
Abstract
Introduction:
Evidence for the role of extracellular vesicles (EVs) in endometriosis pathophysiology suggests EVs may be a novel avenue for biomarker exploration. This study employed small particle flow cytometry to investigate plasma EVs with endometrial stromal cell markers and cervicovaginal fluid EVs with immunological receptors as diagnostic biomarkers of endometriosis.
Methods:
Blood and cervicovaginal fluid were collected from consenting patients undergoing surgery for suspected endometriosis. EVs were isolated from plasma (n = 15 per group) and cervicovaginal fluid (n = 20 per group), stained overnight with antibody probes, labelled with Aco-430 membrane stain then analysed by flow cytometry (Cytek Aurora). The proportions and antigen density of positive EVs were compared between people with endometriosis and symptomatic controls.
Results:
Measuring triple-positive EVs was deemed unsuitable given the variability in staining when multiplexing antibodies. Small proportions of antigen positive EVs were detected for all proteins investigated, however, no differences were observed for CD10+, CD90+, CD10+CD90+ and CD140b+ plasma EVs, or CCR2+, CD55+, CD59+ and CD82+ cervicovaginal fluid EVs.
Conclusions:
Although the EV populations did not distinguish endometriosis from symptomatic controls, this study provides valuable methodological insights into EV phenotyping to support future biomarker research and advance understanding of EV-mediated mechanisms in endometriosis.
Keywords
Introduction
Diagnosing endometriosis remains a clinical challenge. Recent guidelines indicate laparoscopy is no longer required to confirm endometriosis and imaging such as transvaginal ultrasound can detect endometriomas and deep infiltrating endometriosis (DIE) with reasonable accuracy. 1 However, ultrasound is highly operator dependent, and lack of sonographers with expertise in endometriosis ultrasound already limits its use. 2 Furthermore, superficial disease is often not detectable with imaging, and as such, a negative imaging result does not rule out endometriosis. As a result, laparoscopic surgery is often relied on to confirm a diagnosis and still the most common means of diagnosis. 3 However, for around one-third of patients who have laparoscopy for suspected endometriosis, there is no evidence of disease. 4 Thus, there is still a critical need for diagnostic biomarkers. Despite substantial research investigating endometriosis biomarkers, 5 none have been validated for clinical use to date. 6
Extracellular vesicles (EVs) are membrane delimited particles unable to replicate, secreted from all cell types and present in all bodily fluids. 7 EVs are carriers of molecular cargo embedded in the membrane and contained within the lumen, such as proteins, lipids and RNA species. These molecules often reflect the cellular origins of the EVs but can be selectively packaged, meaning their composition does not always mirror the abundance of these molecules in the cell of origin. 8 EVs from a range of biofluids and tissue types have emerged as mediators of the pathophysiological processes underpinning endometriotic lesion establishment and activity. 9 Specifically, it is well established that stromal cells, and EVs from these cells, play an important role in endometriosis pathology and endometriotic lesion development, inflammation and regeneration.10,11 Endometriotic EVs from stromal cells modulate inflammation specifically though regulating macrophage polarisation and further inflammatory cascade signalling, which can lead to neuro-angiogenesis and adhesions.12,13
EVs are known to migrate from their tissue of origin and cross biological barriers to enter bodily fluids, 14 a process enhanced by inflammatory conditions,15,16 which may be relevant in endometriosis given the systemic chronic inflammatory nature.17,18 Differences in molecular cargo from cases and controls have been demonstrated in EVs isolated from plasma,19–23 serum,24–31 peritoneal fluid32–35 and menstrual fluid. 36 Furthermore, the lipid bilayer provides stability in biological fluids and protects luminal molecular cargo from degradation, 37 positioning EVs as promising sources of diagnostic information. Most methodologies analyse EVs in bulk, limiting the detection of rare but potentially diagnostically relevant EV subpopulations. Flow cytometry is increasingly employed to address this limitation, allowing single-particle analysis resulting in increased specificity for disease related EVs. 38
Therefore in this study, we have developed and employed a small particle flow cytometry panel to explore EV biomarkers of endometriosis. We used this developed technique to investigate EVs across 2 different biological fluids.
Firstly, we aimed to assess whether EVs carrying endometrial stromal cell markers from previously described literature (CD10, CD90 and CD140b)10,11are identifiable in plasma. Secondly, we aimed to investigate previously identified immunological receptors 39 involved in the complement cascade (CD55 and CD59) and macrophage function (CCR2 and CD82) in cervicovaginal fluid EVs. Finally we analysed the proportions of these EVS to investigate whether they are increased in people with endometriosis compared to symptomatic controls.
Methods
Ethical approval
This study was approved by the Central Health and Disability Ethics Committee (HDEC) (2022 EXP 12616), received endorsement from the Research Advisory Group – Māori (RAG-M) at Te Whatu Ora – Capital and Coast (#937) and local approval from Te Whatu Ora – Capital and Coast research and audit committee.
Participant recruitment and sample collection
People having surgery for suspected endometriosis at Te Whatu Ora – Capital and Coast (Wellington and Kenepuru Hospitals, New Zealand) between June 2022 and August 2024 were invited to participate in this study, and all patients provided informed written consent. Eligible patients were aged between 16 and 45 years old. People with current known cervical abnormalities were excluded. Data was stored in REDCap (version 15.0.29).
Blood was collected from fasted participants prior to the commencement of anaesthesia at time of surgery. Blood was collected in ethylenediaminetetraacetic tubes (EDTA; BD Biosciences, #367873). Plasma was prepared through double centrifugation at 600 × g for 10 min at room temperature. Plasma was visually inspected for haemolysis and stored in 550 µL aliquots at −80°C until use.
