
Abstract
Morbidity and mortality due to Asthma remains high Australia-wide, especially in Culturally and Linguistically Diverse communities, underscored by low health literacy and a lack of access to culture specific asthma care. A nurse-led asthma education programme incorporating Bicultural Health Educators to improve asthma outcomes was trialled in three of the communities most severely affected during a thunderstorm asthma event in Melbourne, Victoria, Australia. This study aimed to uncover unique asthma management challenges affecting these communities from a consumer perspective. A qualitative explorative design was applied, and 47 participants with asthma from Vietnamese, Sri Lankan, and Indian communities were interviewed. The participants completed two asthma education sessions, six weeks apart, with an Asthma Nurse Educator supported by a Bicultural Health Educator. At the first session, participants completed a questionnaire and undertook a narrative interview in which they shared their views on their asthma healthcare journey. Bicultural Health Educators recorded responses to open questions about perspectives and experiences of their journey, which were coded and thematically analysed. Key factors impacting on asthma management from the consumer and Bicultural Health Educator perspective included limited knowledge and understanding of asthma and its management, difficulties with inhaler technique and difficulty navigating asthma care in the community. Culturally-driven attitudes towards asthma management, along with low educational literacy levels also played a significant role. The study identified factors impacting asthma management in the Sri Lankan, Indian and Vietnamese communities in West Melbourne. Incorporating these insights can inform the delivery of asthma care and education to improve asthma outcomes for patients.
Keywords
Introduction
Asthma is a major cause of mortality in Australia, claiming 474 deaths in the year 2023. 1 Although the number of deaths from asthma has been halved over the last 35 years due to advances in asthma management and patient education, asthma continues to carry significant morbidity and mortality, particularly for people of culturally and linguistically diverse (CALD) communities. During the Thunderstorm Asthma event of 2016, patients of Indian, Sri Lankan and South-east Asian origin represented 39% of the asthma-related emergency department presentations and accounted for six of the ten deaths that occurred; 79% of these patients were born overseas. 2
Consumers from CALD communities face barriers to accessing healthcare at the patient, clinician and health system level, and are reported to have lower primary and preventative care attendances but significantly higher rates of secondary healthcare utilisation due to asthma, 3 culminating in poorer asthma outcomes.3-5
The provision of cultural support via multicultural health workers has been studied in both Australian and international settings as a strategy to help CALD patients navigate barriers in accessing healthcare.6,7 Compared to usual care, culture-specific asthma education programs have been identified to result in a greater improvement of asthma-related quality of life in both adult and paediatric populations and greater reductions in the rates severe asthma exacerbations in children. 4 We are trialling a nurse-led asthma education program, in which culture-specific asthma education sessions are provided to participants from Vietnamese, Indian and Sri Lankan communities in the western suburbs of Melbourne, Victoria with the support of Bicultural Health Educators (BHEs) to improve their asthma outcomes. The aim of this study was to uncover perspectives about asthma and its management from consumers and BHEs from these three communities.
Methods
A qualitative explorative design8,9 with individual narrative interviews was used to gather insights from participants and BHEs.
Participants
A total of 63 participants were approached of whom47 adults greater or equal to 18 years of age living with asthma were recruited, using convenient sampling from three communities: Sri-Lankan (Sinhalese) (n=8), Indian (Hindi) (n=24) and Vietnamese (n=15) between March 2023 to March 2024. Participants were recruited from respiratory outpatient clinics, following asthma-related hospital admissions, GP clinics and directly from the community through advertising and reaching out.
Procedure
Participants received an initial asthma education session led by an asthma nurse educator and a Bicultural Health Educator. Prior to commencement of the education program a baseline questionnaire collected the participants’ demographic data and assessed their initial understanding of asthma and its management. The participants were then invited to participate in an exploratory interview about their perspectives and experiences in managing their asthma with a focus on the role of the emergency department, role of the general practitioner, baseline asthma education and general understanding of asthma self-management. The interview lasted for up to 30 minutes and was conducted in their own language (by participant choice) by the BHE. The BHEs used a standard template and asked open-ended questions following an interview guide (examples are outlined in Appendix 1). This was followed by 1-2 hours of asthma education program that discussed asthma pathophysiology, symptoms, triggers, treatment, inhaler technique and self-management skills using the teach-back method. 10 The education was reinforced in a 6-week follow-up session. Both sessions were led by an asthma nurse educator and supported by a Bicultural Health Educator (defined on page 2). The interviews were not audio-recorded as participants can be impacted by past negative experiences with authority figures. There is evidence in the literature that the use of tape recorders in research among psychologically traumatised populations is discouraged due to several ethical and practical concerns. These include the potential for increased vulnerability to data breaches, third-party access risks, and the permanence of digital data. Additionally, recording sessions can create client self-censorship, therapist hesitation, and disrupted therapeutic alliances11,12 These factors can significantly alter the therapeutic environment and the effectiveness of the research process. In some communities like refugee groups, Indigenous populations, and survivors of political violence, recording devices carry historical or political meaning, like symbolising surveillance, oppression and interrogation, which can make participants reluctant or unable to engage openly.12,13
The Bicultural Health Educators documented participants’ thoughts, ideas and perspectives during and following interviews. Quotes were recorded verbatim by the BHE. The interview was immediately peer reviewed for accuracy and verified by both the BHE and ANE. The BHE and asthma nurse educator obtained detailed field notes and let the participants lead the storytelling. Non-recorded conversations followed by reflective writing were both documented during and after the interview, and the transcript was reviewed immediately. In addition to peer review, the research team reviewed the notes, which enhanced the credibility by ensuring consistency and rigour.
