
Abstract
Background:
Ulnar collateral ligament (UCL) reconstruction has historically been considered the gold standard treatment for severe UCL tears. With the advent of suture-spanning repair techniques, some studies suggest that UCL repair is being performed with increasing frequency. This study provides a large analysis of UCL reconstruction versus repair trends in the United States following the introduction of suture-spanning repair techniques.
Purpose:
To compare the prevalence and complication rates of UCL reconstruction versus repair over a 5-year span following the introduction of suture spanning repair techniques. We also sought to determine if there was an age-related preference for reconstruction versus repair and whether the addition of an ulnar nerve transposition (UNT) affected short-term complication rates.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Using the Merative MarketScan research databases, which contain deidentified patient national claims information, we retrospectively identified patients aged 14 to 30 years who underwent UCL reconstruction or repair between 2016 and 2021, with or without UNT. Patients with a fracture diagnosis at the time of surgery were excluded. Demographic information including age, sex, and geographic region was collected. The number of patients who experienced infection, ulnar neuropathy, device-related complications, and unspecified complications were obtained for each procedure.
Results:
A total of 1191 reconstruction patients and 696 repair patients were identified. 36.8% of patients who underwent either reconstruction or repair had a concomitant UNT. UCL reconstruction patients were approximately 3 years older than repair patients on average (P < .001). Male patients accounted for 89.5% of reconstruction patients and 77.7% of repair patients. From 2016 to 2021, the number of reconstructions declined 32.0% and the number of repairs increased 81.6%. There were no differences in the rate of infection (P = .36) and ulnar neuropathy (P = .73) between reconstruction and repair. The overall risk of developing any complication was higher for repair patients (1.58%) than reconstruction patients (0.67%); however, this difference was not significant (P = .09).
Conclusion:
Between 2016 and 2021, following the introduction of suture spanning UCL repair techniques, the number of UCL repairs increased and the number of reconstructions decreased. There was no difference in complication rates between UCL repair and UCL reconstruction and the rate of complication for either surgery remains low.
Tears of the UCL are often seen in throwing athletes who engage in overhead movements that generate high valgus stress on the medial elbow during the late cocking and acceleration phases of throwing.10,25 These injuries can also occur in individuals who sustain acute and severe valgus stress, including wrestlers and gymnasts.12,19
Treatment of UCL tears may begin with nonoperative methods, including a period of rest and strengthening of the flexor-pronator mass. Surgery is indicated for symptomatic patients who fail nonoperative treatment and are willing to participate in lengthy rehabilitation. 19 Recently, the operative management of UCL tears has become more common, with a study reporting an 11-fold increase over the past decade. 27 Surgery has traditionally involved reconstruction of the UCL using the modified Jobe, docking, or hybrid interference screw technique. 19 However, there has been an increasing incidence of UCL repair following the introduction of a novel suture spanning technique in 2016.6,8 A recent study found that the incidence rate ratio of UCL repair compared with reconstruction significantly increased each year over the past decade. 3 Another study demonstrated that repairs constituted 23% of UCL tear surgeries in 2010, increasing to 40% by 2020. 27 Both studies found that concomitant ulnar nerve procedures occurred in approximately 25% of UCL reconstructions or repairs.3,27
While operative management, especially repair, of UCL tears is becoming increasingly common, there is a paucity of data examining trends in reconstruction versus repair throughout the entire United States. Furthermore, there is a lack of literature investigating complications after each procedure, as well as the impact of concomitant UNT on the rate of complications.
The primary purpose of this study was to compare the prevalence and complication rates of UCL reconstructions versus repairs after the introduction of suture spanning repair techniques. We also investigated whether there was an age-related preference for reconstruction versus repair. We sought to determine if the type of procedure and the addition of an ulnar nerve procedure affected short-term complication rates. We hypothesized that repairs have become increasingly common over time, while reconstructions have been performed less often with the advent of suture spanning techniques. We hypothesized that younger patients would preferentially receive repair, whereas older patients would more commonly undergo reconstruction. We also hypothesized that reconstruction patients are at higher risk of complication than repair patients and undergoing concomitant UNT increases rate of complication.
Methods
Data for this retrospective study were queried from a database between January 1, 2016, and December 31, 2021. This 5-year range was selected in order to isolate pure reconstruction and repair procedures. Recent use of hybrid techniques combining repair and reconstruction may make the results more difficult to interpret. The Merative MarketScan research database (https://www.merative.com/documents/merative-marketscan-research-databases) is among the largest and most comprehensive, representing >273 million privately insured patients in the United States. UCL reconstruction and UCL repair procedures were identified using International Classification of Diseases, Tenth Revision, Procedure Coding System (ICD-10-PCS) codes. UCL reconstructions were obtained from procedure codes 0MR307 and 0MR407 (replacement of elbow bursa and ligament). Numerous codes were used to search for UCL repairs (AppendixTable A1). UNTs were found under code 01S40ZZ (reposition ulnar nerve), and it was noted whether reconstruction and repair patients received concomitant UNT. Of the patients who underwent UCL reconstruction or repair, patients between 14 and 30 years of age with a diagnosis of UCL rupture (S53.3) or sprain (S53.44) were included in the study. Patients with any fracture diagnosis at the time of surgery were excluded. Patient demographic data, including age, sex, and geographic region where the procedure was performed, were collected from the database. The occurrence of complications, including infection, ulnar neuropathy, device-related complications, and unspecified complications, was determined using many ICD-10 Clinical Modification (ICD-10-CM) codes (AppendixTable A2). Complications that occurred within 90 days from surgery were collected for data analysis. Standardized ICD-10 coding was used for identification of both cohorts to minimize selection bias; however, confounding variables and misclassification bias inherent to administrative claims data could not be fully accounted for.
