
Abstract
Background
T2DM Mellitus is a complex chronic disease that affects adults of any age. Diabetes self-management and self-efficacy are associated with glycemic control.
Objective
To assess self-management, self-efficacy, and glycemic control and their relationship in adults with T2DM in the West Bank.
Methods
A cross-sectional descriptive design was used. A convenience sample of 154 patients was obtained from the primary health directorate’s diabetes clinics in Ramallah and Al-Bireh governorate, West Bank.
Results
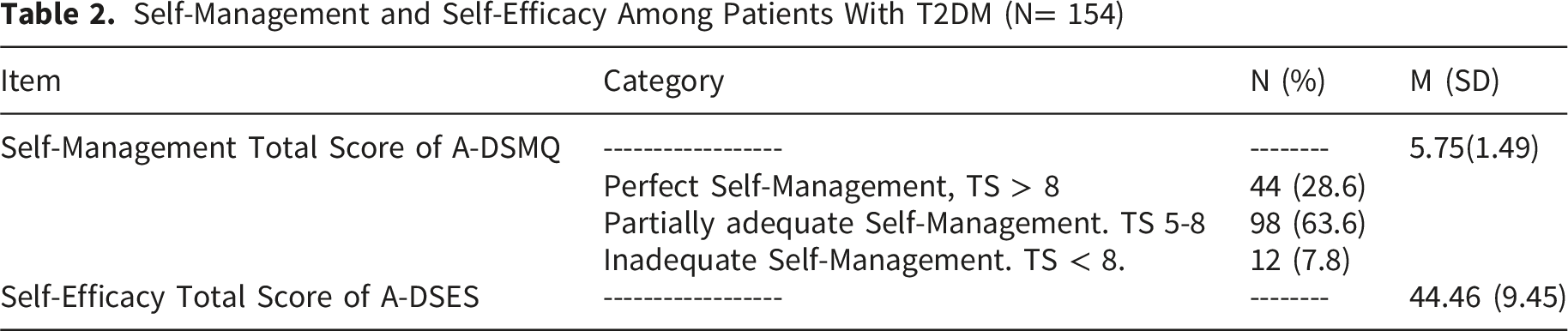
The mean diabetes self-management score was 5.75 (SD = 1.49), with most participants demonstrating low self-management ability (n = 110, 71%). Participants also reported low perceived diabetes self-efficacy, with a mean score of 44.56 (SD = 9.45). Glycemic indicators reflected suboptimal control, with a mean Hemoglobin A1c (HbA1c) level of 8.7% (SD = 1.62) and a mean fasting blood glucose of 175.43 mg/dL (SD = 73.43). Self-management was significantly negatively correlated with body mass index (BMI) (r = −0.165, p = 0.041) and HbA1c (r = −0.209, p < 0.01), while showing a significant positive correlation with diabetes management self-efficacy (r = 0.576, p < 0.01).
Conclusion
Diabetes self-efficacy and self-management were significantly linked to better glycemic control and improved diabetes outcomes. The use of tablets as the only treatment regimen was associated with significant improvement in glycemic control. Fasting blood sugar may serve as a predictor of long-term glycemic changes and support early diagnosis and screening. In addition, body mass index significantly influences diabetes self-management, self-efficacy, and glycemic control.
Introduction
Type 2 Diabetes Mellitus (T2DM) is a complex chronic disease characterized by an impaired glucose balance, which, over time, leads to severe complications such as retinopathy, neuropathy, and cardiac diseases (American Diabetes Association Professional Practice Committee, 2023). Although the causes of diabetes remain unclear, unhealthy lifestyles, physical inactivity, family history, and ineffective diabetes self-management make a significant contribution to developing diabetes (E. Ahmad et al., 2022; Banday et al., 2021). T2DM is considered largely preventable, and remission may be achievable in some individuals when the disease is identified early and managed appropriately (ADAPPC, 2025). Similarly, the Centers for Disease Control and Prevention (CDC) calls for the integration of knowledge from clinical studies into behavioral change, promoting theoretical models of empowerment that overcome the psychosocial impediments to self-management, using the Diabetes self-management education and support (DSMES) to improve the self-efficacy andf diabetes self- care (CDC, 2020).
Literature Review
Diabetes management is increasingly recognized as a global public health priority within international chronic disease agendas. The World Health Organization identifies diabetes as one of the major noncommunicable diseases (NCDs) that contribute substantially to premature mortality, disability, and healthcare burden worldwide, emphasizing the importance of strengthening self-management and continuity of care as core strategies to improve outcomes (WHO, 2026).
Similarly, the International Council of Nurses highlights the central role of nurses in chronic disease prevention, patient education, and long-term self-management support, particularly in underserved and resource-constrained settings (ICN, 2024).
Accordingly, treatment of T2DM is a comprehensive process; it combines adherence to medications and healthy lifestyle changes (ADAPPC, 2025; Suryasa et al., 2021) with a strong association between self-efficacy and self-management as core behaviors in achieving optimal glycemic control (Quynh Anh et al., 2024). Self-management of diabetes includes monitoring blood glucose, eating a healthy diet, remaining physically active, adhering to the treatment regimen, taking medications on time, and reducing risk behaviors (F. Ahmad & Joshi, 2023). While self-efficacy reflects the ability of the individual to take ownership of their motivation, behavior, and social environment, these abilities affect how an individual behaves in a given situation or new experience, such as in the context of chronic disease (APA, 2024).
According to the International Diabetes Federation (IDF) (2021), the burden of diabetes is increasing. About 10.5 % of people aged from 20 to 79 have diabetes (537 million). In the Middle East and North Africa, 72 million people aged from 20 to 79 years have diabetes. This number is expected to be 95 million by 2030. In Palestine, the number of people with diabetes was 124,000 in 2011, increased to 183,000 in 2021, and is expected to reach 262,000 in 2030 (IDF, 2021). The burden of T2DM in the MENA region is increasing significantly, with rising mortality, incidence, and prevalence. The major contributing factors are high Body Mass Index (BMI) and low physical activity (Namazi et al., 2024).
