
Abstract
Chronic endometritis (CE) is an inflammatory disorder of the endometrium, whose pathogenesis has not been fully elucidated. Although CE may be asymptomatic or it may present with subtle symptoms, it may cause significant adverse outcomes on human reproduction including an increased risk of recurrent miscarriages (RM) and recurrent implantation failure (RIF). The diagnostic procedure includes hysteroscopy with a targeted biopsy from areas suspected of having abnormalities. Histopathological assessment involves the identification of immunohistochemical markers for plasma cells, such as CD138 and MUM-1. The treatment of CE in women with a history of RIF may increase clinical pregnancy rates, implantation rates and ongoing pregnancy rates/live birth rates. It mainly concerns antibiotic therapy, with doxycycline as the first-line treatment. Surgical removal is necessary in cases of lesions such as fibroids, polyps or severe intrauterine adhesions. We aimed to summarize current knowledge in the field of the effective diagnosis and treatment of CE.
Keywords
Introduction
Chronic endometritis (CE) is an inflammatory disorder of the endometrium which is characterized by plasma cell infiltration into the endometrial stromal area. 1
The human endometrial tissue is a unique mucosal tissue which undergoes monthly morphologic, transcriptional, and translational changes influenced by estrogen and progesterone. 2 It is infiltrated by a wide variety of immunocompetent cells. Under physiological conditions, natural killers (NK), macrophages, neutrophils, dendritic cells and subsets of T cells are present in this tissue. It is considered that alterations in the composition of immunocompetent cells play a critical role in the establishment of embryo implantation and placentation. 2 It may be the reason why CE is associated with reproductive disorders including difficulties conceiving, pregnancy complications, an increased risk of recurrent miscarriages (RM) and recurrent implantation failure (RIF).3,4
The definition of RM is not obvious. The definitions vary across countries and recommendations. The European Society of Human Reproduction and Embryology (ESHRE) described RM as two or more spontaneous pregnancy losses. However, no pathophysiological proof was provided to confirm that consecutive or non-consecutive loss might be of importance. 5 In turn, RIF is mostly described as the failure to achieve a clinical pregnancy after two to three transfers of good-quality embryos. 6
The prevalence of CE in case of RIF was found to reach about 30.3%–33.7% and about 60% in a group of patients with unexplained RM.7–9 Despite a high frequency of CE in women experiencing the above-mentioned disorders, the condition is often undiagnosed or unrecognized due to the lack of specific symptoms and diagnostic challenges.8–11 Introducing more effective diagnostic methods and treatments could be crucial for improving the chances of conceiving and avoiding pregnancy complications.12,13
In recent years, an increasing interest has been noted as regards the understanding of the impact of CE on infertility, which contributes to a rise in research on this topic. As the understanding of the role of CE in women’s reproductive disorders grows, it is necessary to develop effective methods for diagnosing and treating this condition.
The aim of this article is to present current knowledge on CE, its pathogenesis, implications for reproductive health, effective diagnostic methods and treatment. We analyzed the available scientific evidence regarding the correlation between CE and infertility.
The relationship between chronic endometritis and infertility is summarized in Table 1.
The relationship between chronic endometritis and infertility.
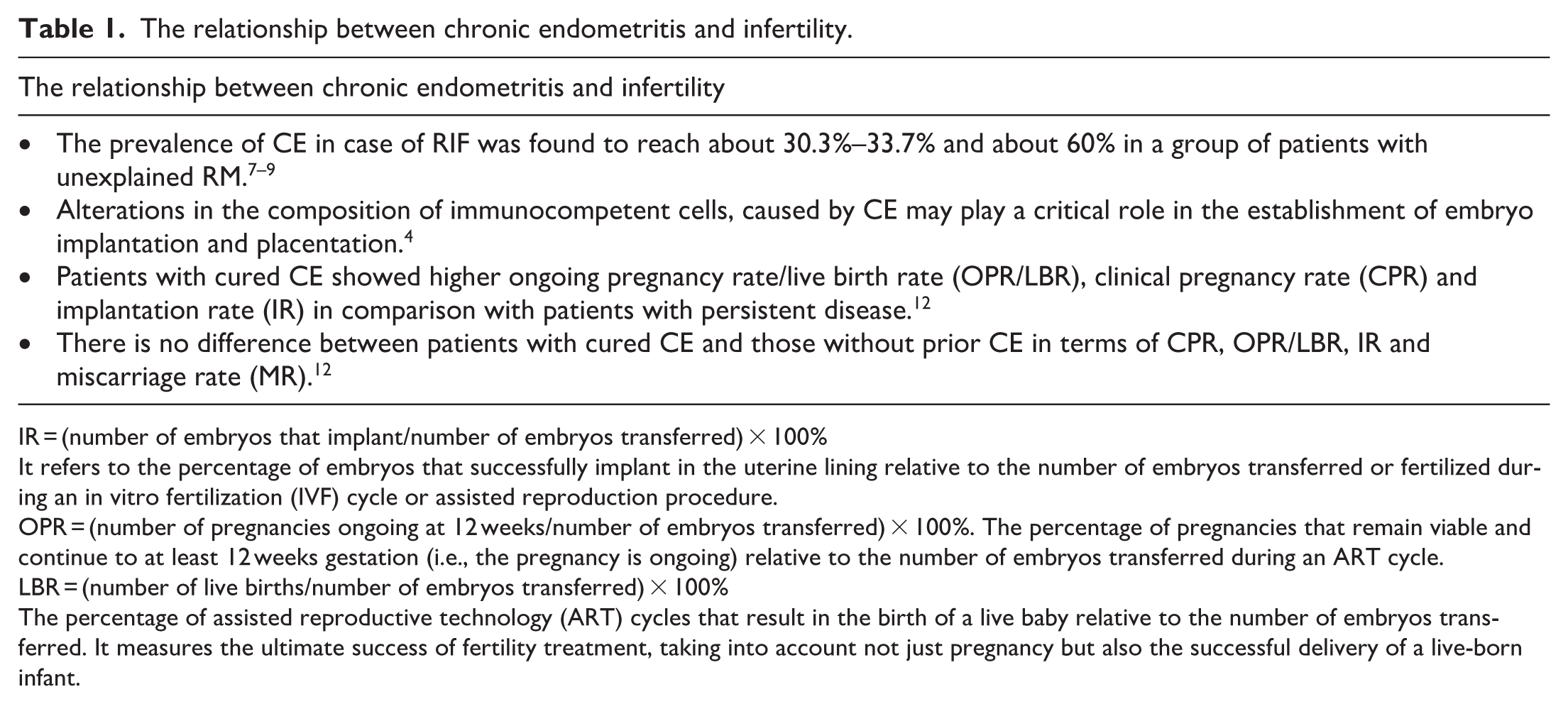
IR = (number of embryos that implant/number of embryos transferred) × 100%
