Sampling procedure and inclusion/exclusion criteria
The sample size was determined based on previous studies on cognitive behavioral therapy and resilience, 18 with statistical power set at 0.80 and significance level at 0.05, resulting in a minimum of 18 participants per group. To increase robustness, 20 participants were assigned to each group. Purposive sampling was first used to recruit participants meeting the diagnostic and demographic criteria, followed by simple random allocation using random numbers to ensure group comparability.
Inclusion criteria: Age 25–45 years (to reduce variability in psychological treatment response), at least a middle school education (to ensure comprehension of intervention materials), diagnosis of IBS with moderate to severe symptoms, no concurrent psychological treatment, and a Connor–Davidson Resilience Scale (CD‑RISC) score of 50 or below.
Exclusion criteria: Receiving any other psychological or medical treatments for IBS during the study period, absence from more than two intervention sessions, withdrawal of consent, or presence of psychiatric comorbidities requiring additional interventions.
Instruments
Connor–Davidson Resilience Scale (CD-RISC)—This 25-item scale assesses resilience on a five-point Likert scale (0–4), with higher scores indicating greater resilience. The original version demonstrated good internal consistency (Cronbach’s α = 0.84), 19 and the Persian adaptation has shown acceptable reliability and validity (α = 0.89). 20
Zung Self-Rating Anxiety Scale (SAS)—This 20-item self-report inventory evaluates somatic and psychological anxiety symptoms on a four-point Likert scale. Higher scores indicate greater anxiety severity. Internal consistency in the original study was α = 0.84 21 ; the Persian version has also demonstrated satisfactory psychometric properties. 22
Bowel Symptoms Severity–Frequency Scale—This 10‑item instrument assesses the severity and frequency of bowel symptoms using a five‑point Likert scale (1–5). Higher scores reflect greater symptom severity. The scale was originally developed and psychometrically evaluated in patients with irritable bowel syndrome by Haghayegh et al., reporting an internal consistency coefficient of α = 0.70 . The Persian version was subsequently validated in an Iranian population, demonstrating acceptable reliability and validity. 23
Intervention design
The CBT program was developed based on the theoretical framework described by Leahy et al. 24 The intervention comprised eight weekly group sessions, each lasting 90 min, conducted over a 2‑month period. Core components included cognitive restructuring, problem‑solving training, relaxation techniques, and graded exposure to anxiety hierarchies.
