
Abstract
Background:
The acetabular labrum plays a critical role in maintaining the hip suction seal, joint stability, and load distribution. When primary repair is not feasible, augmentation is preferred if the chondrolabral junction can be preserved, whereas reconstruction is performed when it cannot. However, biomechanical studies evaluating the effects of graft geometry and labral preservation strategies on suction seal restoration remain limited.
Hypothesis/Purpose:
It was hypothesized that augmentation using an extended graft combined with partial labral preservation would restore femoroacetabular suction seal strength more effectively than standard reconstruction after labrum excision. This study compared the biomechanical outcomes of different graft labral height and preservation width configurations in an ovine hip model.
Study Design:
Controlled laboratory study.
Methods:
A total of 48 fresh-frozen ovine hemipelvises were randomized into 6 groups (n = 8) according to labral preservation width, excision pattern, and graft radial height. Autologous extensor tendon grafts with standard or extended labral height were fixed to standardized segmental defects using suture anchors. The suction seal force was defined as the linear distraction force required to disrupt the femoroacetabular seal and measured in intact, excised, and reconstructed states. Restoration was defined as deviation from the intact condition and improvement relative to the excised state. Intergroup comparisons were performed using nonparametric tests with Bonferroni correction (P < .003).
Results:
The configuration combining one-third native labral preservation with an extended graft demonstrated the smallest deviation from the intact condition (3.8 N) and the greatest improvement relative to the excised state (18 N), showing significant superiority compared with the total excision plus standard graft construct (P≤ .002). The configuration involving one-half labral preservation with a standard graft did not differ significantly from the extended graft group in terms of improvement (P = .115) and exhibited a relatively small deviation from the intact condition (6.6 N). Rim trimming performed within anatomical boundaries did not compromise suction seal integrity.
Conclusion/Clinical Relevance:
Partial labral preservation combined with increased graft labral height provided the most favorable biomechanical restoration of femoroacetabular suction seal strength.
The acetabular labrum plays a critical role in hip joint biomechanics due to its functions such as vacuum effect (suction seal), joint stability, and load distribution.4,5,7,8 Labral tears are one of the most common pathologies encountered in conditions that form the basis of hip-preserving surgery, such as femoroacetabular impingement syndrome.9,40 Therefore, restoration of the labral tissue is a decisive factor in the success of arthroscopic hip surgery.22,26,30
In selected cases involving significant tissue loss, degenerative changes, or a labrum structure unsuitable for repair, selective debridement may be performed when indicated.11,37 However, it has been demonstrated that labrum repair provides better clinical outcomes and lower failure rates compared with debridement.15,16 While labral repair is the gold standard in primary cases, labral reconstruction or augmentation techniques are preferred when repair is not feasible due to severe tissue loss or degenerative changes.6,12,21,28,29,41 These techniques aim to restore the labral seal effect and optimize joint biomechanics.14,23,38
The hip suction seal is a key biomechanical mechanism that contributes to joint stability, intra-articular fluid pressurization, and load distribution, while generating negative pressure that resists distraction.7,26,30 Cadaveric studies have shown that labral repair preserves the suction seal effect better than segmental labral reconstruction.4,26,30 However, it has also been reported that reconstruction is significantly superior to labral excision and partially restores the vacuum effect.18,20,26,30 It has been reported that labral augmentation demonstrates biomechanical performance comparable to reconstruction in terms of suction seal strength and distractive stability, 14 and in certain parameters, provides a superior vacuum effect to reconstruction, although without reaching significance. 38
In systematic reviews of patients who underwent revision hip arthroscopy, significant improvements in patient-reported clinical outcomes and high survival rates were reported after reconstruction and augmentation. 17 However, in a comparative study by Philippon et al, 29 augmentation procedures that preserve healthy labral tissue were associated with better patient satisfaction and clinical outcomes compared with segmental reconstruction. These findings support augmentation as an important alternative for hypoplastic or borderline repairable labrums.
Although primary labral repair remains the gold standard for most tears, recent evidence highlights the importance of appropriate decision-making at the index procedure. Kahana-Rojkind et al 13 demonstrated that primary labral reconstruction achieved superior patient-reported outcomes compared with revision reconstruction after failed repair at a minimum 2-year follow-up. These findings suggest that when labral tissue quality is poor or the chondrolabral junction (CLJ) is disrupted, reconstruction may be a more reliable option than repair. In contrast, when the CLJ is intact and adequate native tissue remains, augmentation may help restore labral height and seal function while preserving native biomechanics.
Although previous biomechanical studies have identified certain geometric factors influencing suction seal restoration—such as graft width 20 and labral height25,35— these parameters have been evaluated primarily in reconstruction models. Existing augmentation studies have primarily compared augmentation with reconstruction or repair, without systematically analyzing preservation strategies and construct geometry as independent variables.14,38 Therefore, the relative contribution of preserved native tissue versus augmented labral geometry to suction seal restoration has not been clearly established.
This study investigated the effects of partial labral augmentation and different graft labral height configurations on the restoration of femoroacetabular suction seal strength, using a systematic protocol in an ovine model biomechanically similar to the human hip.31-33 The objective was to quantitatively compare labrum preservation strategies and graft labral heights to identify the most effective reconstruction configuration. We hypothesized that labral augmentation with partial native labrum preservation would restore suction seal strength more effectively than labral reconstruction after total excision.