The demographic data were analyzed with descriptive statistics. Welch t test and Fisher exact test were used to confirm if observed differences in age distribution or sex between the procedures were significant. Complication contingency data were also compared using Fisher exact test, as the complications associated with each procedure often affected ≤5 patients. The significance level was set at .05.
Results
Between 2016 and 2021, we found 1191 UCL reconstructions and 696 UCL repairs performed on patients 14 to 30 years of age in the MarketScan database. On average, UCL reconstruction patients were nearly 3 years older than UCL repair patients (P < .001) (Table 1). The age distribution of reconstruction patients is symmetric and normal (Figure 1). However, the repair distribution appears to be positively skewed, further suggesting that the mean repair patient is younger than the mean reconstruction patient. Men accounted for 89.5% of UCL reconstruction procedures and 77.7% of repairs (Table 1). Operatively managed UCL injuries were most frequently observed in parts of the Southeast and Midwest (Figure 2). Alabama, Delaware, and Hawaii were among the states with the highest proportion of UCL procedures performed per 100,000 young patients. The total number of UCL reconstruction procedures declined from 250 cases in 2016 to 170 cases in 2021, showing decreases in both pure reconstruction (UNT–) and combined reconstruction (UNT+). UCL repairs followed an opposite trend, rising from 76 cases in 2016 to 138 cases in 2021, with increases in both the UNT– and the UNT+ subcategories (Figure 3). Of all patients who underwent UCL reconstruction or repair, 36.8% received a concurrent UNT; 39% of reconstruction patients and 32.9% of repair patients were treated with concomitant UNT.
Demographic Data for Ulnar Collateral Ligament Reconstruction and Repair Patients a
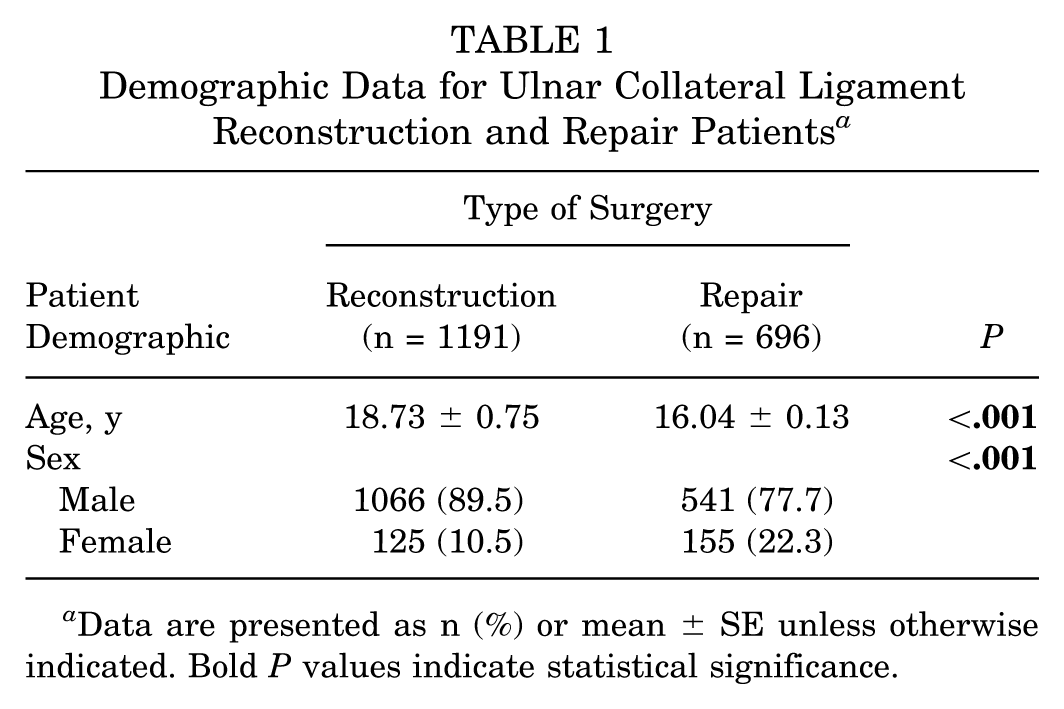
Data are presented as n (%) or mean ± SE unless otherwise indicated. Bold P values indicate statistical significance.