Detailed session content is presented in Table 1, covering participant familiarization, introduction to anxiety and resilience concepts, identification of cognitive distortions, and evidence‑based cognitive challenges. The group format was selected for its efficiency, capacity to provide peer support, and cost‑effectiveness in clinical practice. Participants in the control group received no psychological intervention during the study period.
Summary of group CBT treatment sessions for patients with irritable bowel syndrome.
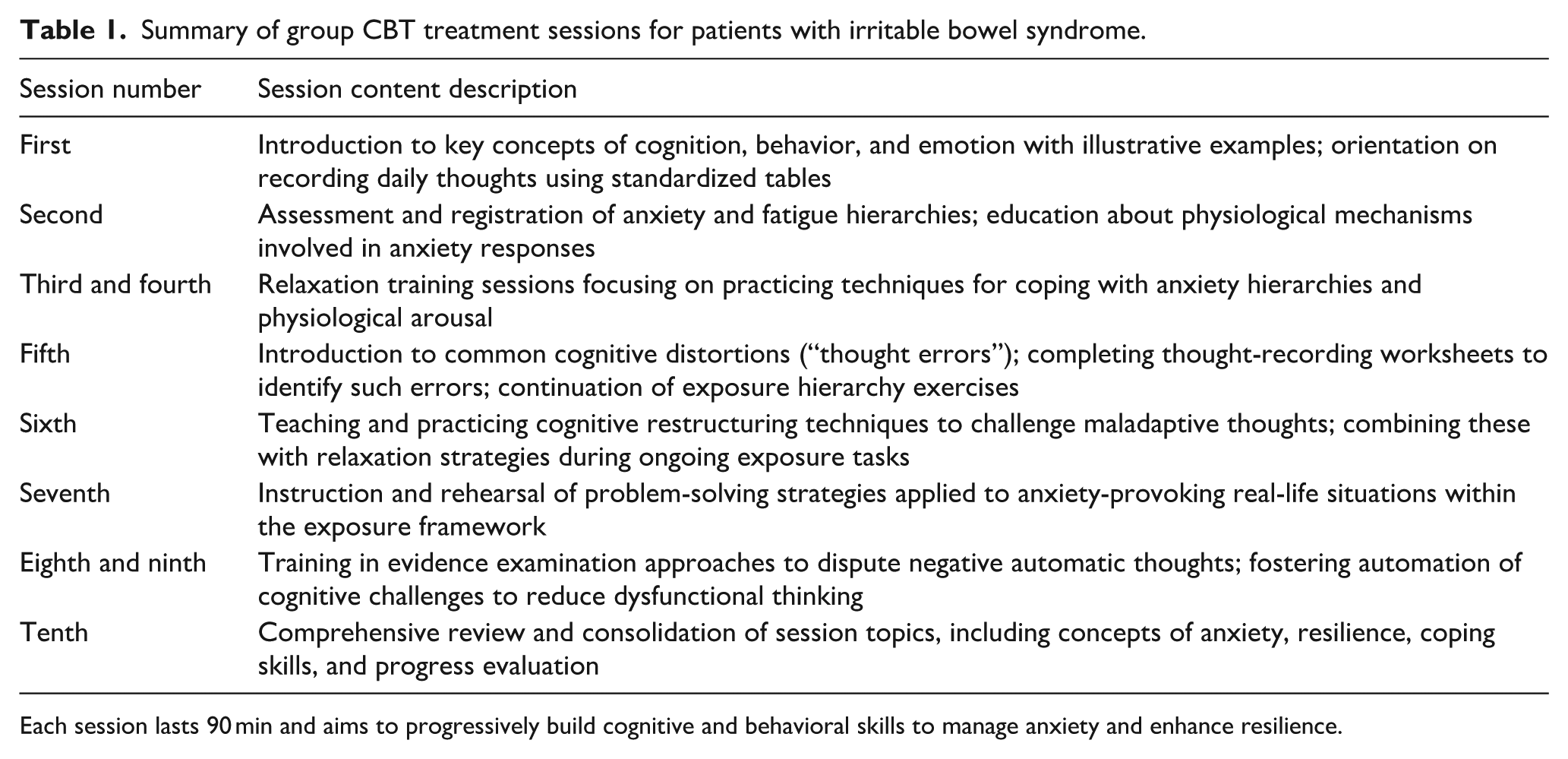
Each session lasts 90 min and aims to progressively build cognitive and behavioral skills to manage anxiety and enhance resilience.
Control of time effects
To control for potential temporal influences on outcomes such as resilience, both the experimental and control groups completed the pre‑test and post‑test assessments within the same 2‑month period. The control group did not receive any intervention during this time, ensuring that any observed changes in the experimental group were attributable to the CBT program rather than seasonal variations or other time‑related factors.
Ethical considerations and data analysis
Ethical approval for the study was obtained from the Islamic Azad University Research Ethics Committee (approval code: IR.IAU.H.REC.1402.079). All participants provided written informed consent prior to enrollment. Data were analyzed using IBM SPSS Statistics, version 25 (IBM Corp., Armonk, NY, USA). Descriptive statistics (means and standard deviations) were calculated, and inferential analyses were conducted using multivariate analysis of covariance (MANCOVA) and analysis of covariance (ANCOVA). The level of statistical significance was set at p < 0.05.
This study employed descriptive statistical methods, including measures of central tendency and dispersion, alongside inferential analyses such as multivariate analysis of covariance (MANCOVA) and univariate analysis of covariance (ANCOVA) to examine data collected from the questionnaires. Statistical analyses were performed using IBM SPSS Statistics version 25.
Results
Of the 40 participants included in the study, educational backgrounds were distributed as follows: 22.5% had no formal degree, 27.5% held a diploma, 25% possessed an associate degree, 20% had a bachelor’s degree, and 5% held a master’s degree or higher. The age distribution was as follows: 17.5% were aged 25–30, 22.5% were between 31 and 35, 25% were 36–40, 17.5% were 41–45, and the remaining 17.5% were over 45 years old.