Methods
Sample Preparation
In this biomechanical study, a sheep hip model that has been shown to be biomechanically similar to the human hip joint in terms of weightbearing properties, long-bone ratios, load orientation, and joint surface contact pressures was preferred.1,31-33 A total of 48 fresh-frozen sheep hemipelvises aged 12 months were used. The samples were obtained from cadaveric specimens with the approval of the ethics committee (Ethics Committee No: 2025/30-12). During dissection, the ligamentum teres was preserved, and the joint capsule was carefully separated from the femoral insertion while preserving the acetabular attachment site. Specimens with trauma, labral tears, cartilage damage, or degenerative changes were excluded from the study. This exclusion criterion was applied to standardize the initial biomechanical integrity of the specimens. In the study design, each hip served as its own internal control, and all biomechanical measurements were compared with the intact baseline condition. The specimens were cryopreserved at −20°C and thawed at room temperature for 24 hours before testing. Each hemipelvis was fixed with plaster in such a way that the acetabulum remained open. The femur was osteotomized at the mid-diaphyseal level and fixed to the test device using a monoaxial screw placed perpendicular to the fovea capitis. All tests were performed with the hip positioned at 90° of flexion (Figure 1). 1
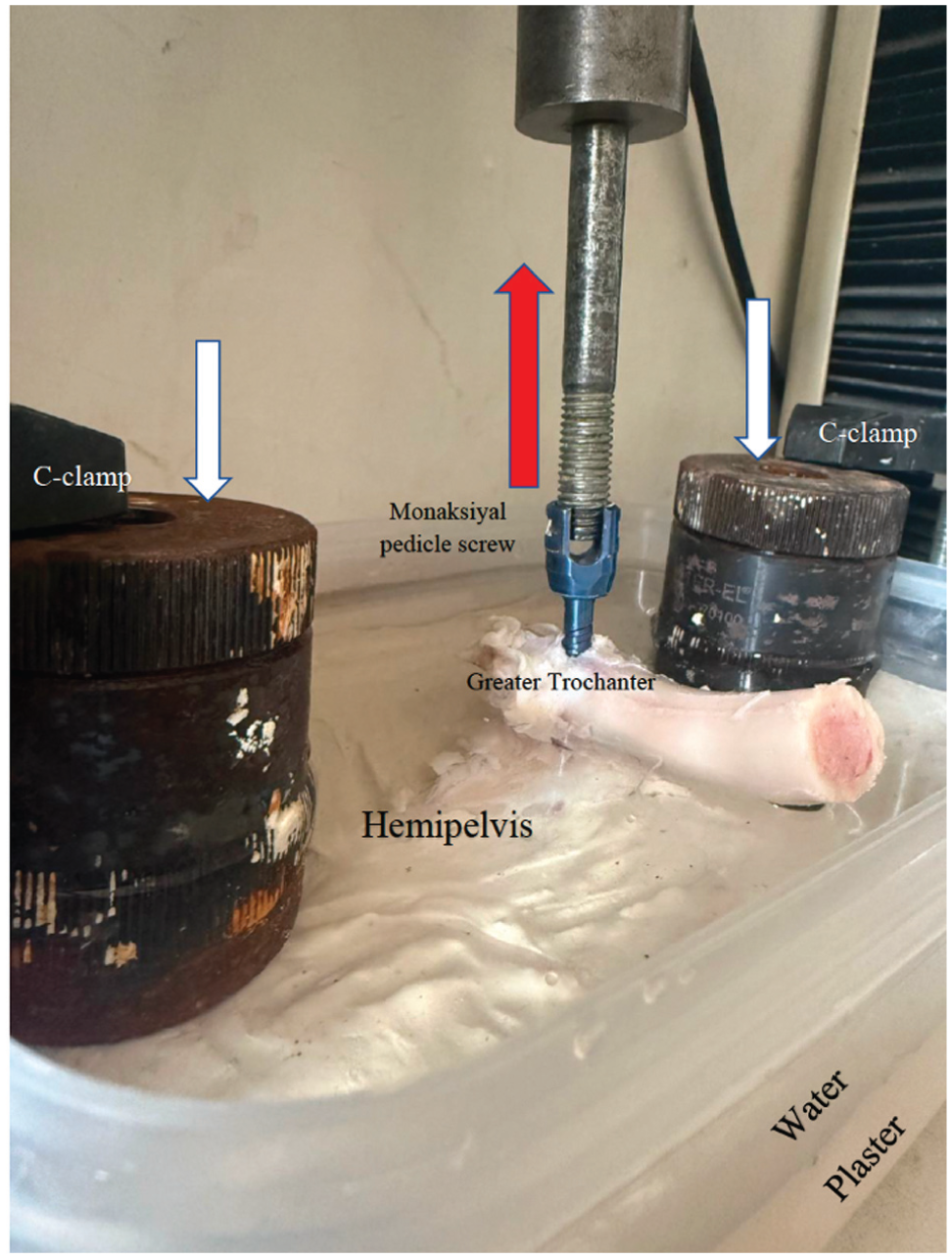
Biomechanical testing setup. The hemipelvis was fixed in plaster within a plastic container. C-clamps were placed on both sides to prevent plaster movement after dissolution (white arrows). A monoaxial pedicle screw was inserted into the femoral head and connected to the testing device, and a tensile force of 200 N was applied (red arrow).