Data Analysis
Descriptive analysis was used to describe baseline demographics and quantitative data was presented as frequencies. The qualitative documentation from each interview was analysed using content (conceptual) analysis to identify the presence and meaning of certain themes or concepts.8-10 Key themes were identified and linked to construct a comprehensive and coherent narrative to answer the study aim.11,14,15 The analysis followed six stages: (1) familiarisation with the data set, (2) coding, (3) generating initial themes, (4) developing and reviewing themes, (5) refining, defining and naming themes and (6) writing up. Coding was blended using broad categories (deductive) initially, and inductive within that framework.11,14,15 In this interpretive framework, all collected data, whether written or observed, is treated as a text that reveals what is at stake within the lived experience, offering insight into the participants’ worldviews. The codes were then cross-checked by members of the research team, ensuring the credibility of thematic analysis. The interview documentation was de-identified and was repeatedly read by members of the research team ((ER, CVN,MJ, SS, LJ) and was grouped into meaningful themes to explain and interpret the content from the interview documentation. Illustrative quotes have been included to highlight the findings. The identified themes were presented regularly during data analysis, and interpretations were discussed among the research team (all authors) until a consensus was reached.
Reflexivity
Reflexivity is the capability to examine your own feelings, values, assumptions and motives for action and how these influence and shape thoughts and actions in a situation. 15 Both the Bicultural Health Educators and the Asthma Educators reflected on their experiences, roles, and responsibilities. The educators documented reflections on their own biases and assumptions, and on evolving themes, in a reflexive process to ensure the research was transparent and to confirm the credibility of the research findings.