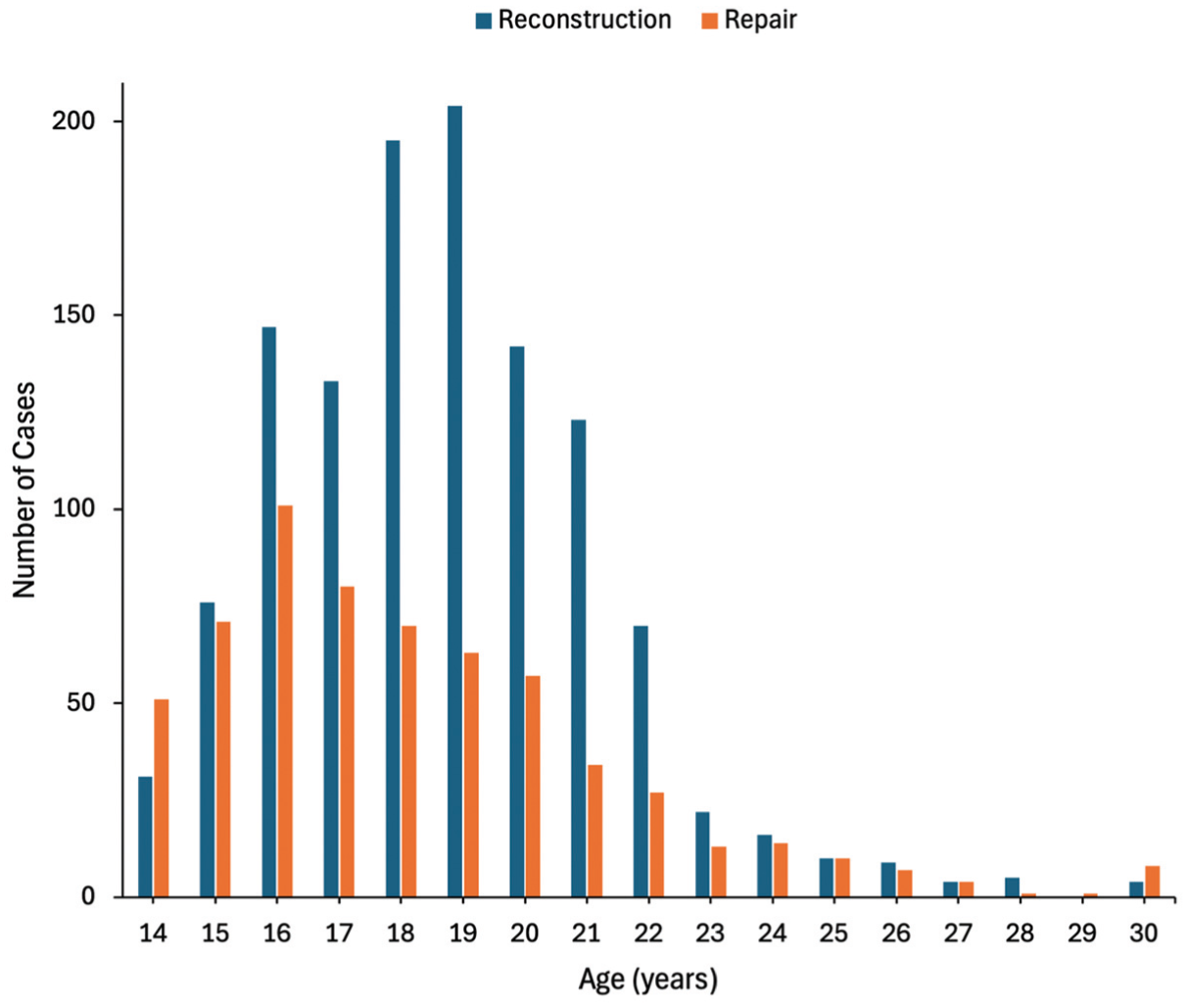
Age distribution of patients aged 14 to 30 years receiving ulnar collateral ligament reconstruction and repair procedures.
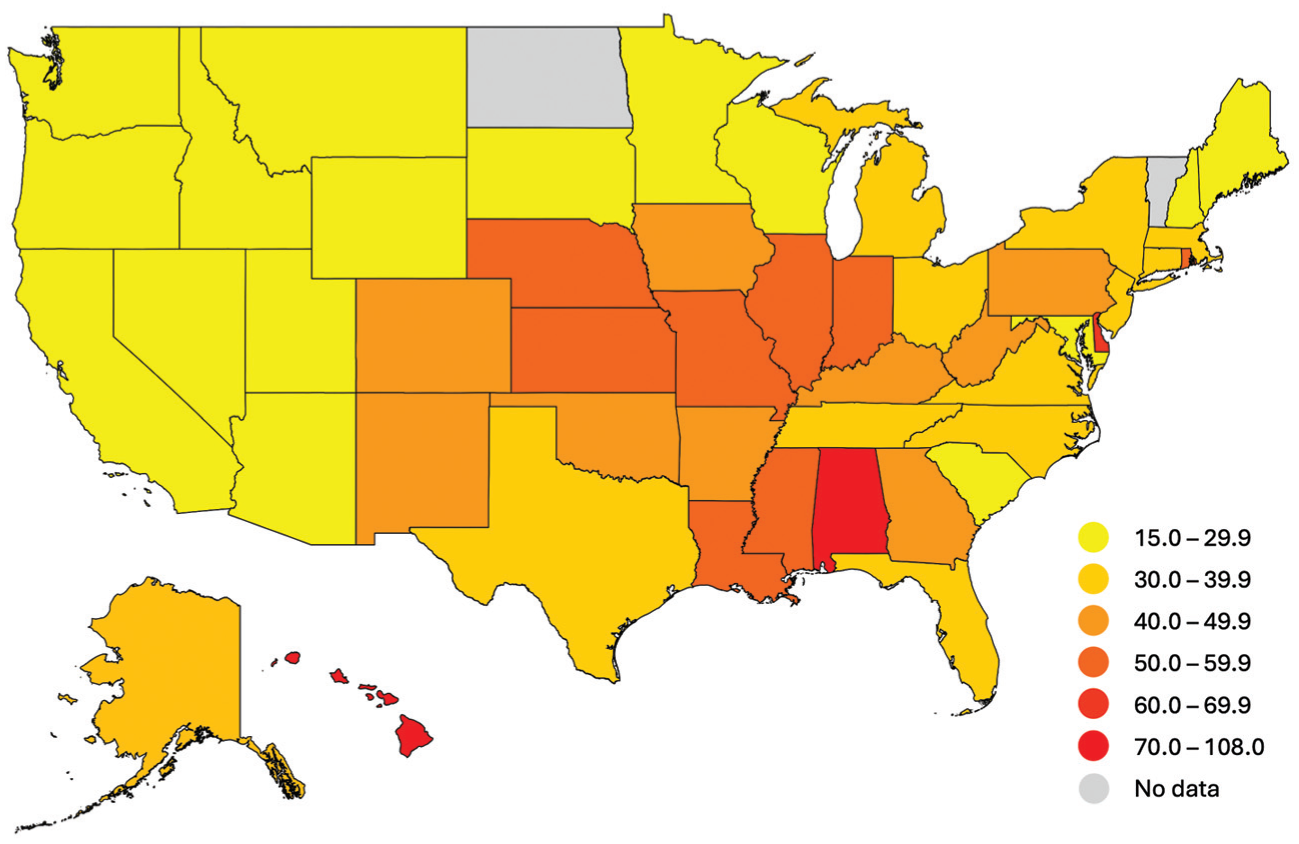
Number of surgically treated ulnar collateral ligament injuries per 100,000 privately insured youth (aged 14 to 22 years) in each state. Data were unavailable for North Dakota and Vermont.