In each sample, the force of the intact femoroacetabular suction seal was measured first. Based on studies demonstrating increased compression in the posterosuperior acetabular region during deep flexion in sheep, 32 a standardized segmental defect region (10:30-1:30) was defined at the acetabular rim. Within this predefined region, the extent of labral excision and preservation was systematically varied according to the group design, and suction seal strength was then measured. Labral reconstruction or augmentation was performed, and suction seal strength was reassessed. For this purpose, autologous sheep extensor tendons were used to prepare grafts. The grafts were cleaned of soft tissue, kept moist in physiological saline, and stabilized by applying a 1 N preload before testing. In the size calculation, the width measurements of the labrum at the 10:30, 12:00, and 1:30 directions were defined as the “y” unit; whereas the corresponding labral height was defined as the ‘x’ unit (Figure 2). The grafts, with a mean diameter of 2.5 ± 0.3 mm and a thickness of 2.2 ± 0.2 mm, were prepared in either standard (×) or extended (2×) labral heights in accordance with the experimental protocol, with y/3 or y/2 width measurements also taken into account during preparation. Each graft was secured to the acetabular rim using 3 single-loaded 2-mm titanium suture anchors (Turpar), providing standardized fixation across all groups, as the segmental defect length was kept constant (10:30-1:30 o’clock). Fixation was performed using a standardized circumferential suture configuration in all specimens. 14 During graft placement, alignment with the acetabular contour was achieved at the micrometric level to ensure physiological curvature.
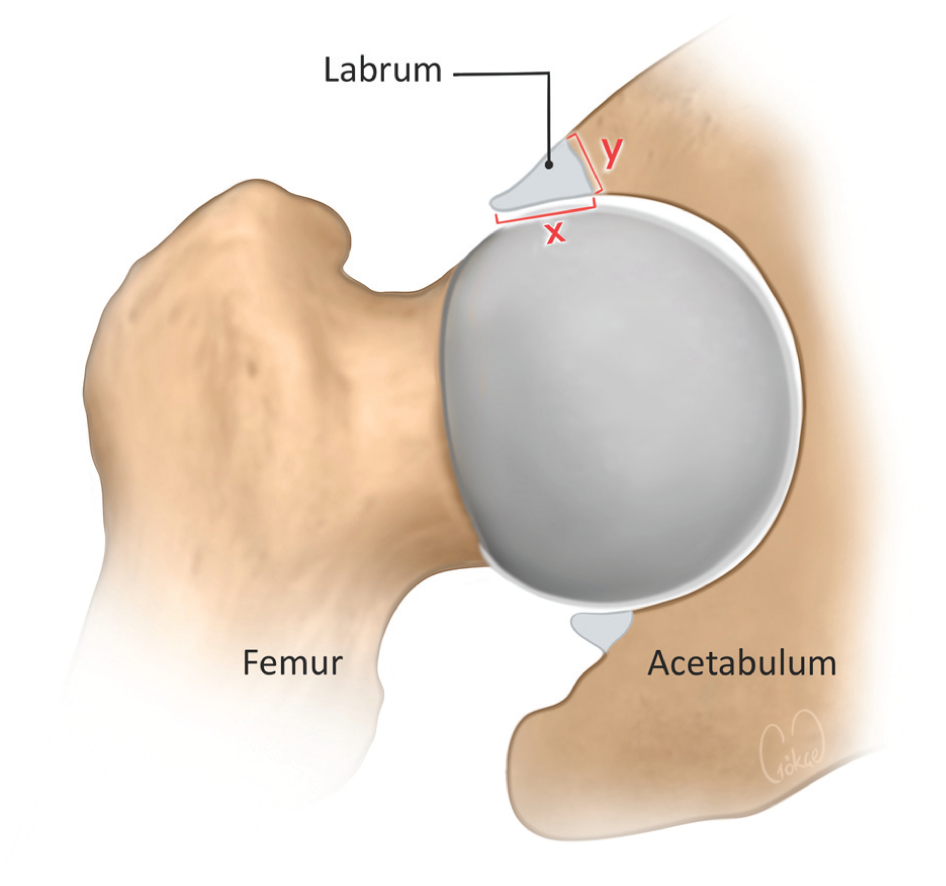
Schematic representation of labral size measurements and graft preparation. The labral width (y) was measured at the 10:30, 12:00, and 1:30 o'clock positions, whereas the corresponding radial labral height was defined as ×.
The samples were randomized into 6 experimental groups (n = 8/group) based on labrum preservation width, excision pattern, and graft labral height. Although labral tears often originate on the articular side, the articular side was preserved in our study because of the biomechanical and biological advantages of preserving viable tissue at the chondral-labral junction.29,34,36
Group 1 (total excision +× graft): The entire labrum was segmentally excised and reconstructed using a graft of natural labral height (×) (Figure 3A).
