
Abstract
Purpose:
This study determined the prevalence of Alzheimer’s disease and related dementias (ADRD) and associated modifiable risk factors among transgender adults in South Carolina.
Methods:
This retrospective analysis of all-payer hospital claims data from South Carolina (2000–2022) included adults aged ≥18 years. ADRD and risk factor prevalence were estimated overall and stratified by age group (18–49 and ≥50 years). Transgender adults and ADRD diagnoses were identified using International Classification of Diseases codes. Results were compared to state prevalence rates.
Results:
Among 1160 transgender adults, ADRD prevalence was 19.4% among those aged ≥50 years and 1.3% among those aged 18–49 years; depression (61.7%), smoking (49.6%), and hypertension (38.2%) were the most common risk factors.
Conclusion:
Transgender adults in South Carolina experience a substantial burden of ADRD and modifiable risk factors, warranting targeted and culturally competent interventions for this population.
Introduction
Alzheimer’s disease and related dementias (ADRD) are leading causes of morbidity and mortality in the United States, affecting over 6 million Americans. 1 Although the burden of ADRD is substantial across all populations, emerging evidence suggests that transgender adults experience disproportionately high risks and distinct challenges related to cognitive decline.2–4 U.S. studies have found higher prevalence of ADRD and subjective cognitive decline (SCD) among transgender and gender nonbinary adults compared to cisgender peers, with increased rates of functional limitations and unmet care needs.3,5
South Carolina faces a significant ADRD burden, with 11% of residents aged 65 and older living with dementia and prevalence reaching 54% among those aged 85 and older. 6 Black South Carolinians aged 65 or older are 45% more likely to be living with dementia compared to their peers. 6 The Southern U.S., including South Carolina, is home to the largest proportion of sexual and gender minority adults in the country, yet there is a notable lack of population-based data on ADRD prevalence and risk factors among transgender adults in this region.
The 2024 Lancet Commission on dementia prevention, intervention, and care identified 14 potentially modifiable risk factors, including less education, hearing loss, hypertension, smoking, obesity, depression, physical inactivity, diabetes, excessive alcohol consumption, traumatic brain injury, air pollution, social isolation, and the newly added untreated vision loss and high low-density lipoprotein cholesterol, that together account for nearly 45% of dementia cases worldwide. 7 The Commission further noted that the burden of these modifiable risk factors is disproportionately higher among minoritized and lower socioeconomic groups and that cisgender men and women generally carry fewer risk factors for dementia in late life than do transgender men and women.2,7 Transgender adults are exposed to a range of social and health-related risk factors, such as discrimination, social isolation, chronic stress, and higher rates of chronic diseases, including diabetes, hypertension, and obesity, that are known contributors to cognitive decline and dementia.8,9 The Alzheimer’s Association has identified ADRD as a high-priority disease for transgender individuals, emphasizing the urgent need for inclusive research and intervention. 1 This study aimed to address this critical knowledge gap by examining the prevalence of ADRD and associated modifiable risk factors among transgender adults in South Carolina by leveraging statewide linked administrative data.
Methods
South Carolina integrated data system
We utilized the South Carolina Integrated Data System, managed by the South Carolina Revenue and Fiscal Affairs Office (RFAO). 10 Agencies voluntarily share their data under statute and formal agreements, with explicit project-by-project approval for each use. This system aggregates data from diverse state agencies (see participating entities in Fig. 1), including health care, education, and service delivery, allowing for comprehensive longitudinal analyses. Because inclusion in the integrated data system depends on individuals’ interaction with participating agencies and programs, the dataset primarily captures people who engage with state health and service systems. As a result, individuals who have limited contact with health care or other state-supported services in South Carolina may be underrepresented.
