
Abstract
Public health leadership requires a complex set of skills encompassing critical thinking, evaluation, planning, collaboration, and negotiation. Effective leaders mobilize stakeholders for change, facilitate decisions during crises, and anticipate unintended consequences. These skills are not easily attained through traditional classroom instruction, however, can be effectively taught through experiential learning. Since 2016, the University at Buffalo has taught Master of Public Health (MPH) students leadership skills through hands-on, practice-based immersion activities using innovative experiential learning methods in a foundational two-credit competency-based course titled Public Health Leadership, Collaboration and Negotiation. Using a scaffolded approach in the course, learners are introduced to leadership skills through in-class workshops. They then apply tools such as Memorandums of Understanding, gap analyses, stock and flow maps, and work plans to address public health issues. Throughout the course learners emulate roles within real organizations, role play navigating challenging topics, and create work deliverables that foster collaboration and community engagement, and facilitate decision-making for course assignments. This paper presents results from a study examining effectiveness of a course designed using experiential learning theory to build these skills in MPH students. Data from students, employers, and alumni, as well as course outcomes and post-degree jobs were analyzed. Results suggest that the pedagogical approach utilized in the course to strengthen leadership, collaboration, and negotiation skills through hands-on, immersive activities helps prepare students to be effective public health leaders and program managers.
Keywords
Introduction
The call to prepare public health leaders and program managers for practice is not new. The 1988 report on The Future of Public Health (Institute of Medicine, 1988) identified the need for leaders to reshape public health services nationwide. Since then, persistent calls have been made for training public health leaders who are skilled in addressing society’s evolving population health needs (Fraser, 2024; Koh, 2009; Rowitz, 2009). Public health leadership requires a complex set of skills such as critical thinking, evaluation, planning and management, collaboration, negotiation, and consensus-building. Effective leaders inspire and mobilize stakeholders and communities to affect change. They facilitate decisions amid emerging challenges or crises, often with few resources. They innovate and build consensus for implementation, applying systems thinking and systems science to problems to address root causes and cultivate sustainable solutions (Fraser, 2024; Koh, 2015; Rowitz, 2009). Public health leaders adapt and apply transformational approaches to drive change and reconcile opposing perspectives for action. They catalyze collective voices to advocate for policies and resources, communicate conflicting and complex information, and lead with communities to build trust and ensure ethical and equitable practice (Fraser, 2024; Holden et al., 2016; Koh, 2009; Rowitz, 2009; Saleh et al., 2004). These less concrete concepts where multiple approaches may be effective can be challenging skills for learners to build in a classroom setting.
Experiential learning theory posits that students can learn to apply skills in spaces where they can do, or practice, those skills (Kolb & Kolb, 2005), representing a more active learning environment compared with traditional classroom instruction which centers on lecturing and knowledge acquisition (Czabanowska et al., 2013; Freeman et al., 2014). When training future leaders to meet population-level health needs, students can effectively learn to apply skills in leadership, collaboration, negotiation, and systems thinking through less passive, more immersive practice-based classroom activities (Czabanowska et al., 2013; Lachance & Oxendine, 2015). Since 2016, the University at Buffalo has taught Master of Public Health (MPH) students the skills of leadership, collaboration, negotiation, and systems thinking, as well as strategies to engage communities and build consensus, through hands-on activities in foundational MPH coursework completed prior to a student’s applied practice experience (APE). The APE is an MPH requirement for degrees accredited by the Council on Education for Public Health (CEPH, 2016, 2024). Learners are introduced to public health leadership in the classroom through innovative experiential learning methods. This paper describes effective ways to build critical leadership skills recognized by CEPH as standards of public health practice for MPH students through practice-based, immersive activities in an academic setting.