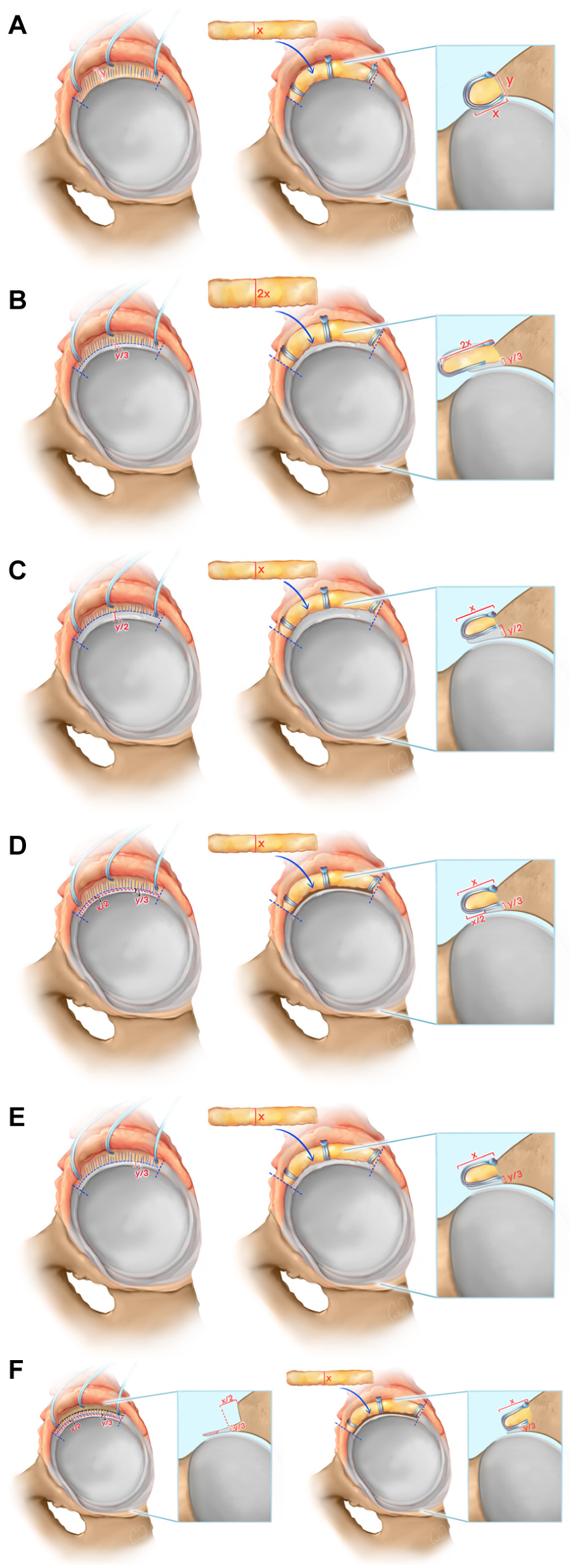
Schematic representation of the experimental groups and graft configurations. Labral width was defined as y, and radial labral height as ×. (A) Total labral excision followed by labral reconstruction (+ x graft). (B) y/3 preservation with labral augmentation (+ 2× graft). (C) y/2 preservation with labral augmentation (+ × graft). (D) y/3 preservation with excision of the upper half of the labrum (x/2) followed by labral augmentation (+ × graft). (E) y/3 preservation with labral augmentation (+ × graft). (F) y/3 preservation with excision of the upper half of the labrum (x/2) and acetabular rim trimming (×/2), followed by labral augmentation (+ × graft).
Group 2 (y/3 preserved from joint side + 2× graft): One-third (y/3) of the labral width on the joint side was preserved; the defect area was reconstructed with a graft twice the natural labral height (2x) (Figure 3 B).
Group 3 (y/2 preserved from joint side +× graft): Half (y/2) of the labral width on the joint side was preserved, and reconstruction was performed with a graft of natural labral height (×) (Figure 3C).
Group 4 (y/3 preserved from joint side, upper half of labral height (×/2) excised +× graft): One-third (y/3) of the labral width on the joint side was preserved, and the upper half of its labral height (×/2) was excised; the defect was reconstructed using a graft of natural labral height (×) (Figure 3D).
Group 5 (y/3 preserved from joint side +× graft): One-third (y/3) of the labral width on the joint side was preserved, and the defect area was reconstructed with a graft of natural labral height (×) (Figure 3 E).
Group 6 (y/3 preserved from the joint side, upper half of labral height (×/2) excised +×/2-unit trimming +×graft): One-third (y/3) of the labral width on the joint side was preserved, and the upper half of its labral height (×/2) was excised. Additionally, controlled rim trimming was performed on the acetabular rim using a 4-mm burr, extending ×/2 units, corresponding to half the labral height (Figure 3F). This group was designed to evaluate the effect of controlled rim trimming on recipient-site contour and graft adaptation in the setting of partial labral preservation, based on prior studies showing that excessive rim trimming may adversely affect hip biomechanics, 3 whereas limited rim preparation may preserve suction seal properties.14,38,39
Biomechanical Tests
The specimens were fixed at 90° of flexion in an electromechanical testing device (AG-IS, Shimadzu Corp), and the femoroacetabular distractive force was measured in accordance with previously defined methods in the ovine hip model. 1 The maximum force was set at 200 N. In each group, a compression force of 200 N was applied for 10 seconds, followed by axial distraction along the femoral axis at a speed of 60 mm/min.1,2 Force and displacement values were continuously recorded at 0.2-ms intervals (5,000 Hz). The maximum distraction force at the point of femoroacetabular separation and seal loss, identified by a distinct drop/transition in the force-displacement curve (and confirmed by an audible popping sound), 10 was defined as the “seal force.” Each test was repeated 3 times, and the mean maximum force was calculated. The same procedure was repeated for each sample after segmental excision and after surgery.
Statistical Analysis
Statistical analyses were performed using commercial software (SPSS 23.0; IBM Corp).
The Shapiro-Wilk test was used to assess normality. Within-group comparisons of suction seal values between testing conditions were performed using the Wilcoxon signed-rank test. Overall, intergroup comparisons were performed using the Kruskal-Wallis test. When the overall comparison was significant, post hoc pairwise intergroup comparisons were conducted using the Mann-Whitney U test. To control for multiple comparisons, the Bonferroni correction was applied, and the adjusted significance threshold for post hoc analyses was set at P < .003. Suction seal strength was defined as the primary dependent variable. P < .05 was considered statistically significant for overall analyses.
Results
In this study, 48 sheep hip joints were randomly assigned to 6 experimental groups (n = 8 per group). Suction seal strength was measured in 3 conditions: intact, excised, and postoperative reconstruction. Values are presented as medians (min-max), IQR, and 95% CIs (Table 1). Intergroup analysis showed no significant differences in the intact (P = .978) or excised (P = .319) conditions.
