
Abstract
Keywords
Shared decision making (SDM) is a collaborative process between patients and providers, where health care decisions are made together based on scientific evidence and patient values and preferences. 1 Studies show that the development and distribution of decision aids (DAs) can facilitate SDM.2-9 Distributing DAs and using SDM increases patient knowledge, improves satisfaction with care,10-13 helps patients receive care aligned with their personal values,14-16 and often results in patients choosing less-invasive treatment options.10, 12, 17-19 DAs are also a key method for translating comparative effectiveness research (CER) results into information patients can understand. 20
Despite evidence as to the benefits of SDM and DAs, spreading their use to everyday clinical practice is challenging. A systematic review by Elwyn and others 21 identified barriers to DA distribution and implementation, including: 1) a lack of provider confidence in DA content, 2) competing demands and time pressure, and 3) concerns about patient reactions to DAs. In two surveys exploring physicians’ and nurses’ attitudes toward specific DAs, most clinicians expressed interest in using the DAs but less than half acted on that interest.22, 23 Overall, the literature suggests that provider attitudes and behavior can pose major barriers to DA delivery and SDM adoption.21,24,25 However, few reports have examined how the attitudes of providers with hands-on experience distributing DAs differ across specialties or change over time. Indeed, Elwyn and others 21 call for a more in-depth exploration of provider perspectives.
We previously reported the successful implementation of a large-scale, systems-level approach to distributing patient DAs for 12 preference-sensitive conditions at Group Health, an integrated delivery system in Washington State.18, 26 Our evaluation revealed commonly reported barriers to DA distribution and increasing SDM 26 conversations, such as time constraints and a lack of applicability to a clinical situation or patient characteristics.27-30 Unique key barriers were providers’ perceptions of the condition or treatment decisions as life threatening, and difficulties in identifying the optimal timing to deliver some DAs to patients.26, 31
This paper extends our previous work to address three major gaps in the literature: 1) limited data from providers who participated in successful, long-term DA and SDM projects, 2) few studies comparing the attitudes of providers in different specialties within the same organization, and 3) limited data examining changes over time in provider attitudes to DA use and SDM. We use the conceptual model of the stages of communication by Halley and others 20 that is needed to support patient-centered care to broadly consider our findings in the context of the fields of CER, SDM and patient-centered care. Table 1 summarizes the stages and future research priorities from Halley and others. 20