Cervicovaginal fluid was collected via low vaginal swab by the operating surgeon after the administration of anaesthesia, prior to surgical preparation. A FLOQ swab (Copan Diagnostics, #5E089N) was inserted into the vagina and turned for approximately 30 s, then placed into 1 mL phosphate buffered saline (PBS; Thermo Fisher, #18912014). Samples were visually assessed, and those with any blood contamination were excluded. The swab was removed and samples were stored at −80°C until EV isolation.
Participants with histologically confirmed endometriosis and participants with extensive disease requiring conversion to a planning laparoscopy were considered the endometriosis group, and were staged using the revised American Society for Reproductive Medicine (rASRM) scoring system. 34 Participants were categorised into the ‘no endometriosis’ when surgical notes stated there was no visible evidence of endometriosis and no biopsies were taken, or when all biopsies were histologically negative.
To prioritise clinical transability, no exclusion criteria relating to menstrual cycle stage or hormonal medication use were applied. Menstrual stage was estimated based on participant reported data, described in Supplemental methods. Groups assigned were combined oral contraceptive pill (COP), progestin medication, gonadotropin-releasing hormone (GnRH) analogue, proliferative phase, secretory phase, irregular periods or unknown.
EV isolation and characterisation
EVs were isolated from stored plasma and cervicovaginal fluid samples using qEVoriginal columns (Izon Science, #ICO-70) on an automated fraction collector (AFC; Izon Science, #AFC-V2). Samples were thawed at 37°C then centrifuged twice at 2000 × g at 4°C for 10 min. qEVoriginal columns were flushed using PBS prior to loading 500 µL of plasma or cervicovaginal fluid to the top of the column. Three 0.4 mL EV rich fractions (fractions 5–7) were collected after the 2.9 mL default buffer volume and pooled.
Plasma EVs were characterised by tuneable resistive pulsing sensing (TRPS), transmission electron microscopy (TEM), and western blotting, as in Paterson et al. 39 and detailed in Supplemental methods.
EV staining for flow cytometry
All antibodies were titrated before use, with final titre chosen based on the signal-to-noise ratio (false positive events in reagent controls/positive EV events), and assessment of the spread of positive and negative populations relative to unstained EVs.
A 47.5 µL volume of pooled plasma EVs was stained with 2.5 µL of antibody diluted in PBS. Firstly, as EVs have limited ability to bind multiple probes due to low surface area, fluorescence minus multiples (FMMs) were performed to assess the appropriateness of multiplexing. Samples were stained with either a cocktail of anti-CD10-BB515 and anti-CD90-BV711, or anti-CD140b-PE alone diluted in PBS (Table 1). Stained plasma EVs were stored at 4°C in the dark overnight in 1.5 mL lobind tubes (Eppendorf, #EPP0030108051).
Antibody details for plasma and cervicovaginal fluid experiments.
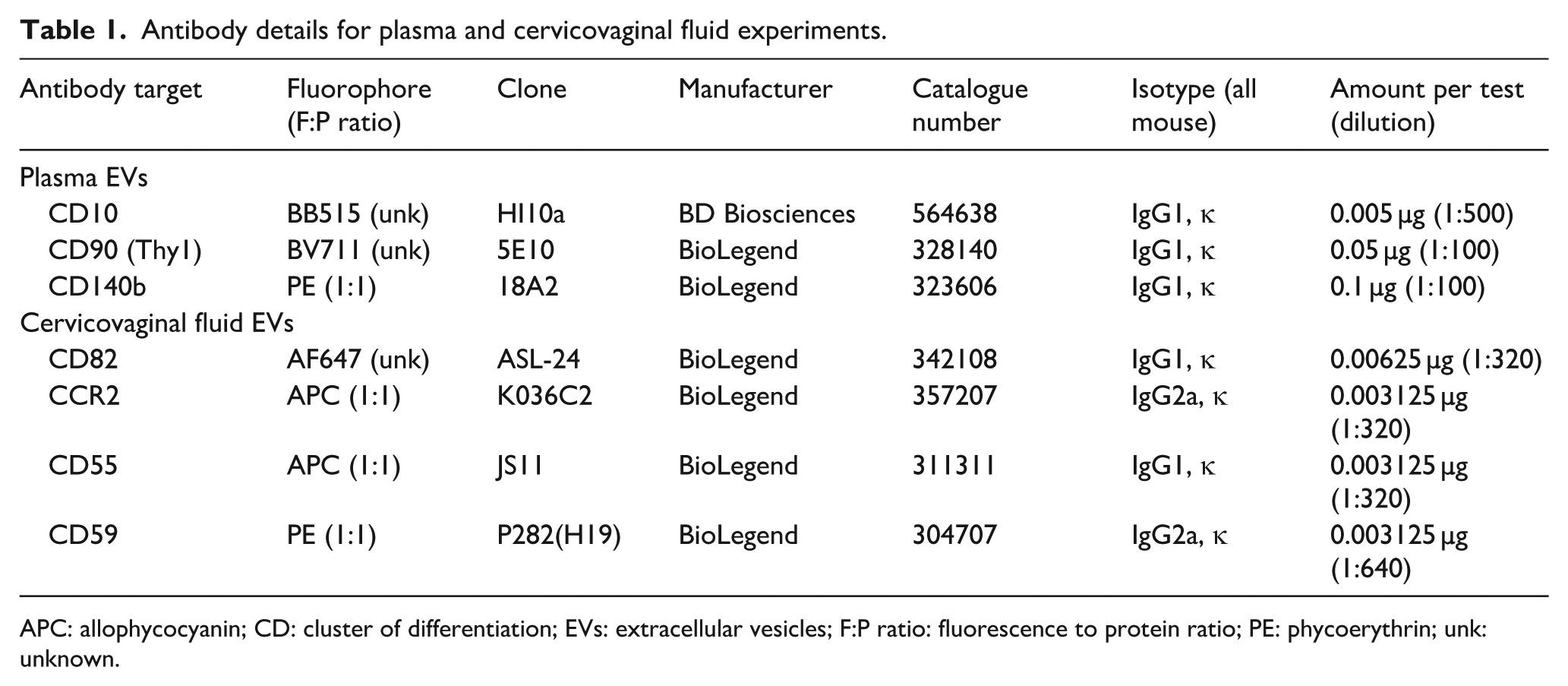
APC: allophycocyanin; CD: cluster of differentiation; EVs: extracellular vesicles; F:P ratio: fluorescence to protein ratio; PE: phycoerythrin; unk: unknown.