Suction Seal Force (Max Distraction in Newtons) by Group a
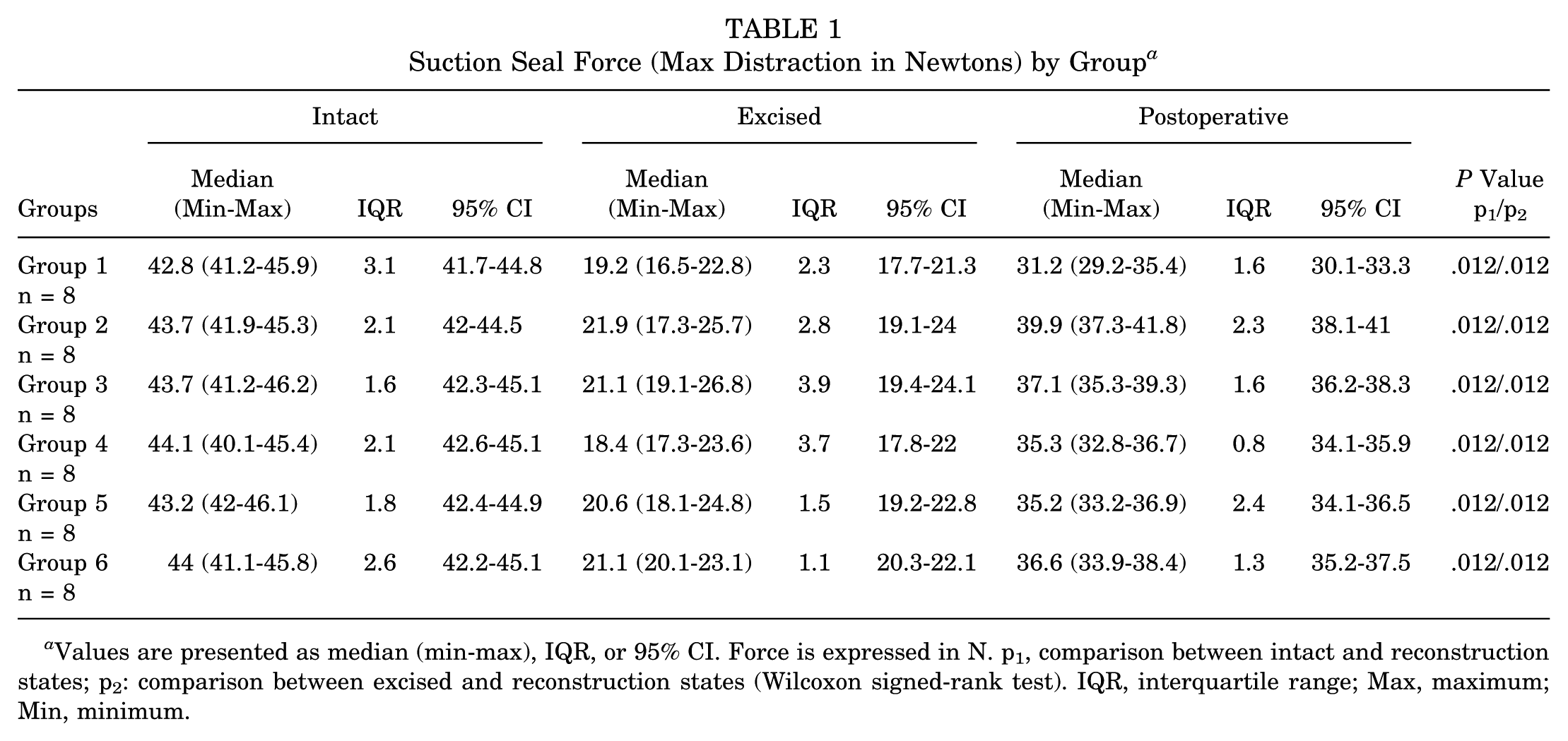
Values are presented as median (min-max), IQR, or 95% CI. Force is expressed in N. p1, comparison between intact and reconstruction states; p2: comparison between excised and reconstruction states (Wilcoxon signed-rank test). IQR, interquartile range; Max, maximum; Min, minimum.
Reconstruction performance was quantified using 2 predefined parameters:

Δ1 represents deviation from the native intact state (lower values indicate closer restoration), whereas Δ2 reflects biomechanical gain relative to the excised condition (higher values indicate greater improvement).
Δ1 (Proximity to Intact State)
Although all postoperative reconstruction/augmentation constructs significantly improved suction seal strength relative to the excised state, none restored native intact values (Table 1).
A significant overall difference was observed among groups for Δ1 (Table 2).
Pairwise Intergroup Comparisons for Δ1 and Δ2 Values a
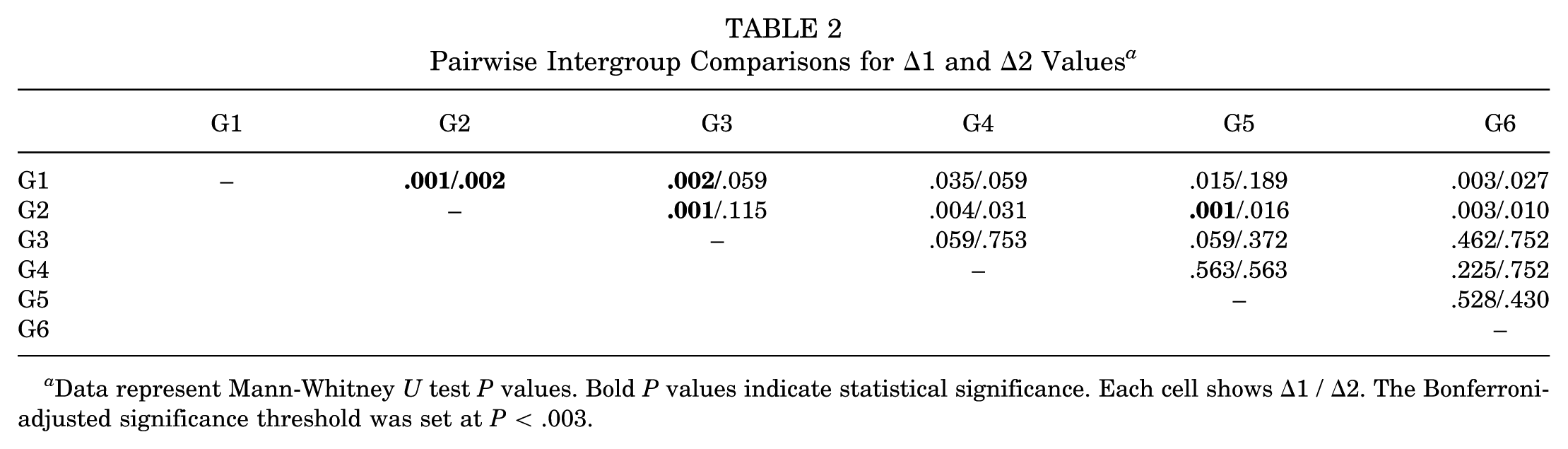
Data represent Mann-Whitney U test P values. Bold P values indicate statistical significance. Each cell shows Δ1 / Δ2. The Bonferroni-adjusted significance threshold was set at P < .003.