Materials and Methods
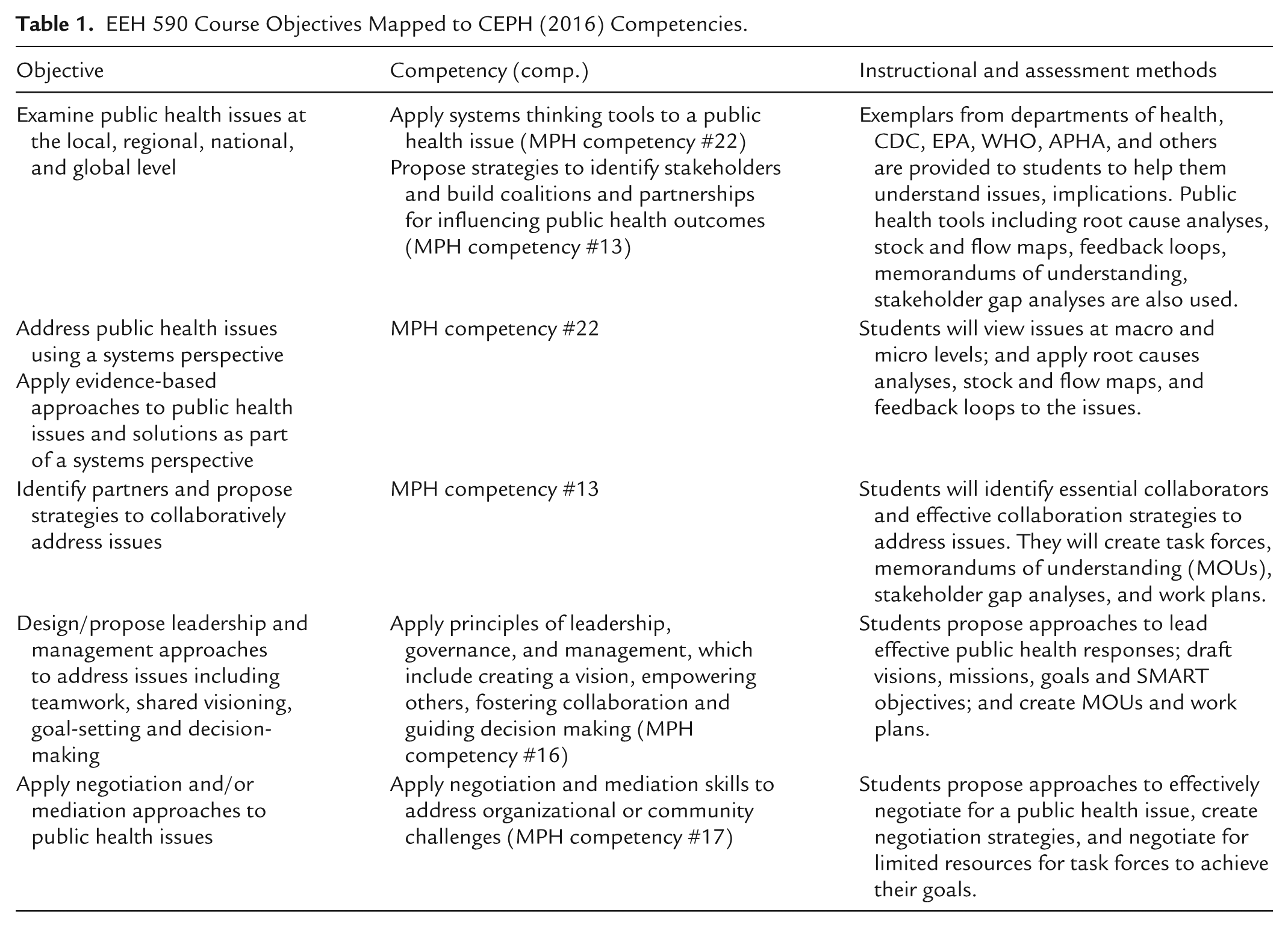
The University at Buffalo introduces MPH students to public health leadership through a required two-credit competency-based course: “EEH 590 Leadership, Collaboration and Negotiation.” This course covers and assesses students on CEPH MPH competencies of leadership, collaboration, and negotiation (CEPH, 2016). Skills introduced in the course are reinforced in other foundational MPH coursework; students then apply them in an authentic setting during their MPH APE or practice experience. The leadership course has been taught every Fall semester in a seated section, and since 2020 additionally in an online section. On average, 100 students complete the course each year, with all sections using the same materials, class activities, and learner assessments to demonstrate skills. The course was designed and is taught by public health leaders, including health directors, ensuring alignment of concepts and activities with current practice. Content, activities, and student assessments map directly to CEPH (2024) competencies 13 (collaboration), 16 (leadership), 17 (negotiation), 21 (interprofessional teamwork), and 22 (systems thinking) shown in Table 1. The course has primary responsibility for addressing and assessing competencies 13, 16, 17, and 21. However, competency 22 is covered and assessed in another foundational course. EEH 590 reinforces systems thinking content, considering it as an essential leadership skill for decision-making.