It refers to the percentage of embryos that successfully implant in the uterine lining relative to the number of embryos transferred or fertilized during an in vitro fertilization (IVF) cycle or assisted reproduction procedure.
OPR = (number of pregnancies ongoing at 12 weeks/number of embryos transferred) × 100%. The percentage of pregnancies that remain viable and continue to at least 12 weeks gestation (i.e., the pregnancy is ongoing) relative to the number of embryos transferred during an ART cycle.
LBR = (number of live births/number of embryos transferred) × 100%
The percentage of assisted reproductive technology (ART) cycles that result in the birth of a live baby relative to the number of embryos transferred. It measures the ultimate success of fertility treatment, taking into account not just pregnancy but also the successful delivery of a live-born infant.
Methods
This study represents a narrative literature review regarding chronic endometritis. A literature search had been conducted in the PubMed of the National Library of Medicine until April 2024.
The search strategy aimed to capture studies addressing CE and its relationship with reproductive outcomes. The following keywords were used: “chronic endometritis,” “CD138,” “syndecan-1,” “MUM-1,” “implantation failure,” “recurrent miscarriage,” “infertility,” and “endometriosis.” These terms were combined in pairs using the Boolean AND operator to focus on intersections of interest (e.g., “chronic endometritis” AND “infertility,” “chronic endometritis” AND “recurrent miscarriage,” “chronic endometritis” AND “implantation failure”).
We included studies published in English, involving human subjects and that concerning CE in relation to infertility, RM, or implantation failure. The analysis focused on original research articles presenting the results of clinical, observational, or laboratory studies on CE and its association with reproductive outcomes and on systematic review.
All titles and abstracts were screened independently by two authors (MK and PP). Discrepancies in screening were resolved through discussion until consensus was reached. After initial screening, full texts of potentially relevant articles were reviewed to determine suitability for inclusion in the narrative synthesis. Finally 49 articles were included.
Discussion
Pathogenesis
Bacterial flora disorders
Due to good response to antibiotic treatment and the inflammatory nature of the disease, bacterial disorders are considered as the main reason of CE.3,14
Studies showed that the composition of bacterial flora varied among women with and without CE.15–24 The results of microbiological studies differ depending on the technical manner of the sampling collection.
In most studies showing the dominance of Lactobacillus species in the endometrial microbiota, the samples were obtained via the trans-vagino-cervical route. 15 Moreno et al. demonstrated that Lactobacillus-dominant endometrial microbiota (LDM, Lactobacillus content of 90% or more) in infertile women was associated with favorable reproductive outcomes in the following IVF-ET cycles. Conversely, the decreased significance of the Lactobacillus colony was correlated with poor reproductive outcomes – implantation failure and pregnancy loss. 16 Similar results were obtained in other studies emphasizing the increasing proportion of not – Lactobacillus genera in the endometrial microbiota of infertile women with CE (Anaerococcus, Bifidobacterium, Dialister, Gardnerella, Prevotella, Ralstonia, Phyllobacterium, Sphingomonas, Lactobacillus, and Streptococcus).10,17–19
When samples were collected via the trans-perineo-myometrial route during laparotomy/laparoscopy, different bacterial genera were identified (Acinetobacter, Pseudomonas, Sphingobium, Vagococcus, Cloacibacterium, and Comamonadaceae) in the general population of women.20–23 A potential contamination of the endometrial microbiota with vaginal microbiota during the trans-vagino-cervical endometrial sampling is one of the explanations for such an observation.
