
Abstract
Background:
Improving shared decision making (SDM) training curricula may support wider training uptake and the use of SDM across health care settings. Limited uptake of a freely available SDM training curriculum suggested it could benefit from a systematic review and revision process. This report describes the process and revisions of the SHARE Approach curriculum, subsequently used in an implementation trial demonstrating that the revised curriculum remained effective.
Methods:
A qualitative study using a systematic review on shared decision making, training, and physicians published between 2015 and 2020; clinician and patient reviews and feedback on curriculum training materials; and synthesis of recommended improvements and a team-revised curriculum for testing in clinical practice.
Results:
Recommendations from the literature and reviewers (9 clinicians and 6 patients) focused on substantially reducing the length of the training curriculum, ideally under 4 h. Reviewers found original content well done and important but suggested removing content that was not explicitly focused on training clinicians how to implement shared decision making in clinical practice by removing discussions of applicable laws, medical interpreters, and patient-centered outcomes research while retaining important strategies for addressing patient health literacy/numeracy and use of decision aids.
Limitations:
Clinician and patient feedback might not represent the full scope of clinical specialties or patient types who may have different recommendations for revising the original curriculum for other clinical settings.
Conclusion:
Literature review and user feedback agreed that training curricula on shared decision making needed to be shorter and focus on only essential techniques clinicians need to effectively implement shared decision making in routine practice.
Implications:
A substantially shortened SHARE Approach curriculum is effective and may facilitate broader shared decision making training of clinicians.
Keywords
Highlights
The original SHARE Approach curriculum incorporated techniques common to SDM training that are associated with measurable improvements.
Clinicians and patients agreed that the SHARE Approach curriculum included useful and important training information but was too long for implementation in busy clinical settings and included portions that were more academic and less practical.
Based on similar recommendations from the literature and clinician/patient reviewers, the SHARE Approach curriculum was reduced from 5 training modules to 3 training modules while retaining essential, effective, and practically relevant content.
Introduction
Shared decision making (SDM) involves communication between clinicians and patients to make health care decisions that are consistent with patients’ values, preferences, and life circumstances.1,2 SDM is increasingly included in clinical care guidelines and in some cases is mandated by payers. 3 Despite interest in improving the use of SDM across health care settings, less is known about how to effectively implement SDM in diverse practice settings. 4 SDM is not often conducted effectively in practice,5 –7 and identifying ways to improve SDM has become an imperative. 8 A lack of clinician support and education has been identified as an important barrier to SDM. 9
The SHARE Approach model was developed in 2014 to teach clinicians steps for conducting SDM, including those applicable to the context of preference-sensitive treatment choice and problem solving, based on Makoul and Clayman’s 10 systematic review. The original design of the SHARE Approach used a train-the-trainer model and included approximately 8 h of didactic workshop learning across 4 modules (plus an introductory module and a trainer’s guide) interspersed with group discussion, videos, role-play activities, 9 topic-specific supporting tools, and patient-oriented materials.11,12 Although adopted and used successfully to obtain specific clinical goals (eg, increased breastfeeding rates) in one health system,13,14 the SHARE Approach has not yet been systematically implemented and evaluated in the diverse clinic and patient populations where it was intended to be used. In 2019, the Agency for Healthcare Research and Quality (AHRQ) contracted with the University of Colorado to revise the SHARE Approach and test its use in clinical practice. This report describes 1) recommended revisions to the SHARE Approach using findings from a literature review and patient/clinician feedback, 2) the revision process, and 3) revisions to the SHARE Approach training curriculum and tools that were then used in a hybrid type 2 implementation-effectiveness study.
Methods
Prior to testing the SHARE Approach curriculum in a hybrid type 2 implementation-effectiveness study in practices, 15 a literature review was conducted and patient and clinician input was sought to determine if there were important updates or recommended improvements to make the SHARE Approach materials. The literature review and user input were conducted independently but were used together by the study team when revising the curriculum through multiple iterations.