Group 1 demonstrated the highest Δ1 value (median 11.6 N), indicating the greatest deviation from the intact condition. In contrast, group 2 showed the lowest Δ1 value (median, 3.8 N), reflecting the closest restoration to the native state (Figure 4).
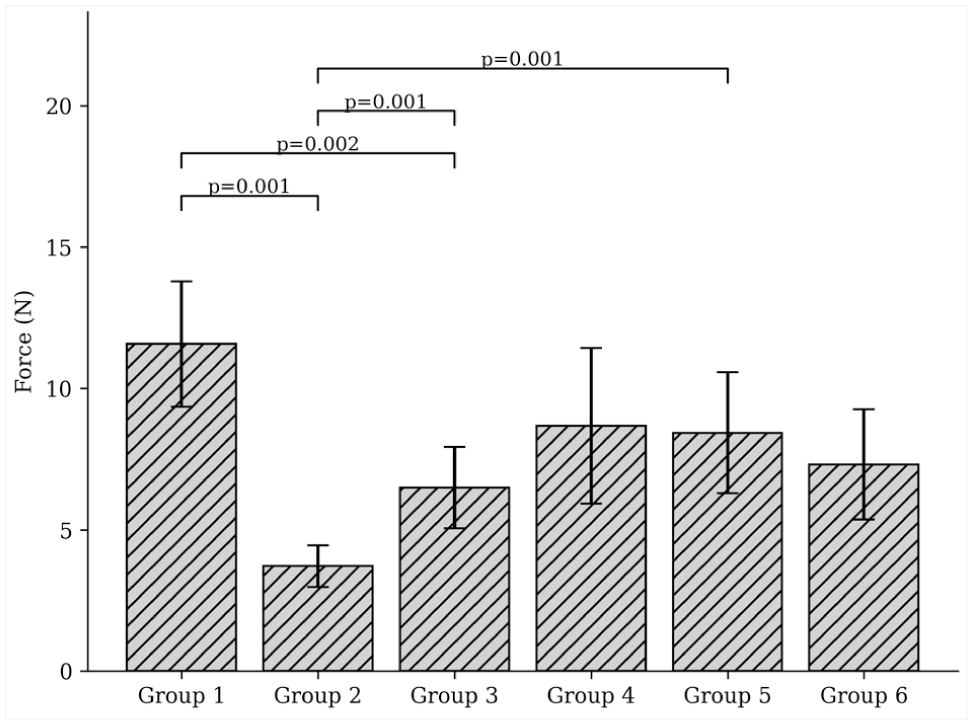
Intergroup comparison of Δ1 values. Bars represent median values; error bars indicate interquartile range (IQR). Lower Δ1 values indicate closer restoration to the intact condition.
After Bonferroni-adjusted pairwise analysis (P < .003):
Group 1 had significantly higher Δ1 values compared with Groups 2, 3, and 6.
Group 2 had significantly lower Δ1 values compared with Groups 3 and 5.
No other pairwise comparisons remained significant after correction (Table 2).
Δ2 (Gain Relative to Excision)
A significant overall intergroup difference was also detected for Δ2 (Table 2).
Group 2 exhibited the highest Δ2 value (median, 18 N), indicating the greatest improvement relative to the excised state (Figure 5).
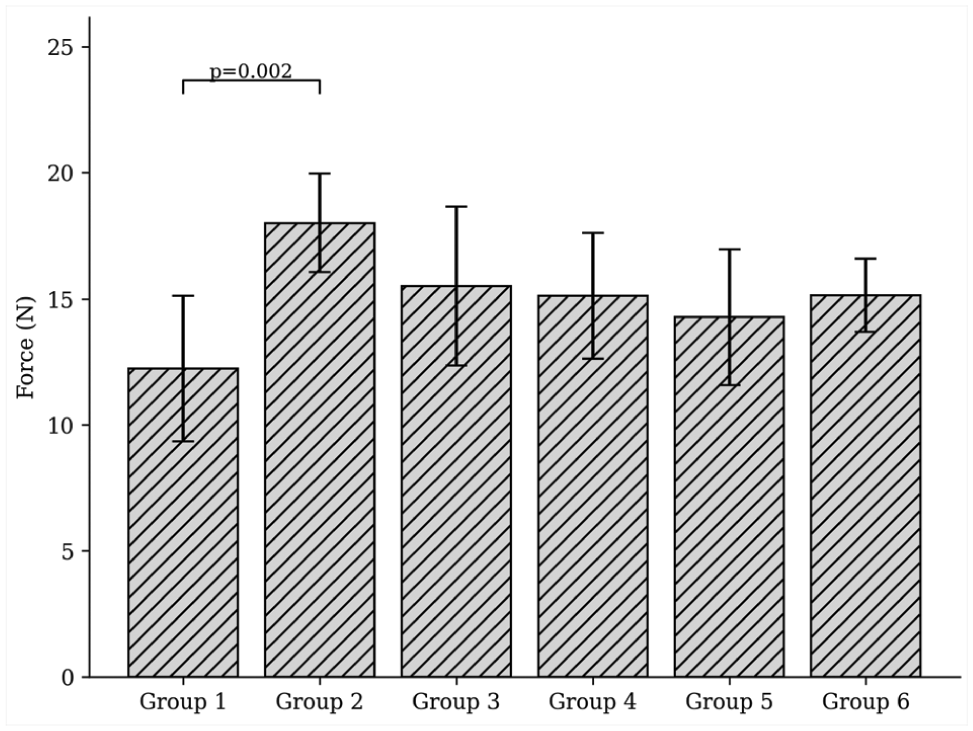
Intergroup comparison of Δ2 values. Bars represent median values; error bars indicate interquartile range (IQR). Higher Δ2 values indicate greater improvement relative to the excised condition.
