
Abstract
Background:
Achilles tendon rupture is a rare but potentially career-altering injury in elite basketball athletes. Contemporary data specific to National Basketball Association (NBA) players are limited, particularly regarding return-to-play (RTP) timing, functional outcomes, and long-term incidence trends in the modern high-pace era.
Purpose:
To evaluate RTP rates, time to return, postinjury performance changes, and temporal patterns of Achilles tendon rupture in NBA players over a 25-year period.
Study Design:
Descriptive epidemiology study.
Methods:
NBA players with a confirmed Achilles tendon rupture between the 2000-2001 and 2024-2025 seasons were identified through multisource verification, including team announcements, league injury reports, Basketball Reference records, NBA.com injury logs, and contemporaneous reporting from major sports media outlets. RTP was defined as participation in at least one official NBA regular season or postseason game after the index rupture. Season-level performance metrics were extracted for the final full preinjury season and the first full postreturn season. Paired pre- versus postinjury comparisons were performed, effect sizes were calculated using Cohen d, and selected metrics were normalized per 48 minutes to account for changes in playing time. The annual rupture incidence was evaluated in relation to league-wide pace using Pearson correlation.
Results:
A total of 22 NBA players sustained a confirmed Achilles rupture. Among athletes with adequate follow-up (n = 15), 13 players (86.7%) returned to NBA competition. The mean time to RTP was 10.8 ± 4.3 months. Significant declines were observed in minutes per game (−7.6 minutes; P < .001), points per game (−5.4; P < .001), effective field goal percentage (−0.055; P = .005), rebounds (−1.3; P = .008), assists (−1.0; P = .002), defensive rebounds (−1.01; P = .014), steals (−0.28; P = .001), and blocks (−0.19; P = .026). When normalized per 48 minutes, scoring production still decreased significantly (−3.36 points; P = .004), while defensive metrics were preserved. Games started decreased substantially (−44 percentage points; P = .003). Annual rupture incidence remained low overall, with a notable spike in the 2024-2025 season, but no significant correlation with league pace was observed.
Conclusion:
This study showed that most NBA players with adequate follow-up returned to professional play after Achilles tendon rupture, typically within approximately 11 months. However, reductions in playing time, scoring output, offensive efficiency, and starting role prevalence were common after return. Per-48-minute analyses suggested that scoring decline persisted even after accounting for reduced playing time, whereas several defensive and rebounding metrics were relatively preserved. Annual rupture incidence remained low overall, although a notable cluster was observed during the 2024-2025 season. These data may be helpful for counseling players regarding performance expectations and decision-making after Achilles tendon rupture in elite basketball players.
Keywords
Achilles tendon rupture is a serious and potentially career-altering injury sustained by elite basketball players.2,6,10 The injury requires prolonged rehabilitation, often exceeding 9 months, and has historically been associated with reduced performance, shortened careers, and substantial economic impact for professional teams.2,6,8,10,13 In the National Basketball Association (NBA), Achilles ruptures have gained particular attention because they frequently affect high-usage, high-value athletes whose performance relies heavily on explosive acceleration, deceleration, and vertical power.2,6,8,10,13
Previous studies in professional basketball have been limited by small cohorts, heterogeneous definitions of return to play (RTP), inconsistent confirmation of injury type, and a lack of standardized performance comparisons before and after rupture.2,5,6,10,13 Most reports have also combined players from multiple eras, leagues, or competition levels, making it difficult to characterize contemporary outcomes in the modern NBA, which differs substantially in pace, spacing, workload demands, and medical management. Although several case series and narrative reviews have suggested that Achilles rupture can be career-altering, robust quantitative data specific to NBA athletes remain scarce.8,13
In recent years, the NBA has undergone major changes in game style and physical demands, including a historic rise in pace and possessions per game.11,12 These changes may influence tendon loading and injury risk, yet long-term trends in Achilles rupture incidence have not been rigorously evaluated.4,7,9 At the same time, improvements in surgical repair techniques, biological augmentation, and accelerated rehabilitation protocols may have altered the likelihood and timing of successful RTP. 4 Despite these developments, no contemporary study has integrated injury confirmation, RTP timing, season-level performance metrics, and league-wide temporal trends over a multidecade period.2,6,8,10,13
A clearer understanding of functional outcomes after Achilles rupture in NBA athletes is important for clinicians, performance specialists, front office executives, and players themselves. Quantifying changes in playing time, scoring efficiency, and role allocation after injury may help refine return-to-sport counseling, expectation management, and medical decision-making. Additionally, identifying long-term incidence patterns may contribute to improved workload strategies and injury prevention efforts.3,7
Therefore, the purpose of this study was to evaluate RTP rates, time to return, postinjury performance changes, and temporal trends in Achilles tendon ruptures among NBA players over a 25-year period. We hypothesized that (1) most players would successfully return to NBA play, (2) significant reductions in playing time and offensive production would occur after return, and (3) rupture incidence would show temporal variation in relation to league pace.