A systematic review was conducted by a medical librarian supported by 2 members of our research team for relevant articles on SDM, training, and physicians, published between 2015 and 2020. Covidence systematic review software (Veritas Health Innovation) was used for screening and full-text review. Of 1,148 potentially relevant articles, 2 members of the research team (C.K. and L.D.S.) scanned all abstracts and excluded articles that clearly did not address or describe an SDM training intervention for practicing clinicians, leaving 34 articles for full review. (The Appendix contains details of the literature review scope and process.)
The review of the SHARE Approach materials was based on human-centered design principles (International Organization for Standardization [ISO], 2019) to identify potential changes to the SHARE Approach. Feedback was sought from clinicians and patients during March and April of 2020, just as the COVID-19 pandemic was emerging in the United States. All clinician and patient reviewers provided feedback and recommendations in structured written review forms with prompts, followed by one-on-one interviews for further clarification and feedback. The forms and interviews asked about the SHARE curriculum content, sequencing, tools, Web site, and resources. Clinicians were also asked about the overall feasibility of implementing the tools in their clinical practice and for any recommendations for improvements in situations that involve problem solving with patients. The review materials described the purpose of the curriculum and the intents and purposes of how their reviews would be used and contribute to the revisions of the curriculum. Interviews were conducted and analyzed by one of the authors (D.H.F.), a masters-level trained qualitative researcher at the University of Colorado Department of Family Medicine with more than 28 y of experience in qualitative and multimethod research and evaluation.
Nine primary care and specialty practice clinicians with and without prior SHARE Approach experience were invited to review SHARE Approach materials, including the 5 training module slide sets, 9 supporting tools, the training video, and other documents (Table 1). Clinicians were purposively identified from existing professional research contacts from the evaluation team and were invited by e-mail and telephone to participate. A single follow-up interview (D.H.F.) was conducted to clarify summary notes and recommendations. The review and follow-up telephone interview were estimated to take between 3 and 4 h. Participating clinicians were offered a $100 gift card for their time.
SHARE Approach Materials and Topics Reviewed by Clinicians and Patients.
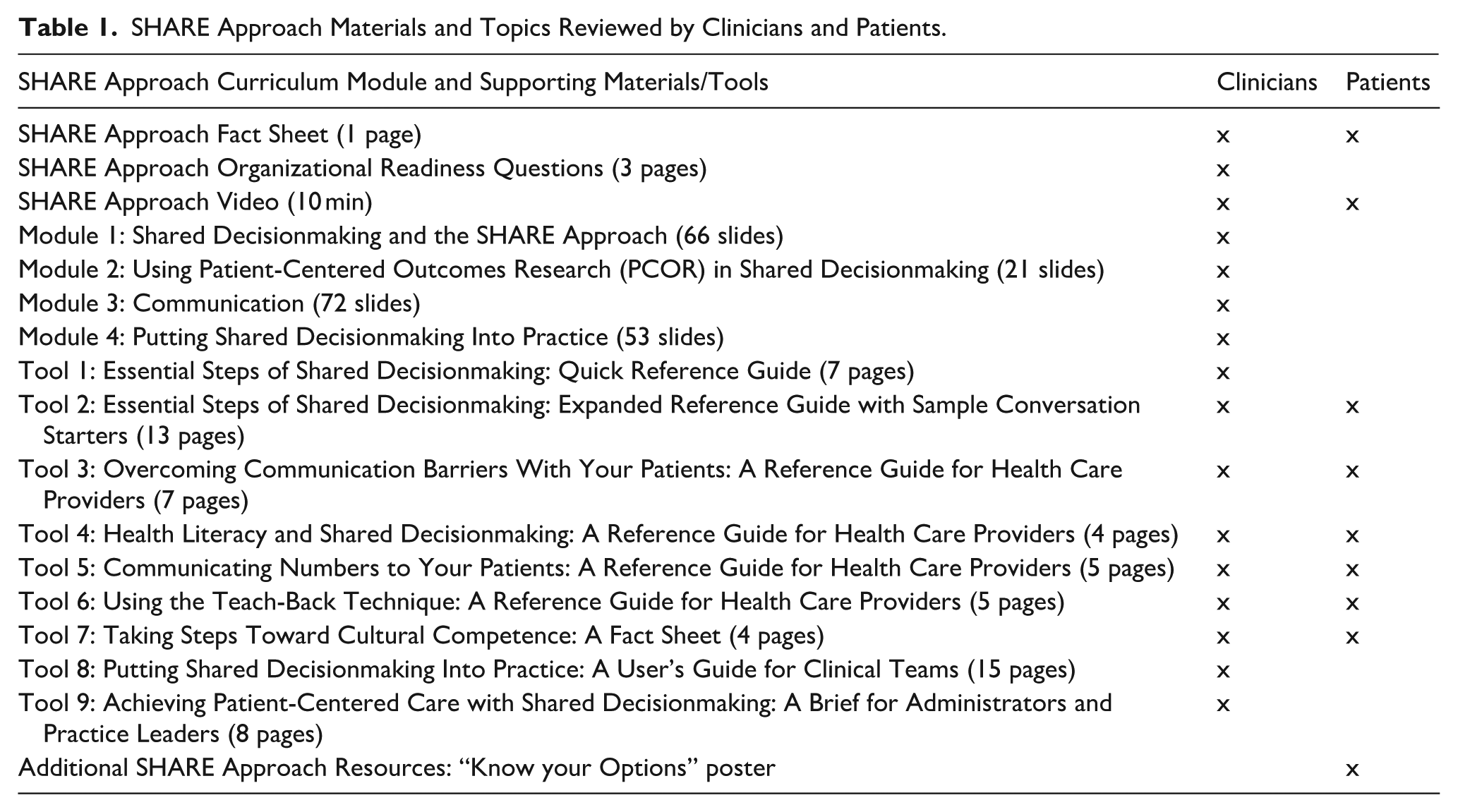
