
Abstract
Background
Patient- and public-led research signals more than a redistribution of decision-making authority, positioning patients and public as key contributors of scholarly inquiry throughout the research process. Despite the growing awareness of patient- and public-led research endeavors, it is unclear how they are conducted. This scoping review aimed to synthesize how patient- and public-led research is defined and practiced in health research.
Methods
Our scoping review was guided by the Arksey and O’Malley’s framework (2005) and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). A comprehensive search of health research databases and grey literature sources was conducted. Included studies were published in English and described how patients and public held final decision-making authority (Empower on the International Association for Public Participation, IAP2 continuum) across various research roles and tasks. These standardized roles and tasks were described using the Contributor Role Taxonomy (CRediT). Through iterative discussions and abductive analyses, groupings of studies that shared similar contexts and extended beyond standardized roles and tasks were identified.
Results
Our search identified 4,723 records, of which 68 articles describing 62 studies met the inclusion criteria. Patient- and public-led research was described using terms including consumer-led, user-led, Indigenous-led; with only 14 (23%) studies offering an explicit definition. Our review identified three contexts in which patient- and public-led research occurred including: how research was carried out (operations), how decisions were made (governance), and how intellectual/experiential contributions from patients and public shaped research trajectories (accountability).
Conclusion
By shifting the focus from involvement to leadership, our findings provide a foundation for more intentional design, meaningful support, and robust evaluation of patient- and public-led health research.
Keywords
Introduction
There has been an increased recognition of the transformative role that patients and public play in the process of health research.1-4 The concept of ‘patient and public involvement’ (PPI) is thought to have originated in the United Kingdom, where in 1996 the National Health Service formally launched the patient advisory body INVOLVE. 5 Long before PPI became formally embedded within research practice, people with lived experience challenged the authorities of health research. 6 In the 1960s and 1970s, disability rights activists, HIV/AIDS advocates, feminist health movements openly contested the exclusion of experiential knowledge from research decision-making, arguing that those most affected by health research should have a meaningful say in how it is conceived and conducted.7,8 Over the years, this movement came to be known as the “nothing about us, without us” movement which has contributed to advancing research conducted with or by patients and public, rather than merely for or about them. 9
Prior to this, patients and public were often relegated to the role of passive subjects or knowledge users, limiting their influence on research priorities.2,10,11 As a result, studies may have overlooked outcomes that matter most to patients and public, thus reducing relevance, and potential impact on health outcomes.12,13 Patients and public were deemed to be too close to the issue and too biased to be a part of the rigors of knowledge production.2,10 A lack of formal research training and academic credentials are well documented barriers to involvement; while hierarchies of knowledge continue to privilege academic and clinical expertise over experiential knowledge.2,10 Since the establishment of INVOLVE, patients and public have increasingly challenged the status quo, asserting the value of their expertise 14 and advancing models of meaningful partnership. 15 Increasingly we see patients and public gaining greater decision-making authority and assuming roles and tasks that were once reserved for researchers. 16 However, many challenges remain in addressing power imbalances on research teams, where patient and public occupy positions that are shaped by structural factors including limited access to resources and institutional hierarchies, which can manifest as tokenistic involvement, limiting their contributions to research. 17 Early evidence suggests that patient and public involvement can improve relevance, quality, and transparency of health research.13,18,19 Yet, despite this momentum, it remains unclear what it means when patients and public assume leadership in health research 20 – how it is defined and how it is practiced. Evidence remains scattered across disciplines, highlighting the need for a literature review to clarify how patient- and public-led health research can be actualized and sustained.
Developed by the International Association for Public Participation, the IAP2 continuum delineates five progressive levels of patient and public involvement, namely Inform, Consult, Involve, Collaborate, and Empower. 21 The latter represents the highest level of involvement, whereby patients and the public lead the research process with or without academic researchers serving as collaborators or allies.22,23 This level of involvement positions patients and public at the forefront of decision-making, leveraging their experiential knowledge to steer research priorities, design, conduct, and outcome evaluation.2,24 Although numerous studies have made calls to action for patient- and public-led efforts,24-26 few have clearly defined what constitutes patient- and public-led health research. 20 For instance, a scoping review by Reinius and colleagues defined patient-led innovations as those initiated and driven by patients. 25 In contrast, funding initiatives such as the Patient-Led Research Hub at the University of Cambridge place particular emphasis on patients not only taking ownership of research projects but also playing an active role in management. 26 Without a clear understanding of patient- and public-led research, and how it is operationalized in different contexts, well-intended efforts risk excluding work that falls outside the dominant research paradigm; worse yet, it may undermine the quality of public scholarship by reducing it to a rebranding of patient and public involvement. 27
This scoping review seeks to address the following research question: “How is patient- and public-led health research defined and practiced in the literature?”