Methods
Study Design, Ethics, and Data Sources
This study was conducted as a retrospective observational analysis of the data of NBA players who sustained a confirmed Achilles tendon rupture between the 2000-2001 and 2024-2025 NBA seasons. The primary objectives were to quantify RTP rates and time to return, compare preinjury and postreturn on-court performance, and evaluate temporal patterns in Achilles tendon rupture incidence in relation to league-wide pace. Because all data were obtained from publicly available sources and no protected health information was used, institutional review board approval and individual consent were not required. All data sources and statistical procedures were publicly accessible, and the full data set used in the analysis is provided in the Supplement.
Case Identification and Eligibility Criteria
Achilles tendon ruptures were identified through a multisource verification process using team medical statements and press releases, NBA official injury reports, NBA.com injury logs, Basketball Reference player transaction and game availability records, and contemporaneous reporting from major sports media outlets, including ESPN and The Athletic. A case was included only when the injury was explicitly described as an “Achilles tendon rupture” or “torn Achilles” by the player's team, the league, or a contemporary report. Partial tears, Achilles tendinopathy, and nonspecific lower leg injuries were excluded. When duplicate reports referred to the same player and injury event, they were treated as a single rupture episode and cross-checked across sources to confirm the date and injury type. For players injured during the 2024-2025 season, RTP status was recorded as pending when insufficient rehabilitation time had elapsed.
RTP and Performance Outcomes
RTP was defined as participation in at least one official NBA regular season or postseason game after the index Achilles tendon rupture. Time to return was calculated in months from the date of injury to the date of the first NBA game appearance after injury. Career-ending injury was defined as failure to return to any NBA game after the rupture among players with adequate follow-up. Adequate follow-up was defined as at least 24 months after the index Achilles tendon rupture or documented return to NBA competition before that time point. Players injured during the 2024-2025 season were excluded from RTP rate calculations because insufficient rehabilitation time had elapsed.
Season-level player statistics were obtained from Basketball Reference for the final full preinjury season and the first full postreturn season. Extracted variables included games played, games started, minutes per game, field goal percentage, 3-point percentage, 2-point percentage, free throw percentage, effective field goal percentage, offensive rebounds, defensive rebounds, total rebounds, assists, steals, blocks, turnovers, personal fouls, and points per game. To account for changes in playing time after return, selected production metrics were normalized per 48 minutes, including points, rebounds, assists, defensive rebounds, steals, and blocks.
