
Abstract
Introduction:
Although healing abutments are designated for single use by most implant manufacturers, it is common practice for clinicians to reuse healing abutments. However, there is a lack of adequate references that describe detailed sterilization protocols for reuse of healing abutments.
Objectives:
The purpose of this systematic review was to compile, organize, and describe the most common techniques for the sterilization of healing abutments and their efficiency in eliminating traces of microorganisms.
Methods:
An electronic search in 5 different databases was performed, including the National Library of Medicine (MEDLINE via PubMed), Embase, Cochrane Central Register of Controlled Trials, Web of Science, and Google Scholar from January 2000 to December 2020. Search variables included were dental implant, healing abutment, contaminate, contamination, reuse, and sterilization. Studies reporting with a minimum sample size of 10 healing abutments (5 per group) published in the English language were evaluated. Risk of bias assessment was elaborated for included investigations.
Results:
In total, 812 articles were identified, of which 8 were included in the analysis. Steam autoclave was the most widely used form of resterilization. Not a single protocol, however, was able to achieve 100% virgin surface of the healing abutments.
Conclusion:
Although reuse of dental implant healing abutments is a cost-effective measure in dental practice, thorough surface decontamination followed by resterilization is highly recommended before reuse.
Knowledge Transfer Statement:
With consideration of cost and patient preference, results of this review would be useful in knowing various sterilization protocols for reusing healing abutments that could lead to more appropriate therapeutic decisions.
Introduction
Improvement of an ideal implant–gingival environment is achieved by use of healing abutments during second-stage implant surgery. Healing abutments help in creating an adequate emergence profile in the esthetically demanding anterior region. A healing abutment (HA), or a healing screw, is a component that comes in direct contact with tissues to ensure a proper seal between implant and the oral cavity. The purpose of an HA is to maintain patency of the internal threaded section for subsequent attachment of the abutment during the second-stage surgery or until restored (Glossary of Prosthodontic Terms 2017). As per manufacturers’ recommendations, practitioners often advocate the use of new or single-use implant components to prevent cross-contamination among patients due to any residual pathogens or biomass (Vezeau et al. 1996; Vezeau et al. 2000; Dunn 2002; Canullo et al. 2014). However, cost containment seems to be a major deciding factor among clinicians to clean, sterilize, and reuse implant components such as HAs.
Adequate decontamination and resterilization is essential prior to reusing HAs. Resterilization is “the repeated application of a terminal process designed to remove or destroy all viable forms of microbial life, including bacterial spores, to an acceptable sterility assurance level” (Dunn 2002). Reusing HAs results in surface alterations, biological contamination, and higher corrosion rate, which can contribute to dental implant complications such as perimplantitis (Jain et al. 2021). The feasibility of reusing dental components with stringent sterilization protocols, however, has shown promising results in the past decade (Canullo et al. 2014; Stacchi et al. 2018; Sánchez-Garcés et al. 2019; Kyaw et al. 2020).
There is lack of data discussing sterilization protocols and the practicality for reusing HAs. To our knowledge, there is no single report in the literature reviewing the status of reuse of HAs per se. The aim of this systematic review was to systematically compile and evaluate various contemporary cleaning and sterilization protocols for reused HAs in the past decade.
Materials and Methods
This study followed the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) protocol (Shamseer et al. 2015) (PROSPERO registration number: CRD42020135873).
Focus Question
What is the effectiveness of various sterilization procedures to achieve complete surface decontamination on reused healing abutments for second-stage implant surgery?
Inclusion Criteria (PICOS)
Population: Reused HAs required for second-stage implant surgery
Interventions: Various surface cleaning/decontamination methods, such as mechanical cleaning, ultrasonic cleaning, alcohol, detergent, or any other methods of disinfection, and various surface treatment/sterilization methods, such as steam autoclaving, plasma of argon, ethylene dioxide, laser irradiation, ultraviolet sterilization, air particle abrasion, or any other methods of sterilization
Comparisons: A control group with new/unused HAs versus test groups with reused HAs
Outcomes: Primary outcome was clean surface/absence of residue of the HA after treatment process, and secondary outcome was functional integrity of the HA surface after various resterilization protocols such as presence of scratches or signs of corrosion.