Adherence to recommended diabetes self-management behaviors remains suboptimal worldwide, particularly given the long-term nature of treatment and the development of complications (F. Ahmad & Joshi, 2023; CDC, 2024; Peng et al., 2022). Further, although patients’ self-efficacy is strongly associated with their ability to self-manage diabetes and achieve glycemic control (AlShezawi et al., 2025; Oluma et al., 2020), a critical synthesis of the literature reveals a fragmented understanding of the interplay between these behavioral variables in conflict-affected or lower-middle-income countries. Regional studies in the MENA region, such as those in Jordan and Oman, report a persistent failure to achieve optimal self-management despite reported high self-efficacy among patients with T2DM (Almomani & Al-Tawalbeh, 2022; AlShezawi et al., 2025). Several countries in South Asia and the Middle East, including India, Oman, Jordan, Iran, and Pakistan, report a substantial burden of T2DM, low self-efficacy, and poor self-management (AlShezawi et al., 2025; Aseela et al., 2024; Saleem et al., 2025).
Consistently, patients with diabetes in the Palestinian context experience the global burden of diabetes, which ranks as the fourth leading cause of death (MOH, 2021), along with poor self-management, inadequate glycemic control, and reduced quality of life (Ghoul et al., 2025; Mosleh et al., 2017; Tietjen et al., 2021). However, in contrast to the limited available evidence, Palestinian patients with T2DM report high perceived self-efficacy despite poor glycemic control and diminished quality of life (Eshtaya et al., 2025).
To address this gap, this study utilizes the Health Belief Model (HBM) as its guiding framework. The HBM suggests that a patient’s adherence to self-management is dictated by their perceived threat of the disease and the balance between perceived benefits and perceived barriers to action. Central to this process is self-efficacy, the cognitive engine that drives an individual’s belief in their capacity to execute essential health behaviors (Alyafei & Easton-Carr, 2024). In the context of T2DM, these constructs are particularly relevant because effective disease management requires sustained engagement in daily self-care behaviors. Examining these variables together adds new knowledge by shifting the focus from descriptive patient deficits to a conceptual exploration of behavioral pathways. By investigating self-efficacy as the psychological driver and self-management as the behavioral manifestation, this study seeks to identify where the ‘behavioral chain’ breaks in the transition to clinical glycemic control.
Although self-efficacy and self-management have been widely studied independently, limited evidence has examined their integrated behavioral relationship with glycemic control among adults with uncontrolled T2DM in resource-constrained settings, who need more attention to enhance their self-efficacy and self-management (Quynh Anh et al., 2024); replication of this study in this context adds valuable insight to the available literature. Thus, this study aimed to assess self-management, self-efficacy, and glycemic control and their relationship in adults with T2DM in the West Bank.
Methods
Design
A cross-sectional descriptive design was used in this study.
Sample and Sampling
This study was conducted in 2025 and took place at the governmental primary health directorate – diabetes clinics in Palestine. A nonprobability convenience sampling approach was used to recruit the study population over a 1.5-month data-collection period. Participants were recruited during their regular visits to the primary health directorate. They were asked to participate after fulfilling the inclusion criteria; patients didn’t receive any compensation to participate in the study. Sample size was calculated using G*Power version 3.1.9.7 with a correlation analysis at a medium effect size (d = 0.30, P = 0.05) and a power of 0.80. The required sample was 82, while in this study, 154 were recruited and agreed to participate.
The inclusion criteria were: Age > 18 and < 70 years, have uncontrolled diabetes, HbA1c > 7, at least six months with a confirmed diagnosis of T2DM and 3 months of treatment, can read and write in Arabic, and free of mental diseases. The inclusion criteria for HbA1c > 7 focused specifically on the suboptimal population of patients with T2DM, as this group has a higher need for educational programs and potential clinical interventions in primary health care centers.
Exclusion criteria were: Type I diabetes, newly diagnosed (less than 6 months), blindness or visual impairment, illiteracy, confirmed mental disease, and physical disability that hinders proper self-management.
Ethical Considerations
The researcher obtained all required Institutional Review Board (IRB) approvals. All participants were asked to sign a consent form; they had the right to withdraw at any time. The researcher answered all questions and inquiries about the study. The study posed no harm to participants, and their rights to privacy and confidentiality were protected by providing a private setting for completing the questionnaire; no names or identifying information were collected or documented.
Data Collection
After obtaining the necessary IRB and facilitation letters, the researcher visited the primary health directorate and informed the directors and staff about the study’s purpose. Patients who met the inclusion criteria and agreed to participate were asked to complete the consent form and questionnaire in a separate room at the diabetes clinic. Laboratory results were obtained from the patient’s files. Data were collected and stored by the primary investigator.
Measurements
A structured questionnaire was used to collect data on participants’ demographic and clinical characteristics. The questionnaire included age, gender, education, income, duration of diabetes, and body mass index (BMI), while recent glycemic control indicators were obtained from participants’ medical records.
In addition, participants’ perceived confidence in performing diabetes-related tasks was evaluated using the Arabic version of the Diabetes Self-Efficacy Scale (ADSES), comprising 8 items and scored on a 10-point Likert scale ranging from 1 (not at all confident) to 10 (totally confident). The total (ADSES) score ranges from 8 to 80, with higher scores indicating higher diabetes self-efficacy. The item-total correlation coefficients were >0.30 for all items, ranging from 0.46 to 0.70. Cronbach’s α coefficient for internal consistency was 0.86, indicating high reliability. Diabetes self-efficacy levels were positively correlated with diabetes self-management skills (r = 0.40, p < 0.001), indicating criterion validity (Kerari, 2023). Furthermore, Adherence to diabetes self-care activities was measured using the Arabic version of the Diabetes Self-Management Questionnaire (A-DSMQ). Cronbach’s α coefficient for internal consistency was 0.76; this tool is a reliable and valid instrument for assessing diabetes self-management (Innab & Kerari, 2024). The tool consists of 16 items assessing four areas (glucose management, dietary control, physical activity, and follow-up appointments) with a total score of 48; each item is rated on a four-point Likert-like scale from 0 (does not apply) to 3 (applies to me very much), giving a total DSMQ score between 0 (minimum) and 48 (maximum). The total sum score was transformed to a 0–10 scale and categorized into three levels of diabetes self-management adherence: perfect (>8), partially adequate (5–8), and inadequate (<5) (Innab & Kerari, 2024).
Data Analysis
The study employed SPSS Version 26 for analysis, ensuring accuracy through data checks and cleaning. Descriptive statistics described participants, while t-tests, ANOVA, and correlations examined differences and relationships. Hierarchical regression analysis was performed to identify significant predictors of HbA1c, self-efficacy, and self-management, with all tests conducted at p < 0.05. Data normality was assessed using skewness and kurtosis, with acceptable values within ±2. Multicollinearity was examined using the variance inflation factor (VIF < 5) and tolerance (>0.2). No violations of statistical assumptions were detected.