Results
Baseline Characteristics of Participants
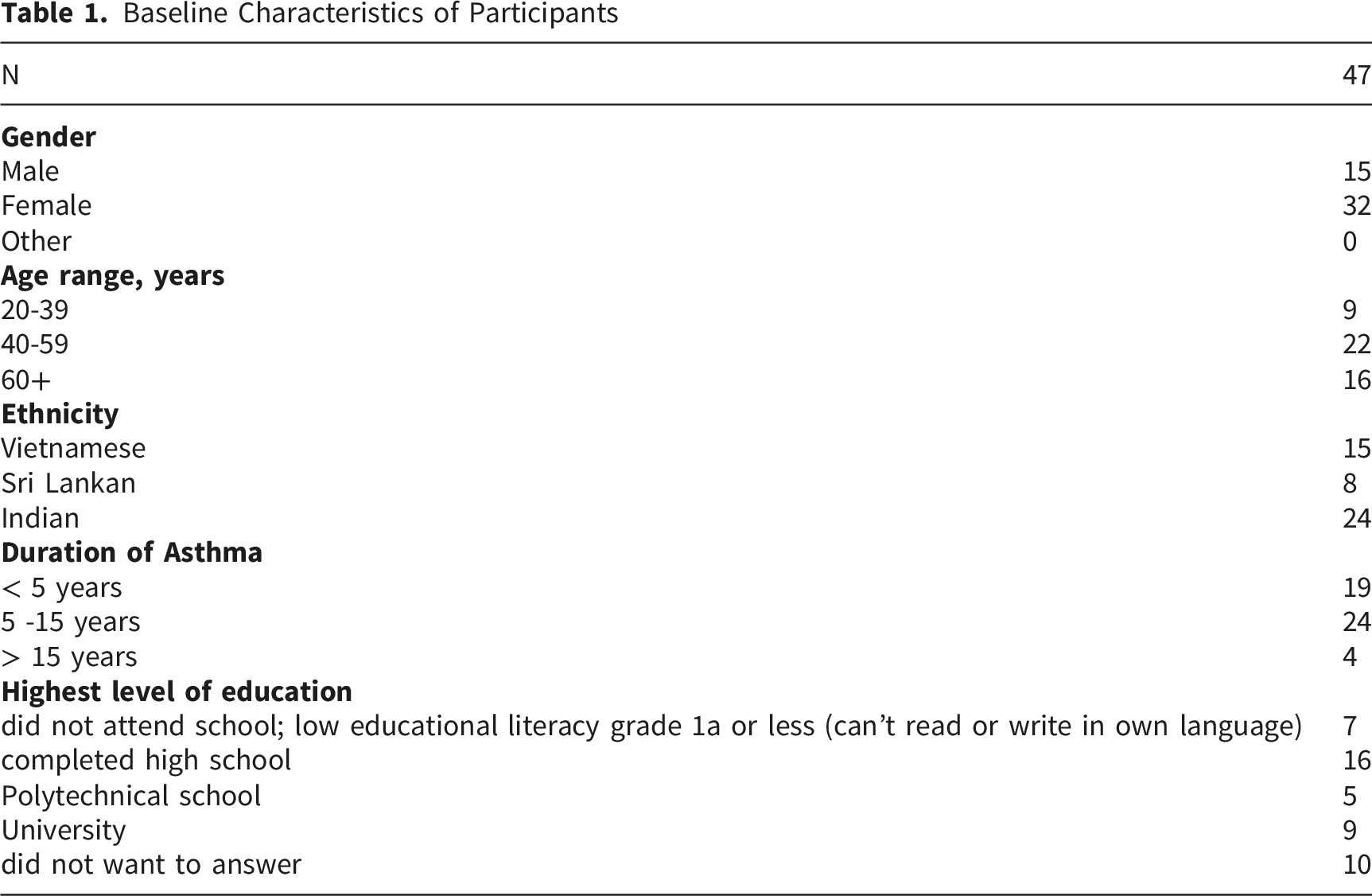
Participants and BHEs identified several factors impacting asthma management and these are detailed below. The overarching themes identified by both participants and BHEs included (1) limited understanding of asthma and its management, which incorporated the correct use of an inhaler and an action plan, (2) difficulties navigating asthma care in the community (3) asthma in the context of sociocultural beliefs and (4) limited educational literacy.
Limited Knowledge of Asthma and its Management
An Overview of Participants’ Responses to the Question “what is Asthma?” During the Baseline Questionnaire
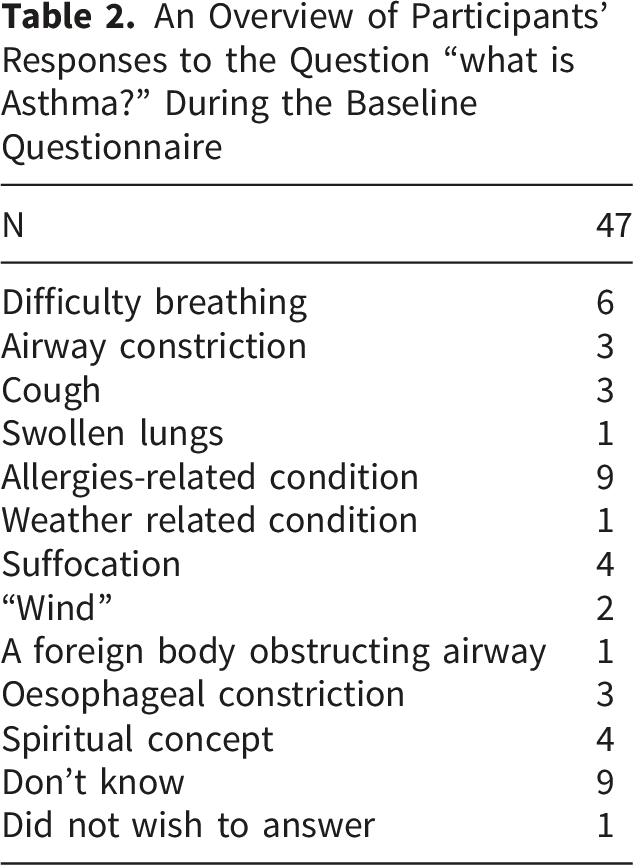
When asked “what is asthma” (defined as episodic wheeze, chest tightness or breathlessness for this study), 80% felt they did not have a good understanding of what asthma is; 19% answered “don’t know”, one attributed it to a foreign body in the airway, and three attributed it to oesophageal constriction. When asked about understanding of asthma, Participant 12 responded: “I don’t know, I was told that I got asthma, but I don’t have any understanding of the disease. The only thing that I know is that I struggle to breathe and to do any form of activity. For example today, I walked from the car to this office and I feel out of breath.”
Many participants were not aware of their asthma triggers.
Some participants did not recognise asthma to be a chronic disease requiring symptom control through lifelong therapy and had expectations of being cured. Participant 4 expected it would “resolve within a couple of years”, Participant 19 was “really confused why he is getting asthma again, thought he was cured when he was given some traditional medicine when he was a child back in Vietnam.” Control of symptoms with regular medication was viewed as being unwell.