EEH 590 Course Objectives Mapped to CEPH (2016) Competencies.
Learners begin the course by establishing ground rules for collaborative work, which introduces them to teamwork and consensus-building approaches and gives them hands-on opportunities to practice these skills. Each learner then chooses a public health or health-related organization they wish to work for and a position or role within it that they wish to represent. For example, one learner may choose to be a behavioral health coordinator at an addiction prevention and treatment center while another may wish to represent a local health department educator. By selecting a real organization and role, learners become representatives of their organization and emulate the role for the duration of the semester, with the course instructor serving as a consultant guiding them to develop community-based task forces. Representatives (students) collectively brainstorm critical health issues, building consensus for priority issues for which they then form task forces.
Each task force works together to revise the ground rules originally established by all learners in the class, to meet their specific task force needs. They then gain agreement for the collaboration style, meeting plan, and decision-making approach each task force will use to function. Examples of health issues learners have prioritized in task forces include housing insecurity, opioid prevention, and reproductive health care access. Effective approaches to collaboration, establishing meeting plans, and making task force decisions are introduced to learners through didactic course content, providing a basis for their understanding of the concepts and giving them tools to weigh their options before determining their operational processes. For example, one task force may choose to make decisions by majority vote, while another may opt to delegate decision-making to specific team members based on their unique skill areas and expertise.
To ensure each learner can function effectively as a task force member addressing a priority health issue, foundational course content is delivered through a series of “workshops” facilitated by real-world leaders with relevant practice expertise. Workshops are held during class time on Visions and Mission Statements, Creating SMART Goals and Objectives, Using Tools for Systems Thinking, Engaging Communities for Strategic Planning, Negotiation Tactics and Approaches, and Evaluating Processes and Outcomes. During the workshops, representatives (students) individually practice creating a vision, mission, goals, and SMART objectives for their chosen organization’s programming, and then revise their purpose statements based on peer and consultant (instructor) feedback. They also practice creating a root cause analysis and stock and flow map for an issue their selected organization addresses, gaining hands-on experience with essential systems thinking tools commonly used by public health leaders.
After foundational leadership concepts are introduced, task forces work together to develop three sets of deliverables: (1) a Memorandum of Understanding (MOU) with a work plan to address their priority health issue, (2) a negotiation for resources supporting activities included in their work plan, and (3) leadership assessments. These deliverables were selected based on feedback from public health leaders who identified tools and practices they regularly use (University at Buffalo, 2023) and align directly with CEPH competencies. While the MOU, work plan, and negotiation are completed in task forces (groupwork), deliverables require individual strategizing by each representative (student) for the unique contributions they can make to task force deliverables based on their chosen organization and role. This instructional approach allows for hands-on learner experiences through immersion and collective deliverables, while maintaining individual learner competency assessment. After each task force member presents their proposed strategy or approach for creating each deliverable, the task force works together to finalize a collaborative version, as they would in a practice setting.
MOU and Work Plan Collaboration
In task forces, each representative shares their unique organization’s vision, mission, and goals, and a summary of their chosen role and responsibilities. To better understand what they can individually contribute to their task force, each representative (student) strengthens their own knowledge of their chosen role by consulting similar organizations, job postings related to their role, and technical information about their priority health issue. For example, a learner who chose to represent an educator for a community health center and is part of an opioid prevention task force would seek out information on evidence-based opioid prevention strategies and opioid-related education programs to continually strengthen their related knowledge and skills. This begins to position each representative as a unique leader on their task force, better prepared to make specific contributions to the team’s work. Representatives then collaborate to create a collective task force vision, mission, goals, and SMART objectives which generate the “Purpose” section of their MOU. To help inform development of task force goals and objectives, each team member completes an individual root cause analysis (RCA) and stock and flow map for the priority health issue the task force is addressing, based on what they learned in the systems thinking workshop. They then work together to generate a consolidated RCA and stock and flow map to guide their team goals and objectives. Task forces also create a roster of the organizations, roles, and responsibilities contributing to their MOU (their chosen organization, role), identifying unique knowledge and skills they will each individually bring to work of the task force. They then conduct a stakeholder gap analysis, identifying organizations, functions, or expertise needed to meet their goals and objectives, but missing from their team. This helps them understand the importance of collaboration across a range of stakeholders, including the community most impacted by the health issue. Task forces propose a plan to collaborate with other stakeholders, filling their team’s knowledge and skill gaps. After each representative individually creates a stakeholder gap analysis, the team collaborates to finalize set of partners they will invite to join, adding all partners in their MOU’s “Parties and Responsibilities” section, along with individual contributions of each. Deliverables are collaboratively created in shared documents so the instructor can see each student’s unique contribution, and each student signs the final MOU as a representative of their chosen organization, as they would in practice. Each task force then generates a related work plan operationalizing work needed to achieve their goals and objectives. MOU and work plan documents are iterative with both peer (other students) and consultant (instructor) feedback until deliverables demonstrate practice expectations.