Pooled cervicovaginal fluid EVs were further concentrated to 47.5 µL using 10 kDa centrifugation units. Then, 9 µL of EVs were stained with 1 µL of diluted anti-CD82-AF647, anti-CCR2-APC, anti-CD55-APC, or anti-CD59-PE (Table 1) antibody overnight at 4°C protected from light in 0.5 mL lobind tubes (Eppendorf, #EPP0030108310). No multiplexing was performed; each 10 µL test contained one antibody probe.
The next day, 9 µL of stained EVs were incubated with 2.5 µM Aco-430 (Acoerela, #Aco-430 25T) for 60 min at room temperature. Every experimental day, a new vial of Aco-430 was reconstituted in PBS to 25 µM, vortexed for 1 min, then sonicated for 15 min at 40°C. EVs were then diluted 1:200 in PBS for analysis. Buffer only, reagent controls and unstained EVs were included every experimental day.
Flow cytometry of extracellular vesicles
All flow cytometry experiments were performed on a three-laser (violet-blue-red) Aurora full spectrum flow cytometer (Cytek Biosciences) equipped with the enhanced small particle detection module and a 0.04 µm in-line sheath filter. Detector configuration is in Supplemental Table 1. Sheath fluid was 0.22 µm filtered de-ionised water. All controls and samples were run on the lowest flow rate (10–15 µL/min) and analysed for 240 s.
Optimal scatter and fluorescence gains were determined using FCMpass (version 4.2.5) semi-automated tool 40 and are listed in Supplemental Table 1. An SSC threshold of 1500 was applied during acquisition. Additionally, a V2 threshold of 1000 was applied for cervicovaginal fluid EV experiments.
Serial dilutions and detergent lysis were performed to demonstrate single, vesicular detection (Supplemental methods).
Data were unmixed in SpectroFlo (version 3.03, Cytek Biosciences) prior to analysis. For unmixing, compensation beads (BD Biosciences, #552843) were used for all fluorophores and lyophilised liposomes (gifted by manufacturer) were used for Aco-430. Autofluorescence was extracted for cervicovaginal fluid data.
To convert arbitrary scatter and fluorescence parameters into standardised units, flow cytometry standard (FCS) files were calibrated using FCMpass (version 4.2.5) semi-automated software according to the developer’s protocol. 40 Scatter calibration was performed using polystyrene nanosphere size standards 70–400 nm (Thermo Fisher Scientific, #3070A, #3080A, #3090A, #3100A, #3125A, #3240A, #3300A, #3400A). Fluorescence calibration was performed using Rainbow Calibration Beads, 8 Peak (SpheroTech, #RCP-30-5A). Detailed data calibration methods are in Supplemental methods. The Rainbow bead data were also used to monitor the performance of the flow cytometer across experimental days (Supplemental methods).
Data analysis
The calibrated FSC files generated by FCMpass were used for analysis, with scatter calibrated to EV size (nm) (average refractive index) and fluorescence parameters in the standardised units of MEAF647, MEAPC, MEBB515-H, MEBV711-H, MEPE-H. Analysis was performed using FlowJo version 10.4.2 (BD Biosciences).
Aco-430 positivity was set based on unstained EVs. Aco-430+ events sized between 100 and 1000 nm were deemed the EV population. The 1500 arbitrary unit SSC threshold conferred an approximately 100 nm limit of detection and an upper limit of 1,000 nm (average refractive index) was set. EVs > 200 nm (small EVs) and EVs < 200 nm (large EVs) gates were also applied. 7
For plasma EVs, CD10, CD90 and CD140b gates were set on the unstained EV autofluorescence. The CD90 gate was then applied to CD10+ EV populations to identify CD10+CD90+ EVs. For cervicovaginal fluid EVs, CD55, CD59, CD82 and CCR2 gates were set based on the Aco-430 single stains, where there were less than 10 positive events. Thresholds for positivity for each antigen are reported in MESF are in Supplemental methods and the gating strategies are in Supplemental Figures 1 and 2.
Acquisitions with less than 10,000 Aco-430+ events were excluded. When the technical duplicate had sufficient Aco-430+ events, this single replicate was used. The number of antigen-positive EVs were expressed as a percentage of the total EV population. Median fluorescence intensity (MFI) statistics for antigen-positive EVs were acquired. Samples with less than 50 antigen-positive EVs were assigned the MESF value of the lower limit of the positive gate. Data from technical duplicates were averaged.
The completed MIFlowCyt-EV document is in Supplemental material.
Statistical analysis
All statistical analyses were performed in GraphPad Prism v10.2.0 with significance set at p < 0.05 or adjusted p < 0.05.
Categorical variables were presented as total count and relative percentages. Gravidity and parity were reported as median (quartile 1–quartile 3). Fisher’s exact tests and chi-square analyses were performed on categorical variables. Age was presented as mean ± standard deviation and compared using a two-tailed unpaired t-test.
The proportions and MFIs of antigen-positive EVs were reported as median (quartile 1–quartile 3), and groups were compared using Mann–Whitney U tests with Holm–Šídák correction for multiple comparisons. For analysis by approximate menstrual phase, proportions of positive EVs and MFI data from both groups were compared using Kruskal–Wallis tests with post-hoc Dunn’s tests corrected for multiple comparisons.