Difficulties in Using Asthma Medication and Action Plans Appropriately
The limited understanding of asthma and its management contributed to the difficulties noted with appropriate use of asthma medication and action plans. Reflections from both participants and BHEs demonstrated that the majority did not know the difference in indication for their preventer (81%) and reliever (64%), could not identify the correct time to use each medication, and could not distinguish the different inhalers from each other (Figure 1). Participant knowledge of asthma relievers and preventers as per baseline questionnaire. Created in BioRender. Jayakody, M. (2024) https://BioRender.com/g14t749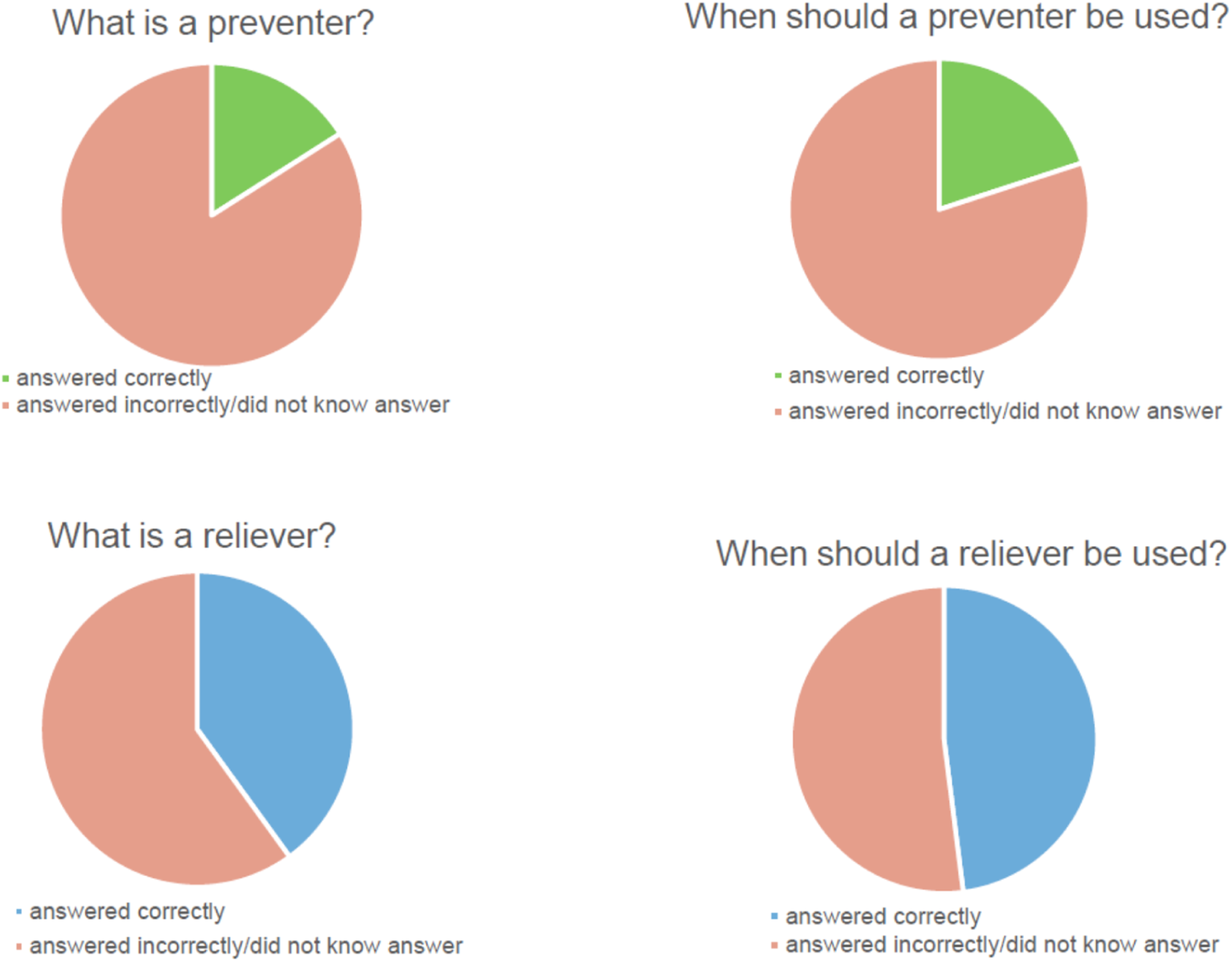
Many participants did not know how to escalate their asthma therapy during exacerbations; for instance, Participant 12 “brought medication with him - they include multiple preventer and reliever inhalers and prednisolone. When he is having an asthma attack, he will take one or two puffs from each of the above medication.”