Conceptual Model of Comparative Effectiveness Research (CER) Communication a
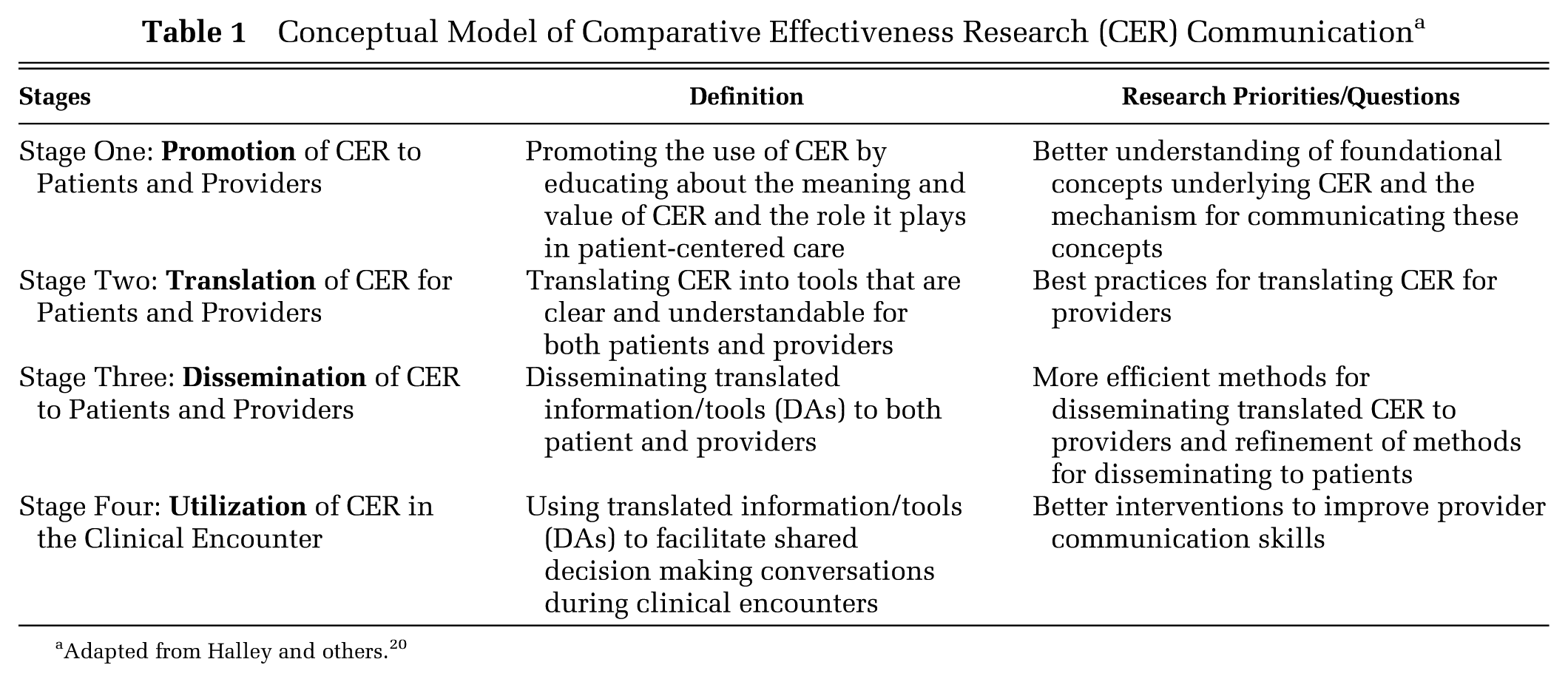
Adapted from Halley and others. 20
Methods
This study was part of a larger Group Health Research Institute implementation and evaluation project18,26,32 that evaluated the effect of DA distribution on health care utilization and care costs for preference-sensitive conditions related to elective surgery. The evaluation captured qualitative information on the implementation process in six specialties and in-depth provider reactions to the project in two specialties. In addition to the implementation processes, the data documented the attitudes, reactions and experiences of frontline providers who distributed the DAs and engaged in SDM with patients.
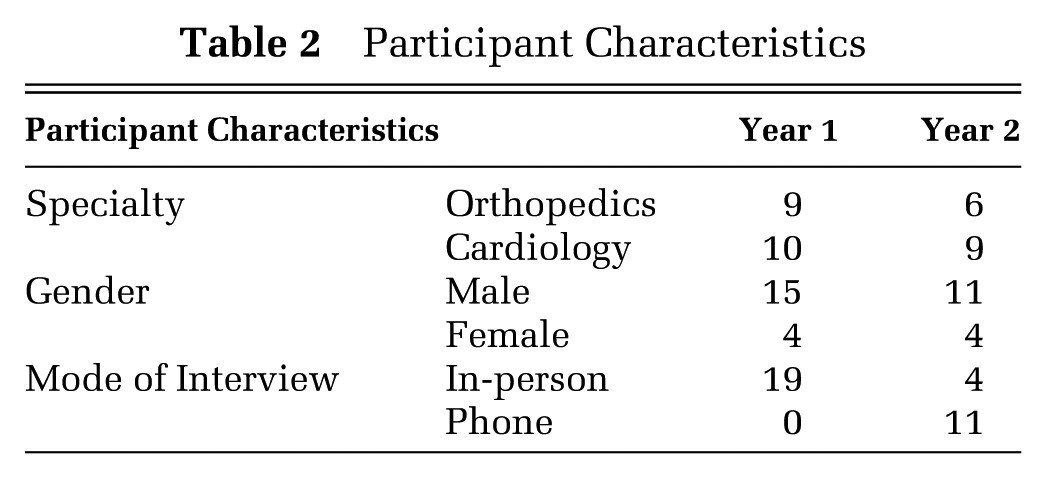
In-depth provider interviews were conducted with 19 orthopedic and cardiology providers; 15 were available for the one-year follow-up interviews (Table 2). These specialties were chosen because the implementation team observed that they represented opposite ends of the spectrum of provider receptivity to the DAs and logistical ease in integrating DAs and SDM into clinical practice during project planning. Receptivity and logistical ease of integration was generally high for orthopedics and low for cardiology. Providers were salaried employees of Group Health without financial incentives that might impact DA and SDM use. However, the organization expressed strong support for DA distribution and SDM over a timeframe that covered the interviews.
Participant Characteristics
The orthopedics service line implemented two DAs: 1) “Treatment Choices for Knee Osteoarthritis”; and 2) “Treatment Choices for Hip Osteoarthritis.” Cardiology implemented the DA “Treatment Choices for Coronary Artery Disease.”33,34 DAs were a video with an accompanying booklet. DA content was developed by the Informed Medical Decision Foundation and Health Dialog.33,35
Providers were defined as physicians and physician assistants. Inclusion criteria required that the provider: 1) planned to actively see patients over the study period (no planned leaves or retirements), and 2) treated patients with the conditions targeted by the DAs. Email invitations were sent to 29 orthopedics and 20 cardiology providers who volunteered by email response. Information from two orthopedics providers indicated they did not meet inclusion criteria. In-person interviews were conducted during the first year of DA implementation, with in-person or phone follow-up interviews approximately one year later. Eleven follow-up interviews were by phone and four were in person.