Temporal Trend and Pace Analysis
Annual rupture incidence was calculated by counting confirmed Achilles tendon ruptures by NBA season from 2000-2001 through 2024-2025. League pace, defined as possessions per 48 minutes, was extracted from Basketball Reference for each season. The association between annual rupture frequency and league pace was assessed across the study period.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics (IBM). Continuous variables were assessed for normality using the Shapiro-Wilk test. Preinjury and postreturn performance metrics were compared using paired 2-tailed t tests. Effect sizes are reported using Cohen d, and 95% confidence intervals were calculated for paired differences. Primary performance outcomes included minutes per game, points per game, effective field goal percentage, rebounds, assists, defensive rebounds, steals, and blocks. Additional analyses evaluated per-48-minute production to account for changes in playing time after return. Statistical significance was defined as a P value <.05. All paired performance analyses were based on complete-case data, including players with both a full preinjury season and a full postreturn season. To explore the potential influence of evolving surgical techniques and rehabilitation protocols, players were stratified into early (2000-2014) and contemporary (2015-2025) eras.
Results
Incidence and RTP
Between the 2000-2001 and 2024-2025 NBA seasons, 22 NBA players sustained a confirmed Achilles tendon rupture. Injury frequency remained low across most seasons, with isolated single-player events in several years and small clusters in 2014-2015 and 2024-2025. The largest observed cluster occurred during the 2024-2025 season, when 7 confirmed ruptures were identified.
