
Abstract
Background:
Venous thromboembolism (VTE) is a potentially deadly complication following orthopaedic surgery. However, its true incidence and risk factors after shoulder arthroscopy are not well understood, as most current evidence depends on symptom-based diagnosis, which may underestimate the actual incidence.
Purpose:
To determine the real-world incidence of VTE using systematic postoperative ultrasonographic screening and to identify independent risk factors.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 282 patients undergoing elective shoulder arthroscopy were prospectively enrolled. All patients had bilateral lower extremity venous color Doppler ultrasonography performed preoperatively and on postoperative day 1. Comprehensive demographic, clinical, and laboratory data were collected. Univariate and multivariate logistic regression analyses were conducted to identify independent predictors of postoperative deep vein thrombosis (DVT).
Results:
The incidence of postoperative DVT, diagnosed through systematic ultrasound screening, was 7.8% (22/282). After accounting for other factors, multivariate analysis found that longer operative duration is an independent risk factor. Specifically, each additional hour increases the odds by about 2.86 times (95% CI, 1.26-6.52; P = .01). No other clinical or laboratory variables, including preoperative coagulation and inflammatory markers, demonstrated a statistically significant association with postoperative DVT in the multivariate model.
Conclusion:
This study reveals a substantially higher rate of VTE following shoulder arthroscopy than previously recognized. Operative duration is confirmed as a significant and identifiable independent risk factor. These findings highlight the need to reconsider VTE risk assessment in shoulder arthroscopy and support further research into risk-stratified prevention strategies.
Keywords
Venous thromboembolism (VTE) is a serious, potentially life-threatening complication following major orthopaedic surgery. Early systematic imaging surveillance studies revealed that without thromboprophylaxis, the incidence of VTE following major hip and knee procedures ranges from 29% to 60%, with fatal pulmonary embolism (PE) occurring in 1% to 3% of cases.3,14,20,27 Shoulder arthroscopy is among the most common procedures in orthopaedic surgery. Globally, ≥1.5 million shoulder arthroscopic procedures are performed each year.21,28,30 However, unlike the well-characterized risk in lower extremity surgery, the epidemiology of VTE after shoulder arthroscopy remains poorly defined and is a subject of ongoing debate. It is important to note that the majority of the existing literature on this topic has focused on upper-extremity deep vein thrombosis (DVT), which is often catheter related or associated with direct venous injury.25,35 In contrast, the incidence, risk factors, and clinical significance of lower-extremity DVT following these procedures are markedly understudied. While guidelines from the American College of Chest Physicians (ACCP) in 2012 and the European Society of Anaesthesiology in 2018 address VTE risk in lower limb and trauma surgeries, the approach to risk stratification for VTE specifically in shoulder arthroscopy is unclear. 41 The actual rate of VTE following shoulder arthroscopy has been a topic of debate for some time. Reported rates vary widely in the literature, from 0.038% to 0.71%.7,25,30,35,36,43 This narrow range likely reflects the predominant detection of symptomatic upper-extremity events and misses the burden of asymptomatic lower-extremity DVT. A critical limitation of these studies is their reliance on symptom-driven diagnosis, which fails to capture asymptomatic events. Consequently, shoulder arthroscopy is not currently classified as a high-risk procedure for VTE, and routine pharmacologic thromboprophylaxis is not recommended by major international guidelines.
This gap between guideline recommendations and the potential underrecognition of risk is concerning. The true burden of lower-extremity DVT after shoulder arthroscopy, detectable only through systematic screening, is unknown. This knowledge deficit hinders the development of evidence-based prevention strategies.
Therefore, this prospective cohort study was designed with the primary hypothesis that operative duration is an independent risk factor for lower-extremity DVT following shoulder arthroscopy. The specific objectives are to (1) determine the real-world incidence of lower-extremity DVT using mandatory postoperative ultrasonographic screening and (2) identify independent patient- and procedure-related risk factors.
Methods
Study Population
This single-center, prospective cohort study received approval from the institutional review board of The First Hospital of Jilin University. All participating patients provided written informed consent. Consecutive patients who underwent elective shoulder arthroscopy in the Department of Sports Medicine, Orthopaedics Clinic, the First Hospital of Jilin University between March 1, 2024, and September 30, 2025, were enrolled. The inclusion criteria were patients (1) age ≥18 years and (2) scheduled for arthroscopic shoulder procedures, including rotator cuff repair, acromioplasty, and/or labral repair. Exclusion criteria included (1) preoperative diagnosis of DVT confirmed by lower limb ultrasonography; (2) a history of VTE within 3 months before surgery or ongoing anticoagulant therapy; (3) incomplete clinical data. After screening, 282 patients were included in the final analysis. The patient selection flow is detailed in Figure 1.