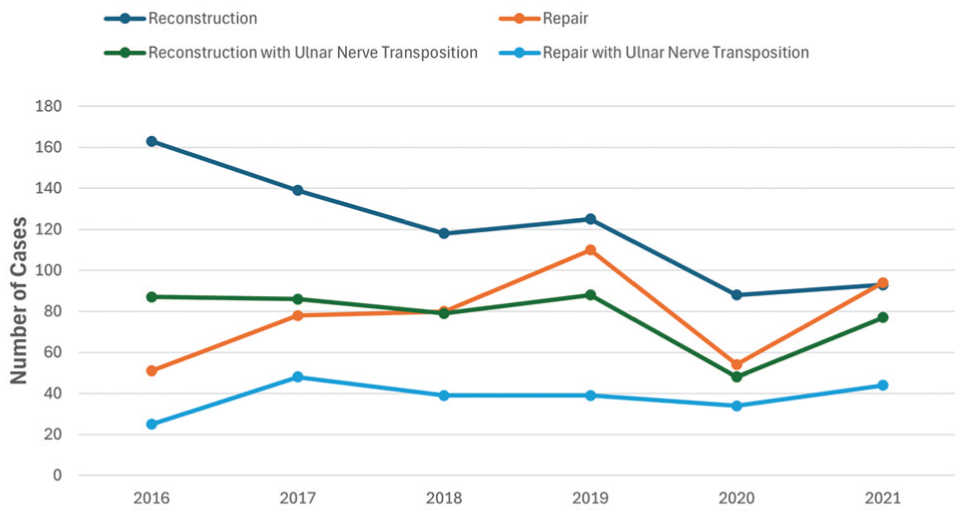
Trends in the number of ulnar collateral ligament reconstruction and repair procedures performed between 2016 and 2021.
The complication rates for reconstruction and repair were very low at 0.67% and 1.58% respectively, indicating the low risk of UCL surgery. The rate of individual complications, including infection and ulnar neuropathy, were also compared between these groups (Figure 4). There were no significant differences in rate of infection (P = .36), rate of ulnar neuropathy (P = .73), or rate of any complication overall (P = .09) between patients receiving any reconstruction procedure (UNT– and UNT+) and patients receiving any repair procedure (UNT– and UNT+). Not shown are the rates of device-related complications and unspecified complications, which can be found in Table 2. Device-related complications were exclusively observed in repair patients. Out of 1191 UCL reconstruction procedures, a single unspecified complication was documented. No unspecified complications occurred following UCL repair. As shown in Figure 5, performing reconstruction with UNT did not affect the rate of infection (P > .99), ulnar neuropathy (P = .08), or any complication (P = .27). Similarly, no differences in rate of infection (P = .25), rate of ulnar neuropathy (P = .60), or any complication (P = .35) were observed between repair with UNT and repair alone (Figure 6).
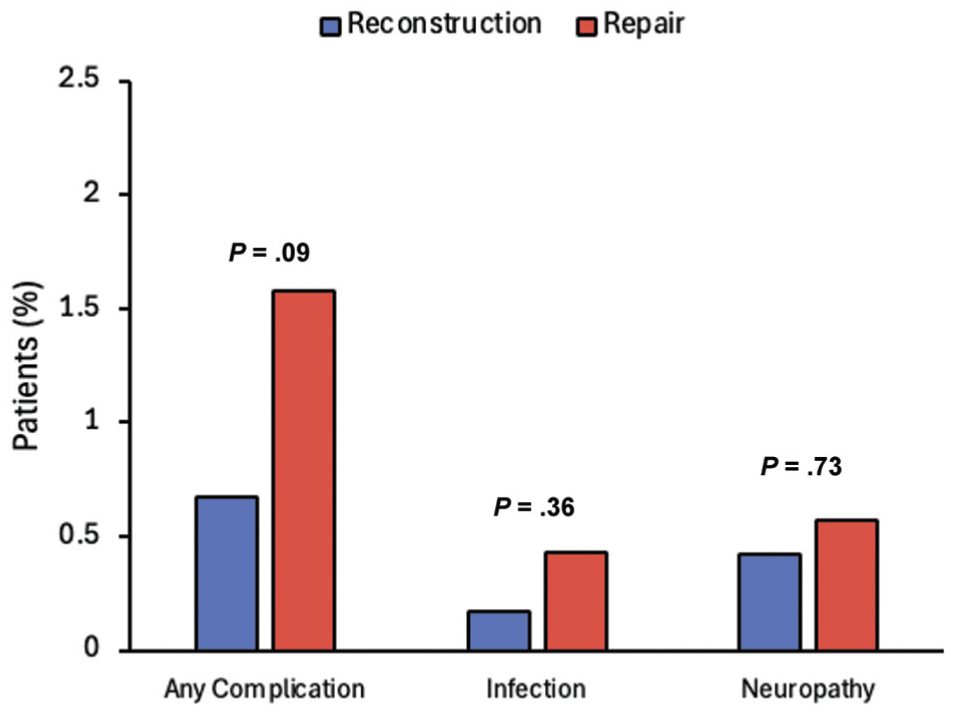
Rates of infection, ulnar neuropathy, or any complication in ulnar collateral ligament reconstruction and repair patients.