The median age at injury was 28 years. Among players with adequate follow-up for RTP rate assessment, 13 of 15 players (86.7%) returned to NBA competition, whereas 2 players (13.3%) did not appear in another NBA game after the rupture. Players injured during the 2024-2025 season were not included in the RTP rate denominator because insufficient rehabilitation time had elapsed. However, one additional player injured more recently had already returned to NBA competition and therefore had a documented time to RTP, although he did not yet have sufficient postreturn follow-up for inclusion in the paired season-level performance analysis. Accordingly, time-to-RTP analysis included 14 players with documented return, whereas paired performance analysis included 13 players with complete preinjury and postreturn seasons. Among players with documented return, the mean time to RTP was 10.8 ± 4.3 months (range, 5.5-20 months; median, 10.0 months). Individual RTP times are shown in Figure 1. Annual rupture counts and league pace are shown in Figure 2.

Individual return-to-play times after Achilles tendon rupture among National Basketball Association (NBA) players with documented return to NBA competition (n = 14). Player names were anonymized and labeled as player 1 through player 14.
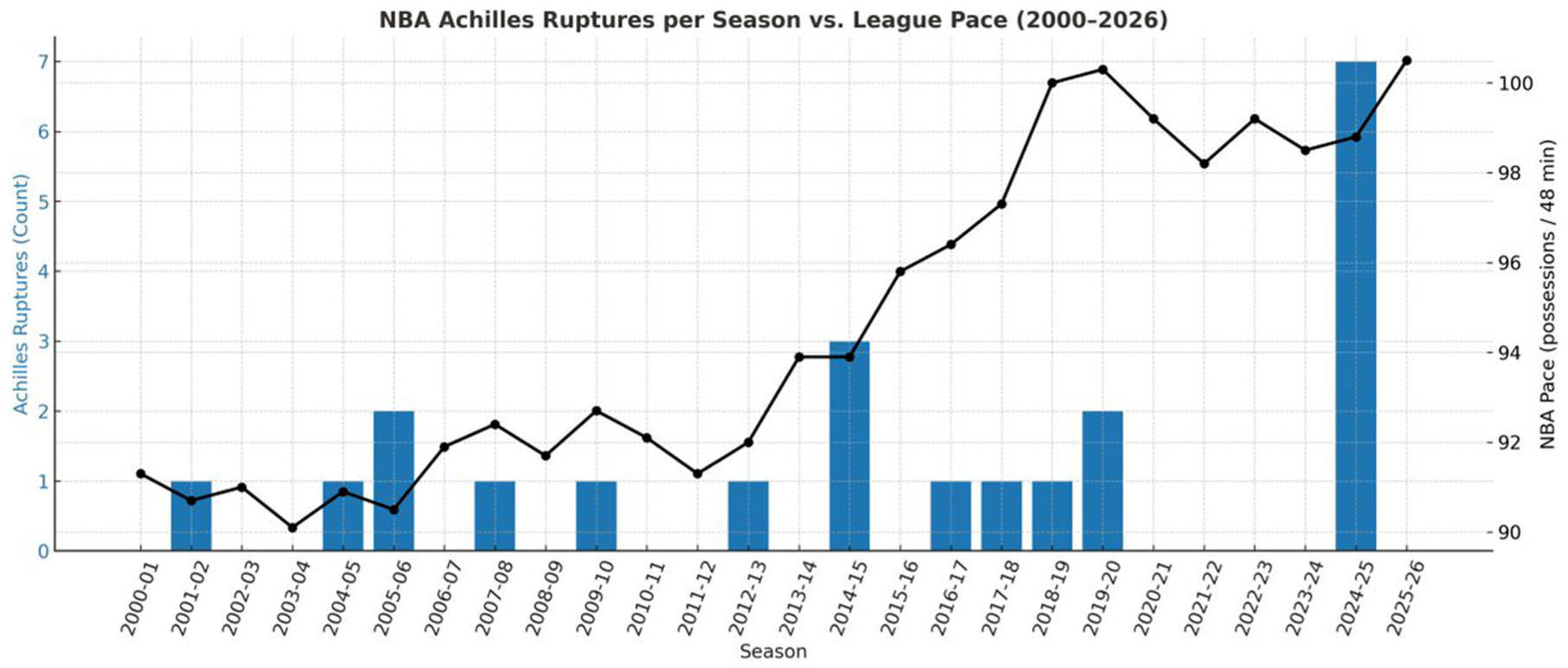
Annual National Basketball Association (NBA) Achilles tendon rupture counts plotted against league pace, defined as possessions per 48 minutes, from the 2000-2001 through 2024-2025 seasons.
Season-Level Offensive and Defensive Performance Before and After Injury