Results
Sociodemographic and Health-Related Characteristics of Study Participants
Sociodemographic and Health-Related Characteristics of Participants (N=154)
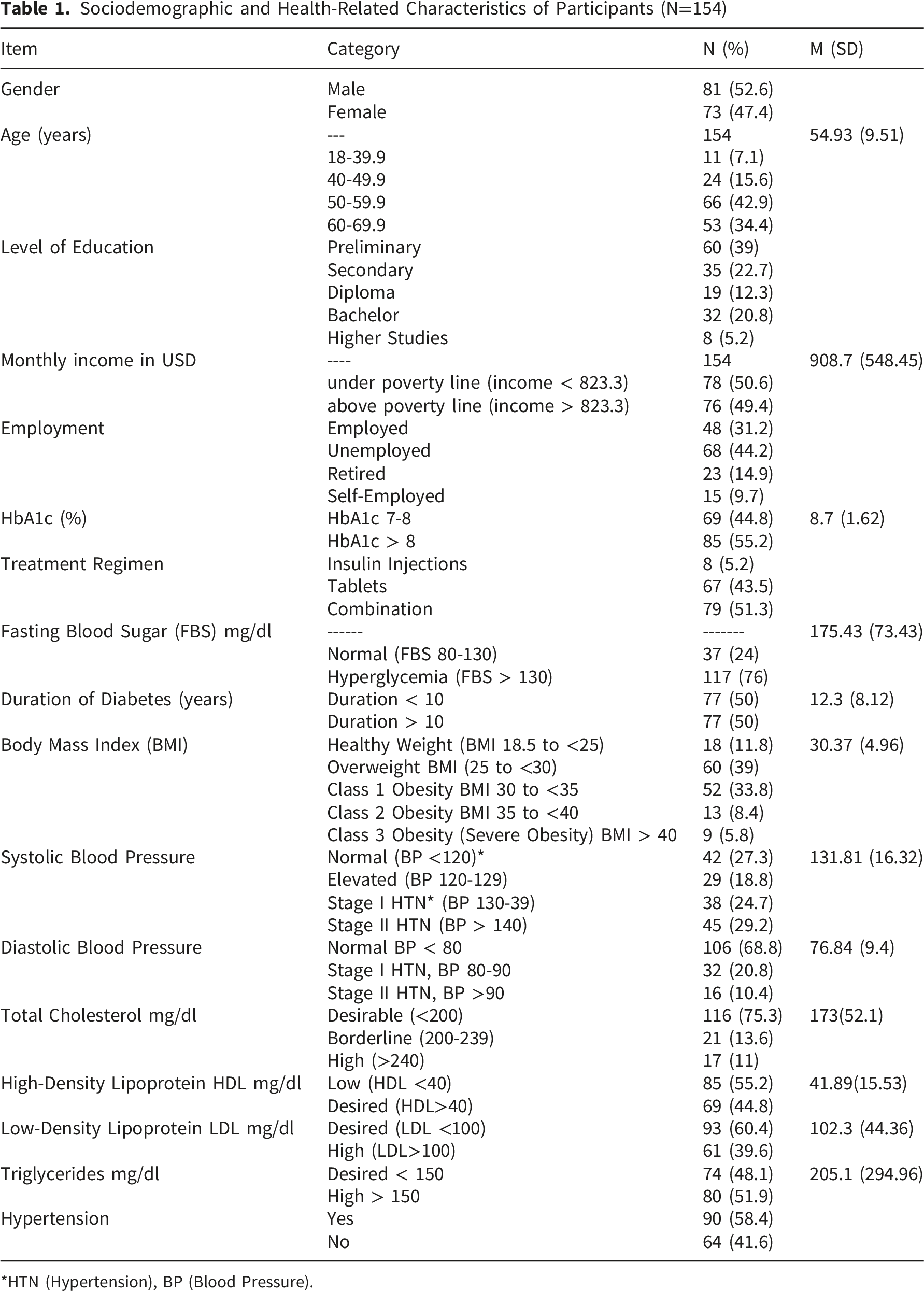
*HTN (Hypertension), BP (Blood Pressure).
Self-Management and Self-Efficacy Among Patients With T2DM
Self-Management and Self-Efficacy Among Patients With T2DM (N= 154)
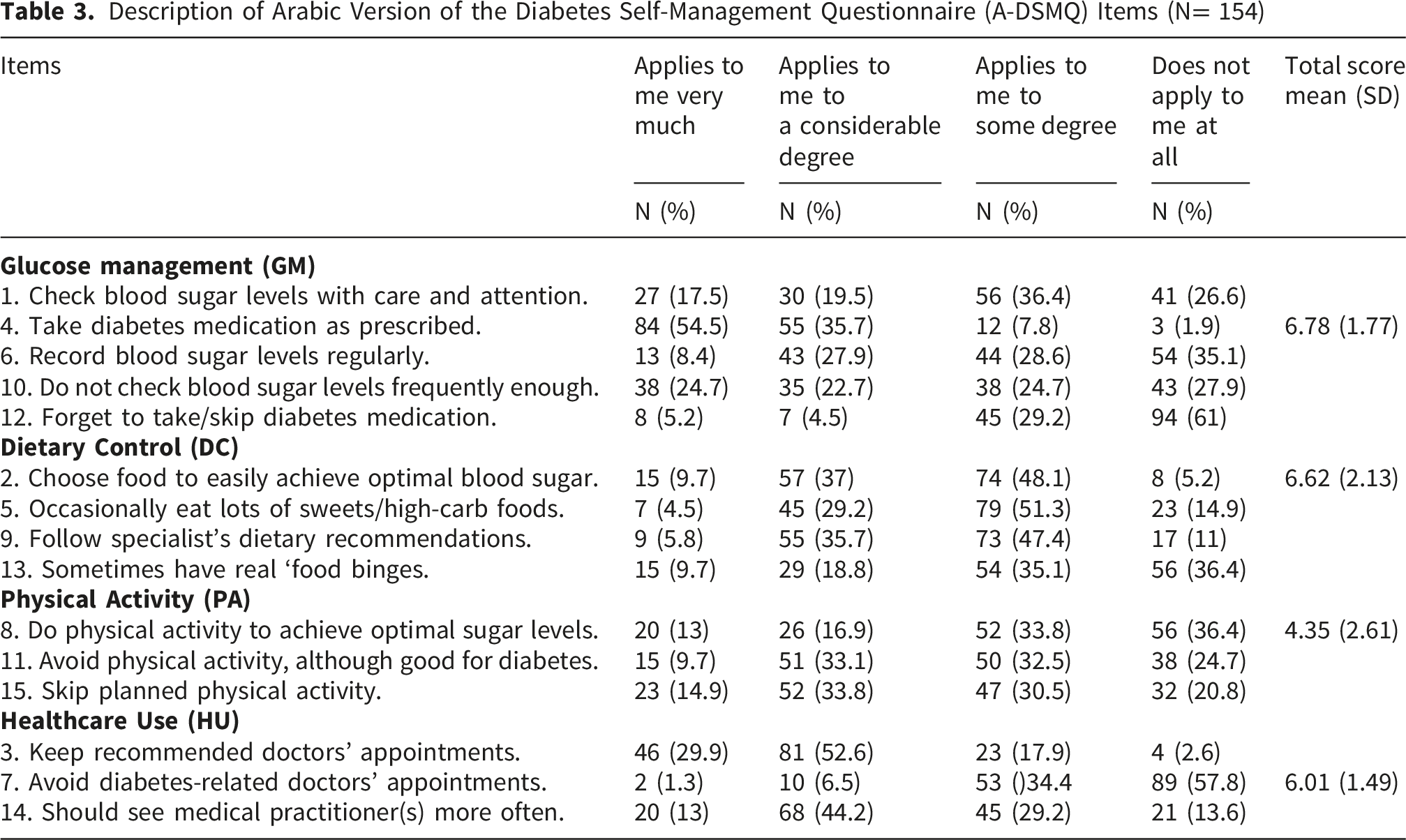