We used a semi-structured interview guide (Appendix) with slight modifications for follow-up interviews. Key questions focused on providers’ views of the patient’s role in decision making, approaches to patient decision making before the DA implementation project, reactions to DA content, descriptions of DA workflow/processes in their clinic, and perceived effect of the DAs on care. Audio-recorded interviews were conducted by the qualitative evaluation lead (CH) and a research assistant. A professional transcriptionist generated near-verbatim transcripts.
Using a thematic approach to coding,36,37 we developed a preliminary list of codes based on the evaluation questions and interview guides. The code list was added to and refined through an iterative, inductive process of reading transcripts, identifying more specific and emergent codes and developing clear definitions for each code. Two study team members (CH and DL) read and coded transcripts, then compared coding. Coding and reconciling was repeated until both coders used the codes consistently about three-quarters of the time (assessed informally by tracking the number of coding differences that required reconciliation). Agreement was considered an indicator of shared interpretation of code definitions and a test of conceptual validity between the codes and the text. One team member (DL) then completed all coding with consultation and input from the second coder. The final codebook consisted of 168 codes, many focused on input on process issues. Analysis was by the lead author (CH), with additional consolidation and code refinement. Coded data were grouped by code, specialty and interview year. Data were reviewed again to assess frequency of comments, nuances and details of responses and to look for overarching differences and similarities between specialties and response year. A coding memo was generated from this process, reviewed by the primary coder (DL) and the project team, and was the basis for the manuscript. We mapped our principal findings to the four stages of communication described as necessary for patient-centered care in the conceptual model of Halley and others (Table 1). 20 Mapping was done by three authors (CH, DF, DA), who reviewed the key findings and assessed if and where they fit in the model. A draft of this manuscript was shared with interviewees and we incorporated feedback from one participant about specifics around procedures and timing.
Results
We interviewed 19 respondents in Year 1 (Table 2). One cardiology and three orthopedic providers did not participate in the Year 2 follow-up interviews: one had left Group Health and the others were unavailable or did not respond. Our analysis identified areas of agreement and divergence between providers in the two specialties and investigated changes over time within specialties.
Comparing Orthopedics and Cardiology Attitudes: Areas of Agreement
Importance of Providing Information to Patients
Almost all providers interviewed stated that giving patients information about their condition and describing treatment options was a desirable clinical practice.
If someone’s going to have this big operation and it’s going to put them out of work and homebound for three weeks and recovering for three months, it’s almost like you can’t give them too much information…so that they really understand the impact of the decision and all the implications and not just the surgeon’s view. –Orthopedics provider
I don’t have any problem with any kinds of information given to any patients at any time. The more information a patient has, the easier it is for me. –Cardiology provider
Providers in both specialties expressed a need for some information to be customized to patient physiology and risk factors.
…with bypass surgery, your [risk] categories are by age because that’s the simplest way to categorize it. But it’s quite a different matter if you’ve already had a stroke and you’re diabetic and you’ve got a lot of vascular disease. –Cardiology provider
But a lot of people have reasons not to have joint replacement surgery…even if they do have bad arthritis, they’re sick or they are addicted to narcotics. They are morbidly obese, they have enough dementia or mental illness that they’ll have a lot of difficulty in the postoperative period. –Orthopedics provider
Emphasis on Initial Conservative Treatment
The general perception among providers in both specialties was that the DAs were useful for educating patients about the need to try more conservative treatment before considering more invasive options. Three cardiology providers stated that the DA increased patient comfort with trying conservative therapy before undergoing stenting or bypass surgery.
I’m a firm believer in medical therapy where it’s reasonable. Some patients are on the other side of the spectrum where they just think, “open the artery.” They watch the video, they realize that they’re seeing interviewed patients who are on medical therapy and are having a great time and doing well. –Cardiology provider
Orthopedics providers acknowledged even more strongly that the DA helped them ensure that patients exhausted all other treatment options before surgery.
People decide that’s what they want and they come in saying, “I want a knee replacement,” even when they’re not necessarily appropriate for it. So I think having information out there that they can review prior to coming in and having, you know, hearing some of the risks, and that is a good thing. –Orthopedics provider
Provider Views on Patients’ Desire to Participate in Decision Making
Both specialties showed variability in provider views about the extent to which patients wanted an active role in making care decisions. More than half of cardiology and orthopedics providers reported that some patients wanted an active role and others did not.