Paired comparisons were performed for the 13 players with complete preinjury and postreturn season-level performance data and demonstrated significant declines in overall workload and offensive production (Table 1). Minutes per game decreased from 32.4 ± 4.2 to 24.8 ± 8.0 (mean difference, −7.6 minutes; 95% CI, −10.7 to −4.5; P < .001; d = −1.50). Points per game declined from 17.8 ± 5.8 to 12.4 ± 7.3 (difference, −5.4 points; 95% CI, −7.2 to −3.6; P < .001; d = −1.74). Effective field goal percentage also decreased significantly from 0.525 ± 0.043 to 0.470 ± 0.055 (difference, −0.055; 95% CI, −0.093 to −0.016; P = .005; d = −0.91).
Season-Level Offensive and Defensive Performance Before and After Achilles Tendon Rupture (Paired Analysis, n = 13) a
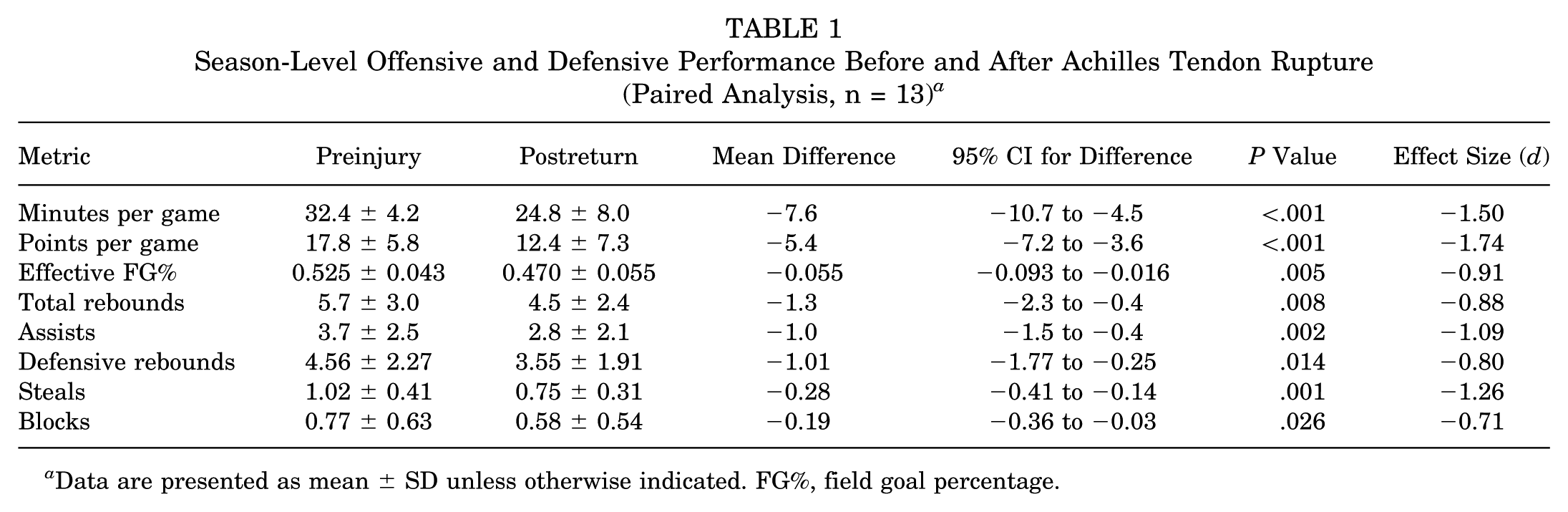
Data are presented as mean ± SD unless otherwise indicated. FG%, field goal percentage.
Additional declines were observed in playmaking and rebounding production. Total rebounds per game decreased from 5.7 ± 3.0 to 4.5 ± 2.4 (difference, −1.3; 95% CI, −2.3 to −0.4; P = .008; d = −0.88), while assists declined from 3.7 ± 2.5 to 2.8 ± 2.1 (difference, −1.0; 95% CI, −1.5 to −0.4; P = .002; d = −1.09).
Defensive box score production also decreased on a per-game basis. Defensive rebounds declined from 4.56 ± 2.27 to 3.55 ± 1.91 (difference, −1.01; 95% CI, −1.77 to −0.25; P = .014; d = −0.80). Steals decreased from 1.02 ± 0.41 to 0.75 ± 0.31 (difference, −0.28; 95% CI, −0.41 to −0.14; P = .001; d = −1.26), and blocks decreased from 0.77 ± 0.63 to 0.58 ± 0.54 (difference, −0.19; 95% CI, −0.36 to −0.03; P = .026; d = −0.71).
Role, Usage, and Per-48-Minute Production
To determine whether declines in box score production were driven primarily by reduced playing time or by intrinsic performance changes, per-48-minute metrics were analyzed (Table 2). Players demonstrated a substantial reduction in role responsibility after Achilles tendon rupture, with the percentage of games started decreasing by nearly half.