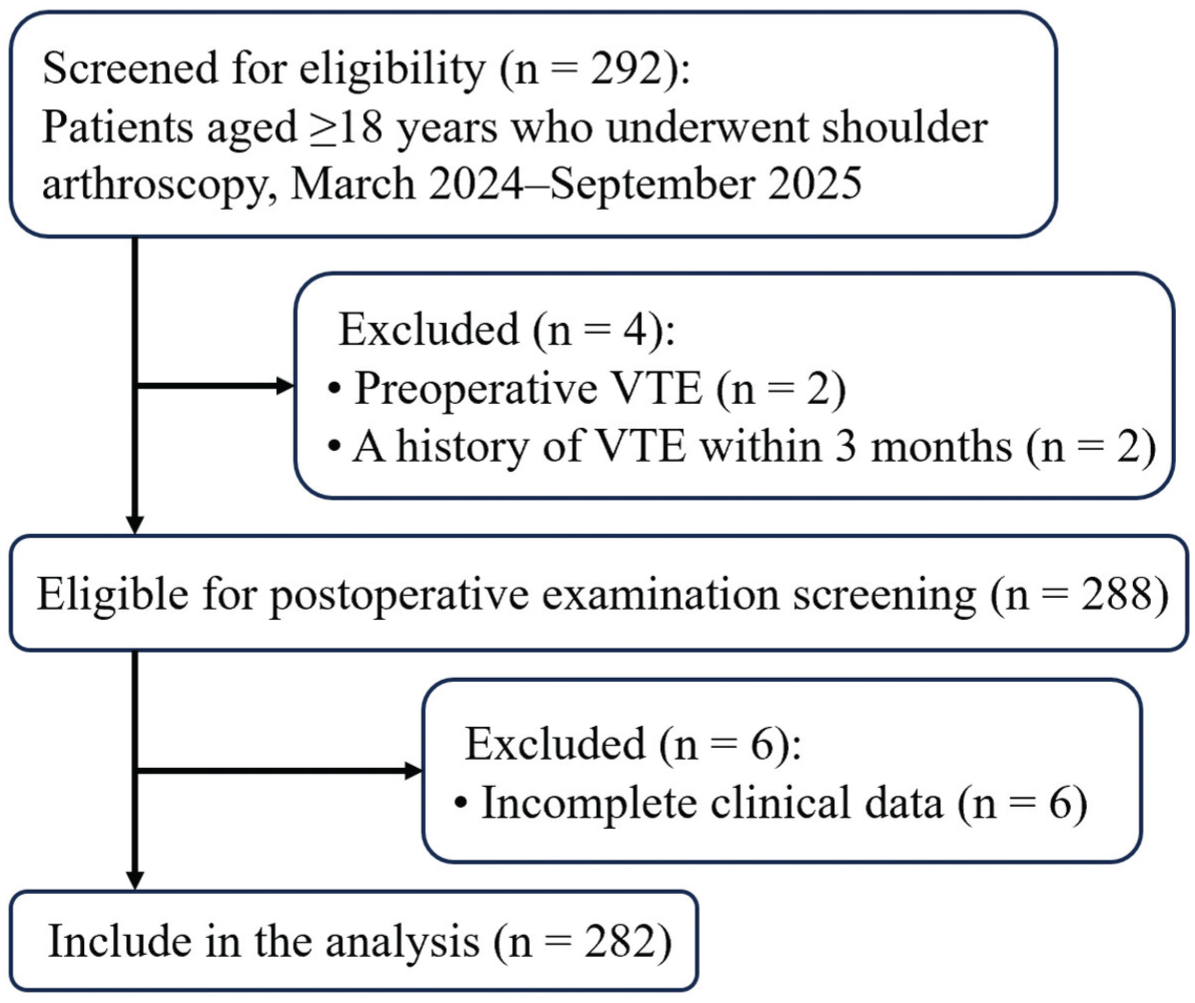
Patient selection flowchart. VTE, venous thromboembolism.
Arthroscopic Surgery
A single senior arthroscopic surgeon (P.X.) performed all procedures under general anesthesia. The surgeries were conducted with patients in the lateral decubitus position, stabilized using a beanbag, standard arthroscopic portals, and established operative techniques consistent with routine clinical practice. 15 A pillow was routinely placed between the patient's legs to protect dependent tissues. Mechanical compression devices were not applied to the calves during the surgery. Our surgical center is located at an altitude of approximately 250 m above sea level. Standard posterior and anterior portals were created for diagnostic arthroscopy, followed by the necessary therapeutic interventions. 34 All cases involved relatively complex procedures, such as rotator cuff tendon repair with suture anchors or labral repair. Operative duration, defined as the duration from anesthesia induction to surgery completion, was recorded.
Postoperative Management and Surveillance
All patients were admitted for overnight observation following the surgery. Postoperatively, all patients followed a standardized rehabilitation protocol, 42 engaging in early functional exercises under the supervision of a physical therapist. Bilateral lower extremity venous color Doppler ultrasonography was performed on the day before surgery and on the first postoperative day. Postoperative management differed based on the presence or absence of a diagnosed DVT. For all patients, bilateral lower limb intermittent pneumatic compression devices were routinely applied after surgery until discharge. Early mobilization was encouraged, with patients advised to ambulate out of bed beginning on the first postoperative day. Upon diagnosis of a postoperative DVT by ultrasonography, a standardized therapeutic protocol was initiated. The pneumatic compression devices were discontinued. Patients were instructed to adhere to bed rest with limited ambulation to prevent thrombus dislodgement. Therapeutic anticoagulation was initiated with subcutaneous fondaparinux sodium at a dosage of 2.5 mg twice daily. 12 The treatment regimen was subject to adjustment based on follow-up duplex ultrasonography and clinical assessment.
Data Collection
All laboratory parameters described below were measured preoperatively. Potential risk factors for postoperative DVT were evaluated based on prospective data collection from electronic medical records. The data collection strategy was designed with reference to the established Caprini risk assessment model and factors previously documented in the literature to be associated with VTE, aiming to encompass the 3 fundamental elements of the Virchow triad: hypercoagulability, endothelial injury, and venous stasis.2,6,16,18 The data collected primarily included the following 5 categories.
Patient Characteristics
Demographic data, including age, sex, height, and weight, were collected, and body mass index (BMI) was calculated. Key comorbidities were also documented, defining as a DVT confirmed by postoperative ultrasonography that was associated with new-onset, non–surgically related symptoms in the ipsilateral lower limb, as reported by the patient or identified on clinical examination. These symptoms included, but were not limited to, pain, swelling, warmth, erythema, or tenderness along the venous tract. These baseline indicators were chosen because they reflect essential aspects of a patient's general health and inherent risk of thrombosis. The inclusion of hypertension, diabetes mellitus, hyperlipidemia, and smoking status was based on their known links to endothelial dysfunction and atherosclerotic vascular disease, which may also relate to venous thrombotic risk.11,32 The American Society of Anesthesiologists physical status classification was also recorded. No patients in this cohort were using oral contraceptives or hormone replacement therapy. Hyperlipidemia was defined as a total cholesterol level ≥240 mg/dL, triglycerides ≥200 mg/dL, low-density lipoprotein cholesterol ≥160 mg/dL, or the current use of lipid-lowering medications, 22 Diabetes mellitus was defined as a fasting plasma glucose level ≥7.0 mmol/L or ongoing hypoglycemic therapy. 1
Imaging Assessment and Outcome Determination
All patients underwent bilateral lower extremity deep venous color Doppler ultrasonography on the day before surgery and on the first postoperative day. All examinations were performed by a single team of experienced sonographers using identical high-resolution ultrasound systems to ensure consistency and reproducibility. The scanning protocol thoroughly evaluated the deep venous system, including the common femoral vein, femoral vein, popliteal vein, posterior tibial veins, and muscular calf veins (soleal and/or gastrocnemial veins). The diagnosis of acute DVT was primarily based on the noncompressibility of the vein, supplemented by additional criteria such as the presence of intraluminal solid echogenicity and the absence of flow signals on Doppler imaging. For all detected thrombi, the following characteristics were systematically recorded: the specific anatomic location (eg, muscular calf veins), thrombus burden including the maximal diameter (mm) and length (cm), as well as laterality (unilateral or bilateral, and which limb). Based on the postoperative imaging results, patients were classified into either the DVT group or the non-DVT group for subsequent analysis.