Description of Arabic Version of the Diabetes Self-Management Questionnaire (A-DSMQ) Items (N= 154)
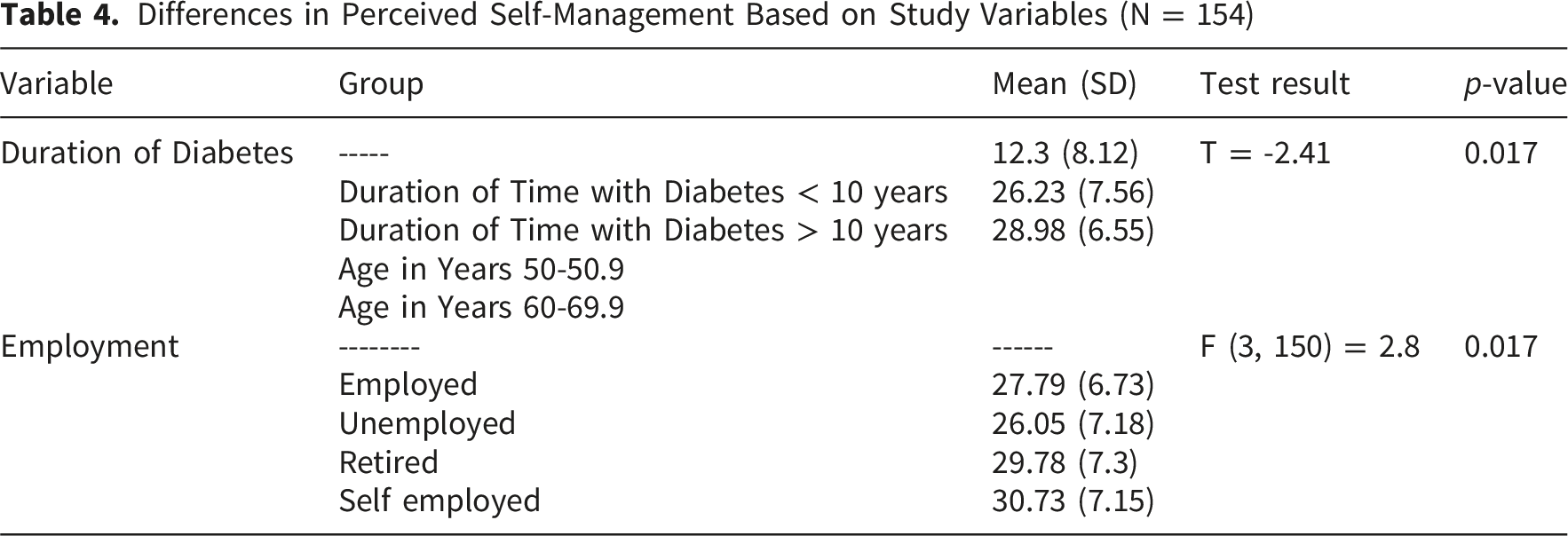
Differences in Self-Management, Self-Efficacy, and Glycemic Control (HbA1c Levels) Among Patients With T2DM
Differences in Perceived Self-Management Based on Study Variables (N = 154)
Differences in Perceived Self-Efficacy Based on Study Variables (N = 154)
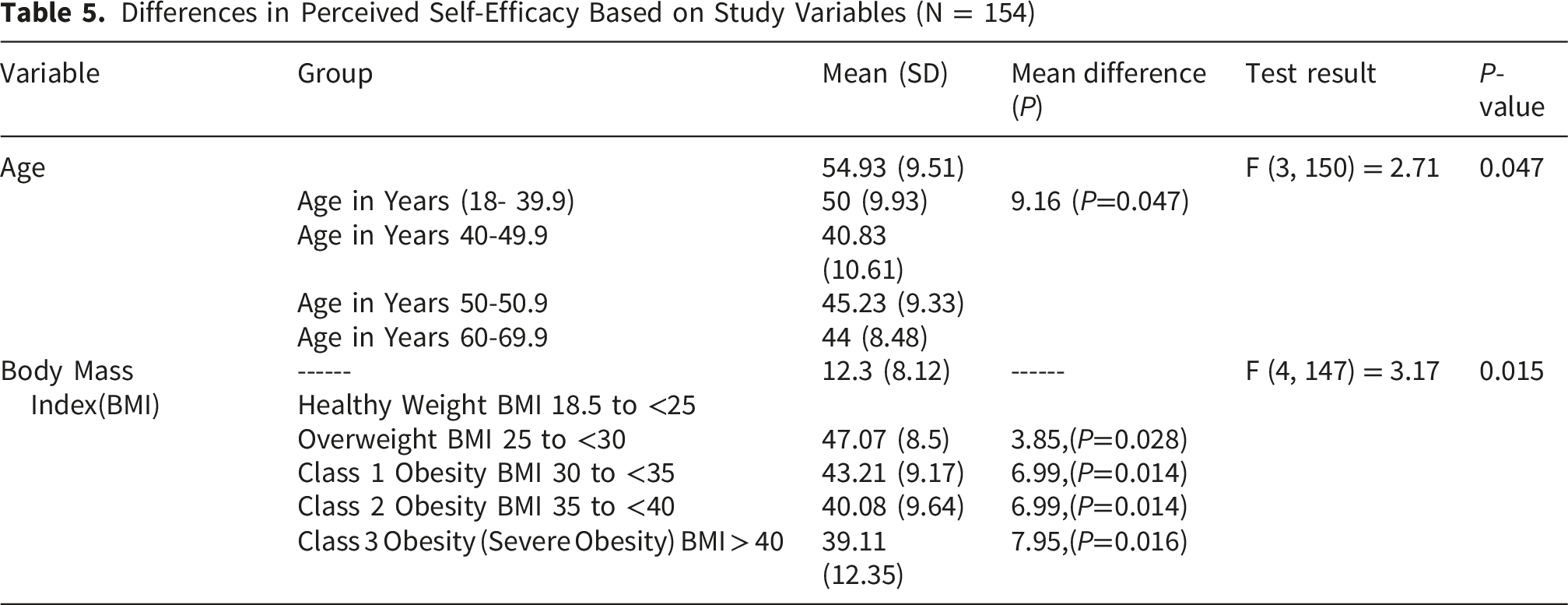
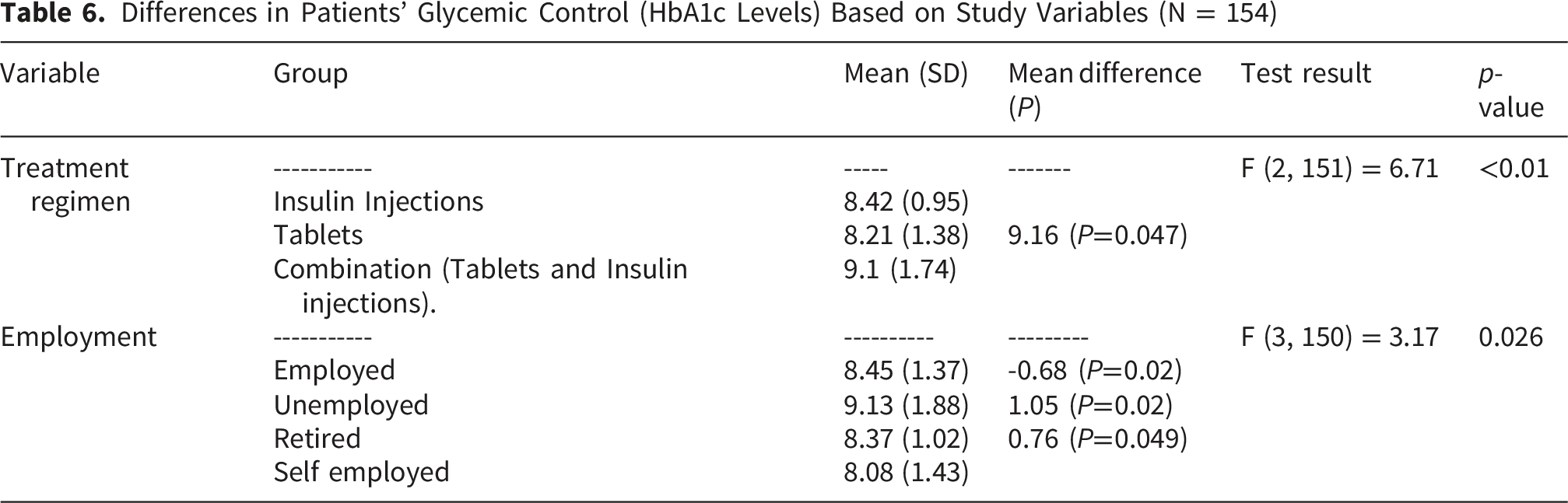