In 2019, Kitaya et al. identified microorganisms in less than half of women with a history of infertility using traditional culture and conventional polymerase chain reaction testing. 22 Conversely, Cicinelli et al. detected at least one pathogen in about 73% of cases of women with histopathologically confirmed CE. On the contrary, bacteria were detected only in 5% of women without CE. 24 The research showed the significance of common bacteria (Escherichia coli, Enterococcus faecalis, and Staphylococcus species) in the probable etiology of CE (detected in about 60% of cases). Ureaplasma urealyticum was detected in 10% of cases and Chlamydia in only 2.7% of positive endometrial cultures.
In developing countries, Mycobacterium tuberculosis should also be taken into consideration as the etiology of CE. 25
Benign gynecological disorders
The augmented prevalence of benign gynecological disorders and CE was observed, but the cause-and-effect relationship was not well examined.26–30 Kuroda et al. reported a high prevalence of CE in a group of infertile women with uterine cavity deformities (85.7% with endometrial polyps, 69.0% with submucosal uterine fibroids, 78.9% with intrauterine adhesions, and 46.2% with a septate uterus). 26
Associations between macropolyps and CE were especially observable in a group of patients with abnormal uterine bleeding, infertility, a history of PID (hydrosalpinx, fallopian tube obstruction) and multiple polyps compared to a single lesion.28–30
In 2023, Xiang et al. observed that the prevalence of histopathologic CE in infertile women with intrauterine adhesions depended on the severity of the lesions. The frequency of CE was higher in the group with severe compared to moderate ones (28.6% vs 15.1%). 30
Endometriosis
Some studies showed a correlation between CE and endometriosis. In 2014, Takebayashi et al. analyzed endometrial specimens obtained from 71 women who underwent hysterectomy. The specimens were immunostained for CD138 plasmacyte marker. The study revealed that women with endometriosis had a higher concomitance rate of CE than those without endometriosis (52.9% vs 27.0%), regardless of the stage of their disease. In addition, no associations occurred between CE and other popular uterine benign diseases, such as leiomyoma and adenomyosis in the study. 31
Similar results were noted in other studies.22–30,32 They were usually performed in populations undergoing pelvic surgery (hysterectomy or laparoscopy) and who had been diagnosed with endometriosis before the operation.
The prevalence of CE in women in the general population with suspected endometriosis may differ and needs more research.
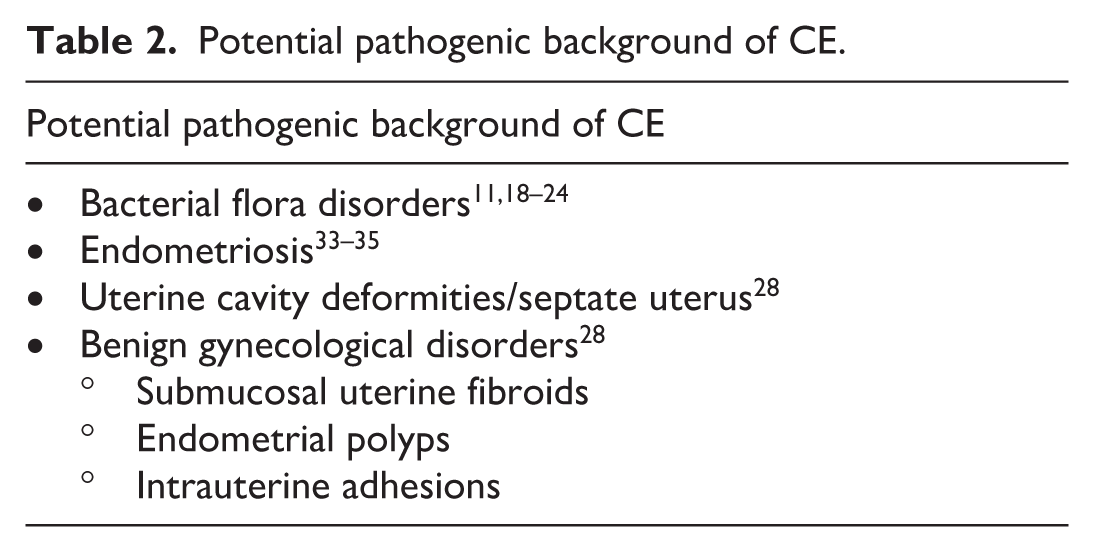
Potential pathogenic background of chronic endometritis are summarized in Table 2.
Potential pathogenic background of CE.