Complications of Ulnar Collateral Ligament Reconstruction and Repair, With or Without a UNT a
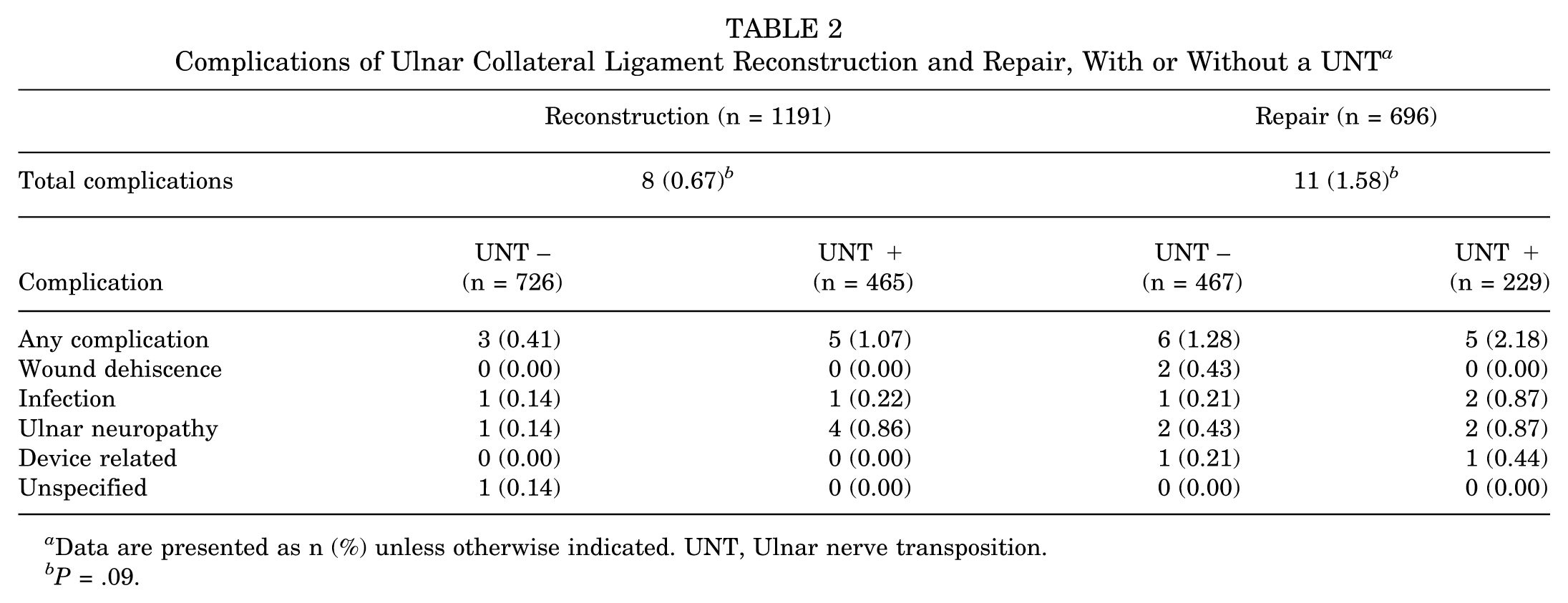
Data are presented as n (%) unless otherwise indicated. UNT, Ulnar nerve transposition.
P = .09.
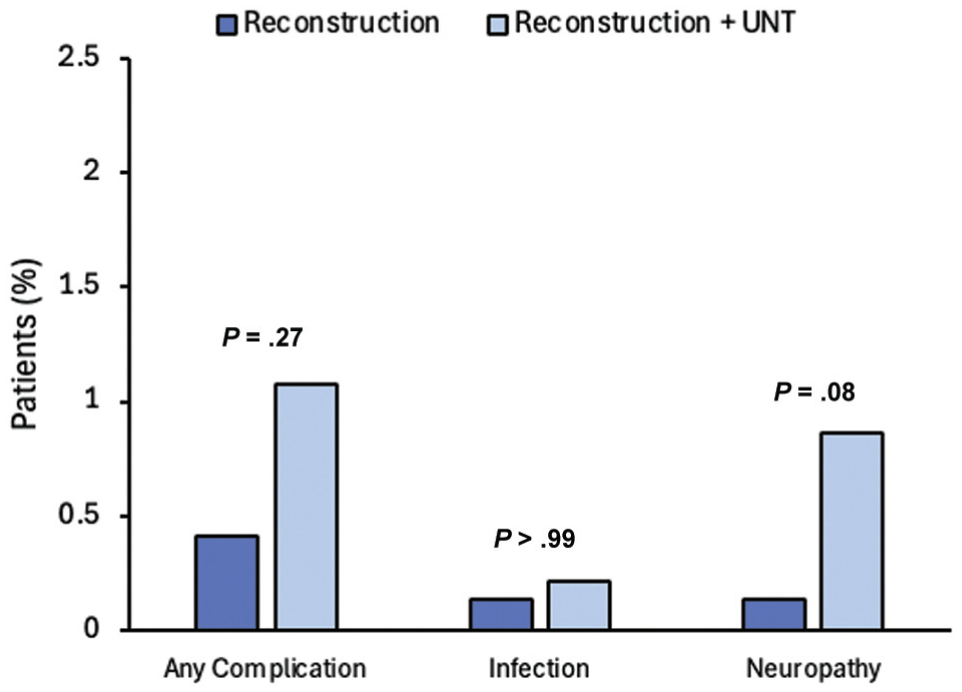
Rates of infection, ulnar neuropathy, or any complication in reconstruction patients with or without ulnar nerve transposition.