Following Bonferroni correction (P < .003):
Group 2 demonstrated significantly greater Δ2 values compared with group 1.
No other pairwise differences retained significance (Table 2).
Groups 3, 4, 5, and 6 demonstrated limited numerical variation in Δ1 and Δ2 parameters. Median Δ1 values were 6.6 N for group 3, 8.7 N for group 4, 8.4 N for group 5, and 7.3 N for group 6. Corresponding median Δ2 values were 16 N, 15.1 N, 14.3 N, and 15.1 N, respectively. However, after Bonferroni adjustment for multiple comparisons, no significant differences were observed among these groups.
Discussion
In this study, none of the augmentation strategies fully restored the suction seal to the intact state. However, all augmentation constructs demonstrated improved suction seal strength compared with the excised condition. Among them, group 2—representing augmentation with partial labral preservation—showed the closest approximation to the native state, with the lowest Δ1 (3.8 N) and the highest Δ2 (18 N), indicating the greatest biomechanical improvement. These results are consistent with the findings of Suppauksorn et al, 38 who reported that augmentation, although not significant, provided greater distractive stability than reconstruction. Kaplan et al 14 demonstrated that augmentation using iliotibial band and dermis allografts can produce suction forces similar to or superior to those achieved with labral repair. In this study, the suction force was higher in the augmentation groups—particularly in group 2—compared with the total excision group (group 1, Δ1: 11.6 N), while the remaining augmentation groups also demonstrated numerically higher values. Clinically, Philippon et al 29 reported that augmentation provides superiority over reconstruction in terms of patient satisfaction and functional scores. Additionally, the biomechanical contribution of the partially preserved labrum segment may enhance reconstruction success by creating a synergistic effect with the graft. Similarly, meniscus studies in the knee joint also support the positive effect of preserving native tissue on joint stability. 27 Furthermore, Su et al 36 demonstrated in an animal model that augmentation provides better vascularity and chondrolabral integration, suggesting that grafts applied with partial preservation may be more effective both biologically and mechanically. Although labral tears are commonly reported to originate at the chondrolabral junction, 24 treatment strategies should be guided not solely by tear location but by the ability to restore native labral function. Preservation of viable labral tissue—particularly at the chondrolabral junction—provides important biomechanical and biological advantages. Previous studies have demonstrated that labral augmentation yields favorable clinical outcomes when sufficient native tissue is preserved, 26 while vascularity has been shown to be more prominent on the capsular side, supporting the biological rationale for tissue preservation. 36 Accordingly, augmentation may be preferred in cases with preservable labral tissue, whereas reconstruction is more appropriate in irreparable defects. 34 In line with this concept, our findings suggest that augmentation in partial labral defects with a preserved chondrolabral junction may enhance early suction seal restoration compared with total reconstruction. However, as these findings are derived from a controlled biomechanical model, clinical superiority cannot be established without further clinical investigation.
One of the most striking findings of this study is the significant effect of graft labral height on hip suction-seal biomechanics. The comparison of group 2 and group 5, which differ only in graft labral height despite having the same labral base and protection width, highlights the influence of this parameter. Group 2, which used a graft twice the labral height of the natural labrum, provided both the closest suction force value to the intact labrum (Δ1: 3.8 N) and showed a greater improvement compared with the excised condition (Δ2: 18 N). In contrast, these values were numerically lower in group 5, which used only standard labral height grafts (Δ1: 8.4 N). These findings indicate that reconstructed labral height may play an independent role in distractive stability. The literature also supports this relationship. In a cadaveric study, Storaci et al 35 reported that in specimens with an acetabular labrum height <6 mm, the suction seal effect was significantly reduced, leading to decreased maximum distraction force and negative pressure values. Similarly, Mortensen et al, 25 supported by clinical data, demonstrated that in patients with femoroacetabular impingement undergoing axial traction under anesthesia, those with a labral height ≥6 mm were able to maintain suction seal integrity at higher traction levels. Both studies revealed a critical threshold for labral height, and that the suction effect rapidly disappears in cases below this threshold. In this context, the differences in suction force observed in our study based on graft labral height suggest that not only the amount of graft but also the total labral height achieved after reconstruction plays a fundamental role in hip distraction biomechanics.