Results
Participant cohorts
For both the plasma and cervicovaginal fluid cohorts, the endometriosis and no endometriosis groups were similarly matched for most recorded characteristics (Table 2). For plasma EVs, two-thirds of the participants were age and approximate menstrual stage matched, while the remaining participants were only age matched. For cervicovaginal fluid, almost half (9/20) of participants were both age and menstrual phase matched with the remaining 11 participants only aged matched. In both cohorts, the no endometriosis group had a significantly higher proportion of participants that had other pathologies identified (plasma, p = 0.035; cervicovaginal fluid, p = 0.008). The most common other pathology identified in the no endometriosis group was paratubal cysts (benign cysts on the fallopian tube, typically self-resolving).
Clinical characteristics of cohorts for plasma and cervicovaginal fluid extracellular vesicle flow cytometry.
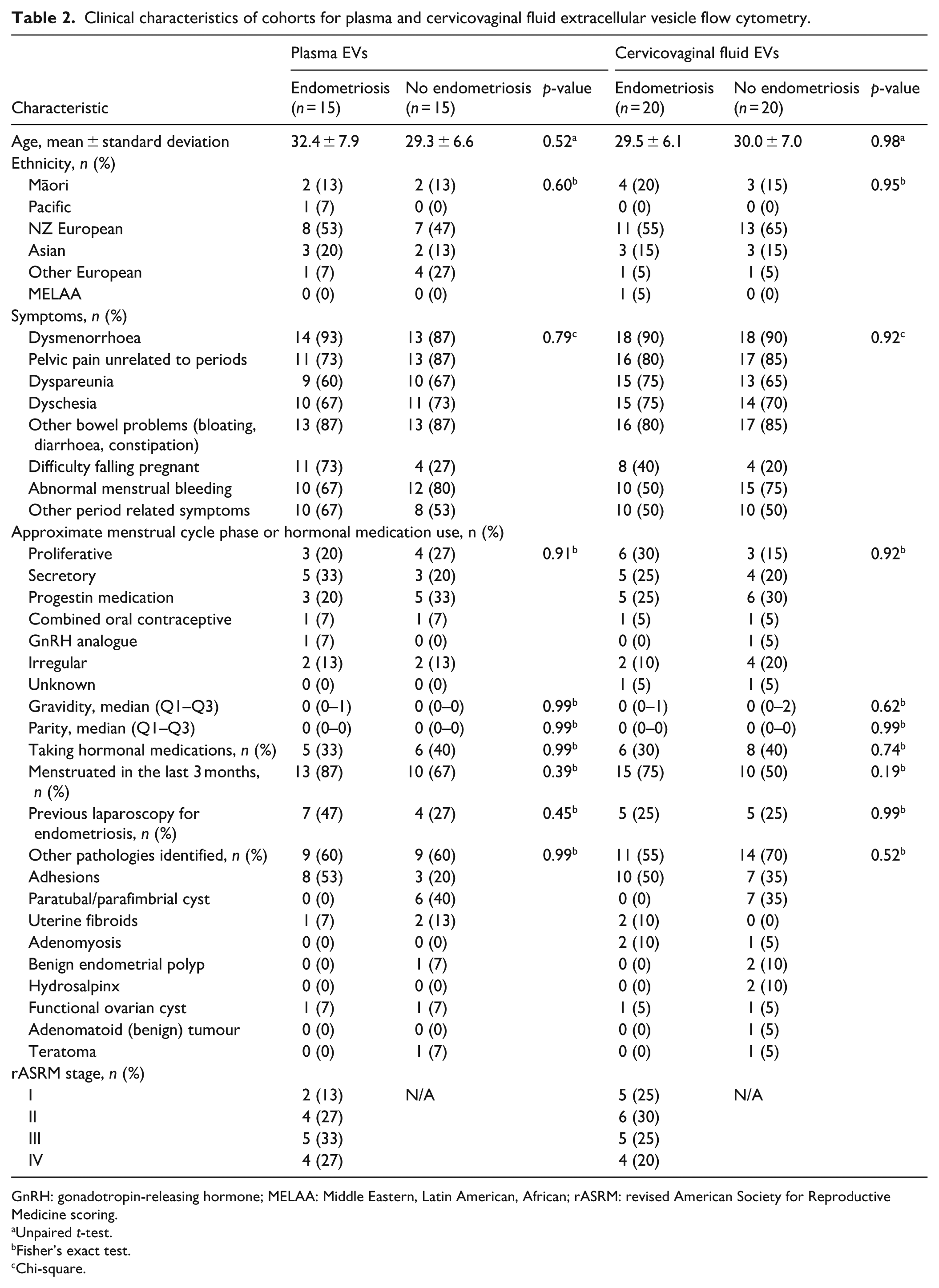
GnRH: gonadotropin-releasing hormone; MELAA: Middle Eastern, Latin American, African; rASRM: revised American Society for Reproductive Medicine scoring.
Unpaired t-test.
Fisher’s exact test.
Chi-square.
Flow cytometry
Plasma EVs were characterised according to international consensus guidelines 7 (Supplemental Figure 3). We have previously reported the characteristics of cervicovaginal fluid EVs isolated from vaginal swab samples. 35
The performance of the cytometer across the experimental days was tracked using 8-Peak Rainbow beads. Five samples (n = 3 endometriosis, n = 2 no endometriosis) from cervicovaginal fluid cytometry experiments were excluded due to poor fluorescence calibration, with the residual percentage exceeding the 5% a priori limit 41 for two of the bead populations in the R1 detector (Supplemental Figure 4).