Probably twenty percent of patients…will rely completely on your recommendations. There’s about another twenty percent of people who will be completely suspicious … And most patients are somewhere in-between. They really appreciate you giving them some information to help them. –Orthopedics provider
Two cardiology and three orthopedics providers implied that all patients want an active role in their care.
Well, I think they do about everything. And that hip and knee replacements are just bigger operations, and so bigger and more important, they want to be more involved, yes. –Orthopedics provider
One cardiology provider talked primarily about patients wanting the provider to make care decisions; although, the provider saw this as undesirable.
People are scared. And when they’re scared, they suspend rational thought and they say to me, which is the scariest thing patients ever say to me, “Whatever you say, Doc”…There’s a certain—even today—there’s a certain acquiescence by patients. –Cardiology provider
Comparing Orthopedics and Cardiology Attitudes: Areas of Divergence
Providers’ Approaches to Decision Making
When asked about best approaches to talking with patients about treatment choices, providers from the two specialties expressed distinct differences about the degree to which patients should or could be involved in decision making.
Orthopedics
Orthopedics providers were almost all adamant that responsibility for treatment decisions remains with the patient. They emphasized that, ultimately, the patient lives through the recovery phase and deals with any complications. At least one provider pointed out that treatment choices become more limited after joint replacement.
It’s their body…it’s very much their decision because if there’s a complication, even if it’s only a one-percent chance, they need to sort of be aware…particularly if that one percent can be something profound like having to return to the operating room…They’d want to know that that can happen. Or, if it didn’t work out, that, you know, I can’t give them their old knee back.
No orthopedics providers found these conversations difficult, as making the decision to have a joint replacement is rarely urgent.
Cardiology
Most cardiology providers supported an active patient role in treatment decisions but found this was much more challenging to practice because decision making for the targeted procedures was complicated by the close link between diagnosis and treatment for chronic stable angina. Diagnosis of this condition usually involves an angiogram, which requires cardiac catheterization with the patient sedated. Angiogram findings often provide critical information about the appropriateness of stent insertion. Many providers preferred inserting stents at the time of the angiogram because deferring stent treatment until after an SDM conversation meant subjecting the patient to a second round of sedation and cardiac catheterization. Six providers mentioned discussing treatment options with patients before the angiogram but these conversations covered treatment options for several potential angiographic findings. Only three providers were comfortable with the level of information they could give about treatment choices before the angiogram.
We very often have an agreement ahead of time. If we find X, we’ll do A. If we find Y, we’ll do B. And if we find Z, we’ll stop everything and renegotiate.
When describing how they talked to patients about treatment options, cardiology providers expressed a willingness to make recommendations and steer patients toward a particular course of action.
The patients do what you tell them. Unless you don’t know what you want to do. And I routinely sound people out… the vast majority tell you, “Do whatever you think is best depending on what you see.”
Perceived Impact of Decision Aids on Patient Care
Providers in both specialties reported that the DAs had little impact on content or type of conversations with patients. However, orthopedics providers more often than cardiology providers attributed positive changes in their patient interactions to DA use.
Orthopedics
Orthopedics providers more often felt that the DAs enhanced patient knowledge and patient engagement, leading toward greater SDM. They described conversations with patients who had watched the DA as “more nuanced,” or “more productive,” and said patients “asked better questions.”
You know, if they go in there knowing nothing, then I’m starting from the beginning and they can’t absorb it all or they don’t have any questions…I don’t think it’s saved an appreciable amount of time. I just think they’re better off.
One provider reported that patients were more empowered to take an active role in decision making.
A more informed patient is more participatory…Now it’s not just something happening to them. They’re not just passive. They understand “I’m involved. I’m the one that’s going to make this knee work.”
Four orthopedics providers reported that the DAs influenced or informed patients’ treatment decisions; although, they tended to describe these instances as rare.
I have had the occasional patient who said, “I thought I wanted a knee replacement but I’ve looked at the video and now I realize I don’t.” But, I would have to say, that’s quite uncommon.
Seven orthopedics providers reported that the DAs reinforced conversations they always had with patients and/or supplemented materials and classes they offered.
I think it’s great…for years, I have given people a lot of written material which I think is similar to what is presented to them in the videos…there are people who will get more out of a video than they will out of some written materials. I really like the idea that the videos, you know, reinforce the fact that there’s not a right or wrong answer for everybody. And sometimes patients don’t quite get that.
Only two orthopedics providers did not feel that the DAs added value beyond already available materials.
…we send them to a hip class that goes over everything over four hours. So anyone that’s interested in a hip or knee replacement, they get a live interaction over four hours going over this and more in greater depth. So I’m not sure where the video fits in.