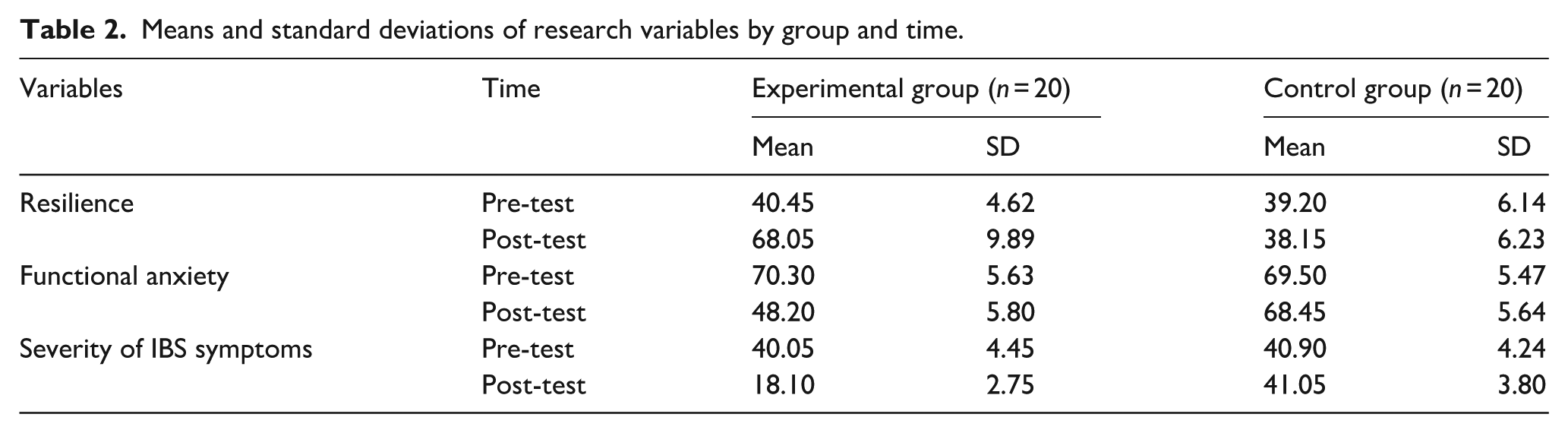
Table 2 presents the means and standard deviations for three variables—resilience, functional anxiety, and severity of IBS symptoms—comparing the experimental and control groups before and after the intervention. The pre-test scores were comparable between groups. However, following the intervention, the experimental group exhibited a significant increase in resilience and reductions in functional anxiety and IBS symptom severity. These group differences were analyzed using multivariate and univariate analyses of covariance (MANCOVA and ANCOVA).
Means and standard deviations of research variables by group and time.
Examining assumptions of parametric statistics and covariance analysis
One of the key assumptions of analysis of variance is the normal distribution of the dependent variables within the groups. In this study, the Kolmogorov–Smirnov test was employed to assess the normality of score distributions. The results indicated that the distributions for all measured variables in both the experimental and control groups did not significantly deviate from normality (p > 0.05).
As shown in Table 3, the variables of resilience, functional anxiety, and severity of IBS symptoms all met the normality assumption. The non-significant z-values (p > 0.05) further confirmed that the dependent variables satisfied the normality criterion required for subsequent covariance analyses.
Assessment of the regression slope homogeneity assumption.

Table 4 presents the results of Levene’s test, indicating that the variances across the studied groups are homogeneous. The F statistic was not significant at the p > 0.05 level, confirming the homogeneity of variances assumption. Furthermore, as shown in Table 3, the test of homogeneity of regression slopes yielded a non‑significant interaction term (p > 0.05), thereby meeting this ANCOVA prerequisite. Given that the core assumptions of covariance analysis—including variance homogeneity and regression slope homogeneity—were satisfied, ANCOVA was deemed appropriate for testing the study’s hypotheses.
Examination of the assumption of variances homogeneity.

Effect of group CBT on resilience, functional anxiety, and IBS symptom severity
To test the main hypothesis, a multivariate analysis of covariance (MANCOVA) was performed. Among the multivariate test statistics reported—including Pillai’s Trace, Hotelling’s T2, and Wilks’ Lambda—the Wilks’ Lambda value of 0.019 reached statistical significance (p < 0.001). This indicates a significant overall effect of the group cognitive behavioral therapy (CBT) on the combined dependent variables of resilience, functional anxiety, and IBS symptom severity.
