
Abstract
The superficial injection needling botulinum (SINB) technique is the dermal injection of microdoses of botulin toxin, not by traditional syringe but with needling technique that consists in multiple microdroplets by electrical device. The intention is to decrease sweat and sebaceous gland activity to improve skin texture and sheen and to target the superficial layer of muscles that find attachment to the undersurface of the dermis causing visible rhytides. The technique is for treatment of face and neck by the injection of the botulin toxin into the dermis or in subdermal plane to improve skin texture, smoothen horizontal creases, and decrease vertical banding of the neck as well as to achieve better apposition of the platysma to the jawline and neck, improving contouring of the cervicomental angle. The botox solution is hyperconcentrated when compared to traditional dilution or compared to microbotox or mesobotox. Furthermore, the injection technique is different because spreading superficial microdroplets are not performed, but small, homogeneous, and controlled amounts of solution are injected. Each 0.8-mL syringe contains 50 units of onabotulinumtoxinA. The solution is delivered intradermally, using an electrical needling pen and setting the depth penetration of the needles at 3 to 3.5 mm. The 2 conjugated techniques play a 2-fold action on the skin. The technique was applied to a group of 63 patients dealing with face, forehead, cheekbones, and neck.
Introduction
Superficial injection needling botulinum (SINB) consists of 2 techniques that, in concert, have a dual effect. The purpose of this technique is to act on the sebaceous glands in the skin and the surface area of the facial muscles. This technique is different in concept and approach from the intradermal techniques that have been published so far. 1 –4
The method may seem similar to mesobotox or microbotox. However, botulinum toxin is not hyperdiluted and applied with intradermal injection through syringe as in the other techniques. In this technique, botulinum toxin is hyperconcentrated and applied with a series of microneedles that, by bathing with the reconstituted botulinum toxin, make it penetrate in very small quantities and homogeneously. This technique was developed by the author Francesco Calvani, and it is not performed with a specific toxin but using those commercially available with the same dilution.
Needling is a technique consisting of a cutaneous micro perforation with a device consisting of a handpiece and a head with microneedles. The number of needles and the possible depth of setting may vary depending on the manufacturer.
It has been observed that the microtrauma induces the production of growth factors by multiplication of fibroblasts and the synthesis of collagen and elastin. 5,6 Therefore, the technique presented has this dual action.
Materials and Methods
Sixty-three patients (51 women and 12 men) aged between 26 and 71 were recruited. All patients were subjected to SINB. The effects induced by botulinum toxin in the skin layer were evaluated by pre- and postskin checkups, patient’s life habits, skin laxity evaluation, and aesthetic requirements of the patient. Informed consent was obtained from all individual participants included in the study.
The various pharmaceutical formulations of botulinum toxin serotype A (onabotulinum toxin-A, abobotulinum toxin-A and incobotulinum toxin-A), marketed in lyophilized form, were resuspended in saline solution for injection (0.9% NaCl). Resuspensions were made by reducing the amounts suggested by the manufacturers, according to dilutions based on personal experience. The dilutions carried out in our study are reported in Table 1.
The Dilutions of Botulinum Toxins Serotype A Used in the Study.

Abbreviations: IU, international units; mL, milliliter; NaCl, sodium chloride.
The dermapen used was set with a 24-needle head with a depth of 3.0 mm extended to 3.5 mm. Forty minutes before the infiltration, patients were prepared with anesthetic cream applied on the areas to be treated, cream removal, and disinfection by hydrogen peroxide.
After disinfection, patients were washed with sterile gauze soaked in 0.9% sterile saline. After thorough drying, we started by delineating the area to be treated in the session.
The treated areas and the amount of toxin used were standardized. The face area was separated from the neck and jaw, and a grid was created based on the size of the head diameter of the instrument used (Figure 1).

Division grid for botulinum toxin. The grid is drawn according to the size of the head of the needling pen, which in this case has a 1-cm diameter.
It is possible to divide the treated area into quadrants. In this case, the amount of recombined toxin in the physiological solution is divided by the number of quadrants. The dilution does not change. Another technique is to divide the area by building a grid. Each grid unit must have the size of the head of the device that you want to use. In our case, a head with a 1-cm diameter has been used throughout the treated area (Figure 1). The maximum amount of toxin used in a full-face session is equivalent to 100 units recombined in 1.6 mL of saline. This amount was injected homogeneously across the surface marked by the grid.
The Technique
The technique involves treating, in a session, the areas selected and divided as mentioned earlier by dropping a drop of resuspended botulinum (10 µL) on the skin and immediately placing the dermapen firmly above the liquid on the same spot for 3 seconds measured by a digital chronometry (Figure 2). Around 3000 perforations per area were applied (the medical device performs around 60.000 perforations/min).