Study design: Studies with a minimum sample size of 10 reused HAs (5 per experimental group) done in human subjects from January 2010 to December 2020 to include contemporary protocols in the past decade
Exclusion Criteria
Case reports, case series, technical notes, letters to editor, or personal communications
Articles in language other than English
Studies lacking information on type of sterilization treatment done
Studies including other possibly reusable implant components such as cover screws, impression copings, and so on
Review articles and meta-analyses
Animal studies
Abstracts/posters published after conferences
Search Strategies
Five electronic databases were used as sources in the search for studies satisfying the inclusion criteria: the National Library of Medicine (MEDLINE via PubMed), Embase, Cochrane Central Register of Controlled Trials, Web of Science, and Google Scholar. These databases were searched for studies published from January 2010 to December 2020. This was to restrict the search to contemporary sterilization regimens for resterilizing HAs. The following keywords and Boolean operators were used in the search strategy: dental implant, healing abutment, contaminate, contamination, reuse, sterilization; AND, OR.
The search was restricted to humans and English-language articles. Manual search of journals was done including the Journal of Prosthetic Dentistry, International Journal of Oral and Maxillofacial Implants, and International Journal of Prosthodontics.
First, studies that met exclusion criteria were eliminated by title. Second, screening of abstracts pertaining to inclusion criteria was performed. Finally, full-text versions of selected articles were collected to confirm the eligibility based on the inclusion and exclusion criteria. In addition, cross-references were also obtained wherever necessary.
Data Extraction
Full-text manuscripts of all included studies were read independently and discussed by the authors. Disagreements were resolved by discussion. Data extraction was performed by taking into account factors that could introduce bias to the results. To assess the methodologic quality of the included studies, Cochrane Collaboration recommendations were used (Higgins et al. 2019), mentioned in Table 1. The potential risk of bias was categorized as “low,” “unclear,” or “high” depending on the quality and detailed explanation of provided information.
Risk-of-Bias Assessment.
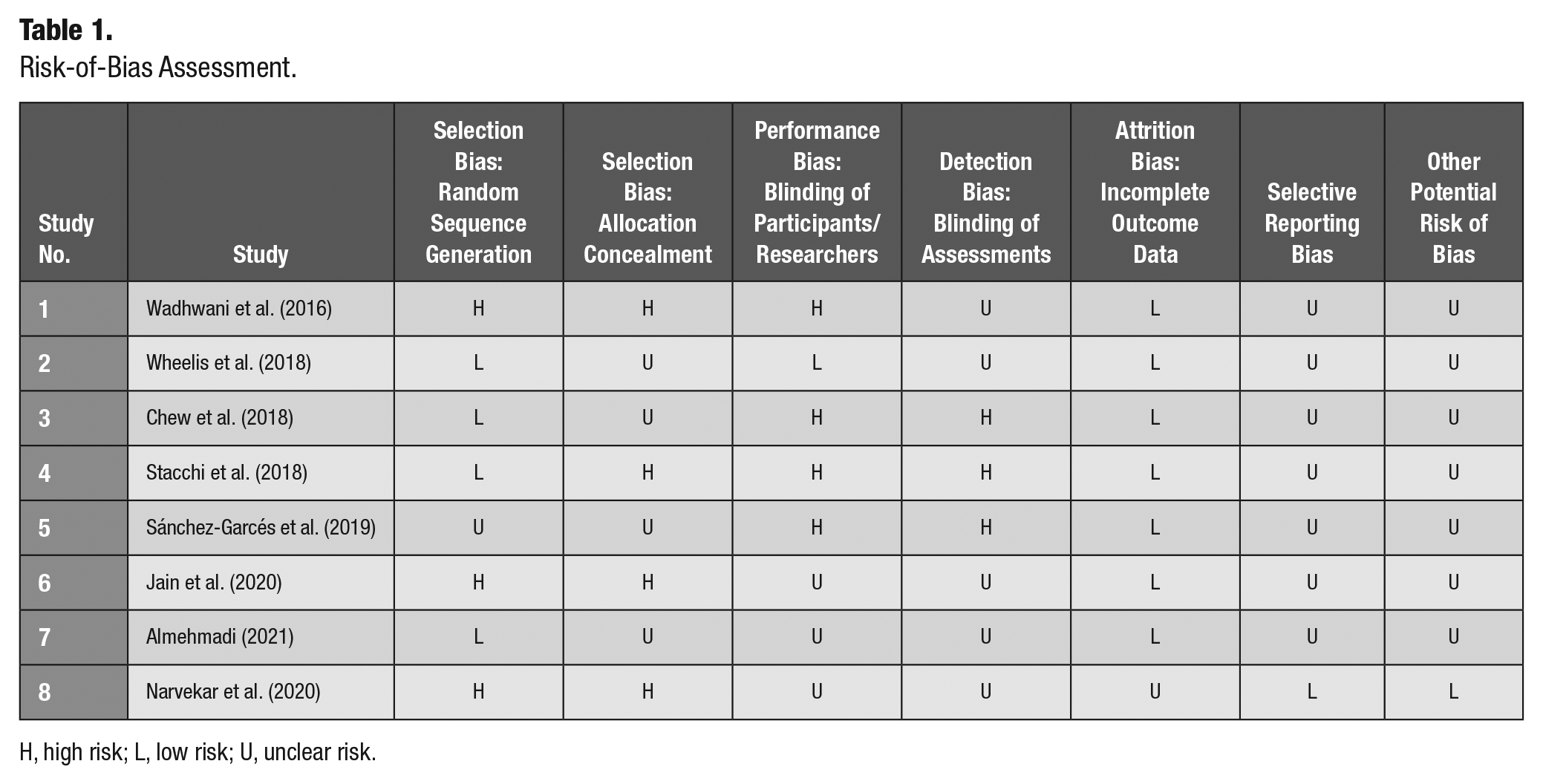
H, high risk; L, low risk; U, unclear risk.
Results
Selection of Articles
The National Library of Medicine (MEDLINE via PubMed), Embase, Cochrane Central Register of Controlled Trials, Web of Science, and Google Scholar resulted in 56, 0, 13, 0, and 740 papers, respectively. Three articles were obtained through hand searching. Deduplication of data was done by exporting selected articles to Mendeley Reference Manager (version 1.19.4). Out of 812 articles, after elimination of articles by title/abstract, 20 articles were selected for full-text reading. Fourteen articles were provisionally selected, of