Negotiating for Resources
After finalizing the MOU and work plan, task forces negotiate with each other for resources to implement their plan. Resources for which they negotiate are limited, replicating situations often experienced in practice. Prior to negotiating, each task force collaboratively prepares an opening position for necessary resources to achieve their MOU goals, as well as alternative positions for compromising if needed. Following a workshop on negotiation strategies and tactics in public health, each representative individually prepares a negotiation strategy with tactics they feel confident they can implement, such as providing data, evidence, or facts to support their team’s position; making emotional appeals to obtain resources; or describing likely impacts if resources are not obtained. After each representative prepares their personal negotiating plan, the task force works together to incorporate individual strategies into a team approach. As part of a simulated class activity, task forces then negotiate with each other, implementing their integrated strategy. After the negotiation, each representative reflects on specific tactics they employed and the degree to which their tactics contributed to the result. Each representative also summarizes their perspective of the outcome, identifying what they believe worked to achieve task force needs, how effective each task force was in meeting priorities, and how compromising impacted the results. Students in seated sections conduct their negotiation during class time and students in online sections conduct their negotiation using a virtual meeting platform.
Evaluating Public Health Leadership
At the end of the semester, students complete two evaluations. First, each task force collaboratively conducts a performance assessment examining team processes such as methods for goal-setting, decision-making, and developing deliverables. Each learner also prepares an individual leadership assessment integrating select 360-degree assessment processes such as peer feedback from other task force members (students) and the consultant (instructor), as well as self-reflection to identify their public health leadership skill gaps.
Pedagogical Approach to Leadership Training
To be most effective, teaching leadership should go beyond traditional or rote learning techniques, leveraging innovative pedagogical strategies (Koh, 2015). Employing applied, hands-on immersive strategies such as simulation are key to building these skills. Reflection, group work, and collaborative learning also help strengthen leadership skills (McCunney et al., 2019; Moodie, 2016) and are important activities for learning.
This course takes a scaffolded approach to all activities. Learners are introduced to a public health skill, such as applying systems thinking to an issue. They then apply related tools, such as stock and flow maps, to the issue to practice applying tools that facilitate decision-making. In most cases, learners indicate that this course provides their first exposure to essential public health tools such as SMART goals, gap analyses, RCAs, stock and flow maps, MOUs, and work plans. Early hands-on practice activities that this course offers are critical for building leadership skills. Examples of authentic materials used during the course, such as CDC MOUs or health department work plans are first introduced to learners during didactic course content and classroom workshops, and serve as models for task forces to design their own materials. Introducing leadership tools and concepts through didactic course content in the form of practice-based workshops, applying tools to real situations, and sharing iterative peer (other “representatives” or students) and expert (“consultant” or instructor) feedback strengthens leadership concepts and enhances final deliverables that learners create. Through these activities, learners become more skilled in applying critical thinking, planning and evaluation, collaboration and consensus-building, negotiation, decision-making, and systems thinking to lead public health initiatives, and team performance and individual leadership assessments provide students with opportunities for reflection and personal growth.
Role Playing
Simulation is an effective way to train students on leadership skills (McCunney et al., 2019), and role-playing is a type of simulation to help students learn. Role-playing is an effective way to achieve a range of learning outcomes beyond cognitive processes (knowledge acquisition), integrating affective and psychomotor domains (practicing responses and actions) described in Bloom’s taxonomy (Anderson & Krathwohl, 2001). In this course, role-playing aims to strengthen leadership skills as each student leads efforts on their task force that align with their unique organization and role. This type of role-playing challenges learners to be the most knowledgeable they can be in their chosen professional area, seeking out resources to best represent their organization and role as would be expected in practice. Learners are immersed in simulated practice by representing a real organization and role and determining how to apply their unique knowledge and skills within a team context. They apply these individual skills to collaborate and create task forces, MOUs, and work plans through consensus-building and agreement, and engage in a live negotiation, considering impacts of gained and lost resources.