Cardiology
In contrast, most cardiology providers felt that the DA did not promote SDM but presented helpful information regarding the nature of the treatment options and helped to ensure informed consent. This perspective emerged in follow-up interviews.
I don’t think it’s shared decision making. I think the video’s great. I think there’s lots of really good information in there, especially the description of what’s going to happen and what the options are. What I don’t like is that we [the cardiologists] decide that a patient needs a procedure. We give them the video. Tell them to go home and watch it. Then they come back to their angiogram. That’s not shared decision making!
It’s a great video for education, but it doesn’t affect us as far as decision making. In fact, I polled our group and I said, “How many of you are aware of patients who use the [DA] in either reinforcing or altering their opinion about whether they should have a coronary intervention?” And one doctor said, “Maybe one patient in the last year.”
Although a few providers mentioned enhanced conversations with patients such as “improved communication” and “facilitating” conversation, compared to their orthopedics counterparts, fewer cardiology providers positively assessed the contribution of the DAs to patient engagement. Instead, they tended to emphasize what they saw as having a negative impact on patient interactions. Four providers reported that the DAs increased the time spent with patients, including two who reported an increase in post-angiogram appointments.
I know that they’re now making some check-back appointments post-angiogram…I think the shared decision making may be part of the reason why this is happening now…
I’ve had many that brought back more questions, which you can argue would be good for the patient because it opened up some new avenues of discussion, but at the cost of a fair amount of time. We love to inform our patients maximally, but we only have so much time.
Nonetheless, two providers reported that the DA saved time during appointments.
It saves me a fair amount of time in explaining what the procedure is. It’s visual, so I find it very useful for extending the amount of information beyond the time that I would have [to take] to describe it nearly as well.
Overall, other positive impacts of the DAs were mentioned less frequently by cardiology than orthopedics providers. Only two mentioned that patients felt more comfortable or confident with their decisions.
I feel that the patient is more comfortable having watched the video, because I can feel that patient is more—they believe that they make a wiser decision and go through this without any uncertainty.
The same provider commented,
I’m more confident of their decision making.
One provider felt that the DA increased the level of informed consent,
I think they are going into the procedure more informed [if they watch it] and that would be the broadest advantage.
Throughout the intervention, many cardiology providers expressed skepticism about the appropriateness of the DA and SDM for coronary artery disease procedures. They had ongoing concerns that patients may choose to forego critical diagnostic testing after viewing the DA.
I think I’ve had a couple of people scared off from getting arteriograms again this past year. I think I had one the first year. It was not good…The video had nothing to do with whether a patient ought to have an angiogram. Nevertheless, it frightened people off into not getting an angiogram. And, so that’s not what we want.
However, cardiologists were open to using DAs for other cardiac conditions. For example, many mentioned that atrial fibrillation would be better suited to SDM.
Provider Concerns about Applicability and Tailoring of DA Content to Individuals or Organizations
Another area of divergence between the two specialties was the frequency and variety of concerns expressed regarding information in the DAs. In the first round of interviews, a few orthopedics providers raised concerns about limited discussion in the DAs about the risks of surgical intervention, especially for patients with other risk factors.
I’m not sure that the DVD sort of goes into risk factors for specific patient situations that would be particularly worse to a surgeon. For example, a patient who is on steroids and might have poor healing. Or a patient who has peripheral vascular disease and might have poor healing. Or a patient who has venous stasis disease and has ulcers in their legs and might be a big infection risk. A patient who has morbid obesity and would be at great risk for premature mechanical failure of the knee just because they’re too heavy for the knee.… So I think those types of situations aren’t always reflected accurately in the DVD and so someone who has those conditions might see something and say, “Oh gee, this operation’s for me,” when in fact, it could be technically done on you, but, you know, there’s a much greater substantial risk of complication with some of those patients. –Orthopedics provider
Other concerns raised by orthopedics providers were: 1) the DA was biased toward surgery, 2) information was confusing and might increase the need for in-depth discussions with patients, and 3) the material was too simple for educated patients. None of the concerns were expressed by more than two orthopedics providers and, overall, they did not have major concerns about the DA content; no concerns about content arose in follow-up interviews.
In contrast, cardiology providers raised numerous concerns about the DA, often questioning the accuracy of the information and statistics. Many respondents felt that the risks of angiography were overstated and influenced patients to refuse angiograms, which they viewed as beneficial for diagnosis.
The part that I disagree with is where they talk about risk [of undergoing an angiogram]. In every single circumstance, they talk about one out of a hundred. Incorrect. I’ve worked in cardiology since the 1980s and every cardiologist I’ve ever been with during a conversation about an angiogram is one in a thousand. That’s a huge discrepancy…And we’ve had patients see that and then cancel…that’s a high risk! One in a hundred of having a heart attack, dying, or a stroke is a high risk… –Cardiology provider
Several cardiology providers were also concerned that the DA seemed to suggest a choice between medical therapy and stenting: they emphasized that all patients get medical therapy, even after stenting.