which 8 articles fulfilled the inclusion criteria (Wadhwani et al. 2016; Wheelis et al. 2018; Chew et al. 2018; Stacchi et al. 2018; Sánchez-Garcés et al. 2019; Jain et al. 2020; Almehmadi 2021; Narvekar et al. 2020), and 6 were excluded (Vezeau et al. 2000; Browne et al. 2012; Cakan et al. 2015; Kyaw et al. 2020; Barreiros et al. 2021; Jain et al. 2021). The PRISMA flowchart depicting the search strategy and characteristics of included and excluded articles is described in Figure 1 and Table 2, respectively.
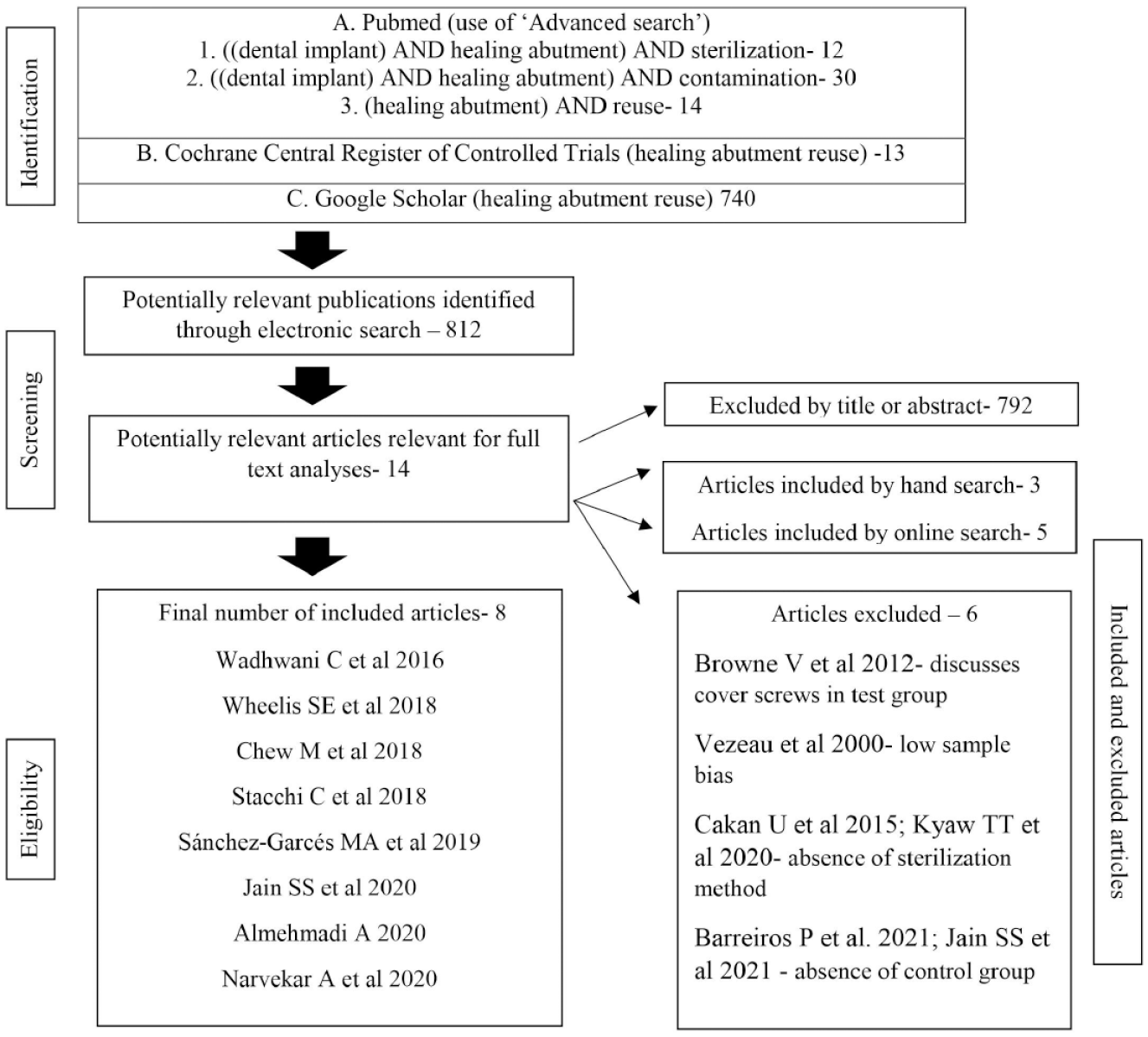
Characteristics of search process and search strategy: Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) flowchart.
Methodological Characteristics of Included Studies.
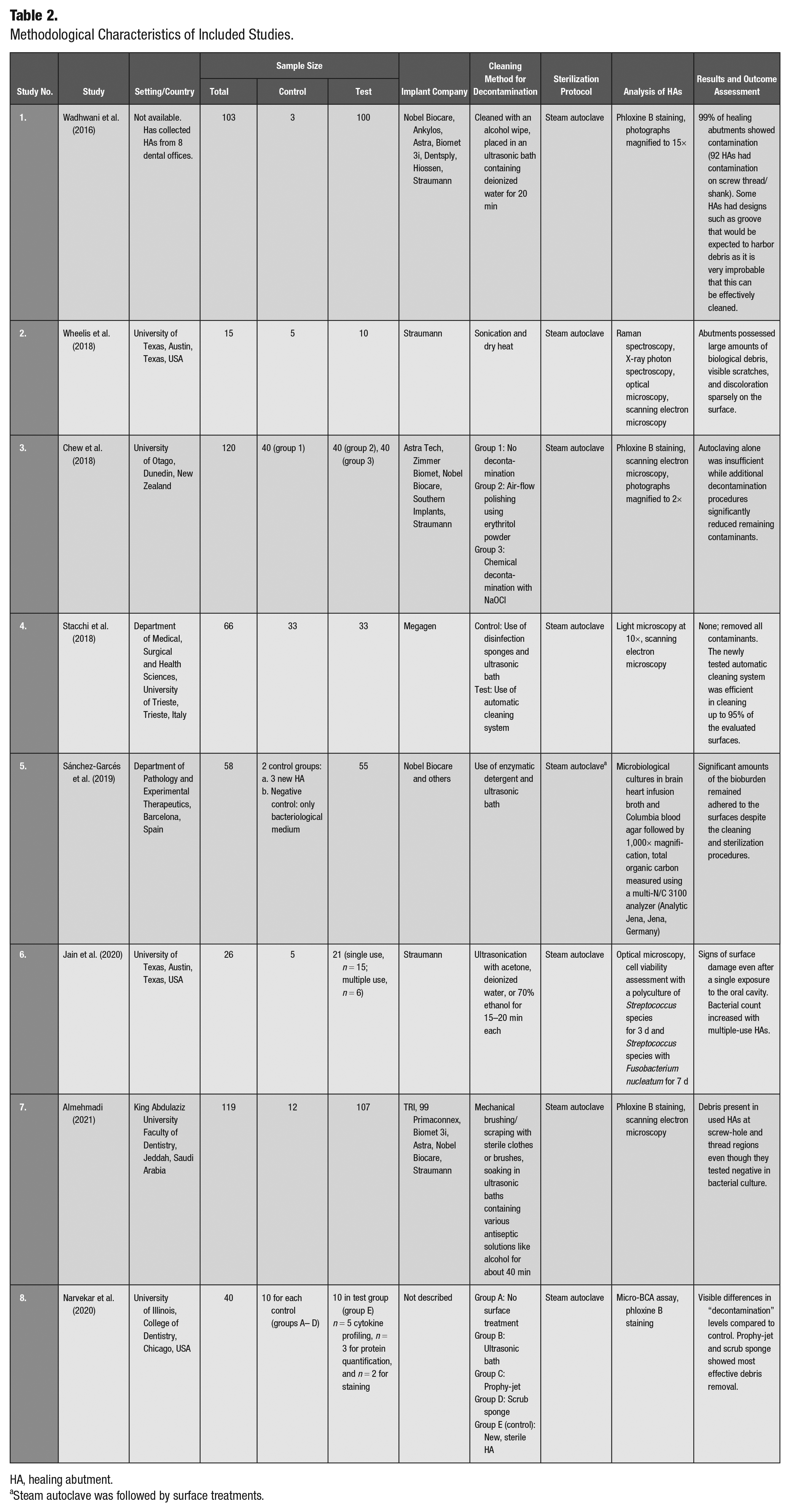
HA, healing abutment.
Steam autoclave was followed by surface treatments.
Discussion
HAs play a pivotal role in sculpting the peri-implant tissues during the critical healing phase of dental implant restorative therapy (Wadhwani et al. 2016). During prosthetic procedures, the pristine surface of HA is altered, and bioburden may get an accumulated surface that deleteriously influences the inflammatory response of the peri-implant tissues (Canullo et al. 2014). This makes manufacturers promote “single-use only” HAs, which may also be to boost their market sale (Wadhwani et al. 2016). However, in developing countries, HAs are reused following rigorous cleaning and sterilizing protocols to offer cost-effective implant treatments to patients (Browne et al. 2012). Unfortunately, failure to adhere to a scrupulous and/or appropriate regimen of debridement and sterilization may not only lead to transmission of contagion among patients but also cause structural deterioration of the component, eventually contributing to implant failure.
It was noted that there was heterogeneity between articles that prevented a quantitative synthesis of data, and hence a meta-analysis was ruled out. Instead, a qualitative descriptive systematic review was performed, and results were represented in the forms of tables. This review has included ex vivo–in vitro studies wherein used healing abutments from patients were tested. No randomized controlled trials (RCTs) were found in the literature search. The included studies compared resterilization protocols followed by clinicians to reproduce a near-virgin implant surface. Not a single protocol has been able to achieve a 100% virgin surface of the healing abutments.
Literature suggests various methods of sterilization such as steam or chemical autoclave and use of ultraviolet light or ethylene oxide (Vezeau et al. 1996; Vezeau et al. 2000; Browne et al. 2012). However, it has been documented that neither of these methods can completely re-create the virgin surface of the abutment and negatively alters the composition of the titanium surface (Wadhwani et al. 2016). The changes in the topography of HA affect the wettability, which further interferes with the ability of the epithelium and fibroblast cells to attach and spread on the implant surface (Canullo et al. 2014).