Botulinum toxin is injected via needling pen.
A moderate pressure is applied with the device on the skin area. On bony prominences, it was necessary to pinch the skin with the fingers to move it up from the underlying bone. On the other hand, we did not find it difficult to apply the technique on the neck areas.
This procedure is repeated throughout the area outlined until the end of the treatment. In order to better dose the drops, a 0.5-mL insulin syringe with 30-g needle was used. This allows the formation of very small drops, because the thin needle and the easy-to-maneuverable syringe are a good aid to the operator and allow a homogeneous distribution. Obviously, the technique required an expert and delicate hand. It is advisable to try with a pure physiological solution to accurately calibrate the strength of the hand on the plunger of the syringe and, only after some attempt, to begin to apply the recombinant botulinum toxin. A circular plastic structure that guides the needles and acts as a stop for the set depth helps the applied skin drop to stay in the treated area.
There are essential factors for the penetration of the greatest number of botulinum toxin into the tissue and thus having the desired effect. The moderate pressure, which helps to increase the depth of the head; the adopted dispenser consisting of a 0.5-mL syringe and 30-g needle, allowing the formation of small drops; and a 3-second needle application time, which helps to increase the microtrauma, the perforation, and the intake of toxin within the dermis.
To increase the duration of treatment time, the protocol was standardized with 3 sessions for 3 months. The first session with the technique described, while the latter 2 with the same technique without administering toxins but only with the tissue trauma of needling.
Follow-Up Period
All patients were followed monthly for 6 months. At the end of the follow-up period, all patients repeated the procedure from the beginning.
Evaluations
To evaluate the improvements and eventual complications during the follow-up, we used the photographic documentation acquired before and after the treatment.
Results
All treated patients experienced improved skin elasticity, reduced laxity of the chinrest area and skin folds of the neck, reduced skin touch imperfections, and smoother skin (Figures 3 –5). There were no main complications. Immediately after the treatment, there was a reddening of the treated areas, with gentle swelling that lasted from 1 to 4 hours, depending on the skin treated. The reddening of the skin lasted no more than 48 hours. Patients did not experience any discomfort when returning to the workplace after treatment. Obviously, the use of cheats and correctors on the treated areas was forbidden for 24 hours. The treatment did not produce ecchymosis requiring cosmetic camouflage. All patients underwent home disinfection of the treated areas for the first night with 10-volume hydrogen peroxide application, without applying cosmetic creams.

Forty-three-year-old woman. Note accentuation of the mandibular profile and the neck.