We synthesized examples of patient- and public-led health research and applied the IAP2 continuum to reflect levels of involvement, focusing on Empower, where final decision-making authority rests with patients and public.21,23 To capture the range of contributions in patient- and public-led research, we mapped roles and tasks using the Contributor Role Taxonomy (CRediT). 28
Positionality Statement & Epistemological Foundation
This manuscript reflects the collaborative efforts of patients, researchers, trainees and clinicians (including a physician, nurses, physiotherapists, an occupational therapist, and a dietitian). More specifically, two team members are active patient partners in Canada (TL and KM), several live with rare chronic conditions, while six have experience with patient- and public-led research. All members have formal research training in the form of advanced or professional degrees. Our collective experiences span various research fields and disciplines from pediatric to adult care, from acute injury to chronic disease, from physical health to mental health. Many of us have had varying experiences in co-leading research projects with patients and researchers alike. Our diverse perspectives allow us to approach the review process with a multifaceted understanding of both the science and practical aspects of patient and public involvement in research.
This scoping review is informed by a pragmatic paradigm, which views knowledge as co-constructed and its value derived from addressing real-world problems. 29 In patient- and public-led research, this means recognising that knowledge can arise from different sources and shaped by collective actions of patients and public alongside researchers. 30 The use of a scoping review to map existing evidence and to capture multiple ways of knowing is in line with a pragmatic lens. Further, our choice of conceptual frameworks: the IAP2 continuum, which models the continuum of patient and public involvement in research and the CRediT contributions, which recognises diverse roles and tasks from all co-authors, are coherent with a pragmatist paradigm.
Methods
This scoping review followed the five stages outlined by Arksey and O’Malley (2005): identifying the research question, identifying relevant studies, selecting studies, charting the data, collating, summarising, and reporting the results. 31 An additional sixth stage, partner feedback or consultation, involving patients and public to enhance the relevance and applicability of the findings is recommended32,33 and will be reported separately. This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) guidelines to ensure transparency and completeness in reporting. 34 The scoping review protocol was registered a priori with the Open Science Framework (https://doi.org/10.17605/OSF.IO/SDZEX).
Stage 1: Identify the Research Question
We used PCC (Population or participants/Concept/Context) to identify the main concepts in the review and inform the search strategy. 35 Our population of interest were individuals with lived/living experience, including patients, caregivers, family members, and community members, who led one or multiple roles or tasks throughout the research study. Our concept of “Patient- and public-led research” was defined at the level of Empower on the IAP2 continuum. 21 Empower describes instances where final decision-making authority rests with patients and the public, and researchers provide advice and assistance in line with patient and public decisions for designing and conducting their research.21,23 We also searched for documents that described patient and public led initiation of a study, data collection, as well as governance and/or ownership of the research process and/or products. We defined the context of health research according to the Canadian Institute for Health Research (CIHR) definition, which encompasses four pillars (Biomedical research; Clinical research; Health services research; Social, cultural, environmental and population health research). 36
Stage 2: Identify Relevant Studies
With the support of a medical librarian, systematic searches were conducted across a range of (1) health science databases (MEDLINE, CINHAL, EMBASE, PsychINFO) and (2) grey literature databases (ProQuest Dissertations & Theses Global, Web of Science Core Collection) from inception to July 2024. Our primary search was conducted on MEDLINE (See Supplemental Material) for English language publications, with no limitations in publication date. We included key search terms such as: Patient-led research, Public-led research, Community-led research, Indigenous-led research, Patient initiated research, Self-experimentation. The search strategy was then adapted to each of the following databases: CINHAL, EMBASE, PsycINFO, ProQuest Dissertations and Theses Global, Web of Science Core Collection (Supplemental Material). We hand-searched the reference lists of included documents and relevant review articles to identify additional sources.
Stage 3: Study Selection
The identified records were deduplicated and managed using Covidence systematic review software (Veritas Health Innovation Ltd, Melbourne, Australia). Two independent reviewers (EW, LT, NH, EQ, KM, TL, ML) screened each title and abstract to determine eligibility. Discrepancies were resolved by a third reviewer (LCL) as necessary. Full-text screening was completed by two independent reviewers (EW, LT, NH, EQ, KM, TL, ML) who then applied the full inclusion and exclusion criteria. Again, discrepancies were settled by the same third reviewer. To ensure conceptual clarity and consistency in applying the eligibility criteria, all reviewers participated in two structured training sessions, one prior to title and abstract screening and another before full-text screening. After the first training sessions reviewers piloted the screening criteria with a random sample of 50 titles and abstracts. See Supplemental Material for additional screening guidance materials that were provided to co-authors. Cohen’s κ was calculated to describe interrater reliability for calibration and at both stages of the screening process.