… I didn’t like how it was said was where they talked about the medications….particularly the part with the male patient where they’re talking about impotence…the guy actually even says something like, “No doubt, you are going to be impotent with this medication.” That’s how I interpreted it from how he said it. Well, if you have men patients watching this and they are going to have impotence on these drugs, they’re not likely going to choose the drugs. And even if they have an angiogram and have a stent, likely they’re going to be on that drug afterwards. So it’s not just a preventative drug, it’s a drug that we use a lot, even after the procedures. So, I didn’t like how that was worded. –Cardiology provider
Cardiology providers also felt the DAs created confusion that necessitated more discussion and had too many numbers and statistics, many of which were based on data that did not contribute to individual patients’ risk factors. Unlike in orthopedics, many concerns were repeated in follow-up interviews.
Change Over Time
Many providers’ attitudes and beliefs about the DAs and SDM persisted over time. However, we did see some orthopedics providers shift from viewing the DAs as primarily for education to a greater understanding of how the tool promoted SDM. This shift was less evident in cardiology providers. Orthopedics providers who started with very few concerns about the DA content expressed no concerns in follow-up interviews. Cardiology providers’ concerns persisted over time; however, they were not as numerous or strongly stated at follow-up. Providers’ beliefs did not notably change between initial and follow-up interviews about providing patients with information, the need for conservative treatment, patients’ desire to participate in decision making, or decision-making approach/styles. Table 3 provides example quotes regarding providers’ decision-making approaches and attitudes towards patients taking an active role in decision making at Years 1 and 2, overall demonstrating the durability of provider perspectives and/or denial that the DA implementation changed their attitudes.
Comparison of Providers’ View of Patients Taking an Active Role in Decision Making at Year 1 and Year 2 Interviews
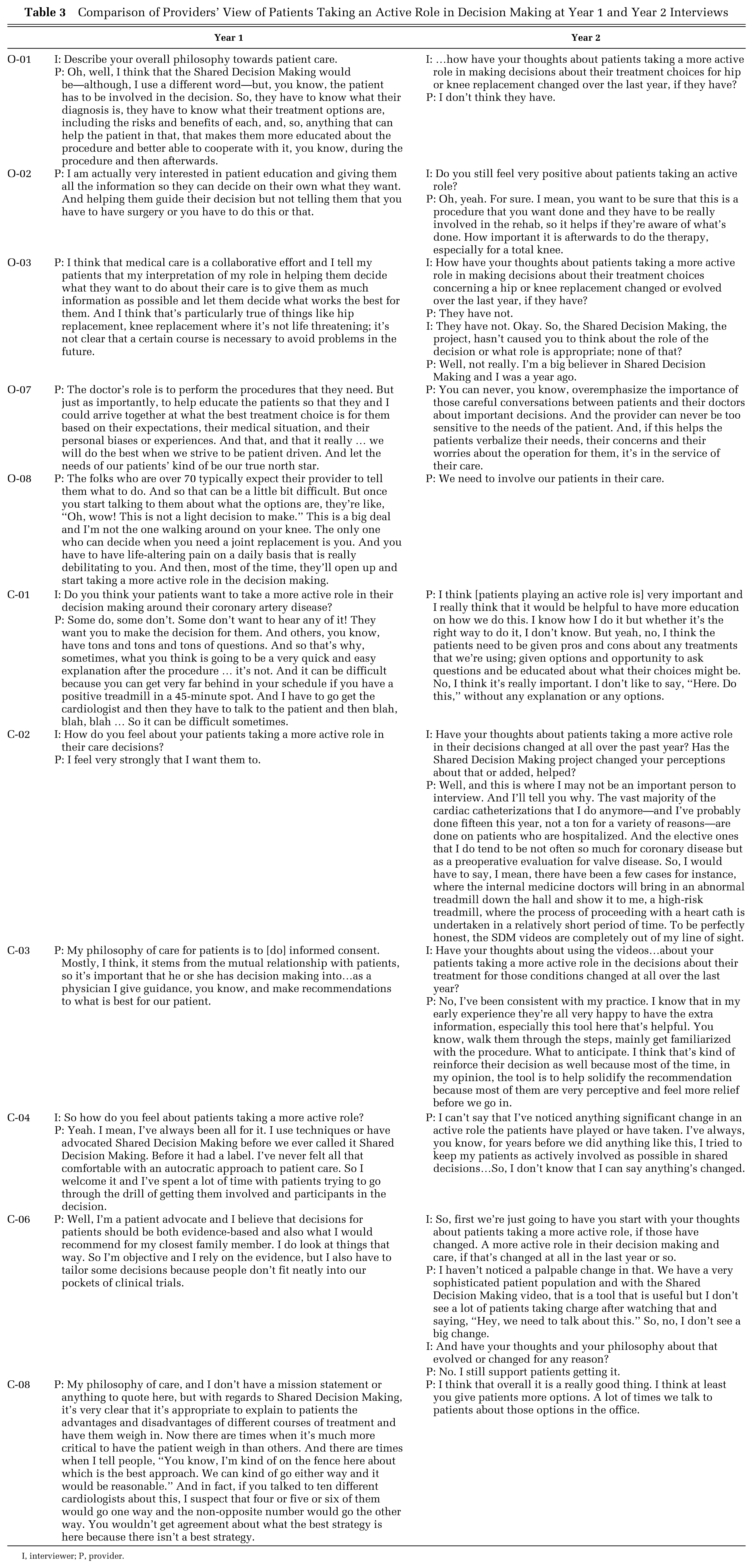
I, interviewer; P, provider.