Table 5 presents the results of the subsequent univariate ANCOVAs, controlling for pre-test scores, which demonstrate significant improvements in all three outcome measures for the experimental group compared to the control group. The findings show that group CBT significantly increased resilience while significantly reducing functional anxiety and IBS symptom severity, with effect sizes indicating these changes are substantial (all p < 0.01).
Results of ANCOVA for the effects of group CBT on resilience, functional anxiety, and IBS symptom severity.
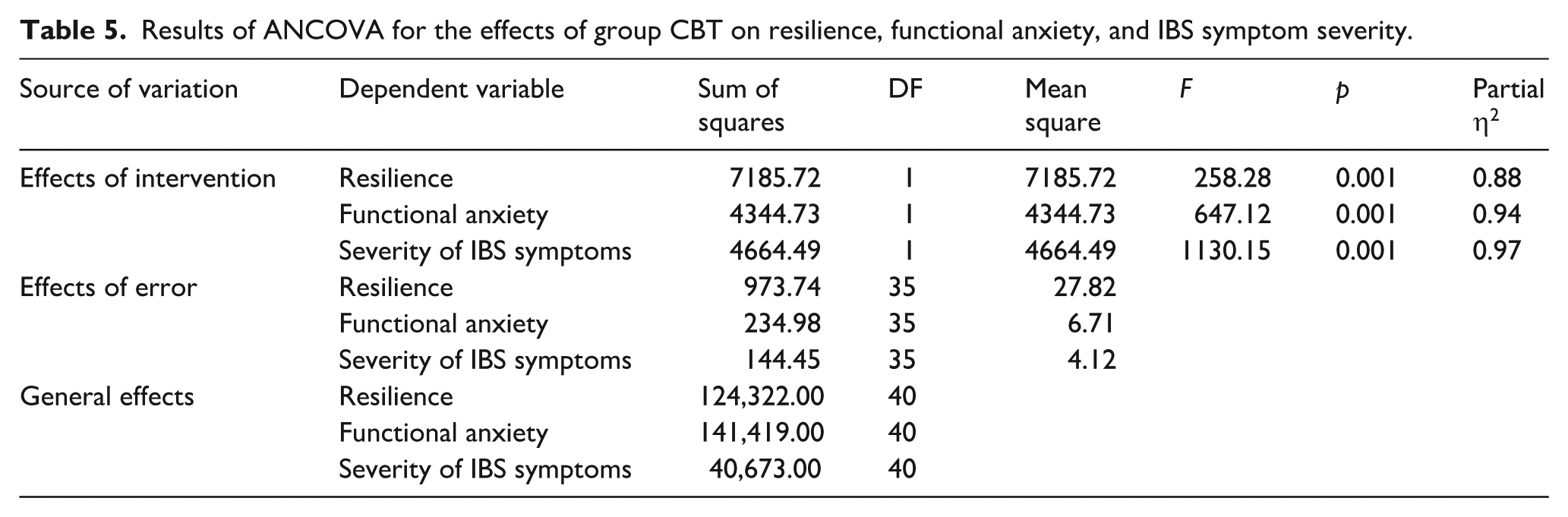
In conclusion, the group CBT intervention was effective in enhancing resilience and alleviating both functional anxiety and symptom severity among patients with IBS in Hamedan, thereby confirming the study’s primary hypothesis.
Group CBT enhances resilience in patients with IBS
Table 6 presents the univariate ANCOVA results examining the effect of group CBT on resilience among patients with IBS in Hamedan. After adjusting for pre-test scores, the analysis revealed a statistically significant improvement in resilience for the intervention group compared with controls (F(1, 38) = 5.72, p = 0.022, partial η2 = 0.13). These findings indicate that group CBT meaningfully enhances resilience in this patient population.
Univariate ANCOVA results for the effect of group CBT on resilience in patients with IBS.

Group CBT reduces functional anxiety in patients with IBS
Table 7 presents the univariate ANCOVA results assessing the effect of group CBT on functional anxiety among patients with IBS in Hamedan. After adjusting for pre-test scores, the analysis demonstrated a statistically significant reduction in functional anxiety for the intervention group compared with controls (F(1, 38) = 5.59, p = 0.023, partial η2 = 0.13). These findings indicate that group CBT effectively alleviates functional anxiety in this patient population.