Similarly, we purposively invited patients by e-mail who were members of local community and patient advisory groups with experience in reviewing clinical guidelines, patient-facing resources, research protocols, and research results to review the curriculum materials. 16 Seven patients were asked to review 6 of the same supporting tools from the SHARE Approach curriculum that clinicians reviewed, plus the SHARE Approach video, the SHARE Approach Fact Sheet, and patient-facing exam room poster (Table 1). Patients completed structured review forms with prompts, plus a single follow-up telephone interview, but with different prompts and questions to focus on patient perspectives, reactions, and recommendations for improving training materials for clinicians. Participating patients were offered a $100 gift card for their time. All interview data were audio-recorded and transcribed for analysis. Handwritten notes from interviews were completed during the interview by DF.
Qualitative data analysis of review documents, commented PDF files, and interview transcript documents proceeded through several iterations using a grounded theory approach called immersion-crystallization.17,18 A grounded theory approach allows findings to emerge inductively from the data review and analysis process. Immersion-crystallization analysis uses iterative, recursive, careful, and probing reading of the data until analytical saturation finds no new “significant insights, patterns, or interpretations emerge from the data.” 17 Emergent findings and themes were documented in case notes and further reviewed, returning to the data to read, reflect, and refine findings. Immersion-crystallization does not require specialized software, although data were organized in ATLASti qualitative data analysis software for managing and reviewing data. Case-based, role-ordered (physicians vs patients) matrices were then developed to represent the data in general categories that aligned with each curriculum video, tools, and modules reviewed by participants to organize the findings for later application to content revisions.17,19 Matrices summarized for each case the key findings, themes within categorical domains, and brief quotations. The matrix of key themes—including summarized primary recommendations for curriculum revisions—were shared with the other co-authors (L.D.S., C.K., D.D.M., and D.H.F.) for review, comments, and questions. The primary analyst (D.H.F.) returned to the data to respond to requests for clarification from co-authors before finalizing the matrix of recommendations that—combined with the literature review results—guided the curriculum revision process conducted by co-authors (L.S., C.K., D.D.M., and D.H.F.).