Conceptual Context
We situated our findings in the broader SDM research by relating them to the conceptual model by Halley and others (Table 1). 20 Regarding Stage One (promotion), while providers were engaged in establishing workflow for implementation, no respondents indicated that they were engaged in the process of deciding which DAs to implement and for which health conditions. Indeed, in this setting, senior organizational leadership made those decisions before engaging frontline providers. Our findings also highlight the need for close attention to the timing of decision making when creating and/or selecting DAs for implementation. In cardiology, decisions about treatment for coronary heart disease often occur during diagnostic procedures—precluding effective shared decision making in the traditional sense and hindering optimal timing of the DA and SDM conversation. Regarding Stage Two (translation), we found that providers raised concerns about DA content and ability to customize the content to individual patient needs. For Stage Three (dissemination), the finding highlighted for Stage One regarding the timing of decision making also affected the dissemination/distribution of DAs. Lastly, we found some of the biggest issues and barriers at Stage Four (utilization), with varying levels of understanding about and ability to engage patients in effective SDM conversations both between providers and across specialties. Several providers questioned the value of shared decisions for some patients and others reported deficits in their understanding of how shared decision making was different than standard informed consent.
Discussion
We are aware of few studies that, like ours, look at providers’ attitudes toward DAs and SDM after a robust organization-level effort to distribute DAs and encourage SDM. Our data included interviews during the first year of implementation and after one year, allowing us to explore the potential for shifting attitudes over time. Our results demonstrated that provider attitudes can differ greatly across specialty and/or clinical topic and that these differences can strongly affect providers’ willingness to engage in DA distribution and SDM.
Providers in both specialties agreed that the DAs helped educate patients about more conservative treatment options. However, providers had concerns about specific content in the DAs that they felt might predispose patients to make higher-risk choices. Orthopedics providers had concerns that the DAs underestimated the risks of surgical intervention, especially for patients with other risk factors. Cardiology providers were concerned that patients would reject diagnostic testing and thereby be unable to integrate important evidence into their decision-making process.
Orthopedics and cardiology providers diverged in their assessment of the practicality and relative importance of the patient’s role in decision making for the targetted health conditions. Orthopedics providers saw the DAs and SDM as a critical component of the care process for joint replacement. Cardiologists felt the DAs and SDM were difficult to implement in the context of chronic stable angina because of specific features about their practice: they pointed to the advantages of evaluating the need for a stent and inserting it during a single angiogram procedure, without stopping to consult with the patient about treatment options. Several cardiologists said they would be more supportive of DAs on different topics, specifically mentioning atrial fibrillation.
The model by Halley and others 20 illustrates the need for future work at Group Health and future SDM studies to consider all stages of communication necessary to successfully implement DAs and SDM into clinical practice to support patient-centered care. Specifically, we found that the lack of attention to Stage One in this implementation process may have been a major barrier to success for cardiology providers because, given the opportunity, they would likely have chosen a different condition and DA for SDM implementation (i.e., atrial fibrillation). Furthermore, the condition and DA chosen for implementation in cardiology presented numerous challenges to the optimal timing for SDM, which was its greatest barrier to effective use in clinical practice. Finally, several providers in both specialties expressed a general lack of understanding regarding the difference between SDM and usual informed consent, emphasizing the need for training and skill building to improve SDM practices in clinical care.