Skill-Based Grading
All learner assessments in this course are work deliverables, such as the MOU, stakeholder gap analysis, negotiation activity, and leadership assessments. All assessments are graded satisfactory (effective demonstration of the skill through the deliverable) or unsatisfactory (lack of demonstration). By using skill demonstration as the metric for success rather than points or grades earned, learners spend less time worrying about grades and more time practicing their skills to ensure they can apply them effectively. Feedback is continually provided to each representative (student), and the consultant (instructor) provides ongoing feedback as task forces complete their work, guiding learners to improve deliverables. Students who initially struggle to demonstrate a foundational skill continue to integrate feedback and practice it throughout the semester until they can effectively demonstrate it.
Data Collection
To evaluate course effectiveness, student, course, employer, and alumni data were analyzed. At the University at Buffalo, courses are typically evaluated using student feedback from course evaluations, as well as student performance on course assessments. Given that this course was specifically designed to meet critical workforce needs, employer and alumni data on leadership, collaboration, and negotiation skills of graduates were also analyzed. Job outcomes and alumni feedback on post-degree skill needs and jobs obtained were further considered in determining course effectiveness.
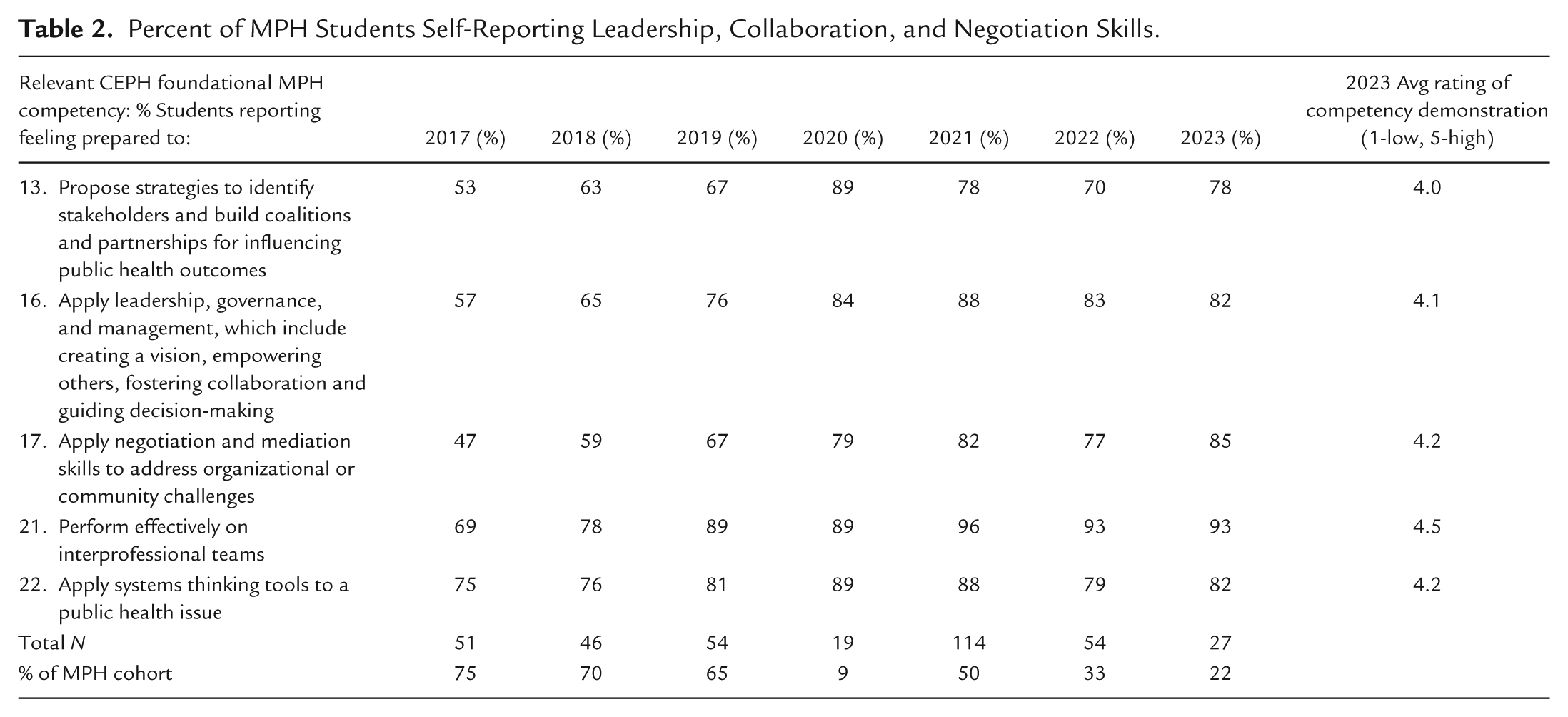
Students self-report their ability to demonstrate MPH competencies through a survey emailed to them annually. Between 19 and 114 students completed the survey each year (presented in Table 2), representing a wide variation in student response rates. Prior to 2020, response rates were 65% or higher. However, in 2020, participation dropped to 9%, likely due to the COVID-19 pandemic. In subsequent years, response rates improved (22%–33%) but did not return to prior levels, possibly reflecting a shift away from email and toward mobile-based communications. Data from all student respondents between 2017 and 2023 were analyzed.