Differences in Patients’ Glycemic Control (HbA1c Levels) Based on Study Variables (N = 154)
Relationships Between Self-Management, Self-Efficacy, Glycemic Control Among Patients and Study Variables With T2DM
Relationships Between Self-Management, Self-Efficacy, Glycemic Control Among Patients and Study Variables With T2DM
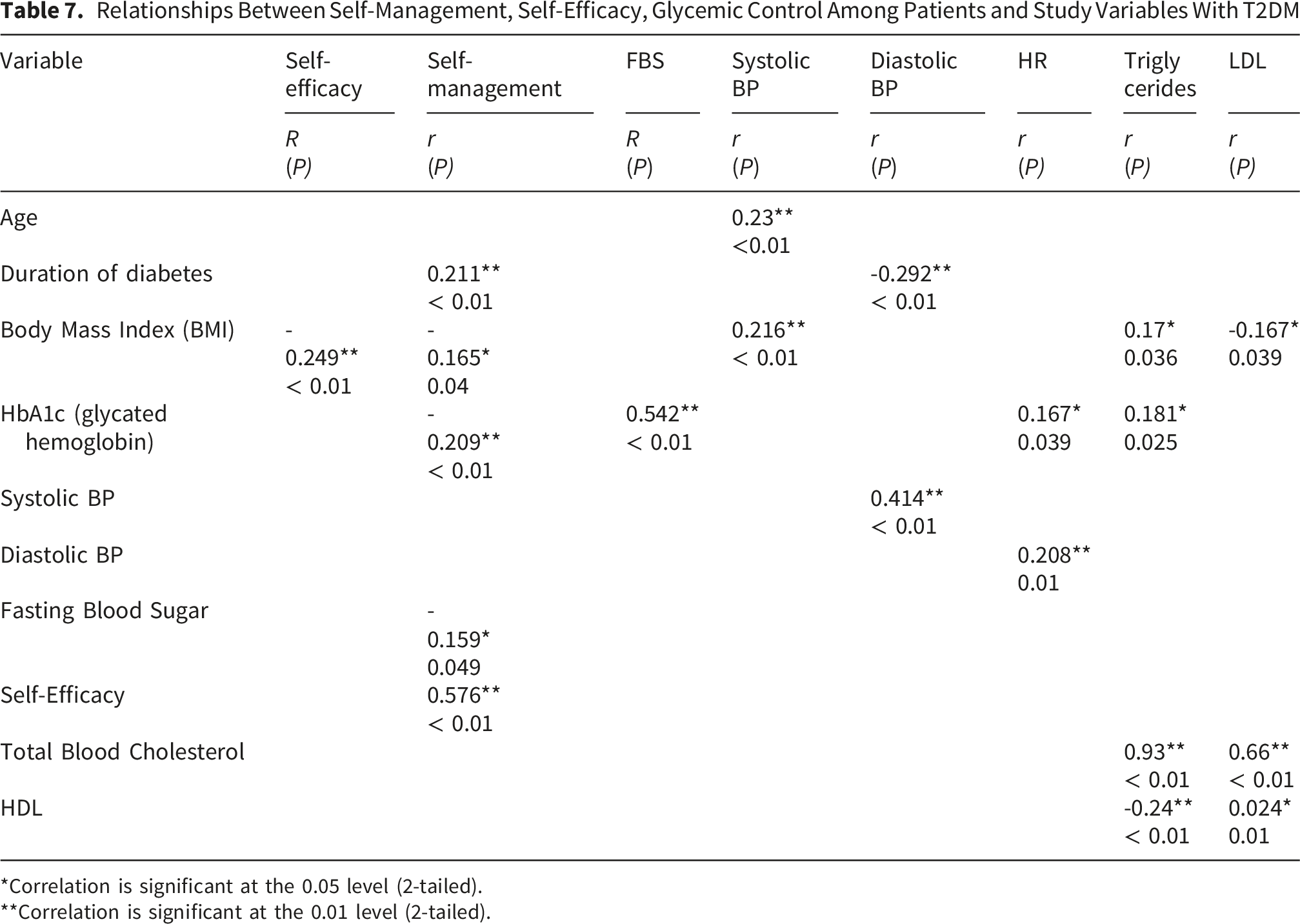
*Correlation is significant at the 0.05 level (2-tailed).