Coagulation and Thrombosis Markers
Coagulation parameters, complete blood count, and serum calcium were measured using blood samples taken before surgery and on the first day after surgery. Standard tests, including prothrombin time (PT), activated partial thromboplastin time (APTT), international normalized ratio (INR), and fibrinogen (FBG) levels, as well as serum calcium levels, were used to assess the intrinsic and extrinsic coagulation pathways. D-dimer, a key degradation product of cross-linked fibrin, was analyzed as an important biomarker for ruling out and diagnosing acute VTE 5 ; a preoperative level >0.5 mg/L fibrinogen equivalent units was deemed abnormal. 44 Collectively, these hematologic parameters directly indicate a hypercoagulable state and provide essential evidence for evaluating the risk of thrombus formation.
Inflammation and Immune Response Markers
All laboratory parameters described below were measured preoperatively. A comprehensive panel of cellular immune and inflammatory markers was included in the analysis. This encompassed the total white blood cell count, along with the absolute counts and percentages of its subtypes (neutrophils, lymphocytes, monocytes, etc). Additionally, high-sensitivity C-reactive protein (hs-CRP) and myeloperoxidase (MPO) levels were measured. The selection of these markers was based on growing evidence highlighting the critical role of inflammation as a linking factor between surgical trauma and thrombogenesis.29,31 Activated inflammatory cells, especially neutrophils, release substances such as MPO, which can directly activate platelets and cause endothelial injury, thereby actively promoting thrombus formation. 47 Hs-CRP functions as a classic biomarker for assessing the systemic inflammatory response. 10
Hepatic and Renal Function Parameters
Laboratory parameters indicating hepatic function (such as aspartate aminotransferase, alanine aminotransferase, gamma-glutamyl transferase, and albumin) and renal function (creatinine, blood urea nitrogen, electrolytes), as well as bilirubin metabolism, were evaluated. The liver is the main site for producing most coagulation factors and anticoagulant proteins, such as antithrombin III. 33 Additionally, renal insufficiency is a well-known risk factor for VTE.23,33 Including these parameters helped assess baseline organ function, ensuring that issues with metabolic balance or internal environment stability would not significantly confound the analysis.
Statistical Analysis
All statistical analyses were performed using SPSS software (Version 29.0; IBM Corp). A 2-sided P value <.05 defined statistical significance. The normality of continuous variables was evaluated with the Shapiro-Wilk test. Since most laboratory parameters showed nonnormal distributions, continuous data are presented as median with interquartile range, and group comparisons were performed using the Mann-Whitney U test. Categorical variables are summarized as frequencies and percentages, and intergroup comparisons were made using the chi-square test or Fisher exact test, as appropriate.
To identify independent risk factors for postoperative DVT, variables with a significance level of P < .05 in the univariate analysis were included in a multivariate binary logistic regression model. Variable selection was performed using a backward conditional elimination method based on the likelihood ratio. The variables entered into the model included operation time, age, hyperlipidemia, and serum calcium level. The regression results are shown as adjusted odds ratios (ORs) with their corresponding 95% CIs. The model's goodness of fit was evaluated using the Hosmer-Lemeshow test. Before fitting the model, it was observed that the serum calcium concentration (in mmol/L) had a narrow numerical range, which caused a quasi-complete separation issue in the model. This problem was indicated by unrealistically large OR estimates and wide confidence intervals. To address this numerical issue, a linear transformation was applied to the calcium data (original value × 10). As a result, in the final model, the OR for serum calcium reflected the risk associated with a 0.1-mmol/L increase in concentration.
For continuous variables identified as risk factors, their ability to predict DVT was further assessed through receiver operating characteristic (ROC) curve analysis. The best clinical cutoff point was found by maximizing Youden index (sensitivity + specificity – 1). 49 It is important to note that this cutoff value is considered exploratory and needs validation in future studies.
A post hoc power analysis was performed using G*Power software (Version 3.1.9.7). Based on the largest effect size observed in the multivariate logistic regression model (adjusted OR, 2.86), the total sample size (N = 282), and the observed DVT incidence of 7.8%, the analysis resulted in a statistical power of 99.9% (α = .05). This finding indicates that the current sample size offers strong statistical power, reliably supporting the detection of the significant associations found in this study.
Results
Patient Characteristics and Surgical Procedures
A total of 282 patients who underwent elective shoulder arthroscopy were included in this prospective analysis. All patients underwent systematic bilateral lower extremity venous ultrasonography on postoperative day 1. Based on the imaging results, the cohort was stratified into a DVT group (n = 22) and a non-DVT group (n = 260), yielding an overall postoperative DVT incidence of 7.8%.
The baseline demographic and clinical characteristics of the entire cohort are summarized in Table 1. The surgical procedures performed were categorized as rotator cuff repair (RCR; n = 169), labral repair (Bankart/superior labrum anterior-posterior; n = 67), and acromioplasty/subacromial decompression (SAD; n = 46). The distribution of these procedure types was comparable between the DVT and non-DVT groups (P = .71), indicating that the specific type of arthroscopic procedure itself was not a primary determinant of VTE risk in this study.