Percent of MPH Students Self-Reporting Leadership, Collaboration, and Negotiation Skills.
Data was also collected from 2018 to 2023 through employer surveys (n = 22), in-depth interviews (n = 25), and qualitative feedback through the school’s community Advisory Council consisting of employers and alumni, and a Regional Alliance of health directors representing 11 of the most frequent employers of the MPH program’s graduates. Through surveys and in-depth interviews, employers provided feedback public health skill needs and gaps among MPH graduates and thematic analysis was used to identify themes in leadership, collaboration/teamwork, interprofessional/interdisciplinary practice, and negotiation. Qualitative feedback from Advisory Council and Regional Alliance members was drawn from semi-annual meeting discussion prompts and ongoing informal feedback to MPH leadership through routine engagement. Alumni data was drawn from qualitative feedback on annual alumni surveys (n = 157), also using thematic analysis to identify skill strengths and gaps of their MPH training.
Results
Student Feedback
Since implementing the leadership course, students report feeling better prepared in leadership, collaboration, and negotiation skills. Results of the survey (Table 2) show a higher percent of students reporting an ability to demonstrate leadership, collaboration, negotiation, and systems thinking competencies prescribed by CEPH after the leadership course was first delivered in 2016. While fewer learners report leadership skill demonstration in 2017, this MPH cohort had a mix of learners – those who completed the revised competency-based leadership course, and those who took the course prior to introduction of 2016 CEPH competencies shown in Table 1. However, in more recent years all MPH students (2019–2023) took the revised course as part of their curriculum. This likely led to consistent increases in students reporting an ability to demonstrate leadership competencies found.
Students providing comments in their course evaluations also reported benefits of immersive, practice-based learning for skill-building. Among students providing comments on course evaluations (n = 22), teamwork/collaboration activities and real-world practice-based assignments were reported as most useful for skill acquisition (n = 11). Two students reported struggling with collaboration course components and an additional two students reported difficulty adjusting to the immersive, practice-based course format. All but one student enrolled in the course passed it (graded Pass/Fail), effectively demonstrating leadership, collaboration, and negotiation skills through course activities and deliverables.
Employer and Alumni Feedback
Employer and alumni data consistently show that practice partners prioritize leadership and collaboration skills in MPH graduates, and that University at Buffalo MPH graduates are sought out for these skills. Leadership, management, and collaboration were ranked as priority skills by employers surveyed, with ratings averaging 3.1 (2018–2019), 3.8 (2022–2023), and 4.8 (2025) on a scale of 1 (least sought) to 5 (most sought). Interview respondents further highlighted the need for these skills, which were sought by nearly all employers when they hired (n = 22, 88%).