Diagnostics
Due to the subtle symptomatic nature of CE, the histopathological evaluation of endometrial biopsies is necessary for diagnosing this condition. 24 In a study by Ryan et al., it was noted that the presence of plasma cells was more common in the follicular phase compared to the luteal phase (59.3% compared to 19.7%), with a higher likelihood of occurrence in the early follicular phase (days 5–8 of the cycle) than in the late follicular phase (days 9–14 of the cycle). 15 Additionally, a higher plasma cell density was observed in the follicular phase compared to the luteal phase. 35
The majority of authors performed hysteroscopy to collect endometrial samples. 24 In 2019, the International Working Group for Standardization of Chronic Endometritis Diagnosis proposed the hysteroscopic criteria for CE listed in Table 3. 1
Hysteroscopic signs of CE.
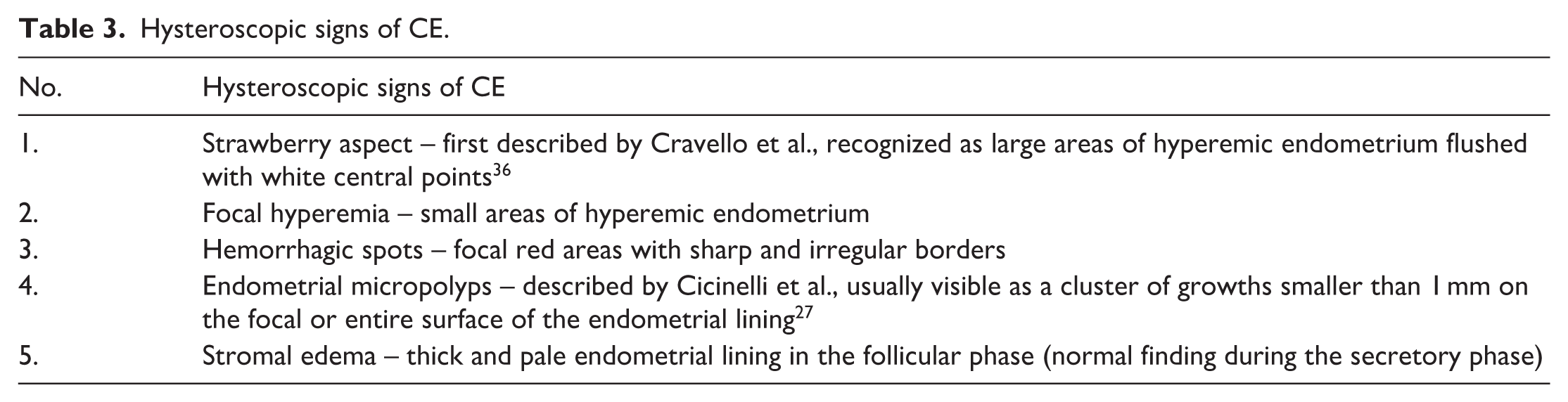
During hysteroscopy, a biopsy of the endometrium is collected from areas suspected of including abnormalities. Subsequently, the biopsy specimen undergoes histopathological evaluation. On microscopic examination, the presence of plasma cells in the stromal tissue of the uterine lining is a characteristic feature of CE. Under physiological conditions, plasma cells are not present in the endometrium. Research showed a strong correlation between hysteroscopic and histopathologic features. 24
It seems that under special conditions, when it is impossible to perform hysteroscopy, endometrial pipelle biopsy might be used. 37
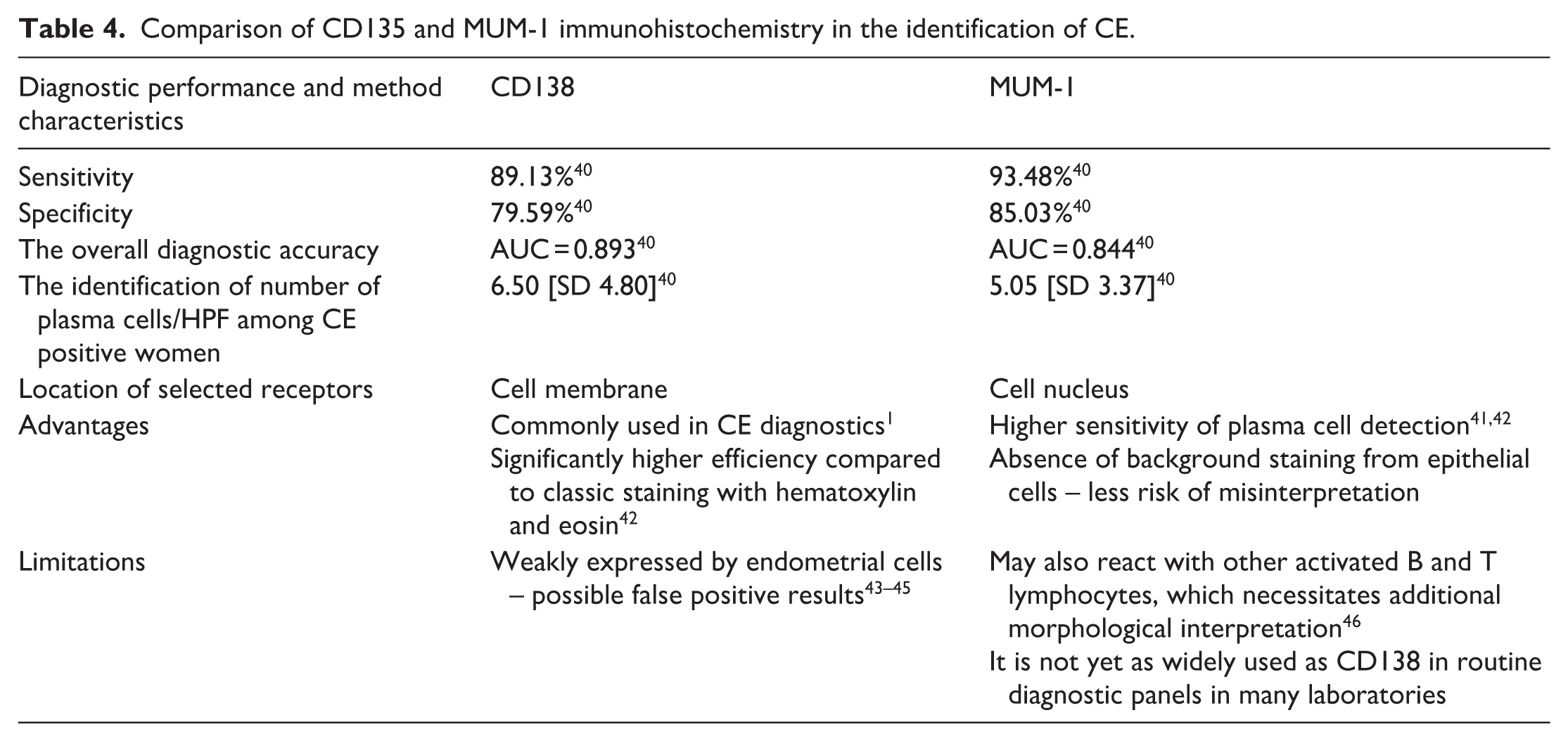
In detecting CE, the traditional method of evaluating microscopic specimens after staining with hematoxylin and eosin was found to be characterized by low sensitivity and specificity. 38 Therefore, immunohistochemical markers for plasma cells such as CD138 and MUM-1 have been introduced in the diagnosis.