Patient Characteristics a
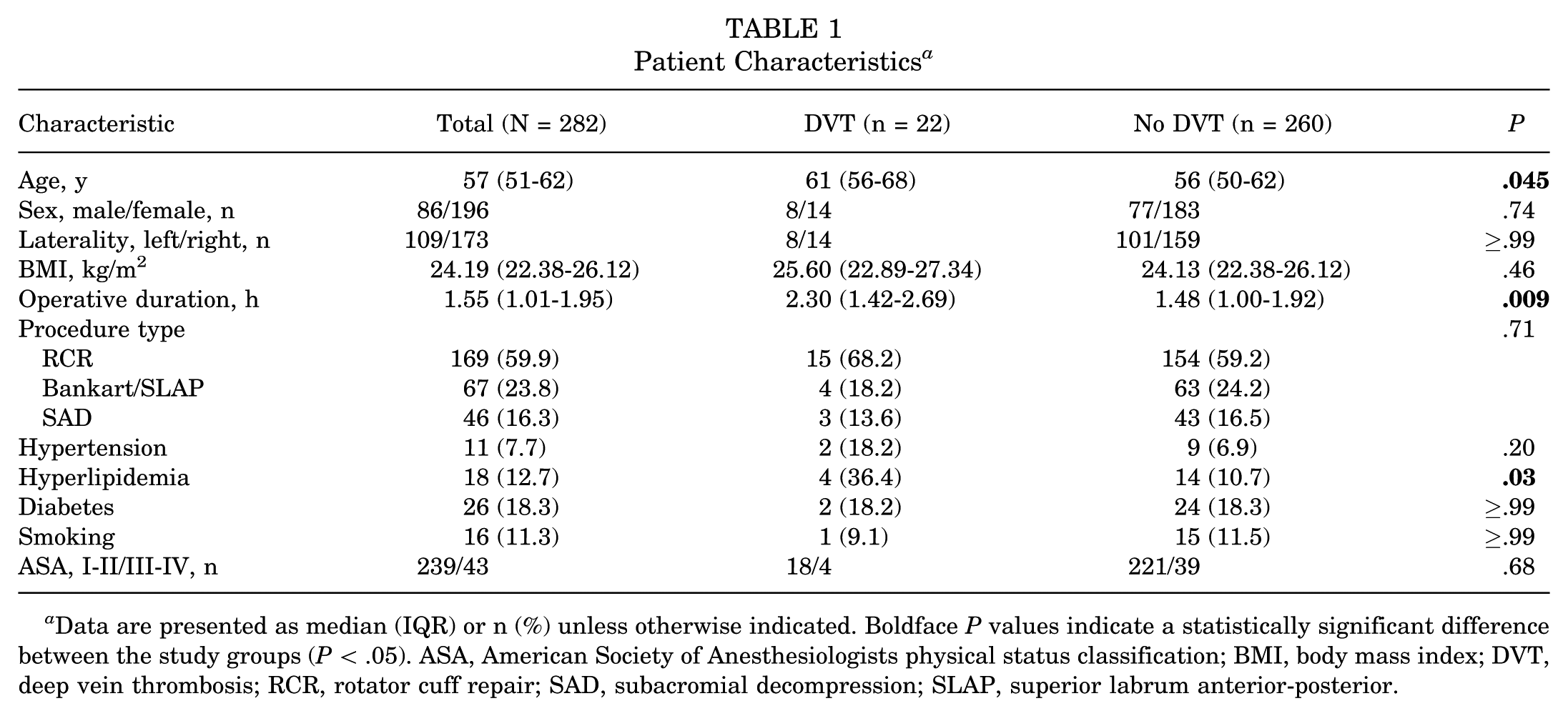
Data are presented as median (IQR) or n (%) unless otherwise indicated. Boldface P values indicate a statistically significant difference between the study groups (P < .05). ASA, American Society of Anesthesiologists physical status classification; BMI, body mass index; DVT, deep vein thrombosis; RCR, rotator cuff repair; SAD, subacromial decompression; SLAP, superior labrum anterior-posterior.
Characteristics of Detected DVT
As shown in Table 2, among the 22 patients diagnosed with postoperative DVT, all thrombi were located in the calf veins (below the knee), specifically within the muscular calf veins (soleal and/or gastrocnemius veins). No proximal (thigh) DVT or PE was detected. Regarding symptomatic presentation, 7 DVTs (31.8%) were symptomatic, while the remaining 15 (68.2%) were asymptomatic and identified solely through systematic screening. The thrombi had a mean maximal diameter of 5.93 ± 2.12 mm and a mean length of 2.47 ± 1.39 mm. Analysis of the relationship between DVT occurrence and the dependent limb revealed that 8 patients had bilateral DVT. Among the 14 patients with unilateral DVT, the thrombus was located in the dependent leg in 8 cases (57.1%) and in the nondependent leg in 6 cases (42.9%); this distribution was not statistically significant (P = .59).
Characteristics of Detected Deep Vein Thromboembolism a
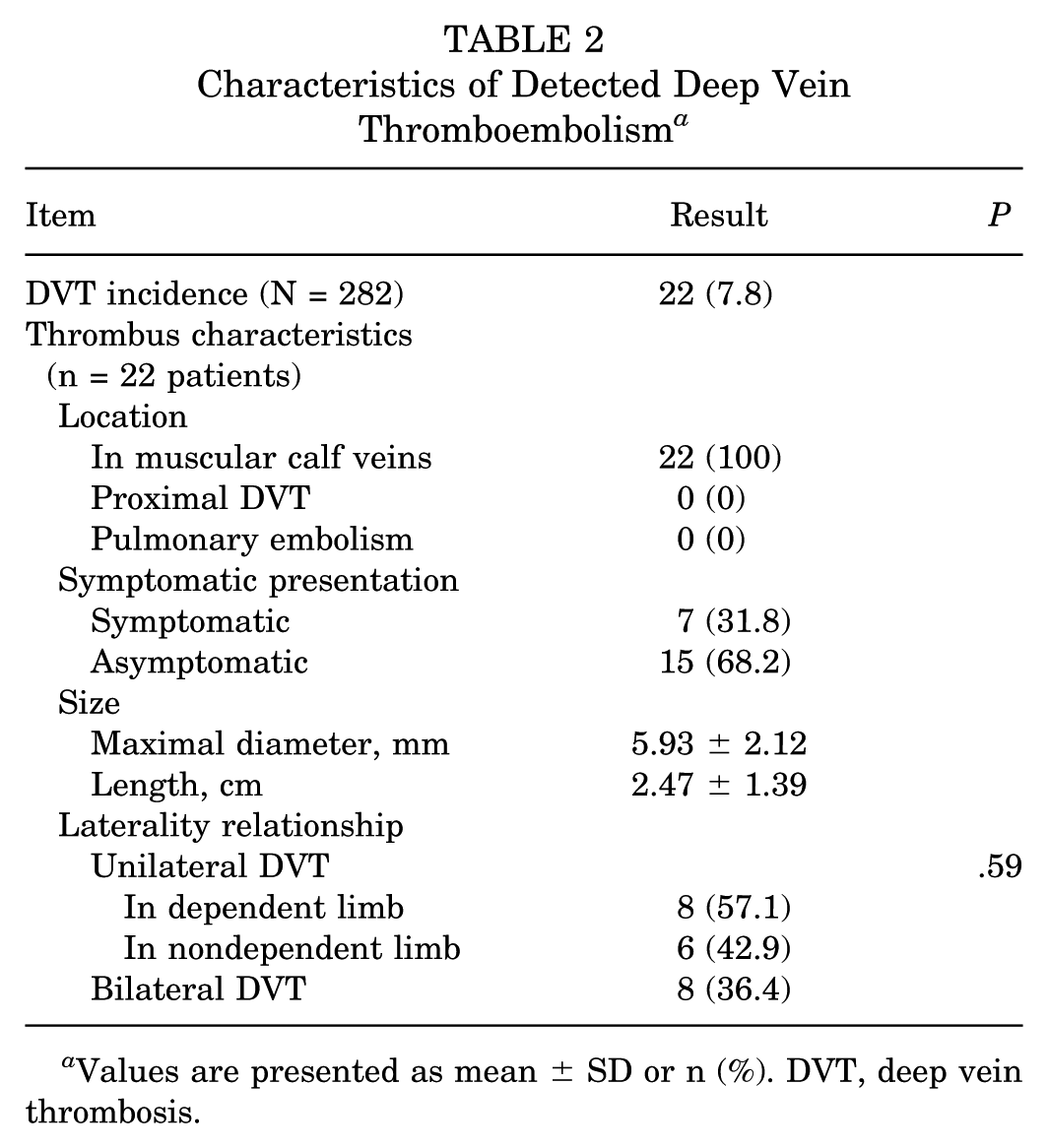
Values are presented as mean ± SD or n (%). DVT, deep vein thrombosis.