Our findings from an in-depth examination of attitudes and reactions of providers in two specialty service lines to a robust DA and SDM implementation project have implications for the planning and implementation of future SDM projects that rely on DAs. First, organizations should carefully consider how the decision-making and care processes for specific conditions may affect the timing and ultimate application of SDM. Involving health administrators and providers expected to use DAs in the design and customization of DAs and strategies for integrating them into clinical processes could proactively address these concerns. Second, DA content may need to be tailored to individual patients and institutions. Therefore, finding ways to better customize DAs or make content interactive may be an important component of increasing provider acceptance and the use of DAs. Many models for more interactive types of DAs are currently being developed and evaluated. Furthermore, we found that most attitudes regarding DAs were durable over time—despite successful distribution of DAs and leadership promotion of SDM. Thus, we need to better understand which issues and factors have the highest likelihood of influencing individual provider beliefs and attitudes, such as better ways of involving providers up front in customizing DA content or addressing specific timing or logistical issues that may be seen as barriers to SDM. Last, although providing DAs is an important and necessary component of SDM, DAs alone do not create a meaningful SDM process. Providers at our site received additional training in SDM, but only after our interviews concluded. Finding ways to move beyond DA distribution to a culture in which providers regularly engage patients in conversations about how treatment decisions fit individual values and life circumstances continues to be an area for innovation and experimentation. A recent environmental scan of SDM training programs for health professionals found a growing number of programs, 38 but few (21%) had published evaluations. This gap highlights the need for systematic evaluations to determine the most effective types of training programs.
This study expands on the substantial literature on the use of DAs and SDM. Numerous studies found that provider attitudes can pose a challenge to distributing DAs and promoting SDM.21-25,28,29,39-41 Elwyn and others 21 specifically note the need for more exploration of provider attitudes. This paper begins to fill that gap through in-depth, qualitative interviews of the attitudes and beliefs of providers in two specialties, all of whom participated in a successful, long-term DA distribution and SDM promotion effort. Our findings contribute new insights into the ways that attitudes can vary across specialties and the extent to which attitudes and beliefs may persist or change over time. In particular, logistical challenges surrounding diagnosis and the timing of decision making can be major barriers to providers embracing fully DA use and the value of SDM.
A major limitation of our evaluation was the lack of patient perspectives. We hope to address this in future research. Social desirability bias may have influenced providers’ responses, causing them to appear more open to SDM and an active patient role. Several providers chose not to participate, causing possible selection bias. However, those who participated had a range of opinions. While we did a limited number of interviews and observations in all specialty groups affected by the DAs, we had sufficient resources for extensive interviews in only two specialties. These two might not have surfaced all possible issues and concerns providers have regarding DAs; a number of more general issues were addressed in an earlier manuscript. 26 Finally, this project was conducted at a large, integrated health care organization with factors that facilitated DA implementation including salaried providers, an expectation that providers follow clinical guidelines and standard work, a practice culture that favors conservative treatment and an active patient role, and a patient population that is primarily employed or retired. Interviews of providers in other settings, such as fee-for-service clinical practice, or with different patient populations, could yield different findings.
Conclusion
Our findings highlight the challenges of implementing DAs outside a controlled research setting. The Group Health intervention was successful in distributing large numbers of DAs 26 and providers generally agreed that DAs were a good way to provide patients with information about specific medical conditions and treatment options. However, these successes were counterbalanced by provider beliefs about appropriate decision-making styles that were sometimes less patient-centered than ideal, and these styles appeared to persist over time. Our findings suggest that health care leaders and clinicians who plan to implement DAs to support SDM should get provider input and engagement when deciding on the use of DAs and SDM for each candidate condition. Our results also suggest a need to assess provider attitudes about the role of patients in decision making for a specific condition prior to implementation.
Footnotes
Acknowledgements
We thank the decision aid implementation team: Marc Mora, MD; Chris Cable, MD; Karen Merrikin, JD; Tiffany Nelson; Stan Wanezek; and Charity McCollum; the Research Advisory Panel: Michael Von Korff, ScD; Douglas Conrad, PhD; Carolyn Watts, PhD; Michael Barry, MD; Richard Wexler, MD; and Jeffery N. Katz, MD; and other GHRI employees that assisted with data collection and manuscript development: Sylvia Hoffmeyer, Carol Cahill. Chris Tachibana, PhD provided invaluable scientific editing expertise. We also want to thank the GHRI clinical staff that made time to participate in interviews and the Group Health leaders and providers who reviewed and provided feedback on this manuscript, including Chris Cable, Matt Handley and David McCulloch.
This manuscript is the result of work done at Group Health Research Institute with a grant from the Commonwealth Fund, the Informed Medical Decisions Foundation, and the Group Health Foundation. Financial support for this study was provided entirely by grants from The Commonwealth Fund, the Informed Medical Decisions Foundation, and the Group Health Foundation. The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.