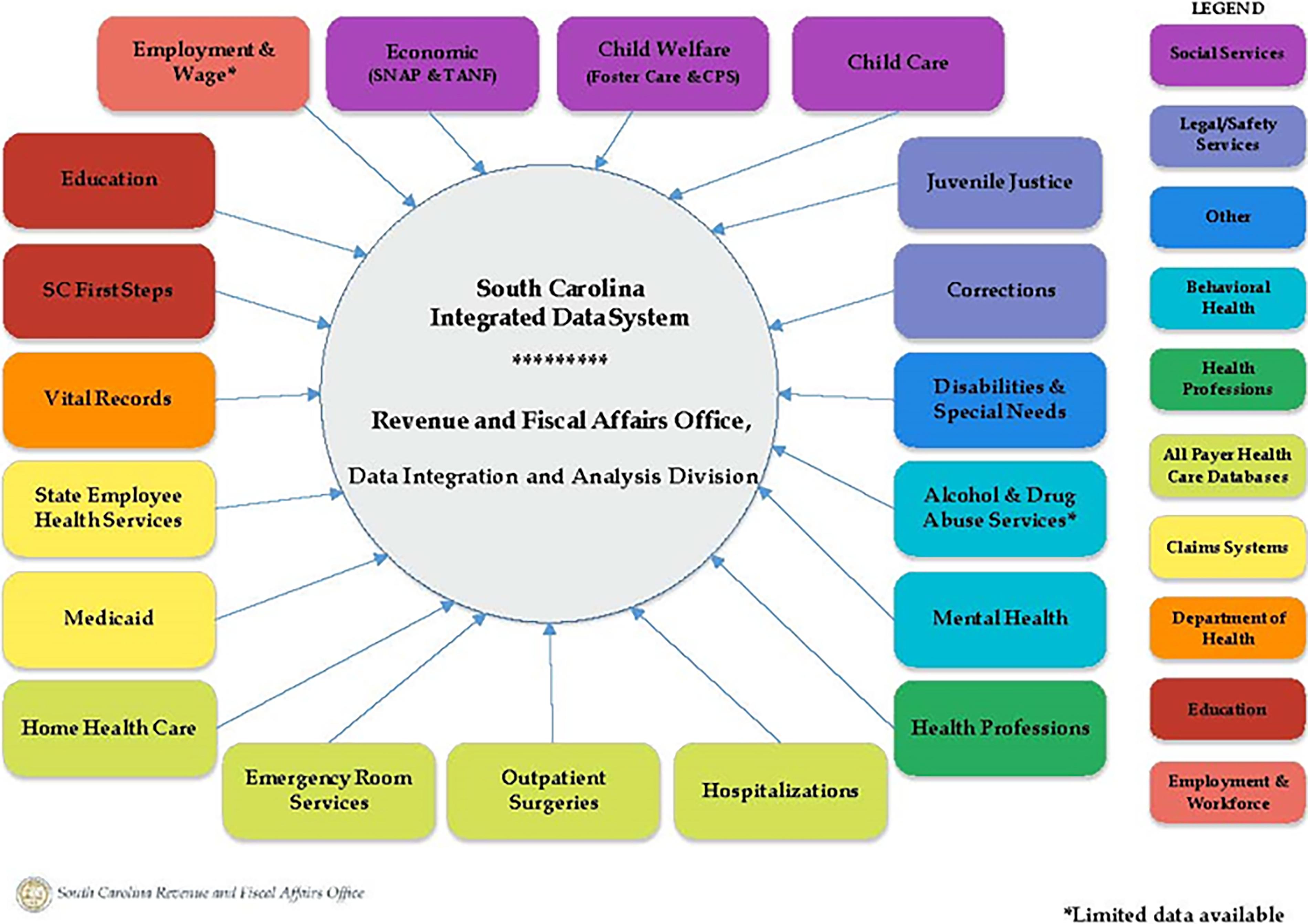
Figure of the available data in the South Carolina Integrated Data System. Used with permission by the South Carolina Revenue and Fiscal Affairs Office. CPS, Child Protective Services; SC, South Carolina; SNAP, Supplemental Nutrition Assistance Program; TNAF, Temporary Assistance for Needy Families.
To access the deidentified data, researchers must apply for each project. Once the application is approved by RFAO, the de-identified data is gathered based on the requesting inclusion and exclusion criteria and sent by RFAO to the requestor via a secured, encrypted file. For this project, our approved data request included only individuals meeting the computable phenotype for transgender status as described below. The study received ethical approval from the University of South Carolina’s Institutional Review Board (Pro00133266) on November 11, 2023. This is an IRB-approved retrospective study; all patient information was deidentified, and patient consent was not required. Patient data will not be shared with third parties.