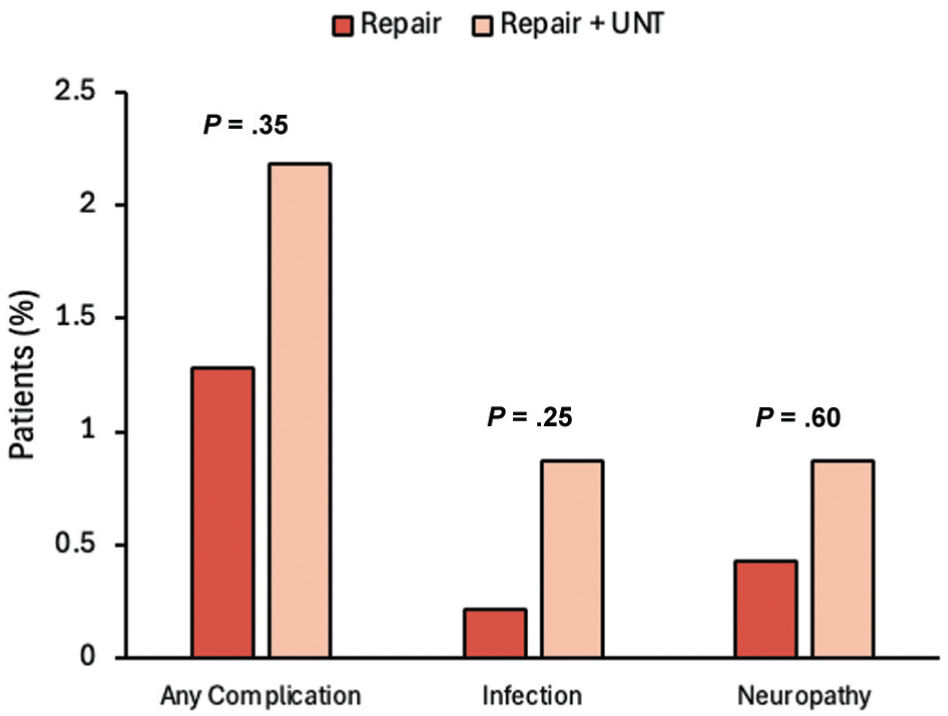
Rates of infection, ulnar neuropathy, or any complication in repair patients with or without ulnar nerve transposition.
Discussion
We found that the number of repairs has risen as reconstructions have declined in recent years, supporting our hypothesis. We confirmed our hypothesis that younger patients are more commonly treated with repair and that older patients more often receive reconstruction. Despite our prediction that reconstruction patients would be at greater risk, we observed no difference in overall complication rate. Overall, the number of complications in either group was very low. Concomitant UNT did not affect complication rate, leading us to reject our hypothesis that UNT places patients at higher risk. A recent study by Lynch et al 13 similarly reported equivalent clinical outcomes among reconstruction patients with or without concomitant UNT.
The primary finding of this study was that the prevalence of UCL repairs has increased amid decreases in UCL reconstruction. This trend in reconstruction stands in contrast to other studies, which note a rising rate of reconstruction in professional athletes from 1974 to 2016 4 and in the general population from 2007 to 2016. 2 However, trends appear to have changed after 2016. Bi et al 3 observed a slight decrease in reconstruction cases and an increase in repairs from 2016 to 2019, mirroring our findings. A study by Solomito et al 23 showed that there was little change in the number of reconstructions performed on 15- to 19-year-olds from 2016 to 2019, and demand for reconstruction for 20- to 24-year-olds actually decreased over the same period. Similarly, a study of college athletes showed a slight decrease in UCL reconstructions each baseball season from 2016 to 2019. 20
We suspect that there are 2 reasons for an increase in repairs as reconstructions decline: (1) the development of suture spanning repair constructs that may match the strength of standard reconstruction and (2) the shorter recovery time associated with UCL repair. Early studies that examined repair as an operative treatment for UCL tear reported unfavorable results.1,5 However, recent literature implementing these novel repair constructs also demonstrated biomechanical strength 8 and outcomes 22 comparable with a standard reconstruction. Additionally, patients who receive UCL reconstruction generally return to sport within 11 to 12 months21,24 but may require up to 16 months. 11 In contrast, repair patients may experience a 6- to 9-month recovery.7,15 The indications for when to choose a repair with suture spanning techniques versus graft reconstruction continue to evolve. Decision regarding the type of surgery is dependent on several factors including, but not limited to, injury chronicity, patient age, sport, level of play, and expected throwing demand, among others. Although the prevalence of reconstruction is declining, it is still a highly effective technique for treating severe or complete UCL tears and remains more common than repair.