**Correlation is significant at the 0.01 level (2-tailed).
Predictor Variables of Glycemic Control (HbA1c), Self-Efficacy, and Self-Management Among Patients With T2DM
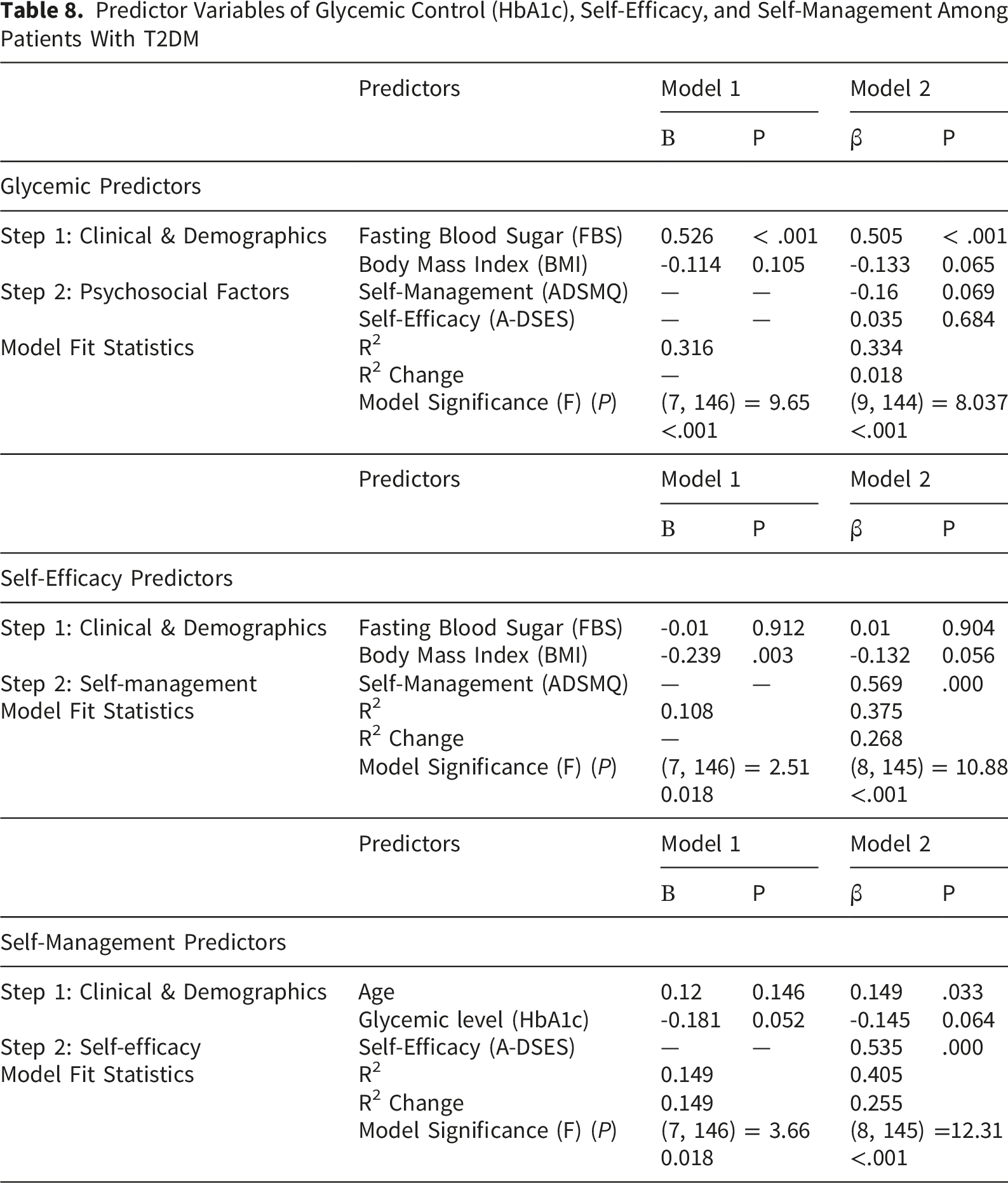
Predictor Variables of Glycemic Control (HbA1c), Self-Efficacy, and Self-Management Among Patients With T2DM
Discussion
This study aimed to assess self-management, perceived self-efficacy in diabetes management, and glycemic control, as well as the relationships among these variables and other study variables. The key findings showed that patients with T2DM in the West Bank have low self-efficacy, poor self-management, and poor glycemic control.
Sociodemographic and Clinical Correlates (Duration, Employment, Age, BMI)
Results of this study revealed that patients with a longer duration of T2DM had a better ability to self-manage their condition; this aligns with Hartuida (2021) in Indonesia, where longer diabetes duration was associated with improved self-management, although that study used a disease-specific self-management scale that emphasized diet and exercise, whereas this study measure also included medication adherence and glucose monitoring (Hartuida, 2021). In contrast, Chen et al. (2022) found no association in a Chinese cohort (M. Chen et al., 2022), which may reflect differences in health system support, cultural self-care norms, or measurement approaches. Patients with longer diabetes duration may have developed greater familiarity with disease-management requirements, contributing to improved adherence to dietary recommendations and medication regimens, according to a study conducted in Palestine. Although that study used different tools to measure self-management, its findings remain relevant given the similar characteristics of participants in the Palestinian context and the larger sample size of 330 participants, which may further support the present study’s results (Mosleh et al., 2017b).