This study was preliminary evaluation work leading to the protocols reviewed and approved by the Colorado Multiple Institutional Review Board (COMIRB). COMIRB approved all aspects of the study, including the methods presented herein for which informed consent was not required. Informed consent was required for the formal experimental research portion of the study (Scherer 2025). Names and other identifiers were removed from the analytical datasets after initial data collection and were not shared beyond the research team.
Results
Literature Review
Three principal findings from the full review of 34 articles suggested strategies for where to focus revisions of the SHARE Approach curriculum. First, it appeared to be common to deliver an SDM training in 4 h or less. Given this observation (in addition to clinician/patient feedback, described next), we believed that it should be feasible to reduce the SHARE Approach trainings to a 3- to 4-h workshop. Second, the SHARE Approach already incorporated a didactic overview of SDM and video learning, which were commonly used in SDM trainings and associated with measurable improvements in SDM-concordant clinician behavior.
Third, role-play was a very common educational approach. The first edition of the SHARE Approach incorporated role-play; however, with a shift away from a train-the-trainer model, challenges included how to make role-play meaningful to different medical specialties without reducing the generalizability of the SHARE Approach or increasing the complexity of its implementation.
Another common approach highlighted in the literature was group discussions about the barriers, challenges, and facilitators of SDM. This type of discussion could be added as a formal part of the SHARE Approach materials and would be feasible to deliver in a webinar format. This type of discussion is thought to be positively received by clinicians because it acknowledges perceived difficulties of delivering SDM—including both logistic barriers such as time necessary to conduct SDM and interpersonal challenges in engaging patients in conversations about difficult topics—and addresses those difficulties by providing mutual support and feedback. This type of discussion would also be naturally tailored to the clinical context. A similar type of activity encourages participants to reflect on their experiences with SDM and their daily practice and behaviors, which may help to provide clinicians with greater insight into their personal use of SDM (or lack thereof).
Other methods observed in the literature, such as audit and feedback and incorporation of standardized patients or actors, appeared impractical for the SHARE Approach, given the level of investment (time and money) that these approaches require.
Clinician and Patient Feedback
A total of 9 clinicians provided feedback. Five primary care clinicians and 3 specialty clinicians from cardiology who did not have experience with the SHARE Approach reviewed SHARE materials. One primary care clinician with SHARE Approach experience also reviewed materials. Clinician participants were all male and were from smaller independent primary care practices, a large academic health system, and 2 other large health system practices all in the Denver metropolitan area of Colorado. Six patients (of the 7 invited to participate) reviewed SHARE materials and provided feedback. Patients included 1 male and 5 female respondents from the Denver metropolitan area and from rural eastern and western Colorado. Follow-up interviews for all respondents ranged from 30 min to 65 min.
Overall, clinicians and patients agreed that the entirety of the SHARE Approach curriculum included useful and important training information but was too long for implementation in busy clinical settings. The main recommendations for improvements to the slides and tools fell into 4 broad categories: (1) rearranging content, (2) deleting or trimming content, (3) rewording or reworking content to emphasize key points in a shorter training, and (4) adding new content.
Rearranging essential content of the slides reflected comments from multiple reviewers that many of the points appearing in later parts of the training made a strong case for the importance of SDM and should be presented earlier.
Deleting or trimming content was recommended to reduce the number of slides and overall content redundancy. Where content coverage is shortened, an accompanying tool could be referred to for additional guidance and support. For example, while the conversation starters may be useful as a starting point for new clinicians, covering all of them in the training is not needed. A single conversation starter could be presented and discussed, and then trainees could be referred to the tools for more ideas if needed. An important message that patients and physicians communicated was that the conversation should be authentic and not “canned” or “robotic.” Another example noted by several reviewers was that while physicians—especially physician researchers—thought information about patient-centered outcomes research was interesting material and relevant to SDM, this content could be reduced to a few slides instead of a stand-alone module.