Single vesicle detection was assessed through detergent lysis and serial dilution analysis (Supplemental Figure 5). Sample lysis resulted in an almost 90% reduction in Aco-430+ events (plasma: 88.6% ± 4.1%, p = 0.011, cervicovaginal fluid: 85.9% ± 7.9%, p = 0.023, n = 3 for both). Serial dilutions performed on the first three consecutive samples analysed demonstrated an absence of swarm detection, with a linear relationship between particle count and dilution factor and a consistent Aco-430 MFI.
Plasma
Fluorescence minus multiples demonstrated a reduction in the number of antigen-positive EVs when multiplexing (Supplemental Figure 6). CD10+ EV detection was reduced to 23% ± 4.9% of the single stain CD10+ EV count when multiplexed with both CD90 and CD140b. CD90+ EV detection was less affected by the addition of a third antibody. CD140b+ EV detection was inconsistent when multiplexed with just one or two other antibodies. Based on these results, CD10 and CD90 were deemed appropriate to be probed in combination, while CD140b was deemed only appropriate for single staining.
There were no differences in the proportion of CD10+, CD90+, CD10+CD90+ and CD140b+ EVs between the endometriosis and no endometriosis groups (Figure 1). This held true when analysing small EVs (EVs < 200 nm) and large EVs (EVs > 200 nm) separately. There were also no differences in the MFIs of BB515 for CD10+ or CD10+CD90+ EVs, BV711 for CD90+ or CD10+CD90+ EVs, or PE for CD140b+ EVs between the two groups (Figure 2). Supplemental Table 2 summarises the proportions and MFIs of antigen-positive EVs.
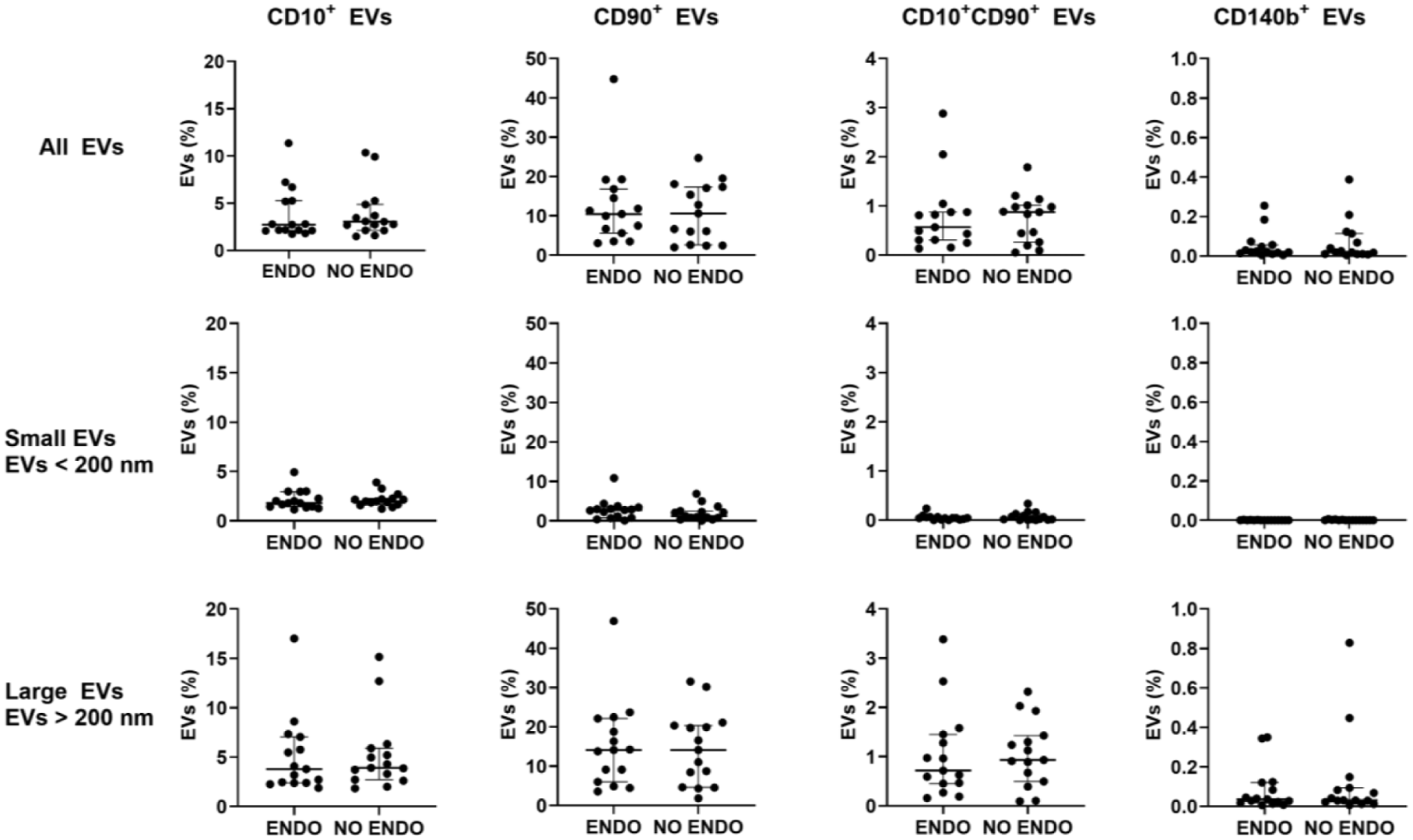
Proportions of CD10+, CD90+, CD10+CD90+ and CD140b+ plasma EVs.