To identify studies with patient and/or public involvement at the IAP2 level of Empower, eligible articles reported health research where patients and public were responsible for one or more of the following roles or tasks: 1) made final decisions regarding the research process 2) initiated the research study (e.g., identified a research gap, set research priorities, and enlisted the support of researchers and other team members) 3) performed the investigation (e.g., collected data) 4) participated in the governance of the research process (i.e., administration and oversight)
37
5) assumed ownership of research products (i.e., control of access and distribution)
38
In keeping with this threshold to identify patient- and public-led research, we excluded articles that: 1) were led exclusively by researchers or healthcare professionals 2) involved patients or public solely as research participants 3) did not describe patients or public involvement in the research process 4) focused on areas outside of health research 5) did not report primary research 6) were not available in English 7) lacked an accessible full text
Stage 4: Charting the Data
A standardized data extraction form (see Supplemental Material) was developed in Excel following the Joanna Briggs Institute’s (JBI) template and guidance to capture key information from included studies (e.g., title, publication date, authors, country of publication). 35 The Guidance for Reporting Involvement of Patients and Public (GRIPP2) tool was incorporated to document aspects of patient and public roles and tasks. 18
Data extraction was pilot-tested in an iterative process according to the description from the JBI. 35 After five articles were extracted, the extraction template and process were reviewed and refined by two co-authors (EW, LT). 35 Through discussion, the co-authors agreed that elements of GRIPP2 overlapping with the JBI framework could be removed. They also determined that extracting complete paragraphs describing patient- and public-led research tasks and roles would best preserve the surrounding context and the nuances of language. 21 For practical reasons, data extraction was completed by the first author (EW). The extracted data was then reviewed by one of two co-authors (LT, NH). They assed the descriptive information and details pertaining to the different partner groups for accuracy, while information regarding patient- and public-led research contributions was checked for completeness.
Stage 5: Collating, Summarizing, and Reporting the Results
Descriptive statistics (i.e., counts and proportions) was used to summarize study characteristics such as publication year, country and study design, as well as characteristics of partner groups. To create our analytical framework for patient- and public-led contributions, we started by adapting the CRediT roles and tasks. 28 Through team discussions, we retained roles and tasks most relevant to patient- and public-led health research and removed those that were not applicable (e.g., Software, Validation, and Visualization). 39 For instance, we combined Data Curation with Data Analysis, Supervision with Project Administration, and Writing–Original Draft with Writing–Review & Editing due to conceptual overlap. Finally, we added Knowledge Mobilization to the taxonomy. See Supplemental Material.
Literature Mapping Framework and Examples
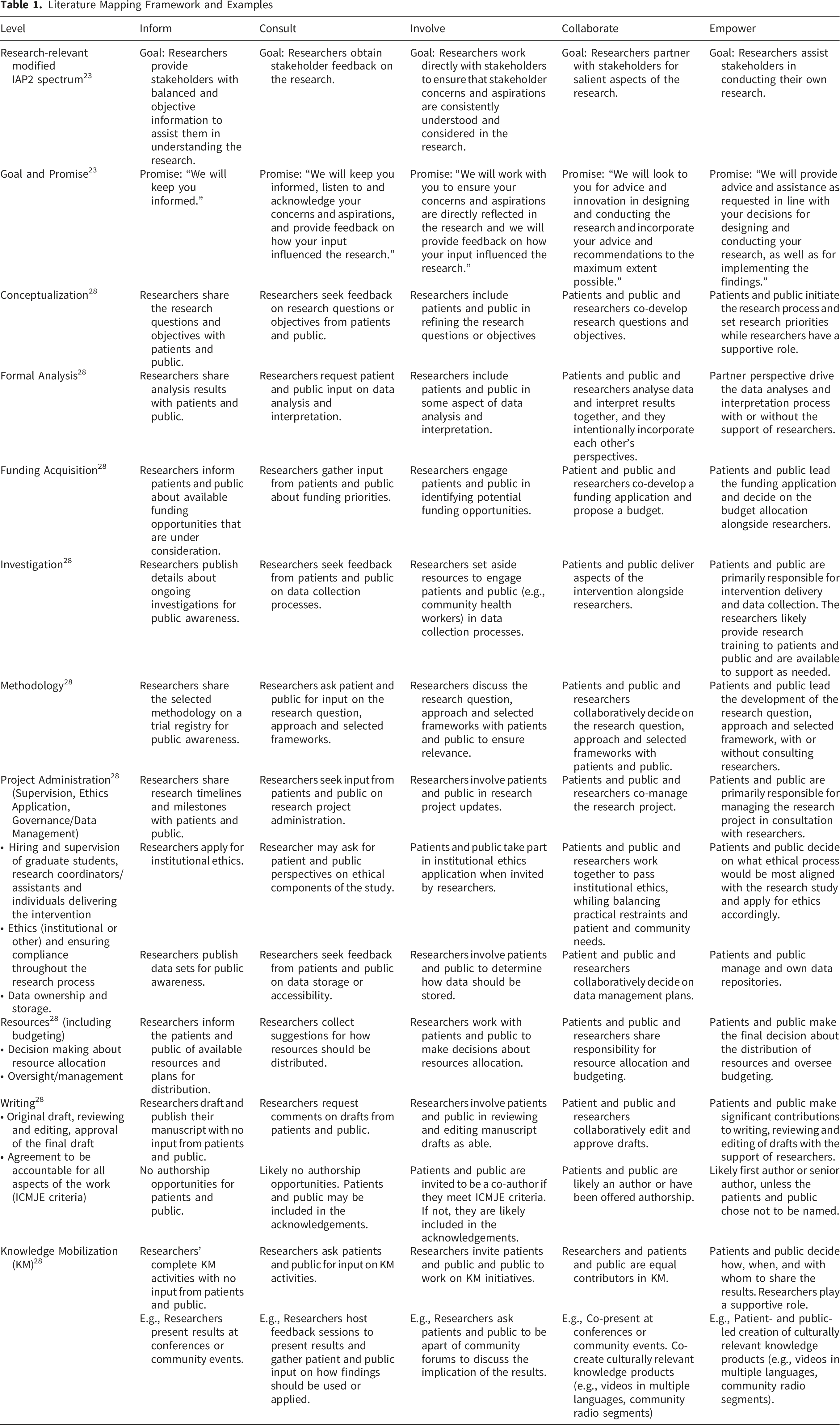