Analysis of Potential Risk Factors
Clinical and Procedural Risk Factors
As detailed in Table 1, univariate analysis of clinical and procedural factors revealed that patients in the DVT group were significantly older (P = .045), had a higher prevalence of hyperlipidemia (P = .03), and had a significantly longer operative duration (P = .009) compared with the non-DVT group.
Laboratory Parameters
(1) Coagulation and thrombosis markers: comprehensive assessment of routine coagulation pathways (prothrombin time, activated partial thromboplastin time, thrombin time, international normalized ratio, fibrinogen), platelet indices (count, volume, distribution), the fibrin degradation product D-dimer, and complete blood count indices (see AppendixTable A1 for details) revealed no statistically significant differences between the DVT and non-DVT groups (all P > .05). This indicates that a baseline hypercoagulable state detectable by standard preoperative coagulation screening was not a predominant feature in patients who subsequently developed DVT.
(2) Inflammation and immune response markers: AppendixTable A2 presents the analysis of systemic and cellular inflammatory markers. Although the neutrophil-derived enzyme MPO showed a nonsignificant trend toward higher levels in the DVT group (P = .18), other established markers of inflammation, including hs-CRP, erythrocyte sedimentation rate, and total and differential white blood cell counts, were comparable between groups (all P > .05). These findings do not support the presence of a significant preoperative systemic inflammatory state as a key driver of VTE risk in this cohort.
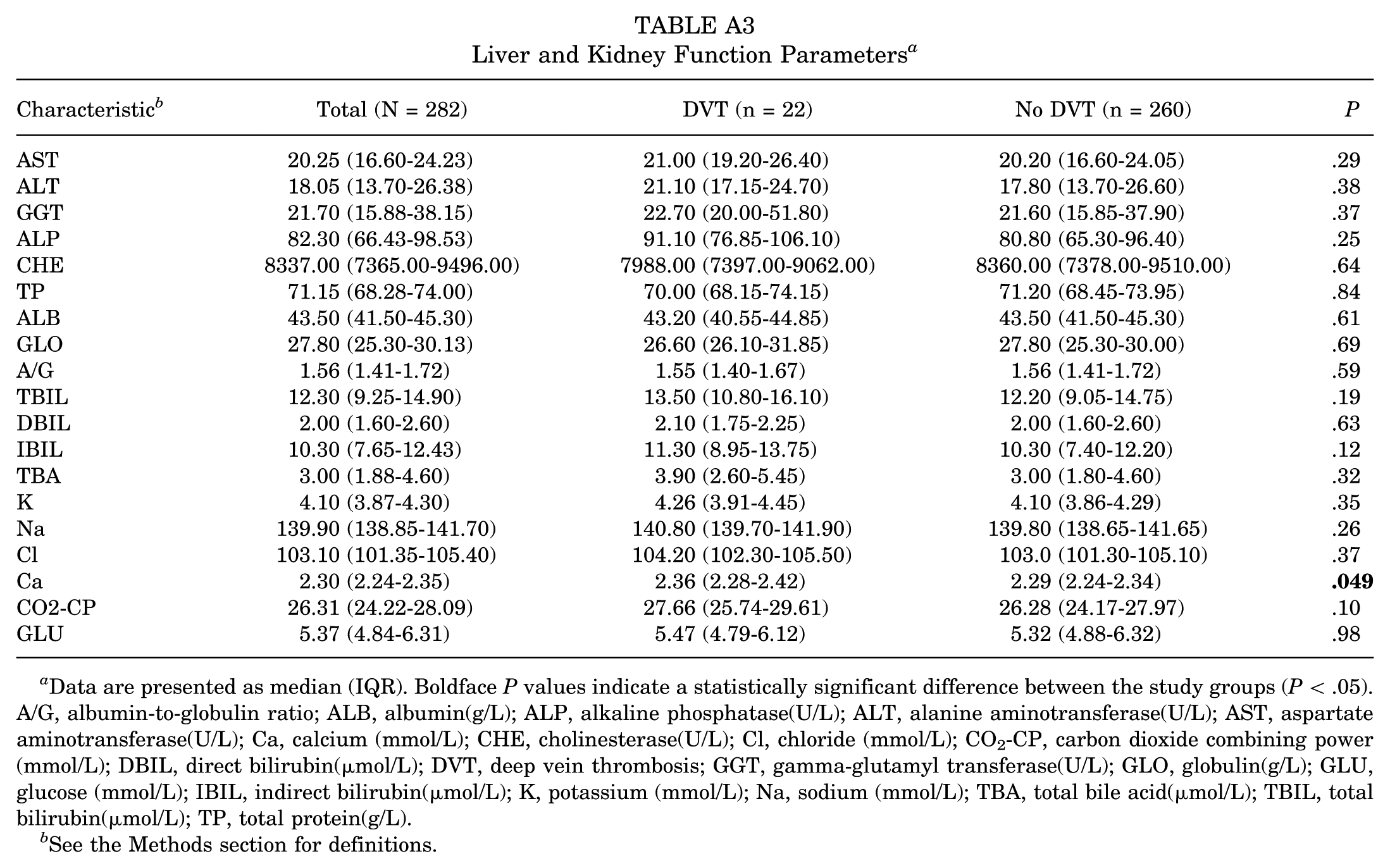
(3) Hepatic/renal function and electrolytes: evaluation of organ function and internal homeostasis parameters (AppendixTable A3) showed that the vast majority of measures, including liver enzymes, bilirubin fractions, protein profiles, and electrolytes (potassium, sodium, chloride), were similar between groups. Serum calcium was the only parameter to reach nominal statistical significance, with slightly higher levels in the DVT group (2.36 vs 2.29 mmol/L; P = .049). However, the absolute difference was small (0.07 mmol/L). The clinical and biological relevance of the minimal calcium difference remains uncertain.