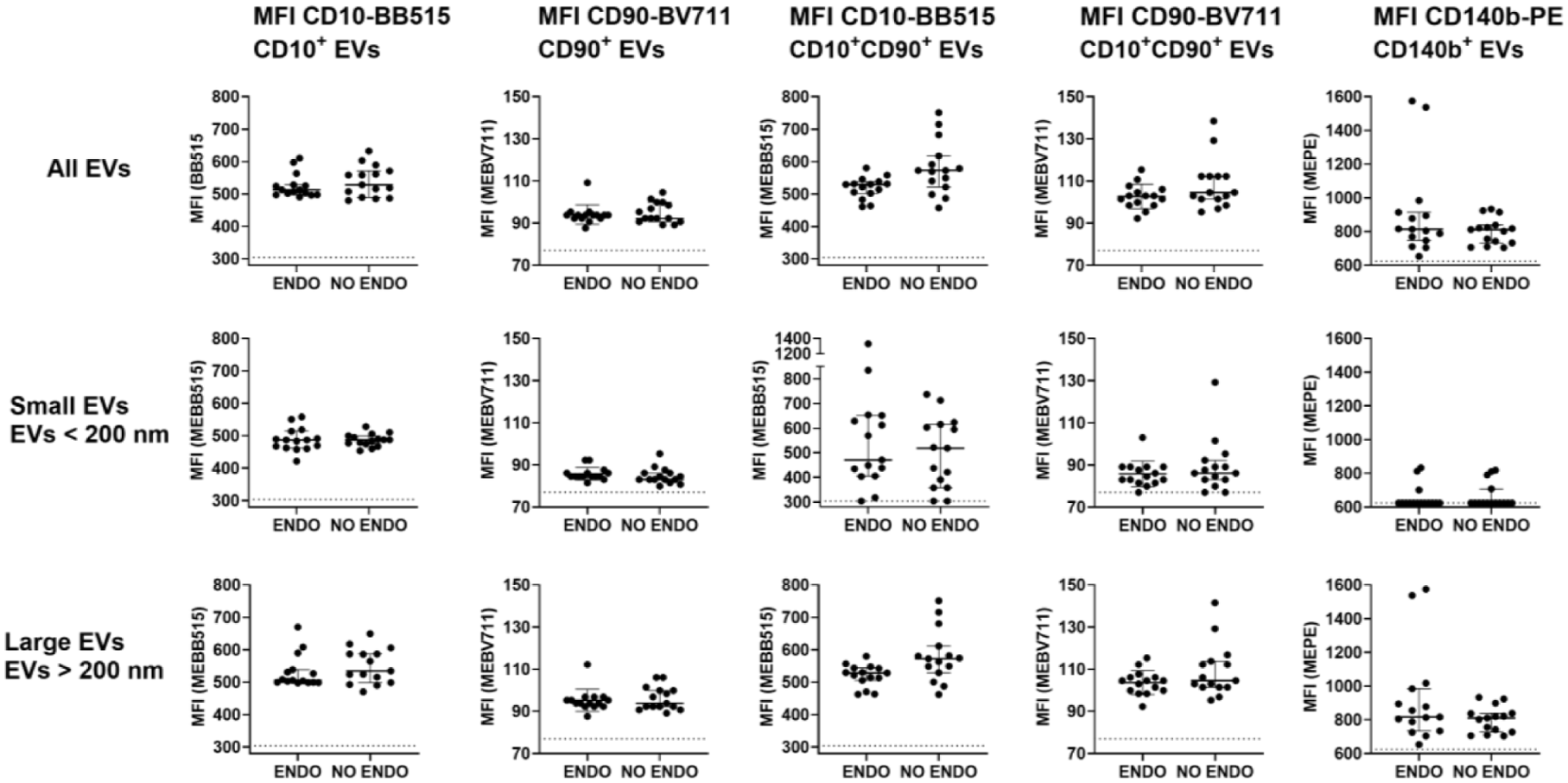
Median fluorescence intensity’s of CD10+, CD90+, CD10+CD90+ and CD140b+ plasma extracellular vesicles.
Data from both groups were examined together by menstrual phase post-hoc. There were no differences in proportions of CD10+, CD90+, CD10+CD90+ and CD140b+ EVs by approximate menstrual phase (Supplemental Figure 7). The MEPE MFI of CD140b+ EVs was significantly decreased from 832 (817–967) in the irregular menstrual period group (n = 4) compared to 706 (705–768) in the secretory phase group (n = 8). No other differences between approximate menstrual phase groups were observed.
Cervicovaginal fluid
There were no differences (adjusted p > 0.05) between the endometriosis and no endometriosis groups in the proportion of positive EVs or MFIs of CCR2+, CD55+, CD59+ or CD82+ total EVs, small EVs or large EVs (Figures 3 and 4). Tabulated results with median, lower and upper quartile values can be found in Supplemental Table 3.