Finally, an abductive analytic approach guided our interpretation of patient- and public-led research contributions. Through iterative team discussions and ongoing reflection, patterns that extended beyond the standardized CRediT roles and tasks were identified inductively, allowing us to expand our understanding of contexts as they emerged from the data. This combination of deductive structure and inductive insight enabled a more nuanced pragmatic synthesis of how patient- and public-led contributions were operationalized and reported across studies.
Results
The search yielded 4723 articles, including 4449 from the health literature databases, 264 from grey literature, and 10 from hand-searching. After duplicates were removed, 4152 articles remained. Following title and abstract screening, 172 articles moved to full-text screening. In total, 68 articles that described 62 studies were included in the review. The PRISMA flow chart can be found in the Supplemental Material. After the initial training sessions reviewers piloted the screening criteria which resulted in 86% agreement (Cohen’s κ) across the seven reviewers.
At the title and abstract screening stage, agreement between reviewers was 93% (κ = 0.25). At the full-text screening stage, agreement was 80% (κ = 0.58).
Study Characteristics
Between 1996 and 2024, the number of publications that mention patient and public leadership in health research had increased steadily year over year (Supplemental Material). A total of 37 (60%) studies were conducted in North America (United States and Canada), 12 (9%) in Europe (Ireland, Sweden, United Kingdom), 7 (11%) in Oceania (Australia and New Zealand), 4 (6%) in Africa, 2 (3%) in South America, and 1 (<2%) in Asia. One study spanned both North and South America through a partnership between two Indigenous nations. 40 Included studies covered a range of health topics from maternal health to water contamination (Supplemental Material). The majority, 53 studies (85%) were non-experimental (i.e., observational). Of these, 27 (46%) used qualitative approaches, followed by 18 (29%) which used prospective or retrospective methods, 4 (6%) cross-sectional methods (e.g., survey), 4 (6%) studies employed mixed or multi-methods. Three (5%) quasi-experimental studies, and 1 (<2%) experimental study was captured. Notably, 5 studies (8%) were self-experimentation involving individuals designing and conducting scientific experiments on themselves (Supplemental Material).
Definitions and Terms Used to Describe Patient- and Pubic-Led Research

Partner Groups
Patient- and Public-Led Research Contexts
There were five (8%) studies led by patients and public with formal research training and academic credentials.53,65,71,84,97 One (<2%) study was led by patients with graduate degrees, but no formal research training in qualitative interviewing or analysis. 102 In five (8%) studies, patients and public completed formalized research training curriculums before taking on research roles and tasks.45,55,62,85,93
Patient and Public Contributions in Patient- and Public-Led Research
Overall, the most reported CRediT contributions, led by patients and public in the form of roles and tasks, were Conceptualization and Investigation (Figure 1). Of the 62 studies, 37 (60%) were initiated by patients and public (Figure 1), 17 (27%) by researchers, 6 (10%) by both patient and public and researchers, and one study each was initiated by multiple interest-holders (including a clinician, a researcher, and patients/public
89
) and by a pharmaceutical company.