In this study, unemployed patients with T2DM demonstrated poorer glycemic control (higher HbA1c levels) and a lower ability to perform diabetes self-management tasks than self-employed and retired patients, who exhibited lower HbA1c levels. This may be explained by lower income and a poorer economic status, particularly given the challenging economic conditions in Palestine. Nevertheless, unemployed patients with T2DM also reported poorer quality of life. (Eshtaya et al., 2025), Whereas retired and self-employed patients had sufficient income to perform diabetes-related tasks and enhance self-management, unemployed patients demonstrated lower self-management knowledge than employed patients. (Bakkar, 2023). These findings further support the potential role of educational attainment and health literacy in facilitating effective diabetes self-management and glycemic control.
Further findings in this study indicate that younger patients had better diabetes management self-efficacy; in particular, patients aged 18 to 39 years had higher self-efficacy than those aged 40 to 49.9 years. The finding that younger adults reported higher self-efficacy may reflect greater cognitive flexibility, health literacy, and adaptation to digital health resources. This pattern is supported by Ataya et al. (2024) and Zhang et al., although the mechanisms may differ across settings. In older adults, declining physical capacity and treatment fatigue may reduce confidence in managing complex diabetes regimens, which may explain the lower self-efficacy observed.
Nevertheless, age showed a significant association with self-management, with increasing age predicting better self-management. According to the available literature, older adults demonstrate greater adherence to self-management behaviors compared with younger patients with T2DM, despite potential limitations in physical activity. (Cha et al., 2024; Xie et al., 2020). However, age alone is considered a weak predictor of self-management when self-efficacy is included in the model. Self-management tends to improve with increasing age, but it is more strongly associated with higher self-efficacy (T. Yao et al., 2025; Zhang et al., 2023). In addition, younger patients aged 18 to 44 years usually have higher levels of distress and less confidence, which leads to poor adherence and self-management(He et al., 2023). Notably, Ataya et al. (2024) demonstrated this pattern in a Gazan sample using the Diabetes Management Self-Efficacy Scale (DMSES), while Zhang et al. (2023) used a different self-efficacy measure in a Chinese primary-care cohort; this study replication with a West Bank sample and the same DMSES strengthens the cross-cultural signal that self-efficacy declines with age, even when the measurement tool is held constant.
Diabetes self-management and self-efficacy were found to be low among obese patients, especially those who have a BMI > 30, and both tend to decrease as BMI increases. Higher BMI was associated with lower self-efficacy and poorer self-management, possibly because obesity increases physical limitations, dietary burden, and psychological distress, all of which may reduce confidence in sustaining self-care behaviors. This mechanism may explain why similar associations have been observed across both Western and regional populations (Bakkar, 2023; Deng et al., 2025; Eshtaya et al., 2025; Wilson & Patrick, 2012; J. Yao et al., 2019).
Self-Efficacy, Self-Management, and Glycemic Control
This study also found that diabetes management self-efficacy and diabetes self-management were strongly and significantly associated. The strong association between self-efficacy and self-management supports behavioral theory, particularly the Health Belief Model, which positions confidence as a key determinant of health behavior enactment. Unlike purely descriptive studies, the present findings contribute to understanding how psychological confidence translates into practical diabetes care behaviors in resource-limited settings. This finding aligns with similar studies reporting that higher self-efficacy is associated with improved diabetes self-management and better glycemic control (Akio et al., 2023; Amer et al., 2018). Higher self-efficacy also predicted better well-being among patients with T2DM (Calli & Kartal, 2021) and better quality of life (Pahn et al., 2025). Patients with T2DM who received educational programs to improve self-efficacy were better at diabetes self-management (Jiang et al., 2024). In addition, consistent results were found for significant associations between self-efficacy and self-management across different cultural and contextual samples in China and Indonesia (Clara et al., 2021; Fereidooni et al., 2024; Xie et al., 2020).
Moreover, self-efficacy was the only significant predictor of self-management among clinical and demographic variables in this study and accounted for the largest proportion of variance in self-management. Higher confidence and stronger self-efficacy levels can enhance diabetes self-management. Similar findings were reported in an experimental study conducted in 2025, in which self-efficacy predicted self-management behaviors during a longitudinal follow-up at 3, 6, and 12 months after an intervention using a focused educational program to improve self-efficacy among patients with T2DM (Fang et al., 2025). However, Fanger et al.’s study confirms the direction of the relationship and establishes causality, whereas the present study identifies associations only. Another study also reported similar conclusions, indicating that improvements in self-efficacy predict better medication adherence and, consequently, improved glycemic control. (Jiang et al., 2024).
Beyond self-management behaviors, several physiological parameters were examined in relation to HbA1c. Glycemic control (HbA1c levels) showed multiple associations with study variables, where higher heart rate, triglycerides, and fasting blood sugar (FBS) were significantly associated with HbA1c levels. These differences may be attributed to variations in lifestyle and dietary habits. Lipid profile results were unfavorable, characterized by higher triglyceride levels and lower high-density lipoprotein (HDL) levels among patients with poor diabetes management and elevated HbA1c. (Adninta et al., 2022; AlZeer et al., 2025), Conversely, triglycerides and other lipid parameters were reduced in patients who achieved lower HbA1c levels. (Gedikli et al., 2022). In addition, resting heart rate (RHR) was higher in patients with inadequate diabetes management and elevated HbA1c levels (X. Chen et al., 2025). These findings may indicate an elevated risk of future complications and warrant further clinical assessment when accompanied by an unfavorable lipid profile.
Regression analysis indicated that FBS was the only variable that predicted better glycemic outcomes and accounted for a significant proportion of the variance in HbA1c levels. Recent studies conclude a robust connection between Fasting Blood Sugar (FBS), Random Blood Sugar (RBS), and HbA1c, in a study conducted in Libya in 2025, HbA1c level had a significant positive association with FBS and RBS; the regression analysis showed a linear positive relationship, which supports that FBS and RBS can predict future long-term glycemic changes and help in screening and diagnosis of T2DM (Badri, 2025), almost the same supporting findings suggest that FBS and RBS have a significant association with HbA1c without giving a preference to one of them to predict long-term glycemic changes, and showed significant and robust correlation in predicting the changes of glycemic levels (Tao et al., 2023; Vittal et al., 2021; Yuan et al., 2023). Routine monitoring of fasting blood glucose may support day-to-day glycemic assessment and facilitate timely treatment adjustments, thereby improving control and preventing long-term complications. However, Badri (2025) employed the same protocol for fasting glucose results, yet studied a Libyan cohort with a wider glycaemic range (HbA1c 5.0–14.2%); the fact that the linear FBS–HbA1c relationship held across both samples reinforces the utility of FBS as a low-cost monitoring proxy in varied resource-limited settings.