Transgender data
The RFAO dataset contains encrypted patient identifiers for longitudinal tracking. Transgender adults were identified by RFAO using a computable phenotype based on International Classification of Diseases, Ninth Edition (ICD-9) 11 and Tenth Edition (ICD-10) 12 diagnosis codes (see Table 1), as described in prior research. 13 ADRD was defined using ICD-9 and ICD-10 codes for Alzheimer’s disease, vascular dementia, and other non-Alzheimer’s dementias, as detailed in Supplementary Table S1. We then analyzed this dataset for ADRD and associated risk factors using ICD-9 11 and ICD-10 12 codes (see Supplementary Table S2), as defined by the Chronic Conditions Warehouse. 14
Transgender International Classification of Diseases, Ninth Edition and International Classification of Diseases, Tenth Edition Codes
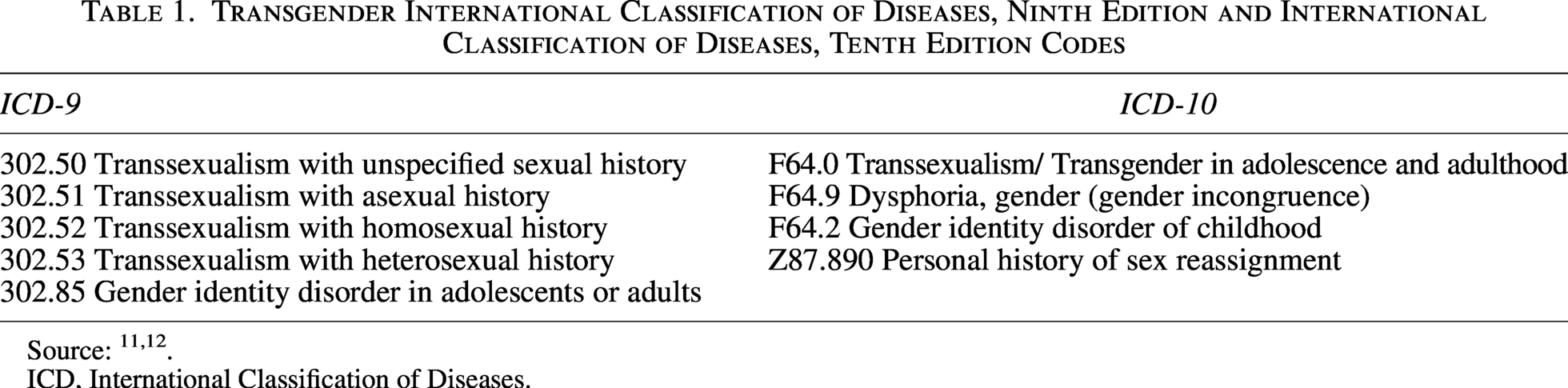
ICD, International Classification of Diseases.
Risk factors of interest
We identified ADRD risk factors from (1) the 2024 Alzheimer’s disease facts and figures special report; 1 and (2) the 2024 Lancet Commission on dementia prevention, intervention, and care. 7 For the 11 risk factors that we could identify in our dataset (i.e., alcohol use disorder, depression, diabetes, hearing impairment, hypercholesterolemia, hypertension, obesity, sleep disorder, smoking, traumatic brain injury, and visual impairment), we compiled ICD-9 11 and ICD-10 12 diagnosis codes using the Chronic Conditions Data Warehouse 14 criteria. Cases were included in our final dataset if a patient’s record contained at least one ICD-9 11 or ICD-10 12 code for transgender status, ADRD, and any risk factor. Prior to data delivery, we requested that the RFAO categorize patients as metropolitan or rural using 2010 Rural-Urban Commuting Area Codes (RUCA). 15
Data analysis
We conducted a secondary analysis of deidentified all-payer hospital claims data from 2000 to 2022, including adults aged 18 and older. Consistent with prior claims-based research on ADRD in transgender populations, 3 we included all adults aged 18 years and older to capture early-onset ADRD diagnoses and stratified results by age group (18–49 and ≥50 years) to allow age-specific prevalence estimation. In line with life-course frameworks for modifiable dementia risk, we examined the prevalence of ADRD risk factors among all adults aged ≥18 years and by age group (18–49 and ≥50 years).