Existing literature broadly examines the age distribution of patients receiving either procedure, spanning from <18 to >59 years.2,9 In this study, we focus on 14- to 30-year-olds to better understand a disproportionately affected population. Erickson et al 9 and Mahure et al 14 have observed that the incidence of reconstruction is much higher among younger patients, particularly those aged 15 to 19 years. There is growing evidence that the mean age of patients receiving either reconstruction or repair has dropped considerably in recent years.17,26 Within this younger cohort, we found that UCL repair patients were approximately 3 years younger than reconstruction patients on average. Although younger patients have less native bone present for osseous tunnels, we propose that surgeons are more likely to recommend repair to patients aged <16 because of concerns about potential physeal growth arrest. Additionally, younger patients are often more suited to repair because they typically have more robust ligaments, having experienced fewer years of ligament attrition from throwing sports. These younger patients aged <16 may also be more likely to have partial ligament injuries, which are not severe enough to require UCL reconstruction. Older patients may undergo reconstruction at a high rate due to poorer quality of the native ligament with chronic changes including calcification, hypertrophy or attrition, and periligamentous edema or thickening. It is also possible that repair is sufficient for younger athletes throwing at lower rates of velocity and workload, whereas UCL reconstruction may be more resilient to chronic workloads. The design of this study only allows us to detect an age-related preference, but future studies could explore whether this preference is based on the demands that younger and older patients place on the UCL.
We observed a high number of UCL procedures per capita in 3 states: Alabama, Delaware, and Hawaii. Home to several high-volume, prominent shoulder and elbow surgeons and such centers as Andrews Sports Medicine, Alabama is a destination state for UCL surgery. However, Delaware and Hawaii are not particularly high-volume states for UCL procedures. Because both states have small populations, small variations in the number of privately insured patients aged 14 to 30 could skew the incidence of UCL surgery artificially high. These observations suggest that the geographic distribution shown in Figure 2 may have limited accuracy for less populous states.
There was no difference in complication rates between repair and reconstruction patients. Despite being a potentially shorter and less complex procedure, repairs do not seem to confer protection from complication. As indications for UCL repair expand and surgeons utilize the procedure more frequently, we may observe that complication rates for repair increase overall. Additionally, undergoing concomitant UNT did not place repair or reconstruction patients at elevated complication risk. In general, regardless of procedure, UCL surgery is safe with low risk of complications.
As a database study, we are inherently limited in our ability to comprehensively capture all complications. Although several studies agree that reconstruction and repair are safe procedures with low complication rates, they reported slightly higher rates of complication than what we found. Nagy et al 16 observed complication rates of 8.59% for modified Jobe reconstruction and 2.35% for docking reconstruction, with the present study showing a rate 0.67%. A systematic review by Puga et al 18 reported complication rates between 5.3% and 11.9% for repair, compared with our 1.58%.
Limitations
This study has limitations on generalizability. The database represents a subsection of the US population and only contains privately insured patients, who are known to undergo surgical intervention more often than patients with public insurance. Database information is limited by the accuracy of coding and billing, and patients become active in the database after 18 to 24 months. Although athletes and baseball players likely account for a large portion of 14- to 30-year-old UCL injury patients, we cannot draw direct conclusions about this population from the study. Patients who had both reconstruction and repair codes were entered as reconstruction. This is a limitation of the study; however, hybrid procedures were not very common in the time frame of this study. The database cannot determine whether patients sustained chronic attritional UCL injuries like those commonly observed in overhead throwing athletes, or acute traumatic injuries characteristic of wrestlers and gymnasts. The database did not specify whether UCL tears were proximal, distal, or midsubstance, which is an important factor in a surgeon's decision to perform a repair. For example, a tear on the well-vascularized proximal UCL is much more amenable to repair than a distal tear. Repair may not be suitable for a midsubstance tear in a throwing athlete but may be appropriate for the same midsubstance tear in an average patient who does not participate in sports. The database does not include information regarding whether or not a repair included a suture spanning construct nor does it include outcome data, such as time to return to play or performance metrics. However, for many surgeons who perform both UCL repair and UCL reconstruction for athletes and nonathletes, the use of suture spanning augmentation has increased substantially since the concept was introduced by Dugas 6 in 2016. Another limitation is that indications for surgery and factors affecting treatment decisions were not included. Although the database specifies whether a procedure included a concomitant UNT, it is unknown whether patients received either a decompression or a transposition. As techniques evolve and surgeons begin to incorporate suture spanning augmentation techniques in reconstructions, this kind of analysis will become less insightful because there is no CPT code for a combined procedure.
Conclusion
Between 2016 and 2021, following the introduction of suture spanning UCL repair techniques, the number of UCL repairs increased, and the number of reconstructions decreased. There was no difference in complication rates between UCL repair and UCL reconstruction, and the rate of complication for either surgery remains low.