Multivariate Logistic Regression Analysis
To adjust for potential confounders and identify independent predictors of postoperative VTE, variables with P < .05 in univariate analysis (operative duration, hyperlipidemia, serum calcium, and age) were included in a multivariable binary logistic regression model. The results are shown in Table 3. After adjustment, a longer operative duration remained a significant and independent risk factor for postoperative DVT (adjusted OR, 2.86; 95% CI, 1.26-6.52; P = .01). This suggests that for each additional hour of operative duration, the odds of developing postoperative DVT increased nearly 3-fold. Neither hyperlipidemia (adjusted OR, 3.78; 95% CI, 0.88-16.20; P = .07) nor serum calcium level (adjusted OR, 1.99; 95% CI, 0.94-4.22; P = .07) retained statistical significance in the multivariable model, although both exhibited strong, nonsignificant trends toward association.
Results of Binary Logistic Regression Analysis for Presence of Postoperative VTE a
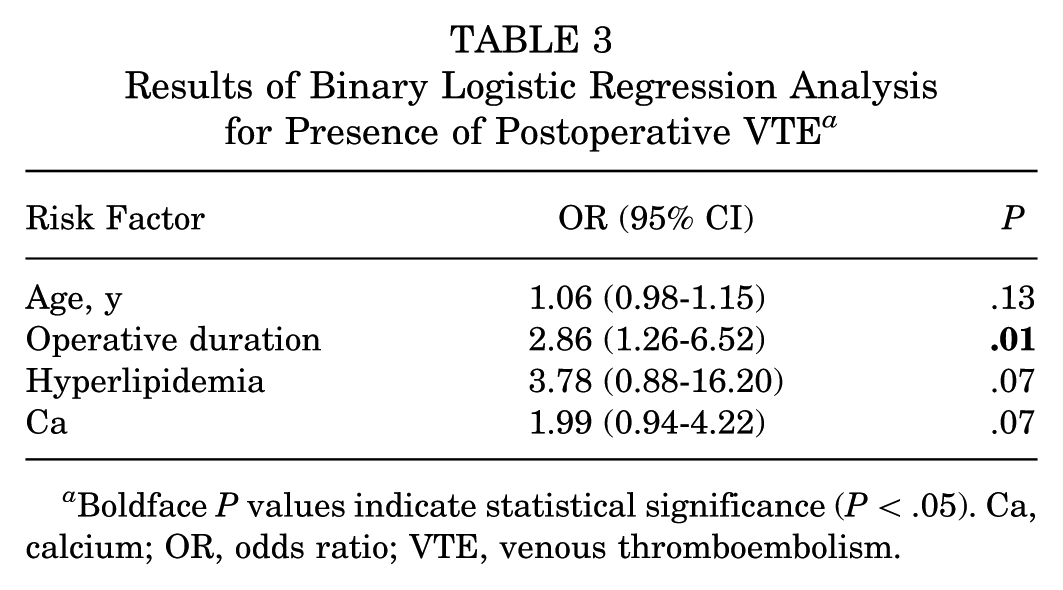
Boldface P values indicate statistical significance (P < .05). Ca, calcium; OR, odds ratio; VTE, venous thromboembolism.
ROC Analysis
The predictive ability of the sole independent risk factor—operative duration—for postoperative DVT was further assessed using ROC curve analysis (Figure 2). The results showed an area under the curve of 0.781. The best cutoff value for operative duration, identified by maximizing Youden index, was 1.39 hours. This cutoff predicted DVT occurrence with a sensitivity of 90.9% and a specificity of 54.6%.
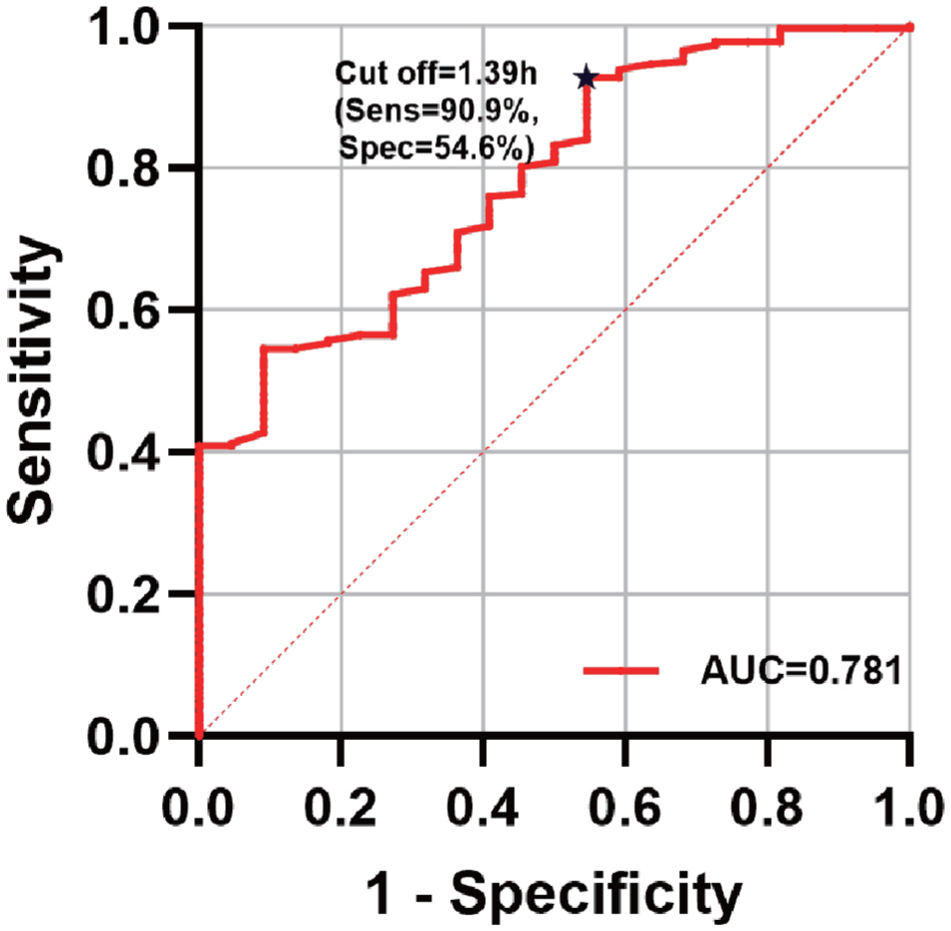
Receiver operating characteristic curve for operative duration in predicting postoperative venous thromboembolism. AUC, area under the curve.