Patients were classified as residing in metropolitan or rural areas using 2010 RUCA codes. 15 The primary outcomes assessed were the prevalence of ADRD and the distribution of the 11 modifiable risk factors identified above. Demographic variables considered included age, race/ethnicity, and urban-rural residence. Prevalence rates for ADRD and each risk factor were calculated as the proportion of the individuals diagnosed with the condition, both overall and stratified by age (18–49 and ≥50 years). Descriptive statistics summarized patient characteristics, ADRD diagnoses, and risk factor prevalence. All statistical analyses were conducted using SAS version 9.4. 16
South Carolina Alzheimer’s disease registry
To contextualize our findings, we contacted the director of the South Carolina Alzheimer’s Disease Registry, which also leverages the South Carolina Integrated Data System, and requested an estimate of ADRD prevalence among all adults aged 50 years and older in South Carolina. This registry-derived prevalence served as a statewide reference point for comparison.
Results
A total of 1160 transgender adults were identified in the South Carolina RFAO dataset from 2000 to 2022 (Table 2). The majority (81.8%) were aged between 18 and 49 years at their first recorded encounter, whereas 18.2% were aged 50 or older. Most individuals resided in urban areas (83.53%) and identified as White (69.3%), followed by African American or Black (24.4%) and other or declined to state (6.3%).
Transgender Adult Diagnosis of Alzheimer’s Disease and Related Dementias and Modifiable Risk Factors in South Carolina Revenue and Fiscal Affairs Office Data: 2000–2022 (N = 1160)
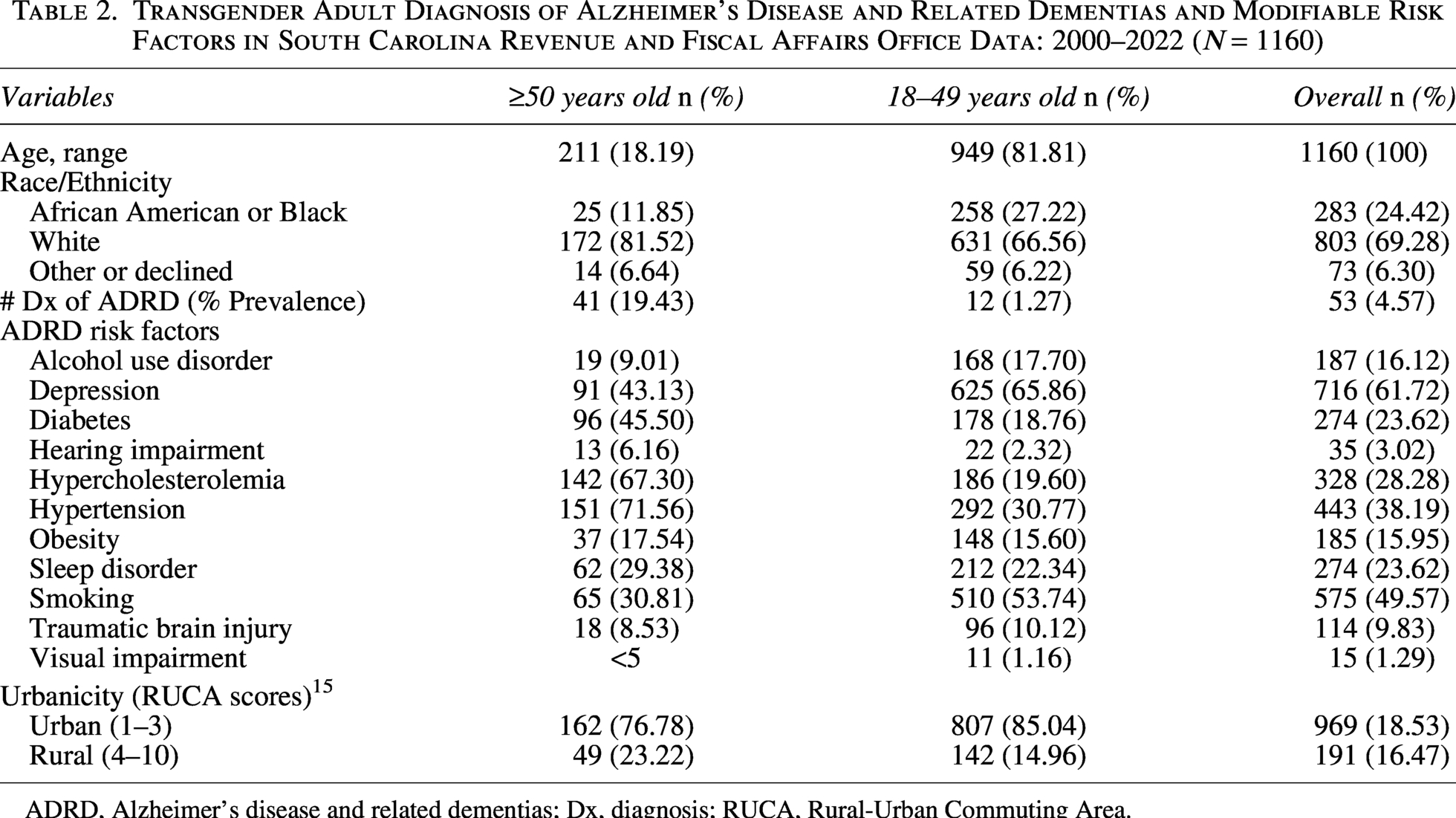
ADRD, Alzheimer’s disease and related dementias; Dx, diagnosis; RUCA, Rural-Urban Commuting Area.
Among 1160 transgender adults, 53 had an ADRD diagnosis. ADRD prevalence was 19.4% among those aged ≥50 years and 1.3% among those aged 18–49 years; overall prevalence in the full 18+ sample was 4.6%. The burden of modifiable risk factors for ADRD was considerable in this population. Depression was the most common risk factor, affecting 61.7% of the cohort, with smoking (49.6%) and hypertension (38.2%) also highly prevalent. Other notable risk factors included hypercholesterolemia (28.3%), diabetes (23.6%), and sleep disorders (23.6%).