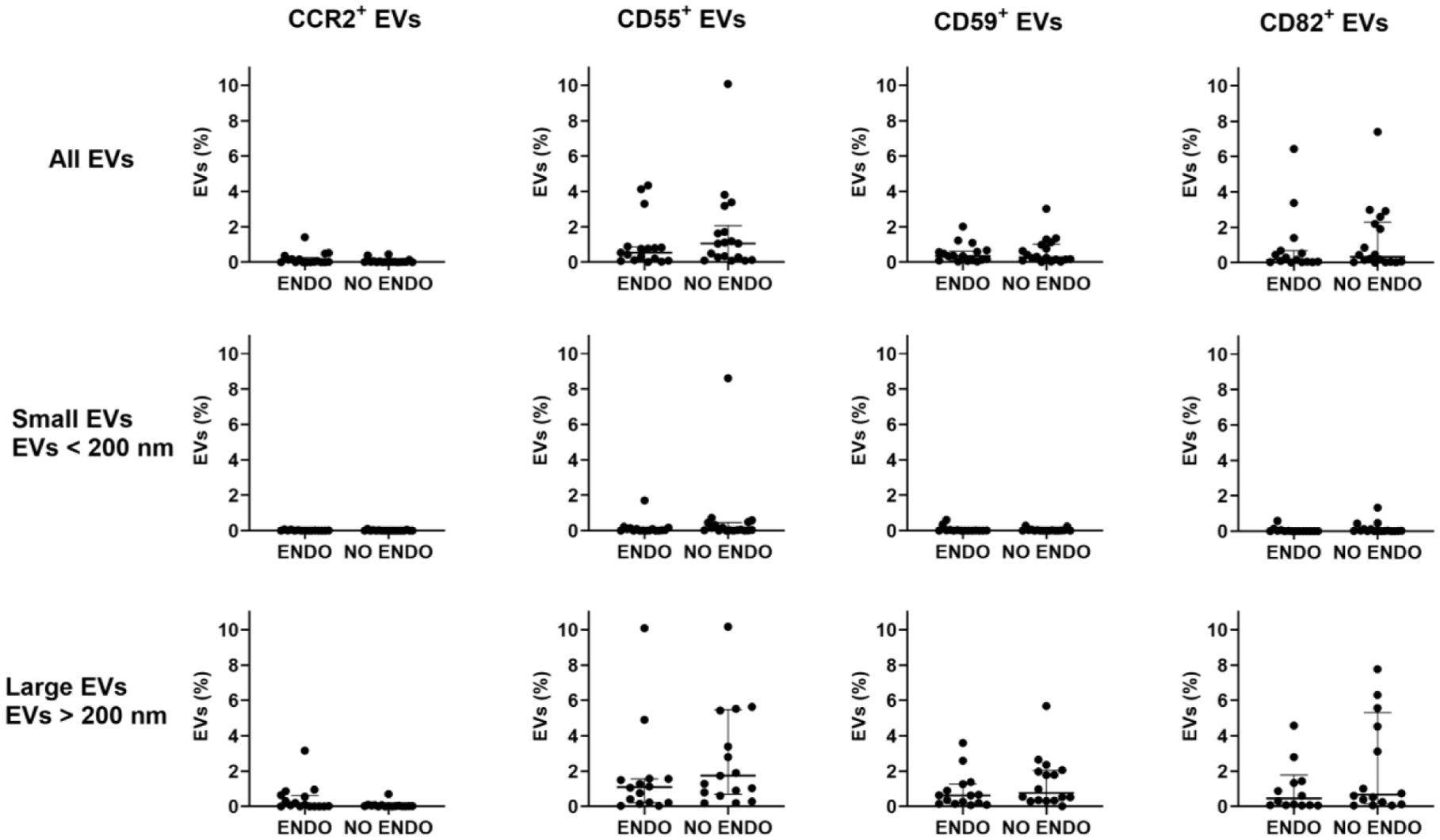
Proportions of CCR2+, CD55+, CD59+ and CCR2+ cervicovaginal fluid EVs.
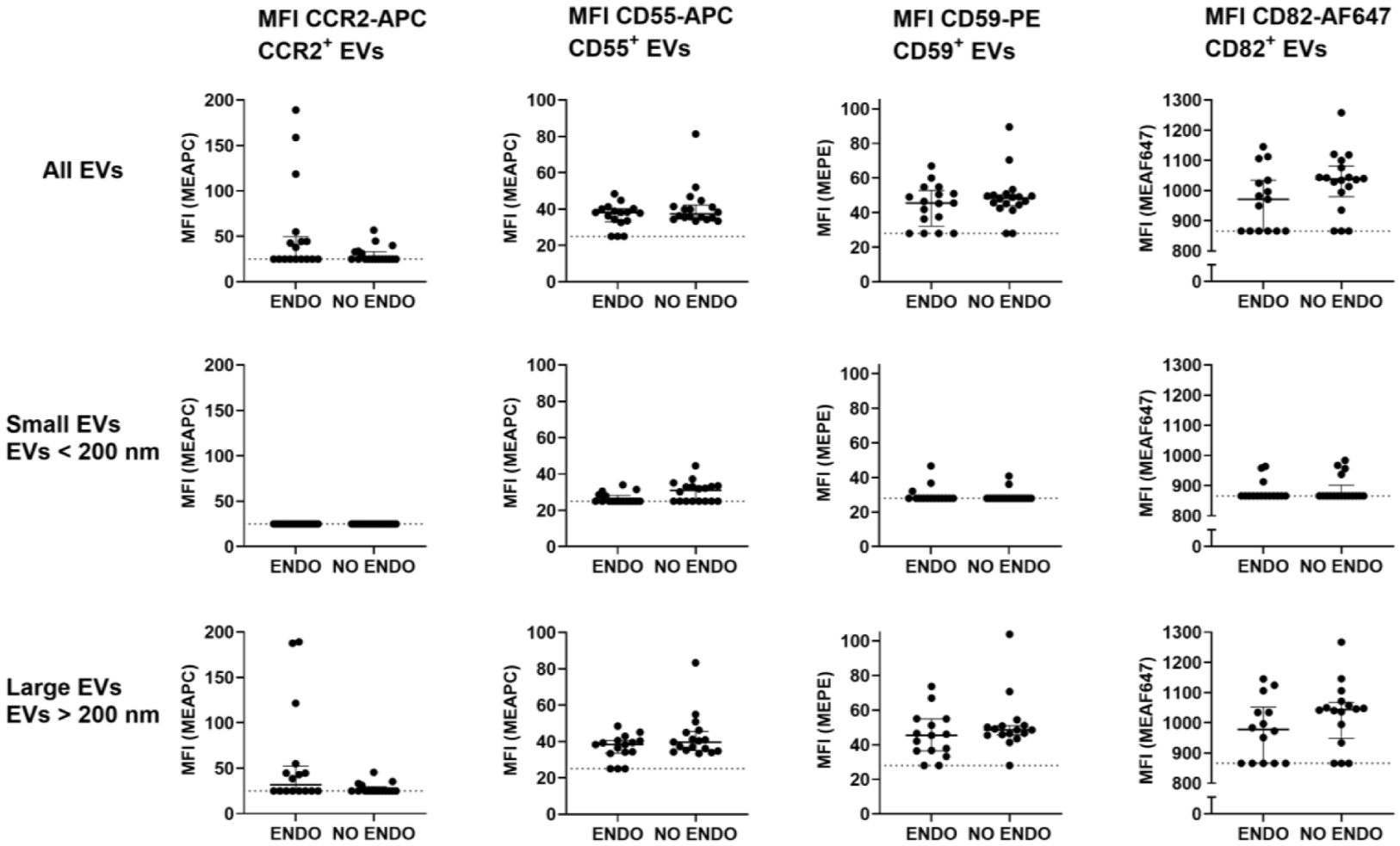
MFIs of CCR2+, CD55+, CD59+ and CD82+ cervicovaginal fluid EVs.