102
In most cases, researchers were the primary holders of study funding; however, 23 (37%) studies reported how patients or public applied for, managed, or made decisions regarding funding allocation (Figure 1). While patients and public led Investigation in 55 (89%) studies, they took the lead on Formal analysis in only 28 (45%) studies. Notably, 52 (84%) studies included patients and public as co-authors (Figure 1). In one (2%) study, patients and public asked not to be named as authors on the manuscript because they did not wish for their names to be published.
99
Of the remaining studies, 5 (8%) formally acknowledged the contributions of patients and public, whereas 4 (6%) did not specify why patients and public who led aspects of the research were neither included as authors nor acknowledged. In many cases, the contribution of writing was not consistently detailed; therefore, the author list was used to deduce patient and public authorship. Further, no studies differentiated patient and public contributions during the initial draft versus reviewing/editing prior to publication. Typology of patient-and public-led research contexts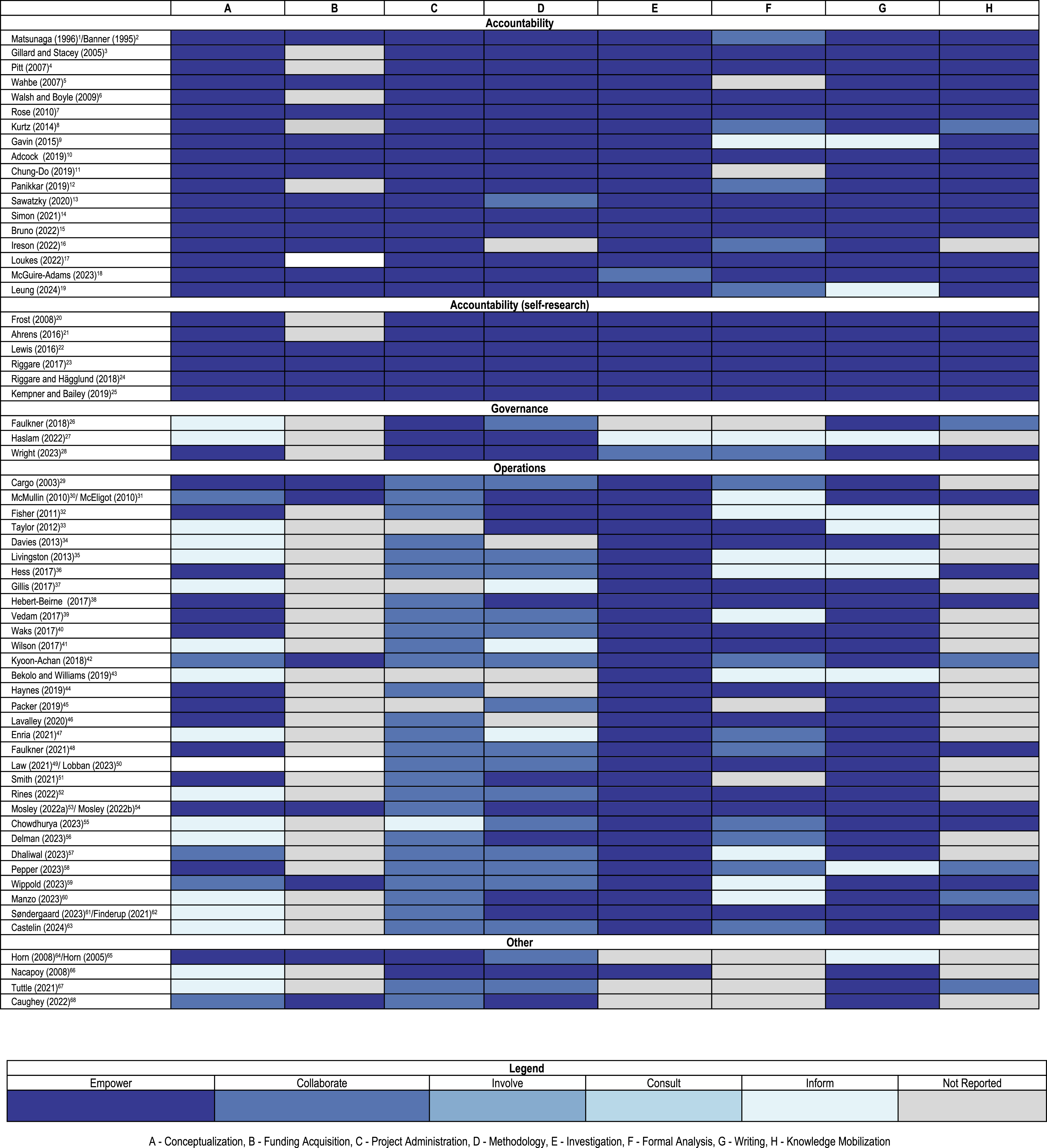
Our findings also revealed specific areas where patient- and public-led research is not only viable, but essential, particularly where traditional research structures are lacking. One such example is the work by PatientsLikeMe, which started as an online community that aimed to explore treatment options for amyotrophic lateral sclerosis (ALS) because mainstream institutional investment did not exist. 