Rewording or reworking content should emphasize key points in a shorter training to highlight information patient and physician reviewers agreed was important but may not be adequately addressed in the slide content. For example, clinicians’ opinions differed regarding role-playing, some favoring and some strongly disliking. One consultant physician suggested relabeling role-play activities as “practice,” having participants rehearse what they would say in different SDM situations. There were also several comments from physicians and patients about offering guidance on finding decision aids and “building a library” of decision aids for common conditions in which SDM is often needed but was not explicitly included in the materials.
New content reflects essential updates from the literature review or where multiple reviewers highlighted new points to emphasize in SDM. For example, several patients and physicians talked about the importance of preparing the patient for SDM during an office visit. A slide could be added with ideas for how different roles in the clinic can be part of a workflow, such as providing materials to patients or explaining what the visit will be about before meeting with a provider. To improve the usefulness of the curriculum to help with problem solving with patients, adding an example of a complex patient case may help. For example, demonstrating how a clinician and patient work together to reach a treatment decision by talking through comorbidities that may need to be managed differently or discussing patient fears or concerns associated with one treatment option versus another.
Curriculum Revisions
The project team reviewed and prioritized revision recommendations that emerged from the literature review and clinician/patient reviews, aiming to streamline and improve the curriculum for wider adoption. An iterative team process yielded a revised SHARE curriculum that was used in the later implementation trial (Scherer 2025). These were the primary revisions: reduce content to 3 training modules that would introduce the SHARE steps, focus training and practice on each step, improve communication with patients and families, and incorporate decision aids into practice.
The original curriculum consisted of 5 modules, including a training module based on a train-the-trainer approach. After reviewer input recommending cuts and based on the results of the literature suggesting a substantially shorter time commitment for training, the content was reduced to 3 modules, including dropping the trainer’s module (as SHARE would no longer be implemented using a train-the-trainer model; Figure 1). Because there was no concrete guidance for how a trainer (in a train-the-trainer model) would train clinicians in any practice interested in the training, we designed the revisions and trial to ensure that clinicians at each practice all had an opportunity to receive the training. Reductions in content were possible by removing content that reviewers thought was not essential to training others to implement SDM in a clinical setting.
“Module 1: Shared Decision Making and the SHARE Approach” provided a good overview of the 5 steps and was reduced from 66 slides to 41 slides, by removing excessive background references and by weaving important content on training practice members into each step of the SHARE Approach process (eg, including others on your team or connecting example conversation starters with specific steps), rather than a separate slides or content unconnected directly to training on a particular step. Although clinician reviewers were divided on role-play as a learning method, based on the literature review results, the role-play activity was retained in the SHARE Approach curriculum revisions but updated to work for practices in different medical specialties. Specifically, the revised role-play activity asked clinicians to pair off, with one clinician playing a patient based on their clinical experiences and having a medical circumstance that required SDM (examples were provided for guidance). The other clinician played the role of the attending, with instructions to engage the SHARE Approach steps with some minimal knowledge of the patient’s characteristics.
“Module 2: Using Patient-Centered Outcomes Research (PCOR) in Shared Decision Making” was considered heavy on text, lacked concrete examples, and focused too much on details about patient-centered outcomes research, which was noted as “intellectually interesting” but not immediately relevant to teaching practicing clinicians how to implement shared decision making. Therefore, this module was dropped from the training.
“Module 3: Communication” content was found to be important, but reviewers thought there were too many slides, some of which could be removed, such as discussions around law (which clinicians should know) and using interpreters (which clinicians should have experience with). By retaining content focused narrowly on training clinicians on improving communication with specific strategies and by moving decision aid content to its own module, content was reduced from 72 slides to 44 slides. Multiple clinicians requested more information and training on finding and using decision aids, especially for conditions that are common in their specialty. Therefore, a new module was developed with some content from the original Module 3 while adding additional training on when and how decision aids can be most effectively used in practice.
“Module 4: Putting Shared Decision Making into Practice” contained a few slides that were important for “making the case” for organizations to use shared decision making, but most of the content was not considered critical for training by our reviewers. Module 1 already included important information about the “why” of shared decision making, and so Module 4 was dropped.