In one of the first publications examining the feasibility of sterilizing implant HAs and impression copings, used components showed sterility equal to new components without any visible distortion (Browne et al. 2012). The specimens were tested after contamination with Enterococcus faecalis using either steam autoclave or chemiclave, and none of the specimens were tested positive after sterilization.
In a study evaluating 100 commercially available HAs, 99% of them were found to have some form of residual contamination (Almehmadi 2021). Another study evaluated a newly tested system that included ultrasonic soaking, tumbling by rotating metal pins, and ion pasteurization (Dunn 2002). It was noted that the new tested device efficiently cleaned more than 95% of the evaluated surfaces. Fifty-seven used HAs were examined in a study of which 10.5% had dirty screw grooves and 5.2% had partially filled driver slots. Penicillium variabile as well as E. faecalis and Enterococcus faecium were detected on 3 abutments in 1 group and on 1 abutment in each of the 2 groups, respectively. Presence of calculus was also seen on the lateral surface of HAs. However, in the same study, it was observed that one of the manufacturer’s HAs was clean, and the procedure can be predictable if a proper protocol is followed (Cakan et al. 2015). Er:YAG laser irradiation is also effective in debriding titanium surfaces of HAs, when used at the output energy of a 50-mJ/pulse and 30 Hz with water cooling. Plasma of argon has been shown to enhance cell adhesion to used titanium HAs (Matsuyama et al. 2003). Pyrex test tubes have been suggested as a multiple-use sterilization vehicle for reusable dental materials (Cain et al. 2000). These tubes are reusable in contrast to the single-use sterilization envelopes.
Use of air-particle abrasion with erythritol powder and use of NaOCl before autoclaving have been found to effective alternate methods of decontamination, strengthening the feasibility of reusing HAs (Chew et al. 2018). Use of NaOCl especially provided encouraging results with regard to decontamination and hydrolyzing the biofilm formation on used HAs. Sterilization regimens can affect cell attachment of subgingival connective tissue (Vezeau et al. 2000). It was reported that autoclaving reduced cell attachment, whereas use of ultraviolet light resulted in a favorable cell attachment. Plasma cleaning done before ultraviolet light treatment can enhance the surface energy of the HAs. However, it did not affect cell attachment and spreading.
Evidence shows that reuse of HAs may serve as a potentially costly risk for the clinician. It has been reported that the design of the screw thread poses difficulty in the cleaning process (Bousquet et al. 2014). Ultrasonic baths and sterilization using steam autoclaving are unable to eliminate tightly packed debris (Wadhwani et al. 2016; Wheelis 2018; Chew et al. 2018; Stacchi et al. 2018; Sánchez-Garcés et al. 2019). Mechanical cleaning using air particle abrasion can structurally damage the healing abutment as well as result in metal contamination due to abrasive impregnation (Wadhwani et al. 2016). Contamination of the screw threads with biological debris is a common finding, which can further lead to various complications. “Locking” of HAs onto the implant can occur due to contamination, and any attempt to unscrew the HA can result in reverse-torquing of implant out of the bone (Wadhwani et al. 2016). Repeated use of HAs results in wearing of the screw thread, which can further cause damage to the abutment/implant connection and thus reduce the sealing capacity of the component due to abrasive impregnation (Darvell et al. 1995; Vezeau et al. 1996; Ntrouka et al. 2011). Clogging of the screwdriver insertion site with debris can result in improper engaging of the HAs with the screwdriver, eventually leading to mechanical failure. The presence of biological debris has been demonstrated even after cleaning and sterilization using steam autoclaving of used HAs (Wheelis 2018).
Not just HAs but also other potentially reusable implant components such as cover screws and impression copings have been studied regarding their influence of reuse on clinical outcome. In a light microscopic pilot study, contaminated titanium abutment cylinders were ultrasonically cleaned with ethanol and inserted in the abdominal walls of rats (Sennerby and Lekholm 1993).
Morphological analysis showed an increase in macrophages and reduction of fibroblasts irrespective of cleaning procedure. The effect of reusing cover screws for dental implants in patients and clinical outcome was examined, and it was found that surface chemistry was virtually unchanged and cover screws can be cleaned and reused without any apparent adverse effect on clinical outcome (Schwartz et al. 2000). The effect of multiple use of impression copings on the accuracy of direct and indirect implant transfer techniques has been assessed, and it was concluded that impression copings can be successfully used, cleaned, and sterilized up to 10 times without compromising the impression accuracy (Alikhasi et al. 2013). There were similar results with use of 10 times resterilized implant impression copings (Aldosari 2014).