46 A second category of patient- and public-led research is self-research or collective self-experimentation, where individuals or groups document their own health data and test interventions outside of conventional research structures. For example, Lewis and colleagues created and collected data through an open-source automated insulin delivery system for people with Type 1 diabetes called OpenAPS. 61 A third area in which patient- and public-led work is highlighted in our review, is Indigenous-led research, where community leadership aligns with principles of self-determination, ensuring that research serves the needs of Indigenous communities rather than external academic priorities.88,92
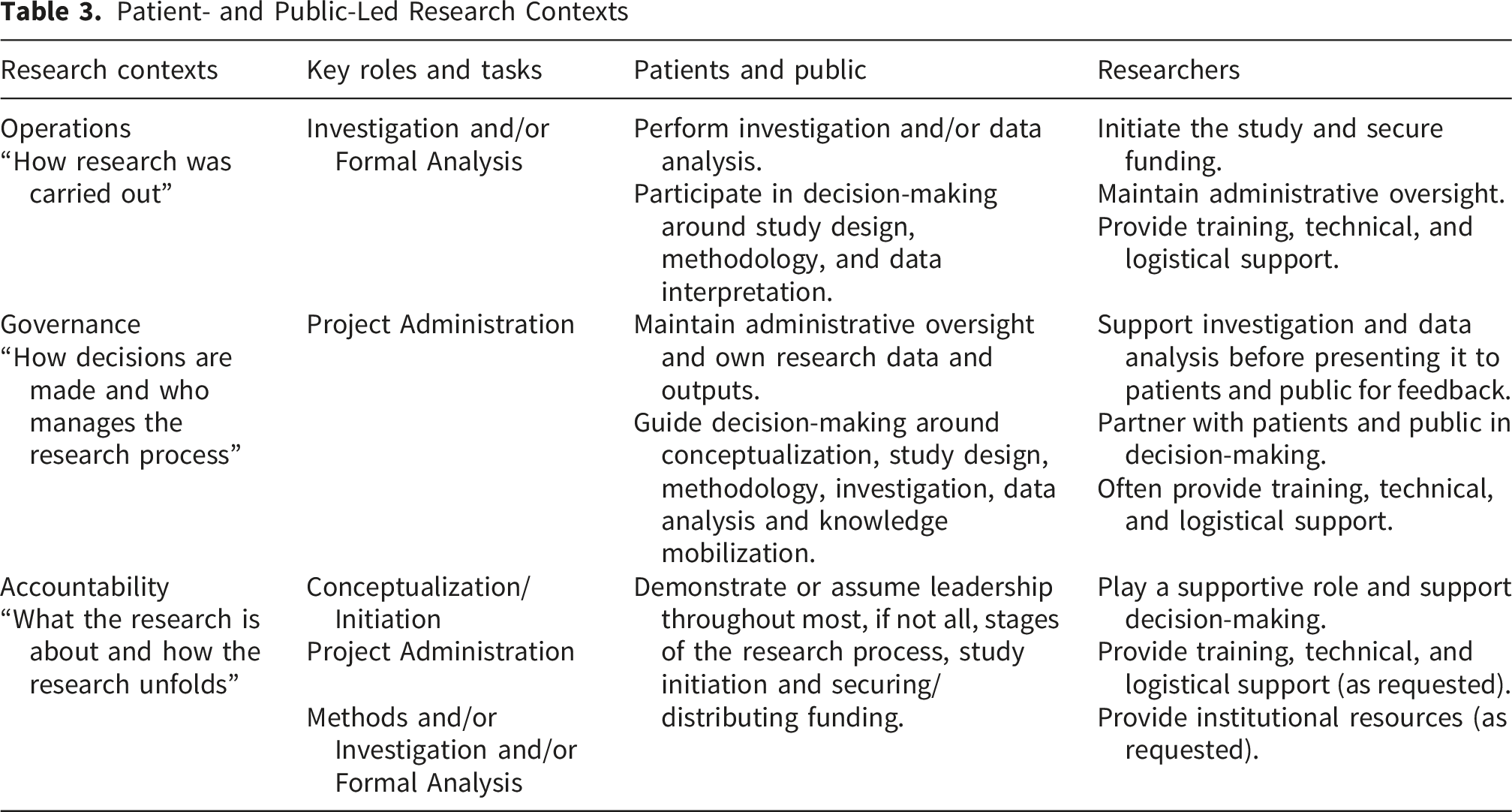
Contexts in Which Patient- and Public-Led Research Occurs
Three distinct contexts for patient- and public-led research were identified that describe how patient- and public-led research occurs, who holds power within these settings, and the role that researchers play: (1) Operations, (2) Governance, and (3) Accountability. These contexts emerged inductively from the mapping process and represent patterns that go beyond the limits of specific roles and tasks described by the CRediT. Of the 62 studies, 31 (50%) contexts are described as Operations, 3 (5%) as Governance, 24 (39%) as Accountability and 4 (6%) as Other.