“Module 5: Trainer’s Module” was dropped since a train-the-trainer approach was deemed impracticable for widespread training adoption.

SHARE curriculum module content changes based on clinician/patient feedback.
Discussion
Based on an updated literature review and clinician/patient reviews and feedback, the overall length of the SHARE Approach training modules was reduced substantially while retaining essential training content and focusing on key points that improve SDM at each SHARE step, including techniques to improve communication and to integrate decision aids.
Interactive teaching of SDM has been shown to be effective, 20 and to overcome SDM barriers and improve uptake, health care providers recommend creating a socially supportive environment through team-based approaches to SDM training and implementation.21,22 The revisions to the SHARE modules can still be implemented in an interactive, team training setting while reducing the time burdens required in the original SHARE approach training materials, which may improve training uptake. Results from the hybrid type 2 implementation-effectiveness trial using the revised curriculum demonstrated that the revised training curriculum remained effective. 15 A curriculum revision process including literature review and user input may be practical for examining and revising other curricula that aim to train clinicians in busy clinical settings.
Clinician reviewers requested more information and training on finding and using decision aids. Patient decision aids improve knowledge, satisfaction, and patient/provider communication; increase patient involvement in decision making; and reduce patient decisional conflict and regret. 23 Yet, barriers to the adoption of patient decision aids persist in clinical practice. Explicitly focusing on patient decision aids in a new curriculum module addressed an important issue from the clinician reviewers and may help to train clinicians to incorporate patient decision aids more effectively.
Although clinician and patient feedback was included, it might not represent the full scope of clinical specialties or patient types who may have different recommendations for revising the original curriculum for more practicable implementation for training in other clinical settings. The number of clinicians (8) and patients (6) who reviewed the materials and were interviewed was likely too few to reach thematic saturation. 24 The revised curriculum was not directly compared with other techniques or other SDM training curricula, although the literature review included results from other relevant clinician trainings.
Conclusion
The literature review and clinician/patient reviews generally agreed that training curricula on SDM need to be shorter (up to 4 h) and focus on only essential steps and techniques clinicians need to know (and practice) to effectively implement SDM in routine practice. A substantially shortened SHARE Approach curriculum that still retains essential content may be suitable for training without a more resource-intensive train-the-trainer approach and may facilitate the use of the curriculum.
Supplemental Material
sj-docx-1-mpp-10.1177_23814683261457450 – Supplemental material for Revising a Training Curriculum on Shared Decision Making for Application in Routine Clinical Care: A Report on the SHARE Approach
Supplemental material, sj-docx-1-mpp-10.1177_23814683261457450 for Revising a Training Curriculum on Shared Decision Making for Application in Routine Clinical Care: A Report on the SHARE Approach by Douglas H. Fernald, Daniel D. Matlock, Christopher E. Knoepke, W. Perry Dickinson, R. Mark Gritz and Laura D. Scherer in MDM Policy & Practice
Footnotes
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Daniel Matlock and Laura Scherer are members of the editorial board of MDM Policy and Practice. The authors declare no additional potential conflicts of interest with respect to the research, authorship, and/or publication of this article. The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided entirely by the Agency for Healthcare Research and Quality (contract No. HHSP233201500025I 75P00120F37005). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethical Considerations
This study was preliminary evaluation work leading to the protocols reviewed and approved by the Colorado Multiple Institutional Review Board (COMIRB). COMIRB approved all aspects of the study, including the methods presented herein for which informed consent was not required. Informed consent was required for the formal experimental research portion of the study, reported elsewhere.
Patient Consent
Not applicable. Patients in this work were not research subjects.
Data Availability
The data used for the literature review are fully described in the Supplementary File and are derived from publicly available sources. Qualitative data are not available due to privacy protections. Sharing these qualitative data could easily identify participants who did not provide permission to share their data beyond the research team.
Supplemental Material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.