Discussion
This prospective cohort study, utilizing systematic postoperative ultrasonographic screening, revealed a 7.8% incidence of lower extremity DVT following shoulder arthroscopy. This rate substantially exceeds the 0.038% to 0.71% incidence typically reported in the literature for symptomatic events.7,25,30,35,36,43 The discrepancy is largely attributable to methodological differences: prior estimates primarily reflect symptomatic upper extremity events, whereas our protocol actively detected asymptomatic lower extremity DVT.13,40,50 This finding suggests that the true thrombotic risk after shoulder arthroscopy may be greater than previously recognized, a pattern similar to that seen in knee arthroscopy studies employing active surveillance.19,39,46
Beyond quantifying the incidence, our analysis sought to identify identifiable and quantifiable risk factors contributing to this elevated risk. The high incidence of VTE observed in this study (7.8%) is particularly noteworthy as it occurred in a surgical center located at an altitude of approximately 250 m, which is classified as low altitude according to standard definitions (generally, high altitude is considered to be >1500 m above sea level).4,8,17 This finding is crucial because it demonstrates that the significant risk of VTE following shoulder arthroscopy exists independently of the well-established risk factor of high altitude, which is known to induce a hypercoagulable state due to hypoxia-driven hemoconcentration and increased blood viscosity.9,24,48 The fact that our cohort exhibited a high thrombotic burden in a low-altitude setting underscores the potent effect of procedural factors, primarily operative duration, and challenges the perception that VTE is a concern only in specific high-risk environments.
The most significant finding is the identification of operative duration as an independent risk factor. Multivariable analysis, after adjusting for confounders such as age and hyperlipidemia, showed that each additional hour of operative duration increased the odds of postoperative VTE by a factor of 2.86 (95% CI, 1.26-6.52). This finding is supported by the retrospective analysis by Sager et al, 35 based on a large database, which also indicated an increased risk (OR, 2.10) for procedures lasting >80 minutes. The difference in effect size between our study (OR, 2.86) and Sager et al's (OR, 2.10) may be attributed to variations in study design, patient populations, or surgical techniques, highlighting the need for standardized VTE definitions and risk assessment in future multicenter studies. Together, these 2 studies confirm operative duration as a consistent and identifiable independent mechanical risk factor for VTE after shoulder arthroscopy.
Beyond operative duration, other patient characteristics showed suggestive trends. In our adjusted model, hyperlipidemia (OR, 3.78; P = .07) and serum calcium level (OR, 1.99 per 0.1 mmol/L increase; P = .07) were not statistically significant but demonstrated strong associations, warranting investigation in larger studies to clarify their potential role.
Analysis of thrombus location did not show a predilection for the dependent limb, and a notable proportion of DVTs (8/22; 36.4%) were bilateral. This pattern suggests that the thrombotic risk is mediated more by a systemic hypercoagulable state induced by surgical stress than by localized venous stasis from positioning. The identification of prolonged operative duration as the primary risk factor further supports this systemic mechanism.
A pivotal finding is that all thrombi were confined to the muscular calf veins, with a mean length of 2.47 cm and a mean diameter of 5.93 mm. Currently, significant variation exists in the management of isolated distal DVT. 26 When contextualized within the 2016 ACCP guidelines, 38 which suggest considering anticoagulation for extensive thrombi (eg, length >5 cm; maximal diameter >7 mm), the thrombi detected in our cohort fall below these proposed thresholds for immediate therapeutic intervention. Consequently, for patients undergoing shoulder arthroscopy, a strategy of routine postoperative ultrasonographic surveillance may represent a balanced approach, weighing the potential benefit of preventing thrombus extension against the inherent risk of bleeding complications associated with routine anticoagulation therapy. The optimal management of screening-detected, asymptomatic distal DVT remains a subject of clinical debate. In this study, all diagnosed DVTs, including asymptomatic cases, received therapeutic anticoagulation based on a precautionary institutional protocol aimed at preventing potential progression to fatal PE. It is important to note, however, that current major guidelines often do not recommend routine full anticoagulation for isolated, asymptomatic muscular calf vein thrombi, favoring surveillance instead. Therefore, while our protocol treated these thrombi, their clinical significance and the necessity of universal therapeutic anticoagulation are uncertain and warrant further investigation. The findings of this study highlight the need for future research to establish evidence-based management strategies for this specific patient population.
Notably, our study found no significant associations between preoperative coagulation profiles (eg, D-dimer, fibrinogen) or inflammatory markers (eg, CRP, myeloperoxidase) and VTE risk. The variability in these laboratory values due to individual patient factors and diurnal fluctuations is a valid concern. The single preoperative measurement in our study may lack the power to detect true associations, and dynamic perioperative monitoring might be more informative for capturing the acute thromboinflammatory response triggered by surgical trauma. Nevertheless, this negative finding is crucial, as it suggests that the mechanism of VTE following shoulder arthroscopy may be more driven by intraoperative mechanical factors and acute inflammatory responses triggered by surgical trauma itself, rather than by patients' preoperative hypercoagulable or inflammatory status. This underscores the importance of focusing on procedural variables, such as operative duration, and calls into question the utility of routine preoperative coagulation or inflammation screening for VTE risk stratification in this specific surgical context.
No significant link was found between preoperative inflammatory marker levels and VTE risk in this study. However, the mechanism behind operative duration as a risk factor may involve the acute thromboinflammatory response triggered during surgery. Modern pathophysiology suggests that surgical trauma can quickly activate immune cells, including neutrophils, leading to a cycle of proinflammatory and procoagulant responses. The rapid release of neutrophil extracellular traps is seen as a key event in this process.37,45 Longer surgeries clearly increase both the intensity and the duration of this response, creating a situation conducive to early postoperative thrombus formation. Therefore, future research should shift from static preoperative assessments to dynamic perioperative monitoring to better detect true pathogenic signals.
A key feature of this study is the preoperative measurement of all laboratory parameters, providing a baseline assessment independent of postoperative changes. Notably, our model, which relied solely on preoperative clinical variables, was able to identify patients at high risk for VTE. This suggests that risk stratification and planning for targeted preventive measures can be initiated before surgery, even in the absence of postoperative biomarkers.
Based on our findings, several practical considerations for risk mitigation emerge. First, for procedures with anticipated or actual durations exceeding the identified threshold (eg, 1.39 hours), the use of intermittent pneumatic compression devices on the calves during surgery warrants consideration, as this directly addresses intraoperative venous stasis. Second, facilitating early postoperative mobilization—a cornerstone of VTE prevention—should be emphasized, potentially supporting a shift toward outpatient surgery models when clinically appropriate to encourage ambulation. Finally, in the absence of high-level evidence for pharmacologic prophylaxis in shoulder arthroscopy, the potential role of low-dose aspirin for patients at elevated risk (eg, prolonged operative time plus other factors) could be a subject for future investigation, balancing efficacy and bleeding risk.