In this study, labral width, indirectly assessed through partial labrum preservation strategies, appeared to influence the biomechanical success of reconstruction. Group 3, in which approximately half of the labral width (y/2) was preserved, demonstrated a suction force closer to the native state, with a lower Δ1 value compared with groups 4 and 5, in which one-third (y/3) of the labrum was preserved. However, this difference did not reach significance (P = .059). Moreover, group 3 (y/2) was the only group that did not differ significantly from group 2 with respect to Δ2. The importance of graft width in determining the vacuum effect was previously established by Maldonado et al, 20 who reported a threshold of 6.5 mm; grafts below this value were shown to produce insufficient vacuum effect. Similarly, Li et al 19 reported higher revision rates in cases with low labral width on preoperative magnetic resonance imaging. This literature highlights that the width of the graft or labral tissue is critical for clinical and biomechanical success. In our study, we indirectly assessed width based on the preservation rate of the native labrum contacted by the graft, and we observed that suction force was more effectively achieved in the group with a wider segment preserved. This suggests that not only the width of the graft but also the thickness of the residual labrum tissue that provides coaptation may influence reconstruction success.
Although the aim in group 4 was to place the graft in a more controlled and directed manner by excising only the upper half of the labrum, the suction force obtained (Δ1: 8.7 N) was lower than that obtained in other groups using partial preservation strategies. This suggests that the disruption of the integrity of the labrum contour and the reduction in the contact surface of the graft negatively affected the vacuum effect. However, the significantly better results it yielded compared with group 1 can be attributed to the preservation of the lower segment of the chondrolabral complex. Utsunomiya et al 39 demonstrated that the integrity of the chondrolabral junction plays a decisive role in the biomechanics of the suction seal, and that even with refixation, complete restoration cannot be achieved if this structure is separated. In this context, even in partial excision strategies where contour integrity cannot be preserved, preservation of the chondrolabral complex may enhance the biomechanical efficacy of the graft.
The effect of acetabular rim trimming on femoroacetabular suction seal force is one of the notable points of this study. Reshaping the acetabular contour may improve the restoration of the natural suction seal by facilitating the anatomical placement of the graft. Indeed, Suppauksorn et al 38 reported that edge preparation alone did not significantly reduce suction force, but that the vacuum effect was markedly weakened after augmentation and reconstruction. Kaplan et al, 14 on the other hand, demonstrated that margin preparation caused only a 11% reduction in suction force, and that trimming alone did not disrupt this effect. One of the most notable studies in this field is by Utsunomiya et al 39 who tested the effects of edge flattening on suction seal biomechanics using human cadavers and demonstrated that trimming alone did not significantly affect suction seal force or fracture distance. However, the amount of trimming is a critical parameter. Bhatia et al 3 demonstrated that edge resections >4 mm increased contact pressure at the acetabular base and could lead to early chondral degeneration. This finding highlights the need to perform the trimming process carefully within anatomical limits. In our study, no significant difference in suction force was found between group 6, which underwent rim trimming, and group 5, which did not undergo trimming but had the same graft configuration. This suggests that trimming does not directly weaken the vacuum effect. Additionally, the absence of a significant difference between groups 6 and 4, where only the upper half was preserved, indicates that the direct effect of trimming is limited. Although group 6 showed a lower P value than group 1 for Δ2 (P = .027), this difference did not remain significant after adjustment for multiple comparisons and should therefore be interpreted cautiously. Taken together, these findings suggest that rim trimming may function primarily as a complementary procedure that facilitates graft adaptation without substantially altering suction seal strength when performed within anatomical boundaries. Its biomechanical contribution may depend on the extent of trimming and the specific graft configuration applied.
This study has some limitations. Although the sheep hip joint used as a model is similar to human hip biomechanics, the direct generalizability of the results to clinical applications is limited. Since the study was conducted in a laboratory setting, in vivo physiological factors, such as muscle strength, synovial fluid, vascularity, and biological healing processes, were not evaluated. In addition, graft positioning and the integrity of the chondrolabral junction were standardized in this experimental model and may not fully replicate the variability encountered in clinical settings, potentially influencing suction seal restoration in vivo. In addition, preservation of the chondrolabral junction may limit clinical generalizability, as many labral tears in vivo involve disruption of this structure. Only specific autograft materials and a fixed implantation technique were used, and different graft types, implantation angles, and patient-specific modifications were not analyzed. Furthermore, graft dimensions in the ovine model were smaller than those typically used in human labral reconstruction, which may limit direct translational interpretation of graft sizing. The biomechanical test protocol focused solely on distraction force; other parameters, such as rotational stability, contact area, and load orientation, were not considered. The limited sample size may have reduced the study's statistical power and prevented some comparisons from reaching significance. An a priori power analysis was not performed before specimen allocation, and the sample size was determined based on previously published biomechanical studies with similar experimental designs.2,14,38 Additionally, only segmental labral defects were modeled, and other tear types were not evaluated. The validity of the results may also have been affected by the test setup and methodological limitations used. Although these factors limit the scope of the study, the findings may shed light on future, more comprehensive biomechanical and clinical research. The discussion was primarily based on the biomechanical trends observed in pairwise comparisons between groups. Although some comparisons did not remain significant after Bonferroni correction, the overall ranking of group performance remained unchanged, with the configuration combining partial labral preservation and increased graft radial height (2× graft) continuing to demonstrate the most favorable biomechanical performance.
Conclusion
This study demonstrated that combining partial labrum preservation with larger-diameter grafts effectively restores femoroacetabular suction seal strength. In particular, augmentation with a double-labral height graft provided the closest result to natural suction strength. Additionally, the width and integrity of the labrum tissue in contact with the graft were found to be important for the success of the reconstruction. Rim trimming, when appropriately applied, can facilitate graft placement. Both graft labral height and the quality of preserved labrum tissue should be considered in labral reconstructions.
Footnotes
Final revision submitted April 11, 2026; accepted April 14, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from Dokuz Eylul University Ethics Committee (2025/30-12).