While this study’s regression analysis showed that self-management scores explained a significant portion of the variance in self-efficacy, this finding should be interpreted cautiously within a cross-sectional design. Consistent with Social Cognitive Theory and the wider literature (Bandura, 1997; Jiang et al., 2024; Soola et al., 2022; J. Yao et al., 2019), self-efficacy is theorized to precede and enable self-management behaviors, which usually predict the glycemic level (Amunkete et al., 2025; Nilmart et al., 2025). The strong association observed in this study likely reflects a reciprocal relationship in which successful self-management experiences further reinforce self-efficacy. Future longitudinal research is needed to untangle the directionality.
Systemic and Contextual Barriers in the Palestinian Healthcare Setting
In terms of diabetes treatment regimen, this study showed that the use of oral hypoglycemic agents (“tablets only”) was significantly associated with lower glycemic levels. In contrast, insulin therapy was associated with a greater reduction in HbA1c compared with the oral medication regimen. Insulin is generally considered the most effective treatment for achieving optimal glycemic control, despite its potential side effects, including hypoglycemia and weight gain. (Naeem et al., 2025). In addition, a 2021 study reported that patients with T2DM who used tablets as their only treatment regimen did not show a significant reduction in glycemic levels, with only 11.3% achieving HbA1c < 7%. In contrast, patients who used a combination of oral agents and insulin showed greater improvement, with 45.72% achieving HbA1c < 7% (Paczkowska et al., 2021).
Findings related to the treatment regimen highlight the influence of contextual factors that extend beyond individual behavior. In the Palestinian context, several key variables should be considered when interpreting these results, including medication availability and accessibility, health status, and socioeconomic conditions. Insulin availability is inconsistent due to ongoing conflict and economic constraints, and the Ministry of Health does not consistently provide insulin to patients covered by government health insurance. This may help explain the findings of the present study and underscores the need for future research to incorporate these contextual factors.
Strengths and Limitations
Despite existing constraints and limitations, this study provides important primary data from a large and vulnerable population of Palestinians living under challenging conditions in the West Bank. Both self-reported measures and validated physiological indicators, including fasting blood sugar (FBS) and Hemoglobin A1c (HbA1c) levels, were used, providing more clinically relevant measures than relying solely on self-report. In addition, the high response rate among participants underscores the importance of the topic and the urgent need for research on diabetes management, with an emphasis on feasible, low-cost solutions. The use of multiple statistical approaches (bivariate and multivariate analyses) also strengthened the study by controlling for potential confounders and providing more robust estimates of associations and predictions.
However, since the study used a cross-sectional design, it can only demonstrate associations between self-management, self-efficacy, and glycemic control. It cannot definitively prove that low self-efficacy causes poor self-management, or that poor se
Lf-management causes high HbA1c. Using a convenience sample from one geographical area (Ramallah and Al-Bireh) and targeting patients with HbA1c >7 limits the generalizability of the study findings, especially among patients who achieved optimal HbA1c levels, and limits the range of glycemic variability. Reliance on questionnaires for measuring self-management and self-efficacy introduces the potential for social desirability bias. Nonetheless, the challenges documented (medication unavailability, economic barriers, and high unemployment) mirror conditions in other low-resource, conflict-affected, or humanitarian settings. The findings may therefore be transferable to populations facing similar structural constraints.”
Implications for Nursing Practice
The findings of this study emphasize the pivotal role of nurses in improving diabetes outcomes through interventions that strengthen patients’ self-efficacy and self-management skills. As nurses are often the healthcare professionals with the most sustained contact with patients living with T2DM, they are uniquely positioned to assess behavioral barriers, reinforce self-care practices, and provide ongoing support throughout the disease trajectory.
Nurses working in primary healthcare settings should routinely assess patients’ confidence in performing diabetes-related self-care activities, including blood glucose monitoring, medication administration, dietary management, and physical activity. Incorporating structured self-efficacy assessments into routine diabetes consultations may help identify patients at risk for poor self-management and inadequate glycemic control.
The strong relationship between self-efficacy and self-management observed in this study supports the implementation of nurse-led educational interventions that extend beyond information delivery to include goal-setting, problem-solving training, motivational interviewing, behavioral coaching, and individualized action planning. Such interventions may enhance patients’ confidence in managing their condition and improve adherence to recommended self-care behaviors.
The significant association between BMI and both self-efficacy and self-management highlights the importance of nurses collaborating with multidisciplinary teams to address weight-management challenges through patient-centered counseling, lifestyle modification support, and referral when appropriate.
Given the socioeconomic and healthcare access barriers identified in this population, nurses should also incorporate assessment of social determinants of health into diabetes care planning. Evaluating medication accessibility, financial hardship, transportation difficulties, and continuity of care may enable nurses to develop more realistic and achievable self-management plans.
At the organizational level, nurse managers and advanced practice nurses should advocate for integrating evidence-based diabetes self-management education and support (DSMES) programs into primary healthcare services, particularly for patients with uncontrolled diabetes. These findings support the development of nurse-led chronic disease management programs that prioritize enhancing self-efficacy as a strategy to improve long-term glycemic outcomes.
Conclusions
This study concludes that adults with T2D in the West Bank exhibit suboptimal diabetes self-management and low perceived diabetes self-efficacy, which are strongly and significantly linked to poor glycemic control (high mean HbA1c of 8.7%). The findings suggest that current diabetes management strategies may not adequately address the needs of this population. These outcomes appear to be associated with limited diabetes self-efficacy and suboptimal adherence to self-management behaviors.
Footnotes
Ethical Considerations
The ethical approval was received from the Institutional Review Board (IRB) Committee of Birzeit University (2024). Consent was obtained from the eligible participants after explaining the purpose of the study.
Consent to Participate
Participation in this study was voluntary and informed consent was obtained from all participants before data collection.
Author Contributions
All listed authors meet the authorship criteria and all authors agree with the content of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: funds were received for this study from Birzeit University, Palestine.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.