Change in Starting Role and Per-48-Minute Production After Achilles Rupture (n = 13) a
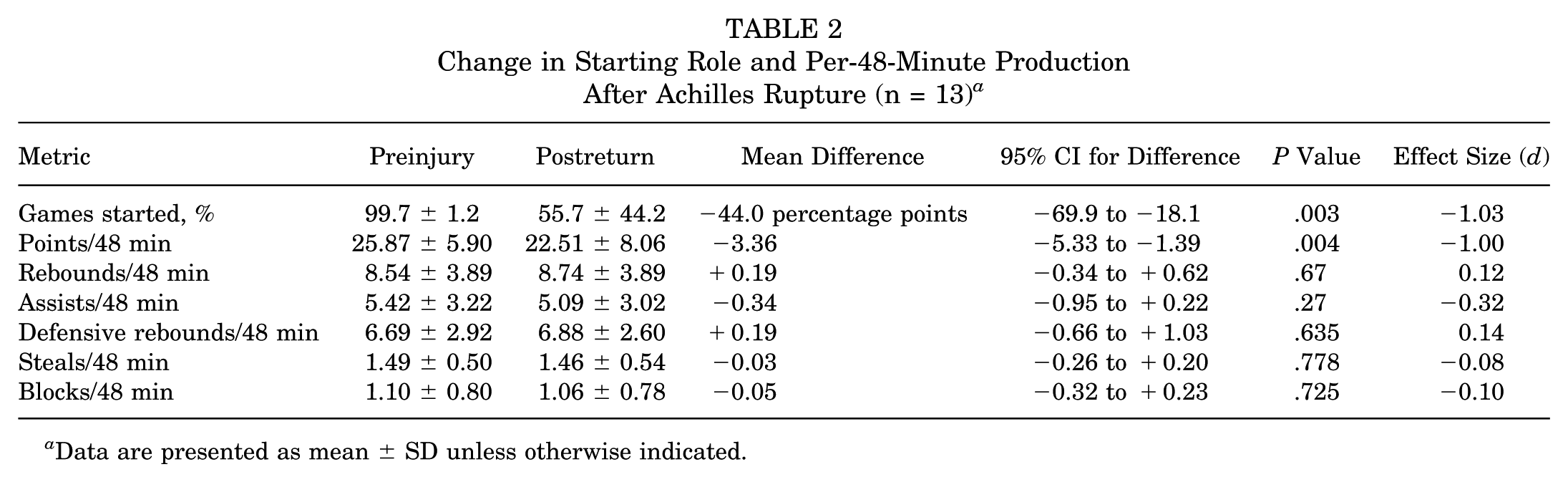
Data are presented as mean ± SD unless otherwise indicated.
When production was normalized per 48 minutes, scoring output remained significantly reduced (−3.36 points per 48 minutes; P = .004), indicating a true decline in offensive productivity beyond simple reductions in playing time. In contrast, rebounding and assist production per 48 minutes were preserved, with no statistically significant differences between preinjury and postreturn seasons.
Similarly, defensive metrics normalized per 48 minutes showed no significant differences, including defensive rebounds, steals, and blocks. These findings suggest that the observed reductions in raw defensive box score production were largely attributable to decreased playing time rather than a substantial decline in minute-for-minute defensive activity.
Era Analysis
When players were stratified into early (2000-2014) and contemporary (2015-2025) eras, no statistically significant differences were observed in RTP timing or postinjury performance metrics, although the small cohort size limited statistical power.
Temporal Pattern and League Pace
Rupture counts were superimposed on league pace (possessions per 48 minutes). Although visually the rise in ruptures after 2015 paralleled the league's historic increase in pace, formal correlation did not reach significance (Pearson r≈ 0.24; P > .10).
Discussion
This study provides a contemporary evaluation of Achilles tendon rupture in NBA players over a 25-year period. The principal findings were that (1) the majority of athletes successfully returned to NBA competition after Achilles rupture, with an RTP rate of 86.7% among players with adequate follow-up; (2) the mean time to RTP was approximately 11 months; (3) players demonstrated significant reductions in playing time, scoring production, and offensive efficiency after RTP; and (4) defensive activity normalized per playing time remained largely preserved. Additionally, although the overall incidence of rupture remained low across the study period, a noticeable cluster of injuries occurred during the 2024-2025 season. These findings provide updated sport-specific insight into functional recovery expectations after Achilles rupture in modern professional basketball.