The operative duration cutoff of 1.39 hours established in this study offers surgical teams a simple and practical tool for intraoperative risk assessment. We suggest that patients whose expected or actual operative duration surpasses this limit be considered for enhanced postoperative monitoring.
Limitations
The present study has several limitations. First, since it was a single-center investigation where all procedures were carried out by 1 senior surgeon, although technical variability was minimized, the generalizability of the findings may be limited. Second, while a post hoc power analysis demonstrated sufficient power to detect the primary outcome, the relatively low number of VTE events (n = 22) may have reduced the ability to identify the true effects of certain secondary risk factors—such as hyperlipidemia and serum calcium—especially for those with moderate effect sizes that would require a larger sample to achieve statistical significance.
A key methodological consideration is that all surgeries in this cohort were performed with patients in the lateral decubitus position. Consequently, our findings regarding VTE risk, particularly the relationship with the dependent limb and operative duration, may not be directly generalizable to procedures conducted in the beach-chair position. The beach-chair position, which is common in shoulder arthroscopy, results in different biomechanical and hemodynamic conditions, potentially influencing venous stasis in the lower limbs. Therefore, comparing VTE incidence and risk profiles between these 2 positioning techniques represents a valuable direction for future research.
Furthermore, all laboratory parameters were measured preoperatively, and the lack of postoperative dynamic monitoring data prevented us from detecting acute biomarker changes caused by surgical stress or from establishing their timing relative to VTE events. However, this approach highlights the unique value of preoperative risk assessment by showing that early risk stratification can be done using readily available preoperative variables.
Fifth, the study cohort included few patients with severe obesity, and all surgeries were performed in an inpatient setting. These factors may limit the generalizability of our findings to populations with different BMI distributions or to the increasingly common outpatient arthroscopy practice.
Future studies should aim to perform large-scale, multicenter collaborative validation and use a longitudinal design, dynamically collecting inflammatory and coagulation biomarkers at key perioperative duration points (eg, 6 hours, 24 hours, and 72 hours postoperatively) to better understand the dynamic development of VTE.
Conclusion
This prospective cohort study with systematic ultrasonographic screening reveals a substantial incidence of VTE following shoulder arthroscopy, which is higher than previously recognized based on symptomatic diagnosis alone. Operative duration was established as a significant and identifiable independent risk factor, with a proposed cutoff of 1.39 hours serving as a practical tool for intraoperative risk assessment. These findings challenge the traditional perception of low VTE risk in shoulder arthroscopy and underscore the need to reconsider risk assessment and explore evidence-based, risk-stratified prevention strategies.
Footnotes
Appendix
Liver and Kidney Function Parameters a
| Characteristic b | Total (N = 282) | DVT (n = 22) | No DVT (n = 260) | P |
|---|---|---|---|---|
| AST | 20.25 (16.60-24.23) | 21.00 (19.20-26.40) | 20.20 (16.60-24.05) | .29 |
| ALT | 18.05 (13.70-26.38) | 21.10 (17.15-24.70) | 17.80 (13.70-26.60) | .38 |
| GGT | 21.70 (15.88-38.15) | 22.70 (20.00-51.80) | 21.60 (15.85-37.90) | .37 |
| ALP | 82.30 (66.43-98.53) | 91.10 (76.85-106.10) | 80.80 (65.30-96.40) | .25 |
| CHE | 8337.00 (7365.00-9496.00) | 7988.00 (7397.00-9062.00) | 8360.00 (7378.00-9510.00) | .64 |
| TP | 71.15 (68.28-74.00) | 70.00 (68.15-74.15) | 71.20 (68.45-73.95) | .84 |
| ALB | 43.50 (41.50-45.30) | 43.20 (40.55-44.85) | 43.50 (41.50-45.30) | .61 |
| GLO | 27.80 (25.30-30.13) | 26.60 (26.10-31.85) | 27.80 (25.30-30.00) | .69 |
| A/G | 1.56 (1.41-1.72) | 1.55 (1.40-1.67) | 1.56 (1.41-1.72) | .59 |
| TBIL | 12.30 (9.25-14.90) | 13.50 (10.80-16.10) | 12.20 (9.05-14.75) | .19 |
| DBIL | 2.00 (1.60-2.60) | 2.10 (1.75-2.25) | 2.00 (1.60-2.60) | .63 |
| IBIL | 10.30 (7.65-12.43) | 11.30 (8.95-13.75) | 10.30 (7.40-12.20) | .12 |
| TBA | 3.00 (1.88-4.60) | 3.90 (2.60-5.45) | 3.00 (1.80-4.60) | .32 |
| K | 4.10 (3.87-4.30) | 4.26 (3.91-4.45) | 4.10 (3.86-4.29) | .35 |
| Na | 139.90 (138.85-141.70) | 140.80 (139.70-141.90) | 139.80 (138.65-141.65) | .26 |
| Cl | 103.10 (101.35-105.40) | 104.20 (102.30-105.50) | 103.0 (101.30-105.10) | .37 |
| Ca | 2.30 (2.24-2.35) | 2.36 (2.28-2.42) | 2.29 (2.24-2.34) |
|
| CO2-CP | 26.31 (24.22-28.09) | 27.66 (25.74-29.61) | 26.28 (24.17-27.97) | .10 |
| GLU | 5.37 (4.84-6.31) | 5.47 (4.79-6.12) | 5.32 (4.88-6.32) | .98 |
Data are presented as median (IQR). Boldface P values indicate a statistically significant difference between the study groups (P < .05). A/G, albumin-to-globulin ratio; ALB, albumin(g/L); ALP, alkaline phosphatase(U/L); ALT, alanine aminotransferase(U/L); AST, aspartate aminotransferase(U/L); Ca, calcium (mmol/L); CHE, cholinesterase(U/L); Cl, chloride (mmol/L); CO2-CP, carbon dioxide combining power (mmol/L); DBIL, direct bilirubin(μmol/L); DVT, deep vein thrombosis; GGT, gamma-glutamyl transferase(U/L); GLO, globulin(g/L); GLU, glucose (mmol/L); IBIL, indirect bilirubin(μmol/L); K, potassium (mmol/L); Na, sodium (mmol/L); TBA, total bile acid(μmol/L); TBIL, total bilirubin(μmol/L); TP, total protein(g/L).
See the Methods section for definitions.
Final revision submitted April 14, 2026; accepted April 17, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Jilin Province Health Talent Special Project (grant No. JLSRCZX2025-145 to P.X.).
Ethical approval for this study was obtained from the ethics committee of The First Hospital of Jilin University (reference No. 25K453-001).