Risk factor prevalence varied by age group, with hypertension 71.6% among those aged 50+ versus 30.8% among those under 50. Similarly, hypercholesterolemia affected 67.3% of those aged 50+ versus 19.6% of those under 50, and diabetes was diagnosed in 45.5% of those aged 50 and above, compared to 18.8% among younger adults. In contrast, depression and smoking were more prevalent among transgender adults under 50 years, with rates of 65.9% and 53.7%, respectively, highlighting distinct age-related patterns in risk factor burden within this population.
Per the director of the South Carolina Alzheimer’s Disease Registry, from the years of 2005 to 2022, “the prevalence of ADRD in South Carolina of all adults aged 50 and older is 3.85%.” (personal communication reported with permission, May 15, 2026). This is based on registry data from 2005 to 2022.
Discussion
This study provides the first population-based analysis of ADRD prevalence and associated risk factors among transgender adults in South Carolina. Our findings align with U.S. research indicating that transgender individuals have a higher prevalence of cognitive decline and dementia.3,8,17 The higher prevalence of ADRD in this population may be attributable to a confluence of social determinants, including discrimination, health care barriers, and chronic disease burden.
Comparison to U.S. data
Our findings reveal an overwhelming disparity in ADRD prevalence among transgender adults in South Carolina. The observed 19% prevalence in this cohort is notably higher than the 3.85% and 13% prevalence of ADRD reported among adults aged 50 and older within South Carolina 6 and the U.S. population, 18 respectively. This represents a prevalence rate more than five times greater than that of the general aging population in South Carolina and approximately 46% greater than that of the U.S. population, highlighting a significant and previously unquantified public health crisis for this group in the state.
