
Abstract

The surgical time-out (surgical verification) is a mandatory and effective tool to minimize iatrogenic complications for ophthalmologists and other medical and surgical specialists. 1 While operating rooms routinely require a time-out to review the procedure and the operative site before beginning the surgery and when another surgeon comes in intraoperatively, it is not common to have additional time-outs during retinal procedures. The Research and Safety in Therapeutics (ReST) Committee of the American Society of Retina Specialists would propose that retina specialists consider intraoperative time-outs at decision points where iatrogenic complications are capable of high morbidity. Specifically, based on recent reports of devastating iatrogenic complications, we propose an intraoperative time-out prior to scraping the cornea and prior to fluid–air exchange.
Time Out Before Scraping the Cornea: Has the Patient Had Prior Laser In Situ Keratomileusis?
In the event that corneal epithelial edema obscures the view to the posterior segment during surgery, retina surgeons often scrape the corneal epithelium to improve visualization for the remainder of the case. Accidental scraping into the edge of a prior laser in situ keratomileusis (LASIK) flap can open the flap (Figure 1) and/or amputate the flap, resulting in corneal epithelial downgrowth, corneal failure, or refractive complications that are not easily managed and may result in permanent vision loss. Since it is important to remember whether the patient had prior LASIK, it would be prudent to perform a time-out prior to corneal scraping by verbalizing whether the patient has a known history of LASIK surgery. This should be followed by examining the cornea for signs of a LASIK flap.
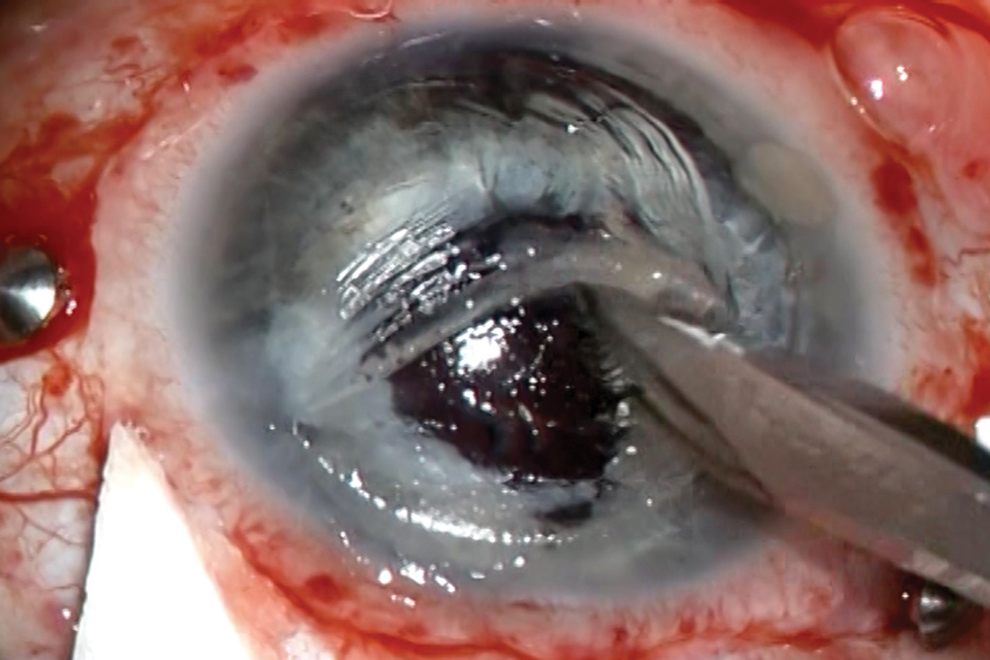
Inadvertent scraping of laser in situ keratomileusis (LASIK) flap during epithelial debridement. Note the blade scraping superiorly rather than from nasal to temporal.
It is best to avoid corneal scraping in patients who previously had LASIK surgery. If epithelial scraping is absolutely necessary, we recommend first visualizing the hinge and the extent of the flap, scraping only in a direction away from the hinge and avoiding the edge of the flap. If the location of the flap cannot be determined by history or clinical examination, it is more likely to have been located nasally. Thus, scraping from nasal to temporal may be safer as a general rule, however, this cannot be fully assumed, so care should be taken regardless. By performing a time-out regarding history of LASIK procedure, it is hoped that extra attention can be provided during corneal epithelial scraping in these eyes, thereby minimizing potential postoperative corneal complications.
Time-Out Before Fluid–Air Exchange: Is the Infusion Confirmed to Be in the Vitreous Cavity?
With the transition to small-gauge surgery, the infusion cannulas are no longer sutured into place and thus more prone to malpositioning (Figure 2). There are recent reports of fatal air embolism associated with fluid–air exchange 2 during pars plana vitrectomy presumably due to the infusion cannula inadvertently positioned in the suprachoroidal space. 3 –5 This complication highlights the importance of double-checking the location of the cannula prior to this maneuver. 6 Inadvertent movement of the infusion cannula to the suprachoroidal space during the fluid–air or air–gas exchange presumably exposes the choroid to air or gas, resulting in rupturing of the connection between the choroid and the vortex veins and driving bubbles into the bloodstream that can lodge in the cardiopulmonary circulation, causing cardiac arrest. 7 An even more common misdirection of air can occur if the line is pointed toward the lens rather than perpendicularly into the central vitreous cavity. In this case, the cannula may rupture through zonules and enter the anterior chamber even in phakic eyes (Figure 3). Retinal surgeons are trained to confirm the location of the infusion cannula in the vitreous cavity at the beginning of vitrectomy but may not be accustomed to double-checking the cannula position prior to fluid–air exchange. The retina surgeons should consider pausing, visually confirming, and verbalizing that the cannula is in good position within the vitreous cavity and pointed perpendicularly away from the lens and iris prior to fluid–air exchange.