Many participants did not know how to track their medication use or read the built-in dose counter on the inhaler, and as a result continued to use empty inhalers. Participant 11 “didn’t know when to tell if device was running out. He has never paid attention to the number/colours on the puffer.” Participant 16’s “Ventolin expired in 2020” as he was “not aware where to find expired date on puffer”. Multiple participants had not visited a GP to get up-to-date prescriptions to replace their medications, including Participant 18 who had “been using her friend’s reliever puffer…”
Notably, no participants reported possessing a current written asthma action plan that they understood. Some participants did not recognise a need for dedicated asthma education as they perceived themselves to have adequate knowledge of asthma through lived experience; Participant 2 “declined an asthma plan, stating that “I have been asthmatic all my life, I think I know what to do.” On further exploration, there were significant knowledge gaps identified in these participants, which were addressed by the BHEs. One BHE observed that Participant 11, who had errors in spacer and inhaler technique that he knew everything as he attended GP and hospital clinic appointments regularly.”
Difficulties in Navigating Asthma Care in the Community
Challenges navigating the healthcare system was a central theme. While most participants had a nominated GP (Table 1), they did not seek regular care or did not have continuity of care with a single GP. BHE 1 and 2 observed: “A lot of patients do not understand the importance of longevity of care by the GP. This should be explained to patients and highly encouraged.”
BHE 1 observed: “Patients are seeking care from health centres but they 1) do not rebook patients with same GP and 2) GP's may not allow patients to ask more than one question/problem in the consult. This is a huge problem because they are not dealing with patients as a whole and can often miss diagnosing or attending to things that need to be looked into.”
Participants reported instances of attending the GP clinic when feeling very unwell with asthma, which resulted in them being sent to ED. This experience led to the perception that General Practitioners may have limited ability to manage acute asthma. However, patients’ insufficient understanding on how to escalate asthma therapy during exacerbations combined with their late presentation to the GP with an asthma flare contributed to this.
Participant 3 “expressed feelings of frustration with his GP. When he attended GP, he felt very unwell, unable to breathe and he was told by GP that he could not give him oxygen,ambulance was called (participant story telling).” This experience negatively impacted his trust in his GP, making him less likely to seek early GP care for subsequent exacerbations, and to present directly to ED instead.
Participants noted challenges to obtaining asthma education during clinic or GP visits. Participant 3 expressed “his discontent as there is no education given about his condition.” Participant 23, who was taking inhalers and tablets for asthma, expressed a need for “more information on side effects of long-term medications” Participant 17 reported that while her doctor provided information on asthma, she “did not comprehend this and would like someone to explain to her in plain English.” BHE1 observed: “Patients are eager to speak in English. But they cannot understand everything in English and their confidence may not be a true representation of their comprehension.
Asthma in the Context of Cultural and Social Experiences and Beliefs
Cultural and social beliefs contributed to participants’ perceptions of asthma and their medication use(Figure 2). When discussing poor preventer usage, participant 9 reported that “in her culture, medication is only used when someone is really sick, if there is no symptoms, medication is disregarded.” Social and cultural factors impacting asthma management prominent in each community. Created in BioRender. Jayakody, M. (2024) https://BioRender.com/g14t749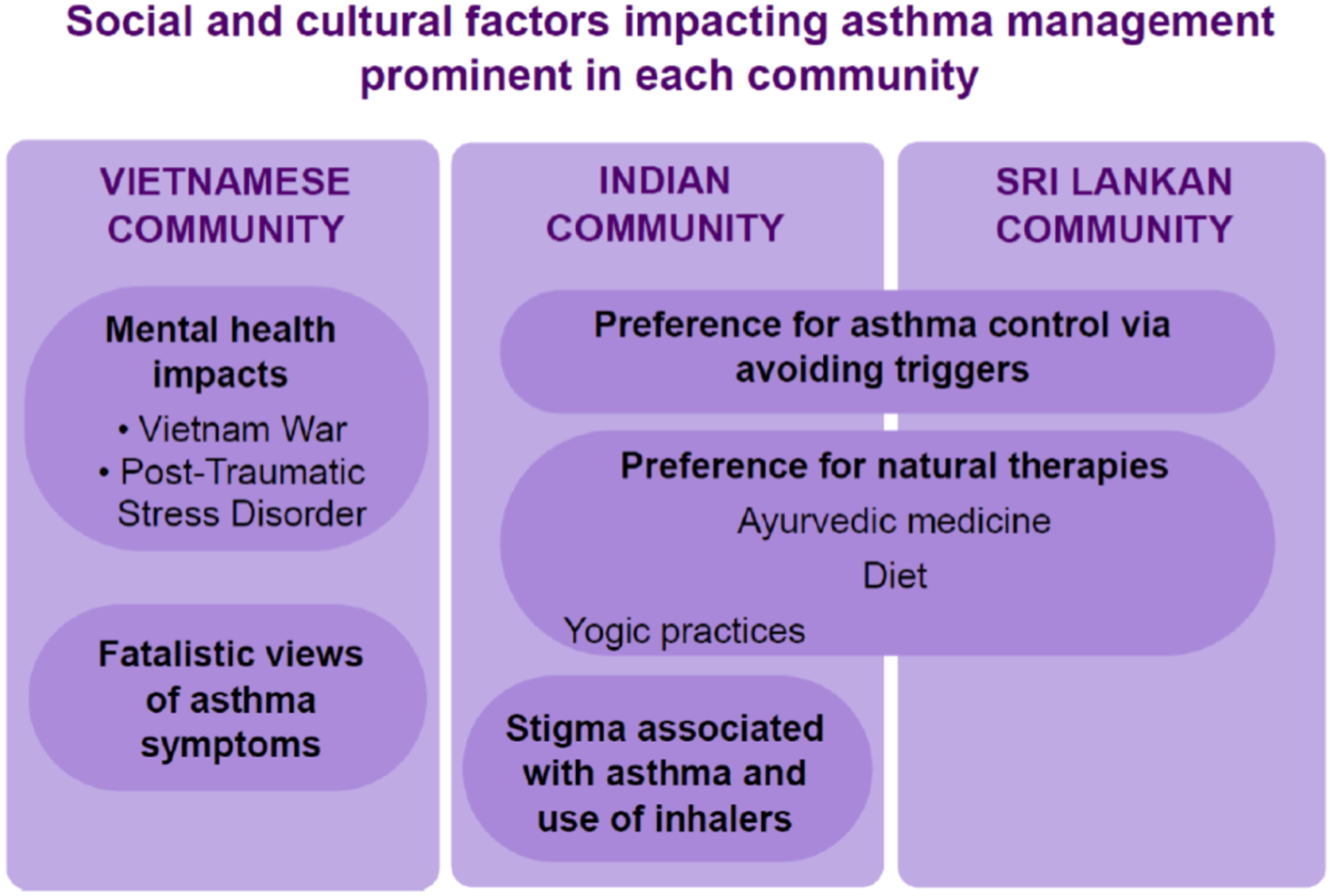