(a) CD138, also known as syndecan-1, is a transmembrane protein belonging to the family of proteoglycans. It is an important marker for plasma cells. In reference to flow cytometry and immunohistochemistry, CD138 is often used for the identification of plasma cells because it is heavily expressed on their surface. Its presence on the cell membrane facilitates the identification and characterization of these cells in laboratory studies and in the diagnosis of diseases such as multiple myeloma.
(b) MUM-1, also known as interferon regulatory factor 4 (IRF4), is a transcription factor found in plasma cells as well as activated B and T lymphocytes. It is an important diagnostic marker in multiple diseases associated with the proliferation of plasma cells. 39
Currently, the detection of CD138 protein is the gold standard. The implementation of immunohistochemistry staining for CD138 detection significantly improved the sensitivity (100% vs 75%) and specificity (100% vs 65%) in the histopathological diagnosis of CE. 40
On the other hand, it is quite common for pathologist to describe the evaluation of 10 randomly selected fields of view at HPF (High Power Field), whereas some authors consider it appropriate to evaluate 20 fields of HPF. However there are pathologist who assess the entire surface of the obtained tissue section or the surface area of 10 mm2. 37 This creates a situation in which the diagnosis of a disease entity requiring antibiotic therapy depends on the diagnostic technique used, and under certain conditions, considerable overdiagnosis should be considered.
A study published in 2021 revealed that the immunohistochemical examination for MUM-1 and CD138 displayed similar sensitivity and specificity in the identification of plasma cells. Notably, MUM-1 was found to be more reliable than CD138 when individual samples were compared. 40 Similar results were reported in the study by Xiong et al., where the sensitivity and specificity of MUM-1 in the diagnosis of CE were slightly higher than those of CD138; however, this difference in sensitivity was not statistically significant.