Although direct U.S. comparisons for diagnosed ADRD in transgender populations are limited, our data are consistent with and extend previous research. Studies have consistently identified high rates of SCD and related functional limitations among transgender adults compared to cisgender adults.5,8,17 Furthermore, our results build upon findings from Florida, where Guo et al. 3 also identified a significantly higher prevalence of ADRD (1.7% vs. 0.8%) and a greater burden of modifiable risk factors in its transgender population. 3 The magnitude of the disparity observed in South Carolina suggests that regional factors, including limited access to culturally affirming health care and heightened exposure to social stressors, may exacerbate the underlying risks driven by systemic inequities. 17 These potential mechanisms need to be evaluated further in future research. Although our study population was restricted to transgender adults and did not include a directly comparable cisgender cohort extracted from the same analytic dataset, the comparison to state-level prevalence estimates provides valuable context for interpreting the magnitude of this health disparity.
Because our ADRD prevalence estimates among transgender adults aged 50 years and older aggregate data from 2000 to 2022, they reflect a cohort observed during a period of substantial demographic, clinical, and documentation change. Over this interval, the number of transgender adults surviving into later life and engaging with health systems likely increased, and the age distribution of transgender adults in care may have shifted toward older ages, which would be expected to increase crude ADRD prevalence even if age-specific risks remained stable. Concurrently, evolving dementia awareness, diagnostic practices, and coding conventions, including transition from ICD-9 to ICD-10 and improved ascertainment of transgender status in administrative data, may have increased capture of both transgender identity and ADRD, such that apparent temporal changes in prevalence may partly reflect differences in documentation and health care access rather than underlying disease.
Implications
The results of this study emphasize the importance of addressing the unique challenges encountered by transgender adults in relation to ADRD. Transgender individuals are disproportionately exposed to risk factors such as social isolation, discrimination, and barriers to health care access, 19 all of which may exacerbate developing ADRD. In addition, chronic diseases such as diabetes, hypertension, and obesity, which are prevalent in transgender populations due to systemic inequities, 19 further compound their risk. Recent work also demonstrates that these modifiable conditions translate into higher dementia risk scores among transgender and gender-diverse adults. Brady et al. 2 found that transgender men, transgender women, and nonbinary adults had higher late-life Alzheimer’s disease risk scores than cisgender adults, driven in part by higher prevalence of depression, hypertension, hypercholesterolemia, and smoking in transgender and gender-diverse groups. The high burden of depression, tobacco use, and hypertension observed in our cohort is therefore likely to contribute meaningfully to ADRD risk across the life course for transgender adults in South Carolina. Our findings indicate the need for targeted interventions and culturally competent care strategies tailored to the needs of transgender adults.
Our findings have important implications for public health and policy. The Alzheimer’s Association has declared ADRD a high-priority disease for transgender individuals, emphasizing the need for inclusive health care practices and research. In South Carolina, where a significant proportion of the population resides in rural areas with limited access to specialized care, 20 it is necessary to develop policies that address these disparities. Public health initiatives should focus on increasing access to early screening and diagnosis for transgender individuals while addressing modifiable risk factors through community-based programs that promote cardiovascular health, mental well-being, and social engagement.
Limitations
A key strength of this study is that the use of a statewide data set with longitudinal tracking capabilities allowed us the opportunity to conduct a comprehensive analysis of ADRD prevalence in transgender adults over time. However, there are limitations. The use of ICD codes to identify transgender individuals may not capture all members of the population due to underreporting and misclassification. In addition, although our inclusion criterion of age 18 and older is consistent with the approach used by Guo et al., 3 the relatively low base rate of ADRD among younger adults means that diagnoses in the 18–49 age group should be interpreted with caution, as they may reflect early-onset dementia or coding variability rather than typical age-related ADRD.
In addition, our reliance on ICD codes to identify both transgender status and ADRD spans a period of substantial change in diagnostic classification and social norms. Over 2000–2022, the transition from ICD-9 to ICD-10, along with the introduction and refinement of codes related to gender identity and dementia, likely altered how clinicians documented transgender identity and ADRD. Increasing awareness and acceptance of transgender populations may have further increased the likelihood that these identities and diagnoses were recorded. Consequently, ascertainment of transgender status and ADRD likely improved over time, so part of the observed burden in our aggregated 2000–2022 estimates may reflect evolving documentation and coding practices rather than solely changes in underlying disease risk.