Experiencing shortness of breath from asthma carried various social and spiritual connotations in some cultures. Participants in the Vietnamese community held fatalistic spiritual views regarding the symptom of breathlessness; Participant 12 expressed the belief that “your breath is your life and once it is gone you are dead,” Each asthma exacerbation was perceived as a loss of ‘vitality’ or ‘life essence’ and a sign of inevitable death which could not be influenced by medical treatment.
Some Indian participants expressed that there was social stigma associated with using inhalers, with 42% therefore feeling reluctant to use inhalers regularly. As one BHE noted: “In India, people often call asthma “Dama”…Participant 3 said her mother told her, “Do not tell anyone in the family, relatives, or friends that you have Dama.” This advice comes from concerns that sharing this information could be perceived as poor health, and affect future prospects. “Because of this, she stopped using her inhaler in public.”
Participants from Indian and Sri Lankan backgrounds showed an interest in controlling their asthma through methods they believed to be more “natural” with less side effects, including dietary modifications, avoidance of triggers, yoga and traditional or Ayurvedic therapies, often preferring these to inhaler therapy. Participant 9 was advised by her friend “Steroids are addictive and have more side effects, which cause more harm than good.”
BHE 2 noted: “Indian participants often select homeopathy or Ayurveda for chronic conditions, viewing these methods as safer over time…Patients often receive Ayurvedic, homeopathic, or herbal supplements from their home country, sometimes without their allopathic doctors knowing. This strong belief in Ayurvedic principles is a key part of healthy living for Asian Indians, taught to them from a young age.”
The hot and cold theory of illness was a prominent belief within the Indian and Sri Lankan participant groups, in which certain foods were attributed the property of being “hot” or “cold”; consuming “cold” foods were believed to exacerbate mucus production and airway disease, and consuming “hot” food was believed to result in inflammation. Participant 13 believed that “eating cold food makes it hard to breathe and causes coughing; otherwise, I have no disease”. As one BHE observed, “allergies are due to an imbalance of hot and cold and that it's important to avoid all foods that are considered “cold,” like rice, yogurt, ice cream, salads, juice, etc.”
Many older participants placed the onus on health professionals to provide all necessary information on asthma management, due to attitudes built through interacting with more paternalistic healthcare systems in their countries of origin. They were inclined to accept their diagnoses without seeking further information. Participant 12 “[did] not have knowledge of asthma; it is something that they have just been told [ they had ] and accepted.”
For many of the participants, the acculturative stress of migration had created a profound sense of displacement, which affected their asthma management experience and their interactions with the healthcare system. This was especially true for the Vietnamese population, which included those who had migrated to Australia as refugees during the Vietnam war. Forty -five percent of all study participants reported stress, anxiety or depression as having an impact on their asthma management – of these, 53% were from the Vietnamese community. BHEs observed that the mental health needs of some participants who suffered from post-traumatic stress following the Vietnam war had not been adequately addressed, and over time led to issues with substance misuse and breakdown of family and community relationships. This resulted in social isolation and feelings of intense anxiety around being unwell from asthma; for example, participant 12 “elaborated on [his] fear of dying from an asthma attack and that he does not have close relatives to check on him.” For this participant, the burden of mental illness was a barrier to regular medication adherence and attending appointments. Memories of conflict experienced in his home country was also a trigger for shortness of breath, which he attributed to asthma and would attempt to treat with inhalers. He had never received formal mental health services and was not equipped to identify or manage physical symptoms of anxiety, including panic attacks.