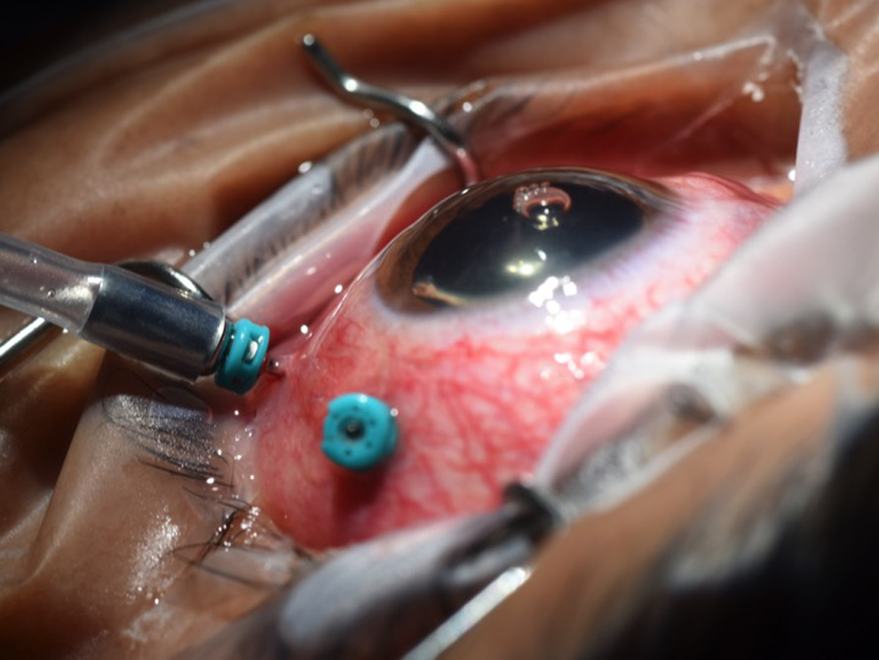
Malpositioned infusion cannula during fluid–air exchange. Note space between the hub of cannula and conjunctiva and also air bubble in the anterior chamber.
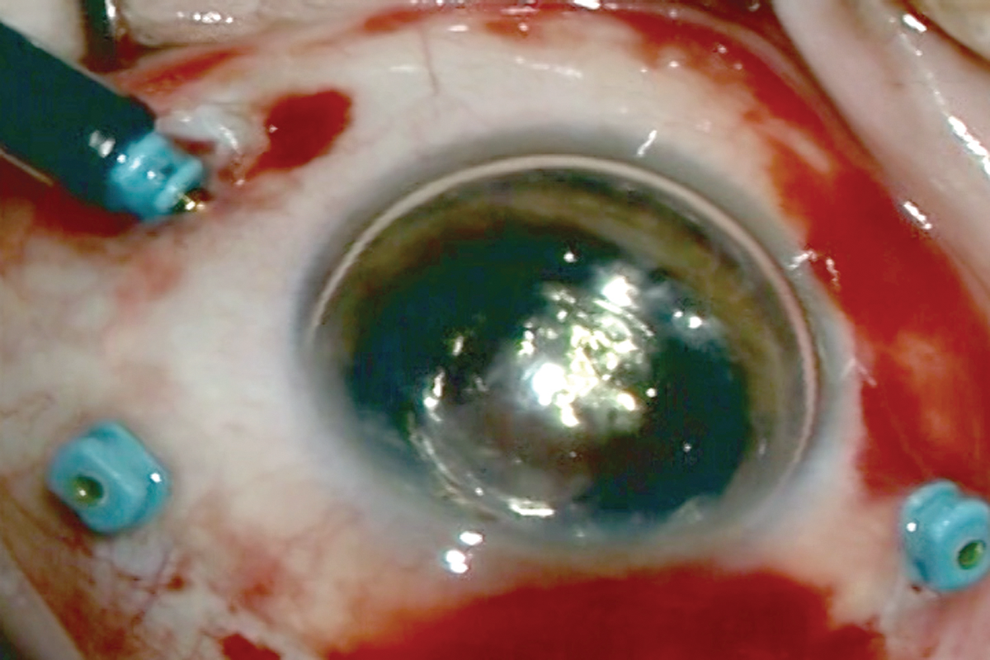
Malpositioned cannula allowing air infusion into the anterior chamber of a phakic eye. Note the tangential lie of the 25-gauge infusion cannula and its direction toward lens rather than perpendicular to the sclera.
Preoperative time-out is universally employed to decrease rates of wrong patient surgery, wrong site surgery, wrong intraocular lens selection, and wrong surgical procedure. The ReST Committee urges retina specialists to consider incorporating intraoperative time-outs prior to scraping the corneal epithelium and prior to fluid–air exchange in order to decrease the aforementioned potentially devastating iatrogenic complications.
Footnotes
Acknowledgments
The ReST Committee would like to thank Jill Blim and Nidhi Batra for indispensable help with this article.