On the other hand, results from two additional studies suggest the superiority of MUM-1 immunostaining over CD138 in the detection of CE.41,42 Klimaszyk et al. examined 54 women with a history of at least two intrauterine pregnancy losses and found that plasma cells were identified in 22 of 54 (40%) endometrial samples using CD138, compared with 31 of 54 (57%) using MUM-1 (p = 0.01), indicating a significantly higher sensitivity of MUM-1 for plasma cell detection. 41 Similarly, Parks et al. demonstrated that MUM-1 immunohistochemistry exhibits superior sensitivity for the identification of plasma cells in endometrial biopsies submitted to rule out CE: in their study of 311 specimens, MUM-1 detected plasma cells in 48% of cases, compared with only 23% identified by CD138 staining, highlighting the greater sensitivity of MUM-1 relative to CD138. 42
Xiong et al. suggested that the combined application of MUM-1 and CD138 staining enables high sensitivity while simultaneously reducing false-positive results. In their study investigating the utility of an artificial intelligence (AI) system in the diagnosis of CE using both MUM-1 and CD138 immunostaining, they reported a sensitivity of 100% and a specificity of 83.3%, with an overall diagnostic accuracy of 91.4%. 43
Comparison of the significance of CD135 and MUM-1 immunohistochemistry in clinical practice is summarized in Table 4.
Comparison of CD135 and MUM-1 immunohistochemistry in the identification of CE.
Treatment
Numerous trials revealed the beneficial role of CE treatment in the improvement of IVF procedure efficiency.11,13,25 The results, defined as the clinical pregnancy and ongoing pregnancy rate, were similar in a group without CE and a group after CE treatment. As the bacterial grounds are claimed to be the pathogenesis of CE, broad spectrum antibiotics seem to be the appropriate first line of treatment. Some authors applied antibiogram-guided antibiotic treatment strategies. 13 However, the identification of microbial cultures is not always possible.
Numerous authors observed a high effectiveness of doxycycline, covering the spectrum from common bacteria to mycoplasma. 47 The subsequent endometrial biopsy confirmed the effectiveness of a 14-day course of doxycycline twice a day. In 2017, Kitaya et al. obtained a 92.3% histopathologic cure rate in a group of infertile women with a history of RIF and CE. 7 When applying metronidazole/ciprofloxacin 500 mg two times a day for 14 days as the second line of treatment, the overall cure rate was 99.1%.
An increasing number of studies emphasized the role of histopathologic re-examination following first-line doxycycline treatment in improving reproductive outcomes in infertile women undergoing assisted reproductive technology treatment. 48 Patients successfully cured of CE after oral antibiotic administration showed significantly higher CPR, IR and OPR/LBR. No benefits of first-line antibiotic therapy could be noted in a group of persistent CE. Such patients should be enrolled for alternative antibiotic regimens.
Clinicians should consider an increasing prevalence of multi-drug-resistant CE. Between April 2010 and September 2021, Kitaya et al. assessed a group of 3449 patients with a history of RIF. 49 Multi-drug-resistant CE (MDR-CE) was defined as resistance to the first-line oral doxycycline and second-line treatment with a combination of metronidazole (500 mg/day) and ciprofloxacin (400 mg/day) for 14 days. The estimated proportion of MDR-CE concerned 7.8% of all CE cases. However, an increasing trend was observed over the years – its prevalence increased 8.27 times from 1.3% (between April 2010 and March 2015) to 9.6% between April 2015 and March 2020. During that time, the prevalence of CE was stable in patients with a history of RIF. It was 30.2% between April 2010 and March 2015, and 31.7% between April 2015 and March 2020. The authors compared a therapy with oral moxifloxacin 400 mg/day for 10 days and azithromycin 500 mg/day for 3 days. 13 Both treatment courses were comparable. The cure rate of histopathologic CE was 79.2% in moxifloxacin group versus 75.0% in azithromycin group. The live birth rate in the immediate subsequent cycle and cumulative three embryo transfer cycles were similar as well (31.6% and 57.9% vs 33.3% and 61.1%). Due to the shorter therapy duration, azithromycin was proposed as the third line of treatment.
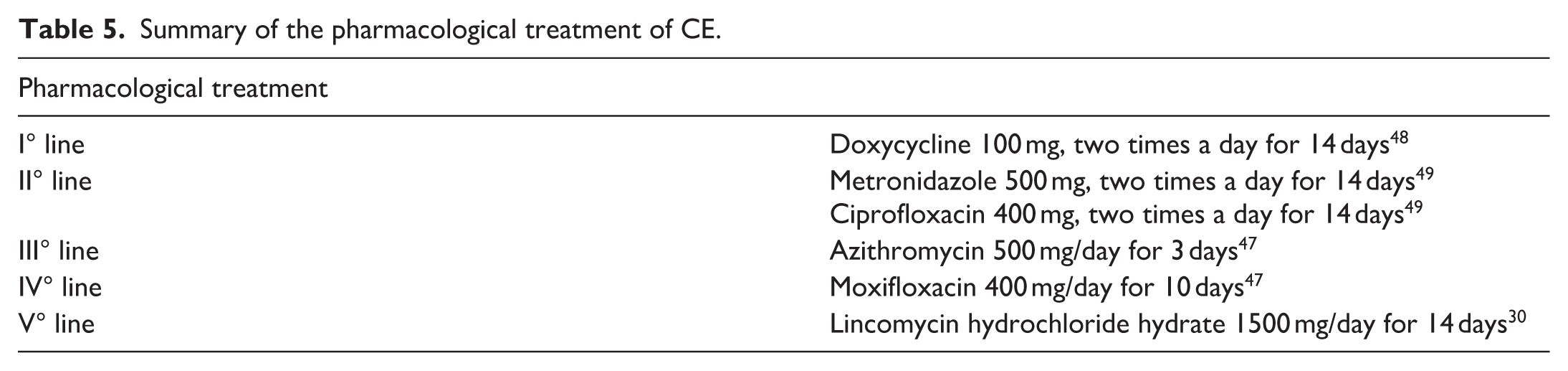
The same authors were looking for an alternative therapy for the remaining patients. They switched the antibiotic course in the group of 11 patients who did not respond to treatment with azithromycin or moxifloxacin, with positive results obtained in 5 patients. 50 Lincomycin hydrochloride hydrate 1500 mg/day for 14 days was introduced in the women who had not responded to azithromycin/moxifloxacin therapy. Five of those patients were confirmed to be histopathologically cured of persistent MDR-CE. Three of them had a successful live birth after an IVF procedure, one experienced an early pregnancy loss in the first trimester of pregnancy, and one patient had a negative pregnancy test. Summary of the pharmacological treatment is described in Table 5.