” Participant 15 reported that her struggles with mental health made it difficult to adhere to consistent asthma medication use, but felt “reluctant to deal with mental health because of social stigma and cost.”
Impact of Language Literacy on Asthma Management
Limited educational literacy (in addition to low health literacy) was a key theme that impacted asthma self-management skills. Low literacy levels in both English and first languages were noted in fifteen per cent of participants, as evidenced by self-report and targeted questions on the baseline questionnaire (Table 1), making it particularly challenging for them to obtain asthma information. Participant 13 was from a “Low education background from a rural area in Vietnam” and stated that she ‘can’t read or write in Vietnamese and this makes things a bit harder’ for her. She believed this interfered with her level of comprehension to follow instructions.
Low literacy levels also affected the participants’ ability to advocate for themselves and to seek further understanding of their diagnosis, as noted by BHE1: “low literacy/academic experience lessens their confidence to feel empowered in their diagnosis. They start the session with little confidence about understanding asthma and accept this without trying to seek understanding. Once they are educated in a way that is understandable to them, it is clear that there is a shift in their confidence and they become more positive regarding their outcome. Fear of dying from asthma is settled.” Participants often responded well to analogies and explanations related to their occupational background. BHE1 observed that “It is very helpful to ask the patient what they do/did for work. This can help with explanations for the lay person e.g. a handy man can have airways described as pipes.”
Discussion
This study describes the complex challenges faced by culturally and linguistically diverse communities in managing their asthma, focusing on three cultural groups (Vietnamese, Indian and Sri Lankan) who were most severely affected by the thunderstorm asthma event in 2016.16,17 While this event has been widely studied in literature, this paper, to our knowledge, is the first that explores specific, persistent challenges to long-term asthma control in these affected groups from a patient perspective.
Themes that impacted asthma management included limited health literacy and self-management skills, often compounded by poor educational literacy. These barriers are likely to worsen outcomes because they reduce patients’ ability to recognise symptoms appropriately, distinguish preventer from reliever therapy, use inhalers correctly, and respond to deterioration in a timely manner. Difficulties navigating the health care pathway further interrupt continuity of care, while spiritual and/or cultural beliefs about illness and medication can shape whether treatment is viewed as necessary or safe. Together, these factors modify a patient’s perspective from preventive asthma care leading to good symptom control towards reactive, symptom-based management which reduces asthma control and increases the risk of exacerbations.
The limited knowledge of asthma among participants was, in part, related to the fact that asthma is a relatively unfamiliar disease within the migrant populations featured in this study. Multiple Australian studies have demonstrated that South Asian and East Asian migrants who have no allergic or atopic symptoms pre-migration show increased susceptibility to asthma following arrival in Australia compared with the general Australian population.16,1718 This is thought to reflect sensitisation to environmental triggers such as grass pollen over time, with asthma incidence directly correlating with length of stay in Australia.18-20 When a condition is both newly acquired and poorly understood, patients are less likely to recognise its underlying pathophysiology (e.g. airway inflammation in asthma) and more likely to interpret treatment through the lens of acute symptom relief. Language barriers intensify this problem by limiting access to predominantly English-language asthma resources and reducing opportunities for independent learning. As a result, there may be gaps in a patient’s understanding of asthma, trigger avoidance, inhaler technique, preventer adherence, and early escalation of care, all of which can contribute to poorer long-term control.
Some patients accepted information provided by healthcare professionals without seeking additional clarification. This attitude appears to reflect a complex interaction between low empowerment within an unfamiliar culture and health system21-23 and prior more paternalistic healthcare settings, where patients may defer to physicians and avoid questioning treatment decisions. 24 This matters for asthma outcomes because effective self-management depends on active participation: patients need to ask when to use each inhaler, demonstrate technique, clarify side effects, and understand what to do when symptoms worsen. When patients do not feel able to voice uncertainty or disagreement, misunderstandings can remain hidden, leading to incorrect medication use, low adherence and delayed help-seeking. Creating a safe space where patients can express concerns, identify and address knowledge gaps, negotiate treatment plans and build the confidence required for sustained asthma control is paramount, as articulated by the BHEs in this study.