Univariate ANCOVA results for the effect of group CBT on functional anxiety in patients with IBS.

Table 8 presents the results of the univariate ANCOVA examining the effect of group CBT on the severity of symptoms in patients with IBS in Hamedan. After controlling for pre-test scores, the analysis demonstrated a statistically significant reduction in IBS symptom severity in the intervention group compared to the control group (F(1, 38) = 5.03, p = 0.042, partial η2 = 0.20). These findings indicate that group CBT effectively alleviates symptom severity in this patient population.
Univariate ANCOVA results for the effect of group CBT on the severity of IBS symptoms.

Discussion
This study evaluated the effectiveness of group cognitive-behavioral therapy (CBT) in enhancing resilience, reducing functional anxiety, and alleviating symptom severity among patients with irritable bowel syndrome (IBS) in Hamedan. Multivariate and univariate ANCOVA analyses confirmed that, after controlling for pre-test scores, the intervention group demonstrated significant improvements in all three target outcomes compared with the control group.
Resilience
Group CBT yielded a statistically significant increase in resilience scores (F(1, 38) = 5.72, p = 0.022, partial η2 = 0.13). These findings support prior evidence by Aliyari Khanshan Vatan et al. 25 and Jacobs et al., 26 indicating that CBT enhances adaptive coping abilities. The intervention’s emphasis on identifying maladaptive beliefs, accepting uncontrollable internal experiences, and committing to value-driven behavioral change likely contributed to enhanced resilience.
Functional anxiety
The intervention led to a significant reduction in functional anxiety (F(1, 38) = 5.59, p = 0.023, partial η2 = 0.13), consistent with the work of Otte 23 and Slouha et al. 27 By addressing cognitive distortions, targeting emotional regulation, and implementing relaxation techniques, CBT appears to effectively diminish anxiety’s cognitive, affective, and behavioral components. The program’s structured nature and group-based format may have reinforced its impact.
Severity of IBS symptoms
Group CBT produced a notable decrease in IBS symptom severity (F(1, 38) = 5.03, p = 0.042, partial η2 = 0.20). This outcome is consistent with CBT’s theoretical framework, which posits that modifying catastrophic cognitions can reduce symptom amplification and improve behavioral adaptation. The dual focus on cognition and behavior appears more effective than targeting either domain in isolation.
Limitations
Several limitations must be acknowledged. First, the sample size was relatively small and drawn from a single geographic location, limiting generalizability. Second, purposive sampling and the absence of long-term follow-up may have constrained the strength and duration of observed effects. Third, although instrument reliability and validity were addressed, additional psychometric evaluation tailored to IBS populations is encouraged. Finally, the study did not explicitly control for the potential influence of time-related effects on resilience outcomes.
Implications and future directions
These results contribute important evidence supporting group CBT as a cost-effective, accessible intervention for IBS patients, with simultaneous benefits for psychological resilience, anxiety management, and symptom control. Clinicians may integrate group CBT protocols into multidisciplinary care plans for IBS. Future research should examine larger and more diverse samples, employ randomized controlled trial designs with extended follow-up, and explore the specific mechanisms through which CBT exerts its benefits. Investigating combinations of CBT with pharmacological or lifestyle interventions may also be valuable.
Conclusion
Group CBT demonstrated significant effectiveness in increasing resilience, reducing functional anxiety, and alleviating IBS symptom severity among patients in Hamedan. These findings underscore the value of integrating group CBT into multidisciplinary management strategies for IBS. Broader implementation of this intervention, alongside further research in diverse populations and over extended follow-up periods, is recommended to consolidate and expand these outcomes.
Footnotes
Acknowledgements
We are grateful to everyone who helped us in writing this article.
Authorship
The authorship has been agreed upon by all contributors. The corresponding author is Dr Mahdi Nobakht, and all authors have approved the final manuscript for submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The current research has received the code of ethics with the number IR.IAU.H.REC.1402.079.
Informed consent to participate
Informed consent was obtained from all individual participants included in the study.
Informed consent to publish
Informed consent for publication was obtained from all individual participants included in the study.
Trial registration (where applicable)
This study is not a clinical trial and, therefore, did not require trial registration.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.