Summary of the pharmacological treatment of CE.
Surgical therapy is another therapeutic option. A hysteroscopic resection of some intrauterine lesions may constitute a therapeutic option for infertile women, reducing the need of antibiotics. 1 Kuroda et al. reported a high rate of recovery after surgical treatment in a group of infertile women with CE and uterine cavity deformities including endometrial polyps, myomas, IUA, and a septate uterus (89.7%, 100%, 92.8%, and 83.3%, respectively). 26
In 2023, Xiang et al. obtained similar results. 30 They observed a higher prevalence of histopathologic CE in infertile women with severe intrauterine adhesions compared to women with moderate ones (28.6% vs 15.1%). A combined therapy involving a hysteroscopic resection of the lesions and single 14-day oral doxycycline treatment was applied. The analysis showed no differences in OPR and miscarriage rates in subsequent ET cycles in a group of women with CE and those without CE.
In 2021, Kuroda et al. observed that a single 14-day course of doxycycline twice a day following polypectomy did not improve clinical pregnancy rates. Moreover, inappropriate antibiotic therapy might delay CE recovery, decreasing the efficacy of polypectomy on CE and pregnancy rates. 51
Hysteroscopic surgery may be effective in CE treatment in patients with endometrial micropolyps or stromal edema. However, further research is necessary to confirm the results. 1
Zhang et al. demonstrated that 77.98% of CE cases were cured in a group of 109 infertile women with RIF due to an intrauterine infusion of antibiotics and dexamethasone. 46 The group of women with no histopathological signs of CE achieved a significantly higher implantation rate (31.33%) and clinical pregnancy rate (51.76%) as compared to both 126 cases without CE (Group 1; 16.30% and 30.15%, respectively) and 24 cases with persistent CE (Group 3; 14.89% and 25.00%, respectively).
ESHRE and ASRM position on CE
Both ESHRE and ASRM currently do not have separate, formal guidelines dedicated exclusively to the diagnosis and treatment of CE. Experts from both societies emphasize the limitations in the evidence base, largely due to a lack of large, randomized controlled trials, and consequently most recommendations are derived from expert opinion and small studies, frequently conducted on heterogeneous groups.6,52
ASRM does not recommend routine screening for CE in all women with infertility; rather, testing may be considered in subgroups presumed to be at higher risk, such as those with a history of unexplained recurrent pregnancy loss, endometriosis, with abnormal uterine bleeding or chronic pelvic pain. According to ASRM expert commentary, diagnosis is generally based on histopathological identification of plasma cells, and when CE is diagnosed, antibiotic treatment should be considered. Doxycycline is proposed as a first-line therapy, with assessment of treatment success via repeat biopsy (“test of cure”), and, if persistent, a combination of ciprofloxacin and metronidazole may be considered. 6
ESHRE appears even more cautious regarding CE diagnostics and treatment. In the “Good Practice Recommendations on Recurrent Implantation Failure,” ESHRE does not recommend routine CE diagnosis and treatment in every case of patients with RIF but suggests that investigation can be considered on an individual clinical basis.
Although multiple diagnostic methods are described – including hysteroscopy, hematoxylin and eosin staining, CD138 immunostaining, and other techniques such as PCR and bacterial cultures – ESHRE underscores the absence of a standardized diagnostic technique and consensus on the threshold number of plasma cells required to establish the diagnosis of CE. 6
Due to current challenges in the histopathological diagnosis of CE, both ASRM and ESHRE envisage the future of CE diagnostics as involving more standardized techniques, such as DNA-based tests that allow exploration of microbiome composition.6,52
Summary
CE is an inflammatory disorder of the endometrium whose pathogenesis has not been fully elucidated. Although CE may be asymptomatic or it may present with subtle symptoms, it can cause significant adverse outcomes regarding human reproduction including an increased risk of RM and RIF.