Discussion
In this study, we investigated plasma and cervicovaginal fluid extracellular vesicles for endometriosis biomarkers using small particle spectral flow cytometry, with no differences between groups identified. Although the findings were negative, they demonstrate the utility of small particle cytometry for measuring plasma and cervicovaginal fluid EV surface markers.
CD10, CD90 and CD140b were assayed in plasma EVs as these proteins are expressed by mesenchymal stromal cells and are stably expressed across the menstrual cycle in most endometrial and endometriotic stromal cells.42,43 This study originally aimed to quantify triple-positive EVs (CD10+CD90+CD140b+ EVs) to enhance specificity for endometrial or endometriotic EVs, given estimates are only 0.2% of circulating EVs are tissue derived. 39 The proteins assayed are also expressed by many other cell types abundant in circulation, for example neutrophils express CD1040,44 and CD90 is expressed by natural killer cells and activated endothelial cells.45,46 However, measuring triple-positive EVs was deemed as unsuitable given the variability observed in CD140b+ detection when multiplexing. Our results, and others,47,48 suggest a reconsideration of how multiplexing might be applied in future nanoparticle flow cytometry studies.
We then investigated immune regulatory EVs in cervicovaginal fluid, a potentially more biologically relevant biofluid. 5 Small proportions of the overall EV population were positive for CCR2, CD55, CD59 and CD82. Antigen density of CD55+ small EVs may be increased in the no endometriosis group, as the difference was significant before p value adjustment for multiple comparisons. Further studies are required to confirm this difference. The decreased antigen density of CD55+ EVs in endometriosis may be passive, reflecting the downregulation of CD55 observed in the endometrium in endometriosis. 49 Our limit of detection were particles sized approximately 100 nm, and as EV size follows a power-law size distribution where the smallest particles are the most abundant, 50 there were likely a significant proportion of EVs that were undetectable. Given the differences between small and large EVs regarding recipient cell uptake, proteome, and EV-induced functional changes, 51 employing a cytometer designed for nanoparticle analysis would benefit future research investigating CD55+ EVs in cervicovaginal fluid.
The main limitation of this study is the small sample size which may limit detection of meaningful differences. This was a pilot investigation to direct future research in this field and establish rigorous measurement techniques for EV flow. In addition, we included participants in various stages of the menstrual cycle, with menstrual cycle staging estimated using patient reported information. We did not exclude participants taking hormonal medications as an ideal endometriosis biomarker would perform accurately independent of menstrual cycle stage or hormonal medication use. Nonetheless, this heterogeneity may have affected our ability to detect differences between groups.
Further heterogeneity was introduced from the use of a symptomatic control group, where some participants had no other pathologies identified, others had benign pathologies not matched to the endometriosis cohort, and some reported previous surgical confirmation of endometriosis. However, we view this as a strength – our control group was chosen as to evaluate our proposed markers in clinically relevant cohorts in which a biomarker would ultimately be applied.
The emerging evidence for the role of EVs in endometriosis pathophysiology has generated excitement for their potential as non-invasive diagnostics. 9 However, the results of this study suggest the techniques developed here may have greater application to pathophysiological studies. This technology takes significant time, cannot be automated, and requires rigorous scientific optimisation. Future biomarker studies may benefit from technical innovations to EV detection platforms, such as surface-enhanced Raman spectroscopy biosensors, 52 which demonstrate improved multiplexing capabilities, positioning them as promising tools for increasing sensitivity to detect clinically informative EV populations. Further studies could include increasing the sample size to include control of biological variables which is a common challenge in endometriosis research.
Supplemental Material
sj-docx-1-pev-10.1177_22840265261458937 – Supplemental material for Spectral flow cytometry of plasma and cervicovaginal fluid extracellular vesicles for diagnostic endometriosis biomarkers
Supplemental material, sj-docx-1-pev-10.1177_22840265261458937 for Spectral flow cytometry of plasma and cervicovaginal fluid extracellular vesicles for diagnostic endometriosis biomarkers by E. S. J. Paterson, S. Scheck, S. McDowell, G. Roopi, N. Bedford, J. E. Girling and C. E. Henry in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Acknowledgements
We thank Richard Easingwood and Dr Fátima Jorge at OMNI Electron Microscopy for carrying out the cryo TEM. Thank you to the participants and their whānau for their generous contribution to this work. Open access publishing facilitated by University of Otago, as part of the SAGE – University of Otago agreement via the Council of Australian University Librarians.
Ethical Considerations
This study was approved by the Central Health and Disability Ethics Committee (HDEC) (2022 EXP 12616), received endorsement from the Research Advisory Group – Māori (RAG-M) at Te Whatu Ora – Capital and Coast (#937) and local approval from Te Whatu Ora – Capital and Coast research and audit committee. All participants provided written informed consent to participate in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Wellington Medical Research Foundation.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability Statement
Data is available from the NanoFlow Repository.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.