Forty-four-year-old woman. Note accentuating skin elasticity with double chin reduction.
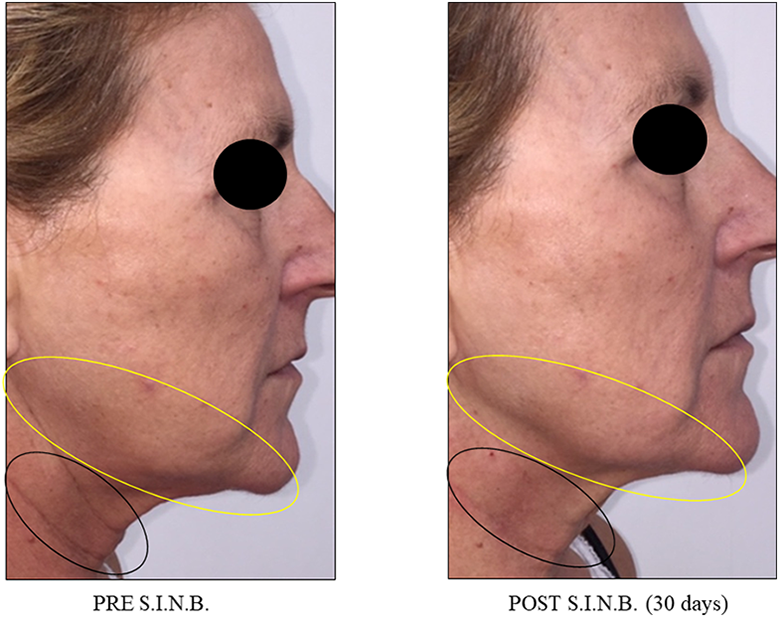
Sixty-four-year-old woman. Note reduction in neck folds and accentuation of the mandibular profile.
In 5 patients, there was slight skin sensitivity to touch for a few days. All patients applied, after treatment, total solar screen for about 1 week. The first visible results were observed between the 7th and 10th days after treatment.
Clinically, a smoother and shiny skin was observed in all treated areas, a more marked delineation of the jaw and neck and an improvement in face and neck wrinkles, resulting in a cleaner appearance (Figures 3 –5). Patients reported a feeling of greater skin elasticity with improved neck and jaw tightness.
The duration of improvement after SINB usually lasts 3 to 4 months. The protocol we adopted, which includes other 3-week needling sessions repeated twice, amplifies the result by increasing the time of improvement up to 5 to 6 months from the start of the treatment, without the need for additional sessions.
Discussion
The world of aesthetics is constantly evolving. Biochemical and pharmaceutical technology are increasingly offering a wide assortment of new molecules. Techniques are constantly evolving, especially for this wonderfully used molecule in different areas.
Wu 7 –13 proposed the microbotox technique, an injecting technique of botulinum toxin type A (BoNT/A) microdoses for treating the signs that time draws on the face (lower third), periorbitary, on the forehead, and on the neck. He introduced the platysma effect; the technique improves the mandibular profile, reduces the skin’s laxity, softens the dynamic wrinkles (those caused by the hypertonia of the mimic muscles), and an increase in gloss and more polished skin is noted without the notorious plasticization of the aesthetic appearance. 7 –13
The microbotulin is characterized by a greater dilution of type A neurotoxin and by the fact that the injections are performed intradermally. Thirty grams 4- or 12-mm needles and 1- mL syringes are used. By making intradermal injections, the flaccid paralysis that occurs only affects the superficial muscle fibers of the mimic muscles innervated by the seventh pair of cranial nerves, the facial nerve. In short, the function of mimic muscles is largely preserved while achieving an appreciable clinical outcome.
The areas of the face and neck to be treated must be well identified and marked with a dermograph marker indicating the various districts. The technique adopted for this work, unlike microbotox, contemplates a hyperconcentration and not a hyperdilution. Moreover, the inoculation technique is different because in our technique no infiltration needles are used. Recombined toxin is not mixed with local anesthetic.
Permatasari et al in 2014 14 demonstrated in vitro that botulinum toxin not only has a skin effect on texture and thickness but also on photoaging. The results of this study indicate that BoNT/A significantly antagonizes UV-B-induced early senescence in human dermal fibroblast (HDF) in vitro. Therefore, the BoNT/A intradermal injection potential as photoaging treatment can be valid.Bonaparte et al in 2015, 15 in a study of 48 patients, explained the effect of botulinum toxin on the skin, describing the alteration in elasticity and viscoelasticity after treatment. Zhang et al in 2016 16 have shown that treatment with botulinum toxin at the skin level of facial maxillary scars is a valuable aid for better scarring, as it is possible to treat post acne scars with cutaneous micro infusions.
Ziade et al, 17 instead, highlighted the action of superficial muscle fibers on tension vectors acting on the edges of traumatic wounds. These are transmitted to immature collagen fibers synthesized during the normal healing phase. This causes enlargement of the scar as well as hypertrophic and hyperplastic scars. 18 The aim of the work was to reduce tension vectors on the edges of the wound and to improve the scarring of facial wounds with botulinum toxin application.
It has been concluded that botulinum toxin decreases and improves the cosmetic wounds. 19 Other authors have suggested that skin thinning and increased tonicity can improve the appearance of the face in a very natural way. 20,21
Our technique has been tested on participants between the ages 31 and 67. For too long, botulinum toxin has been proposed to over 50 patients considering it as a “last beach” treatment, although it has never really been this way.
The technique adopted by us is far from being synthetic and inexpressive. The result obtained on all patients is visible but natural; the level of satisfaction was outside any expectation. Of the 63 patients, anyway, only 2 were not satisfied and did not note any subjective improvement, while the remaining sample was fully satisfied and would recommend treatment to other patients. It should be noted, however, that this remains a combined treatment. Needling has been widely studied in the literature.
Fabbrocini et al in 2014 22 published the dermapen posttreatment effects on patients with acne scars. In 2011, the same authors published an article about neck rejuvenation with the same technique, highlighting an increase in elasticity and attenuation of the signs of time. 23 Aust et al 24 –27 have shown how mechanical skin insult leads to induction of collagen fiber production and how this could have effects on tissue elasticity.
El-Fakahany et al 28 have conducted a study on perception of pain with the aid of micro-vibrations. There was a reduction in pain perception when the treated area was subjected to vibration. Therefore, the treatment we adopt also presents a good patient compliance, as it is almost painless.
In light of what has been studied and so far reported in the literature, there are no contraindications to our technique. The purpose of this technique is to blend 2 different methods that are so valuable to improve skin texture, to treat premature blemishes that do not always require more important therapies, to improve regulation of the sebum of the sebaceous glands, and to give the participants a fresher look, with a refined and elegant change.
Conclusion
In the light of the literature, of the proposed and applied technique and the results achieved, we believe that SINB is a possible variant of botulinum techniques so far known. In addition, this technique combines on the one hand the stimulation of new collagen in the long term and on the other faster effects. These latter include improved mandibular profile, reduced skin laxity, attenuation of dynamic wrinkles caused by hypertonia of mimic muscles, increased gloss, and a smoother skin without causing the notorious plasticization of the skin’ aesthetic appearance.
This technique is also well tolerated by younger patients who are often borderline to traditional techniques. Additionally, the result is confirmed by the patients themselves who would recommend this treatment to other people.
Footnotes
Level of Evidence
Level 5, Therapeutic
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.