Although this study describes the prevalence within South Carolina, our approved data extract did not include a cisgender comparison cohort, precluding calculation of internal, age-adjusted prevalence ratios comparing transgender and cisgender adults using the same analytic dataset. This limits our ability to directly quantify the disparity within a single controlled analysis and constrains broader generalizability to other states. Finally, our data arise from an all-payer database based upon hospital and outpatient surgery encounters in South Carolina. This will not include individuals whose care does not utilize these services during the observation period. Hence, it may be that our prevalence estimates are underestimated.
Future directions
The findings from this study have implications that extend across research, clinical practice, and public health policy. The disproportionate burden of ADRD among transgender adults in South Carolina necessitates a multi-pronged response to move from identifying this disparity to actively dismantling the systems that perpetuate it. Future research must first establish a precise baseline of risk by conducting direct comparisons with the cisgender population in South Carolina within the same analytic dataset, using the same stratification or adjustment, to precisely quantify the disparity in ADRD prevalence and associated risk factors. Subsequently, investigators should explore the mediating and moderating factors, such as social determinants of health, chronic stress, and the compounded effects of intersectional identities such as race and rurality, to highlight the mechanisms driving this health inequity. In parallel, these findings call for immediate clinical action through the integration of routine, culturally sensitive cognitive screening into primary care for transgender adults. 21 Ultimately, sustainable solutions will depend on developing community-partnered interventions that are co-designed with transgender individuals to promote resilience and address modifiable risks within a culturally relevant and affirming framework.
On a broader scale, public health policy must evolve by mandating the inclusion of sexual orientation and gender identity (SOGI) data 22 in all health surveillance systems to ensure disparities are consistently monitored. 21 As the collection of SOGI data becomes an essential component of health equity efforts, prioritizing privacy protections and implementing rigorous data security protocols will be critical to safeguard the well-being of transgender individuals. Some communities may experience heightened concerns regarding disclosure and potential misuse of sensitive personal information; therefore, clinicians, researchers, and policymakers must advocate for and adhere to best practices in confidential and voluntary SOGI data collection to ensure that patient trust is not compromised and that data are used solely to advance health equity and improve clinical outcomes.
Conclusion
This study provides the first population-based evidence of a profound health disparity, revealing that transgender adults in South Carolina face a disproportionately high burden of ADRD. The elevated prevalence of ADRD and its associated modifiable risk factors for this population is not a biological inevitability but rather a manifestation of systemic inequities, including health care discrimination, social marginalization, and chronic stress. Addressing this public health crisis requires a concerted effort to move beyond mere surveillance toward transformative action: implementing culturally competent clinical care, mandating inclusive public health data collection, and co-designing community-based interventions that decrease the structural barriers to cognitive health and advance health equity for all transgender South Carolinians.
Authors’ Contributions
J.T.M.: Conceptualization, methodology, data curation, supervision, writing—original draft and review and editing; H.S.: Formal analysis, methodology, writing—original draft and review and editing; S.A.A.: Methodology, supervision, writing—original draft and review and editing; M.L.: Writing—methodology, supervision, original draft and review and editing.
Data Availability
The data supporting the findings in this study are derived from the South Carolina Integrated Data System and are not publicly available due to privacy and data sharing restrictions. Requests for de-identified data access can be directed to the South Carolina Revenue and Fiscal Affairs Office and will be evaluated in accordance with institutional policies and state regulations.
Disclaimer
This information is from the records of the South Carolina Revenue and Fiscal Affairs Office, Data Integration and Analysis Division. Our authorization to release this information does not imply endorsement of this study or its findings by either the Revenue and Fiscal Affairs Office or the Data Oversight Council. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical Considerations
The study received ethical approval from the University of South Carolina’s Institutional Review Board (approval Pro00133266) on November 11, 2023. This is an IRB-approved retrospective study, all patient information was deidentified and patient consent was not required. Patient data will not be shared with third parties.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Footnotes
Acknowledgments
The authors would like to thank the South Carolina Revenue and Fiscal Affairs Office for the data used in this analysis. They would also like to thank the South Carolina Alzheimer’s Disease Registry for assisting them in state prevalence information.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Statement
Research reported in this publication was supported by the NIH
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.