The RTP rate observed in this study compares favorably to historical concerns that Achilles rupture is often career-ending for elite basketball players.1,2,6,8,10,13 Earlier reports from the mid-2000s suggested high rates of incomplete recovery and shortened career trajectories.8,11 Contemporary series, however, including analyses from other professional leagues, have demonstrated gradual improvement in surgical repair techniques, rehabilitation strategies, and return-to-sport protocols. Our findings are consistent with this evolution: although a minority of players did not return, most athletes were able to resume NBA play within the typical 9- to 12-month rehabilitation window.4,9
Despite high RTP rates, players experienced substantial decreases in workload and performance. Minutes per game decreased by >7 minutes, and points per game declined by >5 points. Importantly, these reductions were not solely attributable to reduced playing time. Even when normalized per 48 minutes, scoring output decreased significantly, while rebounding per 48 minutes remained stable and assists showed a nonsignificant decline. These findings may reflect the greater dependence of scoring efficiency on high-intensity explosive actions, such as first-step acceleration, vertical elevation, and rapid directional change, although the present study was not designed to directly measure these biomechanical mechanisms. This interpretation is consistent with biomechanical studies demonstrating persistent deficits in plantarflexion strength and push-off mechanics after tendon repair.4,11
Role allocation also changed meaningfully after injury. The proportion of games started dropped by nearly half, indicating that players often return in reduced or modified roles, potentially reflecting both physical limitations and load management decisions by teams. This finding has important implications for expectation counseling, contract valuation, and performance forecasting, and may help explain the perception among fans and analysts that players “return but are not the same.” 3
The temporal analysis revealed no statistically significant correlation between league pace and rupture frequency, although the descriptive pattern showed an increase in ruptures during the league's pace acceleration era after 2015. This could reflect increased cumulative load, greater game intensity, or simply random variation given the small annual numbers. 12 The spike in 2024-2025 stands out but requires caution in interpretation; short-term clusters may emerge due to chance, media visibility, or reporting patterns. Larger multileague data may clarify whether changing style of play contributes meaningfully to Achilles injury risk.
This study has several strengths, including strict confirmation of injury type, comprehensive cross-platform verification, standardized pre- versus postinjury performance comparisons, and use of per-48-minute metrics to isolate underlying efficiency changes. The 25-year scope and focus on a single elite league provide a detailed view of outcomes specific to NBA athletes.
Several limitations should be acknowledged. First, the cohort size was relatively small, with only 22 confirmed ruptures and 13 players available for complete paired performance analysis. Although this reflects the rarity of Achilles tendon rupture among NBA athletes, the limited sample size reduces statistical power and requires cautious interpretation of statistical comparisons, particularly subgroup and era-based analyses. Second, the study relied on publicly available data sources, which may be affected by reporting variability and did not allow access to detailed clinical variables such as rupture location, surgical technique, biological augmentation, postoperative complications, rehabilitation protocols, or objective strength and functional testing. Third, RTP was defined as participation in at least one NBA game after rupture. Although this definition captures return to league participation, it may not fully reflect a meaningful competitive return or restoration of preinjury role. Fourth, long-term career outcomes beyond the first postreturn season were not formally analyzed because subsequent performance may be influenced by aging, roster changes, contract status, coaching decisions, additional injuries, or retirement. Finally, the temporal analysis was descriptive and limited by the small number of annual rupture events; therefore, the observed 2024-2025 cluster should be interpreted cautiously and should not be considered evidence of a causal relationship with league pace.
Conclusion
Our study showed that most NBA players with adequate follow-up returned to professional play after Achilles tendon rupture, typically within approximately 11 months. However, reductions in playing time, scoring output, offensive efficiency, and starting role prevalence were common after return. Per-48-minute analyses suggested that scoring decline persisted even after accounting for reduced playing time, whereas several defensive and rebounding metrics were relatively preserved. Annual rupture incidence remained low overall, although a notable cluster was observed during the 2024-2025 season. These data may be helpful for counseling players regarding performance expectations and decision-making after Achilles tendon rupture in elite basketball players.
Footnotes
Final revision submitted April 29, 2026; accepted May 16, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was not sought for the present study, as all data were derived from publicly available, nonidentifiable historical records of professional athletes.