Available data suggested that the treatment of CE in women with a history of RIF increased CPR, IR and OPR/LBR.
CD138 and MUM-1 immunohistochemistry is not routinely performed as a standard part of the pathohistological examination. However, it should be performed in this group of patients. Observations suggest that successful treatment of CE should be confirmed after antibiotic administration by histopathologic examination. The administration of the second or third line of treatment in resistant cases increases cure and pregnancy rates.
A proposed clinical algorithm for the diagnosis and management of CE is depicted in Figure 1.
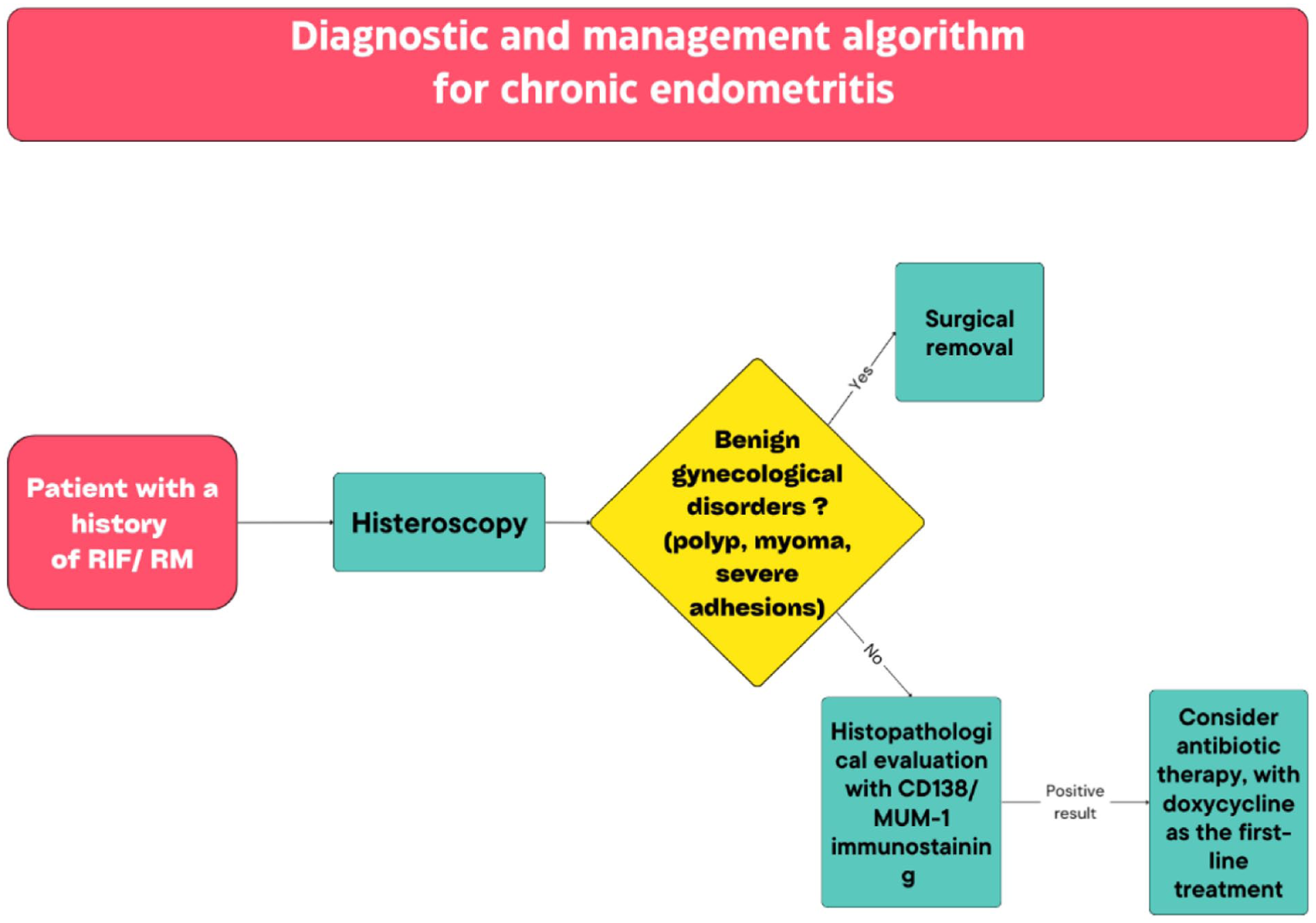
Diagnostic and management algorithm for CE.
Footnotes
ORCID iDs
Author contributions
Patrycja Monika Piwowarczyk and Michalina Kołodziejak have contributed equally to this work and share first authorship. They researched literature, and conceived the study and also wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Michał Ciebiera is the Editor-in-Chief of the Journal of Endometriosis and Pelvic Pain Disorders. He was not involved in the peer review or editorial decision-making process for this manuscript.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.