The University’s MPH job placement rate, represented by the percent of graduates seeking employment who report obtaining a job within 1 year of degree completion, is also high, further indicating that skills graduates bring to their employers are valuable. Between 2016 and 2024, the University collected job outcomes on 75% to 80% of each graduating cohort, reporting a 100% job placement rate in 7 of 9 years and a 99% job placement rate in the remaining 2 years. Qualitative data collected from employers and alumni also suggest that as many as 50% of MPH graduates are promoted or placed into managerial or leadership roles within 1 year of entering the public health workforce, with employers stating that MPH graduates need to be job-ready on “day-one” as they are often the only public health-trained person on their staff (University at Buffalo, 2023). Positions obtained by graduates with titles including “manager,” “director,” or “lead” ranked third among most common post-degree job placements. Further, between 2021 and 2023, half of MPH alumni who provided qualitative comments in their alumni survey identified collaboration or leadership (12 of 24) as most valuable skills gained from their MPH. The remaining 12 comments emphasized technical skills such as statistical analysis or epidemiology. Two alumni reported skill gaps in related areas: one in project management skills (leadership domain), and one in conflict resolution skills (collaboration/negotiation domains).
Discussion
The EEH 590 leadership course is one component of a broader MPH curriculum, yet is essential to address foundational competencies that are less concrete when compared to technical skills such as applying epidemiologic methods. Public health tools and concepts introduced in the course are reinforced through other foundational courses, and through each student’s practice experience where they can apply knowledge and skills in an authentic setting. Immersive and experiential pedagogical approaches employed in this course to teach leadership, collaboration, negotiation, and systems thinking, skills that are often challenging to teach in a traditional classroom format, have been practical and effective for increasing student skill demonstration. Specifically, simulation, groupwork, scaffolding, real-world experiences, reflection, immersion, and assessment through skill demonstration are used in this course to prepare future public health leaders with skills employers need. Importantly, course design and delivery by experienced public health leaders ensures that content is presented in the context of practice, further facilitating a more immersive and applied learning experience.
Challenges in Implementing Experiential Learning
Public health leaders served as course instructors and recruiting them as adjunct faculty was not a barrier. Practitioners were willing and enthusiastic about teaching the course. However, challenges emerged for students, some of whom expressed discomfort with non-traditional pedagogical approaches, particularly immersive activities and practice-based assessments graded on skill demonstration. Following initial course orientations to the experiential learning model employed in EEH 590, most students adapted well. However, two reported feeling “lost,” citing uncertainty with grading based on skill demonstration rather than knowledge gained from lectures or readings, as well as expectations for individual contributions to task force deliverables stemming from each learner’s unique organization and role. Ongoing coaching and hands-on guidance from the instructor, along with concrete examples of real-world deliverables, helped alleviate many concerns and supported student adjustment to the course format.
Given the MPH program’s high job placement and promotion rates, it is essential that students have opportunities to learn and practice applying these skills throughout their training to best meet workforce needs. The goal of this course was to replicate a practice environment using authentic hands-on activities, tools, and resources in the classroom to strengthen MPH students’ less technical or concrete skills. This required transforming the learning environment from a traditional to an immersive, experiential setting. Students who received applied, practice-based, and immersive instruction in EEH 590 reported the ability to demonstrate leadership, collaboration, negotiation, and systems thinking, and employers recognize these skills as necessary and valuable to their organizations. Leadership skills gained or strengthened through this course may also contribute to more graduates obtaining jobs after degree completion by preparing them to better meet employer skill needs, and may lead to greater opportunities for promotion into leadership roles.
Limitations of This Study
Leadership, collaboration, negotiation, and systems thinking became required MPH competencies in 2016 (CEPH, 2016). In response, the University at Buffalo newly established EEH 590 in that year to cover these competency gaps in its MPH curriculum. Consequently, no baseline data exist on how these skills were taught or how effectively students perceived they could apply them. Similarly, this study does not permit comparison between traditional and experiential instructional approaches; it is possible that non-experiential teaching methods could also foster acquisition of these skills. However, the experiential learning design more closely aligns with recommendations for preparing the future public health workforce, which emphasize experiential learning and authentic assessment (Association of Schools and Programs of Public Health [ASPPH], 2024) over traditional lecture-based approaches. Further, although the EEH 590 experiential learning approach differed from the more traditional structure of other MPH foundational courses, most MPH students adapted well and reported meaningful gains from the instructional methods used.
A key limitation of this analysis is the primarily qualitative nature of employer and alumni data through open-ended survey and interview comments, making it difficult to systematically assess needs and gaps of skill areas discussed in this study. Without standardized measures, findings may be subject to variability in interpretation and potential response bias among those who chose to participate. While employer and alumni data were limited, triangulating these data with student self-assessment of skill attainment, course outcomes, and job placement and promotion data, provides a clearer picture of the strength of leadership skill development through an experiential learning framework.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.