Footnotes
Appendix
International Classification of Diseases, Tenth Revision, Clinical Modification, Codes for the Complications of UCL Reconstruction and Repair a
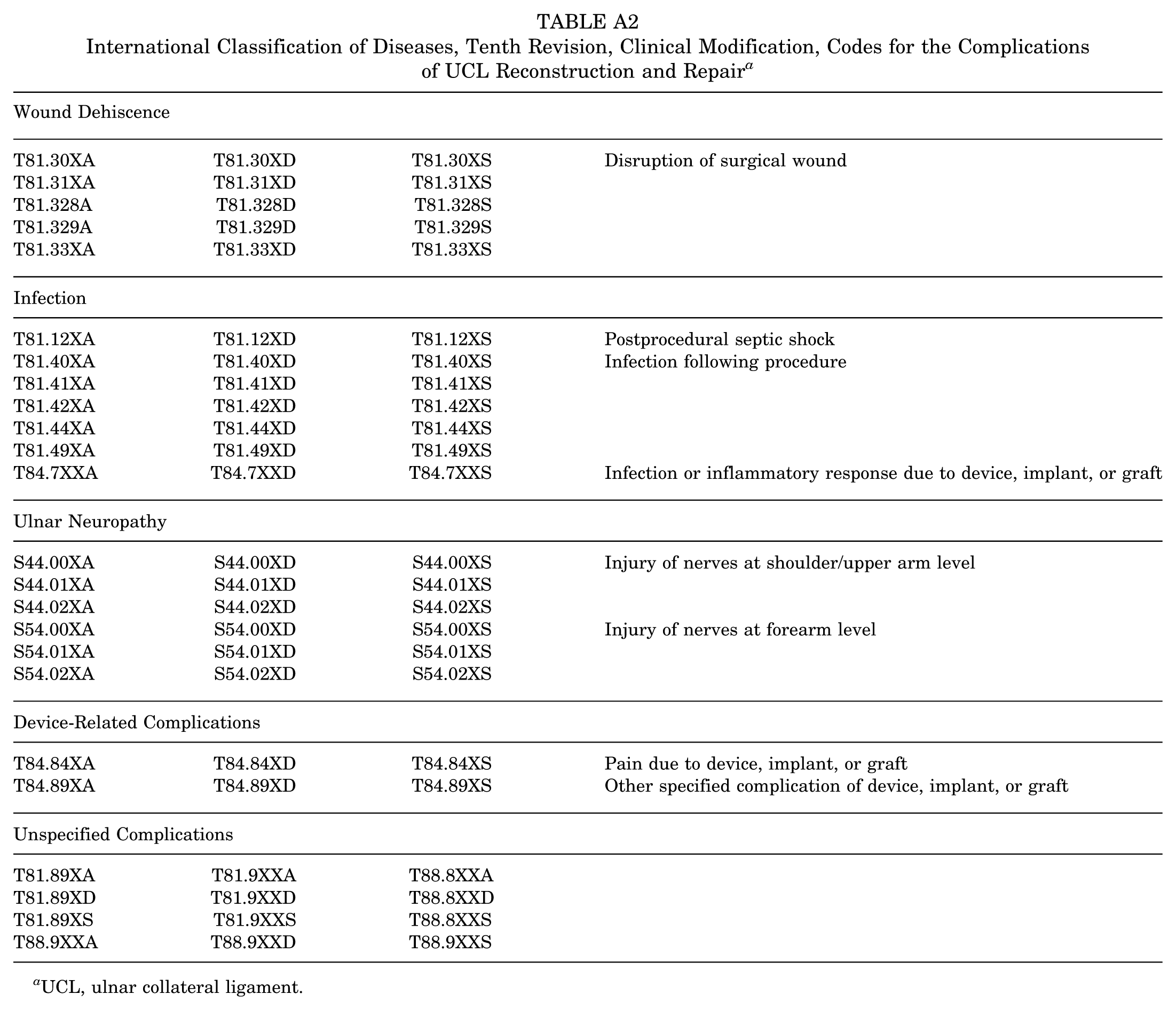
| Wound Dehiscence | |||
|---|---|---|---|
| T81.30XA | T81.30XD | T81.30XS | Disruption of surgical wound |
| T81.31XA | T81.31XD | T81.31XS | |
| T81.328A | T81.328D | T81.328S | |
| T81.329A | T81.329D | T81.329S | |
| T81.33XA | T81.33XD | T81.33XS | |
| Infection | |||
| T81.12XA | T81.12XD | T81.12XS | Postprocedural septic shock |
| T81.40XA | T81.40XD | T81.40XS | Infection following procedure |
| T81.41XA | T81.41XD | T81.41XS | |
| T81.42XA | T81.42XD | T81.42XS | |
| T81.44XA | T81.44XD | T81.44XS | |
| T81.49XA | T81.49XD | T81.49XS | |
| T84.7XXA | T84.7XXD | T84.7XXS | Infection or inflammatory response due to device, implant, or graft |
| Ulnar Neuropathy | |||
| S44.00XA | S44.00XD | S44.00XS | Injury of nerves at shoulder/upper arm level |
| S44.01XA | S44.01XD | S44.01XS | |
| S44.02XA | S44.02XD | S44.02XS | |
| S54.00XA | S54.00XD | S54.00XS | Injury of nerves at forearm level |
| S54.01XA | S54.01XD | S54.01XS | |
| S54.02XA | S54.02XD | S54.02XS | |
| Device-Related Complications | |||
| T84.84XA | T84.84XD | T84.84XS | Pain due to device, implant, or graft |
| T84.89XA | T84.89XD | T84.89XS | Other specified complication of device, implant, or graft |
| Unspecified Complications | |||
| T81.89XA | T81.9XXA | T88.8XXA | |
| T81.89XD | T81.9XXD | T88.8XXD | |
| T81.89XS | T81.9XXS | T88.8XXS | |
| T88.9XXA | T88.9XXD | T88.9XXS | |
UCL, ulnar collateral ligament.
Final revision submitted April 6, 2026; accepted April 28, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.K.E. has received fees for advice or consultation with Arthrex Inc, has received travel reimbursement, and is on the editorial board of the Journal of Arthroscopy. R.J.F. has received fees for advice or consultation with Advita Inc, speaking and lecture fees, and travel reimbursement.
Ethical approval was not sought for the present study.