Reused HAs exhibited signs of mechanical damage even after single use (Jain et al. 2020; Barreiros et al. 2021; Jain et al. 2021). As decontaminated HA abutments have increased surface energy, reusing not only promotes surface degradation but also stimulates deposition of organic products that may be quite tedious to remove (Souza et al. 2010; Wadhwani et al. 2016; Noronha Oliveira et al. 2018). Although only 30% of the tested HAs in a study showed bacterial presence, the remaining HAs had a strong adherence of biomass (Barreiros et al. 2021). Similarly, another study showed presence of no bacterial or fungal contamination on treatment with NaOCl followed by steam autoclaving, but debris was observed in scanning electron microscopy images in some regions of the thread regions primarily attributed to ledge design (Almehmadi 2021).
Use of traditional methods of sterilization has been found to cause surface alterations such as an increase in titanium oxide layer thickness (Baier et al. 1982; Lausmaa et al. 1985; Stanford et al. 1994; Wälivaara et al. 1994; Schwartz et al. 2000). Glow discharge has been proposed as an alternative means for the sterilization of medical devices. It has demonstrated the thinnest titanium oxide layer and the cleanest surface (Youngblood and Ong 2003; Wheelis 2018).
It is worthwhile to note that no single protocol reviewed could achieve complete sterilization, but this does not translate to an unacceptable decontamination protocol. Also, only 1 of the included studies noted the number of times HAs have been reused (Jain et al. 2020). Failure to note it can jeopardize the clinical outcome. The ability to reuse HAs could save a substantial amount of money for both the clinician and patient, which can vary depending on the manufacturer’s price, as well as the number of times components will be used or reused per implant placed. Clinical outcome with regard to reusability of other implant components such as cover screws and impression copings has also been studied with inconclusive results (Alikhasi et al. 2013; Aldosari 2014; Bidra et al. 2020). It is ironic that manufacturers’ have labeled implant drills as “reusable” while healing abutments are onetime use (Sirona Implants 2017; Narvekar et al. 2020). In an evidence-based profession where the practice of sterilizing and reusing these implant components is becoming common in clinical practice, research to verify the safety and validity of this practice is necessary. Although not ideal, studies show promising results with respect to achieving decontamination in used healing abutments (Stacchi et al. 2018; Sánchez-Garcés et al. 2019; Almehmadi 2021; Kyaw et al. 2020; Sahin and Dere 2021). However, the authors recommend further research including RCTs to establish standard protocols in achieving complete resterilization of used HAs. The effectiveness of sterilization on customized, lab-contaminated titanium abutments was beyond the scope of this review and hence not evaluated.
The trend in developing nations of reusing titanium healing abutments for environmental and economic benefits should certainly not hinder implant survival rate and pose a risk of cross-infection among patients. Even though there is no reporting of any contamination or failed implant owing reused HAs, some practitioners do believe that manufacturers label these devices for single use to maintain their profit margin. It is the need of the hour for the clinicians to establish comprehensive resterilization protocols to ensure no damage to mechanical properties as well as to achieve complete surface decontamination of the reused HAs.
Conclusion
Based on the current systematic review, it was noted that steam autoclaving was used as the sterilization technique in all the included studies. The authors recommend that after thorough disinfection by surface decontamination techniques such as mechanical/ultrasonic cleaning or use of chemical disinfectants, non–surface-altering sterilization techniques such as steam autoclaving must be used prior to reusing implant components such as HA. It is also a prime requisite that clinicians note the number of times the HA has been reused and resterilized. Contrary to the popular belief that healing abutments may be reused multiple times, such practice needs to be done with caution until supported by further evidence. We advocate that newer clinical trials regarding practicability and ethics of reusing healing abutments need to conducted to establish a better scientific inference.
Author Contributions
P. Eswaramurthy, contributed to conception, design, and data acquisition, drafted and critically revised the manuscript; M. Aras, K.M. DSouza, A. Nagarsekar, R.B. Gaunkar, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.