A UK study involving South Asian participants with asthma 25 found limited familiarity with preventer inhalers and asthma action plans among first-generation and recent migrants, with reactive and curative care, rather than preventive care, reported as the norm in their countries of origin. This helps explain why preventer therapy may be underused in our cohort: if medication is understood primarily as something to be taken only when there are symptoms, daily inhaled corticosteroid use can appear unnecessary or excessive. Social stigma around inhaler use and reluctance to take medication unless symptomatic further reduce adherence. 21 The preference for alternative methods to control asthma among South Asian patients, such as avoiding certain foods and practising yoga, has also been demonstrated in previous studies21,22 and was reflected among the Indian and Sri Lankan participants in our cohort. These holistic practices are often beneficial, but poorer outcomes may arise when they substitute for, rather than complement, evidence-based preventive treatments which target the underlying airway inflammation in asthma.
For many participants of this study, poorly controlled asthma affected mental health, social life and physical activity. This is congruent with findings in previous literature; for example, 55% of adults surveyed in Singapore found asthma to have limited their physical activity in the last month, and 42% felt low in mood because of their asthma. 26 Mental health issues were noted to impact asthma control in nearly half of our study participants, and in some Vietnamese patients, it was compounded by post-traumatic stress and social isolation. Managing the complex mental health overlay to asthma care in these patients requires cultural support and community de-stigmatisation of the diagnosis and management, in addition to referrals to appropriate mental health services. The presence of Bicultural Health Educators is particularly valuable in uncovering such issues, which patients are unlikely to disclose to their clinicians during routine care even with interpreter support.
Studies have also shown the benefit of multicultural health workers in improving health behaviours in culturally and linguistically diverse communities.7,27 The likely mechanism is not simply language translation, but improved comprehension, trust, disclosure, and tailoring of advice. In our program, Bicultural Health Educators functioned as a form of community-based language-concordant care. Because optimum asthma control depends on mastering several initially complex skills, including inhaler technique, symptom interpretation, trigger avoidance management, and action-plan use, the high level of health literacy among the BHEs enabled them to adapt education to the schooling, occupational, and cultural background of patients. This likely reduces misunderstanding, increases confidence and adherence, and strengthens patients’ capacity to manage asthma before deterioration occurs.
The perspectives and solutions provided by patients and their bicultural health educators in this study incorporated broader frameworks of patient experience and supported self-management models of care. For example, Oben 28 has contextualised the health journey through the perspective of the individual, from a person in good health to a patient experiencing disease, and finally as a consumer of health services. While the person moves across this health continuum, it is attention to the 4 dimensions of the human experience (physical, psychological, social and spiritual) that determines the quality of the patient experience. 28 Frameworks to support self-management skills for chronic disease have also been developed. 29 These incorporate a patient-centred, health systems and shared responsibility approach, encouraging relevant stakeholders to collaborate and deliver appropriate, equitable supported self – management programs to all consumers. 29
Strengths and Limitations
Hearing directly from consumers navigating the health system with asthma is a key strength of this study. Only three communities’ perspectives are documented, and therefore these results may not be generalisable. Given that some participants were recruited from respiratory clinics and following hospital admissions, the study may be capturing a cohort with a higher prevalence of severe asthma than noted within community settings. A greater proportion of females than males participated in this study, and again this could impact the generalisability of the results. While some of the perspectives identified in this study may apply to other CALD communities, each community may have their own barriers to care, which require exploration through further research. The lack of audio-recorded verbatim transcripts and the presence of the educators during the interviews could have been potential limiting factors. We, however, made an apriori decision not to record the interviews to establish participant trust and took appropriate counter measures to address this (described under the Methods section). We also found that during the interviews Educators were perceived as allies, as participants felt that they could express themselves freely with people who understood their situation. The research team acknowledge that the dual role of the BHE as interviewer, translator and recorder might influence data collection and interpretation; however, the risk of making the participants reluctant or to engage was greater than the limitation the dual roles might have. This method might, in fact, be a strength and be innovative for obtaining data when participants feel they are in a culturally safe environment.
Implications for Future Practice
The reflective nature of this study provides insights into unique cultural experiences and perspectives on asthma management among the three communities, and provides a roadmap for structuring future Bicultural Health Educator-supported asthma education sessions to better fulfil the needs of these consumers.
Conclusion
This study highlights the complex barriers to asthma management and emphasises the need for asthma care that considers linguistic, cultural, and individual factors. Moving forward, integrating cultural support into the provision of asthma education and asthma management may contribute to improved asthma outcomes in our communities.
Footnotes
Acknowledgments
This study is supported by the Western Health Disease Alliance, Western Health and Asthma Australia. We thank the participants for their time and contribution.
Ethical Considerations
The study was approved by our Regional Low-Risk Ethics Committee (LNR/22/WH83847) and was conducted according to the Code of Ethics of the Declaration of Helsinki and Good Clinical Practice Guidelines.
Consent to Participate
Participants provided informed consent.
Author Contributions
All authors contributed to the study conception and design, material preparation, data collection and analysis. The first draft of the manuscript was written by MJ and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Grant Support provided by Asthma Australia through the Ray O’Donnell Belgrave Lions Asthma Research Fund.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.