In the Operations context, patient and public were most active in how research was carried out—primarily making decisions regarding investigation, and data analysis. Although they might also participate in conceptualization and study design, researchers generally retained decision-making authority throughout the remainder of the project. In this context, researchers often provided training and logistical support to patient and public partners.
In the Governance context, the focus shifted to how decisions are made and who manages the research process. Here, patients and public maintained administrative oversight, leadership in the study’s direction, and ownership of the research data and products. Further, they took on key roles during conceptualization and methodology development, while researchers typically provide support by carrying out investigation and conducting data analysis.
Finally, in the Accountability context, patients and public provided leadership in shaping what the research is about and how it unfolds. This includes identifying research priorities, which reflects their intellectual and experiential contributions. Further, patients and public assume power in project administration and play a notable role in the study design, data collection and analysis, writing, and knowledge mobilization. Researchers, when requested, act in a supportive capacity, providing technical expertise and institutional infrastructure.
Specific details regarding each of the three research contexts can be found on Table 3.
Studies categorized as “Other” did not provide sufficient information to determine whether patients and public contributed to investigation or formal analysis and were therefore coded separately.
Defining Attributes
Despite the IAP2 framework’s emphasis on decision-making authority as the primary distinguishing feature of patient and public involvement, our review demonstrated that patients and public exercise multiple forms of power through their contributions. For instance, they hold the power to set the research agenda and to determine which voices are included at the research table. Further, patients and public are viewed not only as legitimate contributors but as individuals whose positionality uniquely equipped them to answer the research questions. Secondly, our findings showed that patients and public draw on their own perceptions, understanding, and experiential knowledge to inform study design and conduct—much like a principal investigator (Table 3). These intellectual and experiential contributions were particularly evident in patient- and public-led study conceptualization (initiating the research and assembling the team), administration (maintaining control over the study’s direction), and delivery (deciding what data to collect and how to ensure alignment with community needs and values).
Discussion
The findings from this scoping review demonstrate that patient- and public-led health research is far from a monolith; rather, it is a dynamic and context-dependent process. By mapping the IAP2 continuum onto the CRediT contributions, we captured how patients’ and public’s decision-making authority varies across standardized research roles and tasks and identified three distinct contexts in which patient- and public-led research occurs. Our abductive, pragmatically oriented analysis sought not to impose rigid categories but to understand how patient- and public-led research is defined and practiced. What emerged is a landscape with little cohesion around formal definitions, yet one in which a meaningful typology can help reflect the complexity of real-world practice. Our review found that 11 studies (18%) were led by patients and public with graduate-level education or structured research training, challenging binary distinctions between “researcher” and “patient and public” and demonstrating that individuals can meaningfully occupy multiple roles within the research space.108,109 Moreover, researchers often assume supportive roles that require technical expertise and institutional access. Such tasks include registering study protocols, obtaining ethics approval, or managing research funds, and are closely linked to regulatory and institutional requirements that patients and public typically cannot navigate. While some community organizations and Indigenous groups have developed their own ethics processes40,58 and manage funding independently,41,94 these remain the exception rather than the norm. Taken together, these findings underscore the structural conditions that shape its practice. 110
Our findings revealed that decision-making authority does not distinguish patient- and public-led research from other forms of involvement. Instead, it is defined by who holds power within the research context. Specifically, power that extends beyond decision-making or taking on standardized roles. Steven Lukes’ influential theory describes three “faces” of power: visible power refers to decision-making authority. 111 Hidden power refers to control over the agenda itself. For instance, deciding which questions are asked (and which are not) and whose voices are amplified. Invisible power is the most subtle form as it shapes norms in ways that influence how research questions are defined and what “solutions” are considered possible. Without redistributing power across all three layers, patients and public may participate in visible decision-making, but remain excluded from shaping research trajectories.17,111 Arnstein’s warning that “representation without power” is a form of tokenism remains highly relevant to contemporary patient and public involvement practices. 112 Alongside power, intellectual/experiential contributions mark a second defining attribute of patient- and public-led research. Those with lived experience are not merely team members contributing perspectives to someone else’s project, but innovators. Together, re-distributed power in its multiple forms and patient- and public-led scholarly inquiry represent the essence of patient- and public-led research.
While patient- and public-led research is valuable for centering lived experience, it is not suitable in all contexts. Empower is sometimes assumed to represent the highest or most meaningful form of involvement, 15 yet what constitutes a mutually beneficial and effective partnership varies across contexts. 113 Recognizing the continuum of involvement does not diminish the value of patient- and public-led approaches. Our work deliberately focuses on this specific end of the continuum, where power is helped by and research is shaped by the intellectual/experiential contributions of patients and public to better understand its unique opportunities and challenges. For instance, our scoping review identified areas where patient- and public-led research has addressed and continues to address critical gaps in health research, not only those resulting from limited funding, 25 but also gaps in priority areas, 114 and methodological approaches. 68 When deciding on the level of involvement, it is important to consider the context, available supports, as well as the intentions of patients and public. Not all patients or public wish to lead research, nor are there resources available for them to do so in all case.115,116 Therefore, it is more productive to consider patient- and public-led research as part of a broader continuum of involvement, where diverse approaches serve differing needs. 20 By recognizing these distinctions, we can advance patient and public involvement more responsibly.
This scoping review highlights several important directions for future inquiry in patient- and public-led research. First, research efforts should focus on developing and assessing the transferability of frameworks and tools to support the conceptualization and practice of patient and public leadership. Second, there is a need for empirical studies that examine the processes and impacts of patient- and public-led research across diverse contexts. Platforms such as PatientsLikeMe illustrate the growing role of patient-driven data generation and knowledge production, yet the mechanisms through which these models influence clinical outcomes, healthcare decision-making and issues around equity remain underexplored. Finally, comparative studies can be helpful to understand how patient- and public-led approaches differ from PPI in terms of rigor and implementation to ensure the right supports are in place.
Limitations
Firstly, only English-language articles were included, which may have excluded relevant evidence written in other languages and skewed the distribution where we identified published literature. Second, due to the common constraints of publishing and word count, we were limited in our ability to extract specific details regarding patient- and public-led roles and tasks. As Sheikhan and colleagues (2025) observed, specific details regarding the negotiation of power, co-authorship processes and emotional labor are often cut or underreported, reducing both transparency and opportunities for collective learning. 117 We urge journals to consider developing a supplementary material guide to ensure detailed reporting of PPI and to mandate the use of reporting frameworks such as GRIPP2 to improve transparency and reproducibility.117,118
Conclusion
This scoping review clarifies the concept of patient- and public-led research by identifying three distinct contexts in which such leadership occurs. Together, these contexts offer a more coherent foundation for understanding patient- and public-led research. Further, our findings challenge the notion that the highest level of involvement is solely defined by decision-making authority. Instead, we argue that it is characterized by a redistribution of power across hidden, and invisible domains, alongside the intellectual and experiential contributions of those with lived and living experience. Finally, patient- and public-led research should be understood as one approach within a broader continuum of involvement, rather than a universal ideal. Moving forward, improved reporting practices, and the development of supportive frameworks will be essential to advancing this field in a rigorous and sustainable manner.
Supplemental Material
Supplemental Material - Patient- and Public-Led Research – How is it Defined and Practiced: A Scoping Review
Supplemental Material for Patient- and Public-Led Research – How is it Defined and Practiced: A Scoping Review by Ellen Wang, Linda Truong, Nejat Hassan, Erica Quershi, Khole Merry, Trinity Lowthian, Marisa Lin, Nelly D. Oelke, Heather Gainforth, Janet Curran and Linda C. Li1 in Journal of Patient Experience.
Supplemental Material
Supplemental Material - Patient- and Public-Led Research – How is it Defined and Practiced: A Scoping Review
Supplemental Material for Patient- and Public-Led Research – How is it Defined and Practiced: A Scoping Review by Ellen Wang, Linda Truong, Nejat Hassan, Erica Quershi, Khole Merry, Trinity Lowthian, Marisa Lin, Nelly D. Oelke, Heather Gainforth, Janet Curran and Linda C. Li1 in Journal of Patient Experience.
Footnotes
Acknowledgements
We would like to thank Rachael Bradshaw, subject librarian for Rehabilitation Sciences at the University of British Columbia for her support with designing, piloting and refining the search strategy.
Ethical Consideration
Ethics approval was not required for this scoping review.
Author Contributions
LCL – Conceptualization, Supervision and Visualization, Writing – reviewing and editing. EW – Conceptualization, Project administration, Investigation, Formal analysis, Visualization, Writing – first draft, Writing – reviewing and editing. NDO, HG, JC, LT, NH, EQ, KM, TL, ML – Methodology, Investigation, Writing – reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data underlying this study are available from the corresponding author upon reasonable request, subject to ethical and legal restrictions.
Open Access
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non-Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: ![]()
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.