
Abstract
Purpose:
This work evaluates a microincisional vitrectomy surgical (MIVS) approach to endolaser ablation of small uveal malignant melanoma by incorporating genetic tumor classification as a means to avoid radiotherapy while maintaining local tumor control without compromising visual acuity (VA).
Methods:
An institutional review board–approved, single-surgeon, retrospective analysis was conducted of a consecutive case series of all patients with tumors less than 2.5 mm in apical thickness who underwent MIVS, endolaser tumor ablation, fine-needle aspiration biopsy (FNAB), and intravitreal triamcinolone acetonide for small uveal melanoma between 2012 and 2015.
Results:
A total of 226 patients underwent FNAB from January 2012 to January 2015 for uveal melanoma. All 58 patients treated for a small uveal melanoma were included. This group of patients had a minimum follow-up of 60 months (range, 60-93 months). At initial diagnosis, subretinal fluid was present in 52 eyes (89.1%), macular edema was present in 24 eyes (41.4%), and epiretinal membrane was present in 11 eyes (20.1%). Fifty-six specimens (96.5%) received a molecular classification of either class 2 (4 of 56, 7.1%) or class 1 (52 of 56, 92.8%). Initial VA was 20/40 or better in 26 eyes (44.8%), and final VA was 20/40 or better in 48 of 58 eyes (82.8%).
Conclusions:
Endolaser tumor ablation delivered at MIVS surgery enables excellent tumor control (98.3%) and improves VA to better than 20/40 in more than 80% of treated eyes. FNAB achieves molecular classification in 96.5% of all patients undergoing treatment for small choroidal melanoma independent of tumor size.
Introduction
The incidence of uveal malignant melanoma has been reported to be as high as 1 case per 200 000 per year. 1 Small uveal melanoma continues to represent a diagnostic and therapeutic challenge despite being the most common primary intraocular malignant tumor in adults. 1,2 The mechanisms and risk factors leading to primary uveal melanoma continue to be elucidated. 2 -9 During the last 20 years there has been widespread use of radiotherapy, either brachytherapy or charged-particle delivery for the treatment of uveal melanoma; however, significant morbidity and mortality are still associated with this disease. 10 Definitive treatment of malignant melanoma, especially small tumors, has been controversial because of the similarities with atypical uveal nevi. Furthermore, radiation retinopathy and radiation optic neuropathy can be seen following brachytherapy in virtually all patients with macular and juxta papillary tumors. 11 -13
Recently, molecular testing including chromosomal analysis, gene-expression profiling (GEP), and RNA screening either by incisional biopsy or fine-needle aspiration biopsy (FNAB) has elucidated the most common genetic mutations associated with uveal melanoma. 14 -19 At this time, the most extensively validated, commercially available, prognostic genetic test for uveal melanoma is the GEP FNAB. 20
Multiple surgical strategies have been described for FNAB. 21,22 However, the literature regarding FNAB for GEP in small choroidal melanoma is scarce. The purpose of our study is to evaluate a large, consecutive case series of individuals with small uveal melanoma undergoing definitive pars plana vitrectomy (PPV), endolaser ablation of tumor, and transvitreal 25-gauge FNAB for molecular classification with GEP with a minimum follow-up of 5 years.
Methods
An institutional review board–approved (LCH-3-012015), single-surgeon, retrospective analysis of a consecutive case series of all patients undergoing microincisional vitrectomy surgery (MIVS)–delivered endolaser tumor ablation coupled with FNAB during PPV using a 25-gauge needle and multipass approach for GEP analysis of small uveal melanoma between January 2012 and January 2015 was performed according to the Declaration of Helsinki. All treated tumors had shown increases in apical height, risk of focal serous retinal detachment (RD), and/or increase in basal diameter.
Inclusion criteria for this review were limited to patients with a tumor apical height of less than 2.5 mm and a minimum follow-up of 60 months. All FNAB specimens were processed for uveal melanoma diagnostic testing using a standard, commercially available processing approach, and all testing was completed by a single laboratory (Castle Biosciences, Inc). Patients underwent primary 532-nm diode endolaser ablation of uveal melanoma prior to the FNAB procedure. Tumors with an apical height equal or greater than 2.5 mm, prior treatment, or iris involvement were excluded from the study.
Technique
The transvitreal FNAB was performed in combination with a 23- and 25-gauge microincisional PPV system under microscopic visualization in all eyes (surgeon T.G.M.). The technique involved a 3-port PPV trochar-cannula set with valves. Valved cannulas were placed using transconjunctival displacement and oblique insertion to enhance scleral closure. No conjunctival dissection was performed. After primary vitrectomy was completed, peeling of the posterior hyaloid was performed with specific attention to vitreotumoral adhesions; complete confluent tumor endolaser ablation was performed as the primary tumor treatment in these cases of small choroidal melanomas. Laser ablation extended to at least 0.2 mm beyond tumor margins. A multipass biopsy with a 25-gauge, 1-inch needle attached to a 5.0-mL syringe was performed via the valved-cannula system. During the biopsy, the assistant aspirated the syringe while the surgeon directed the needle with multiple passes through a single transretinal needle penetration. Intraocular pressure was elevated to 50 mm Hg immediately prior to the biopsy to reduce intraoperative hemorrhage and then returned to normal after the biopsy was complete. If tumoral hemorrhage was seen on termination of the FNAB, endolaser was used to cauterize the hemorrhagic site (Figure 1).
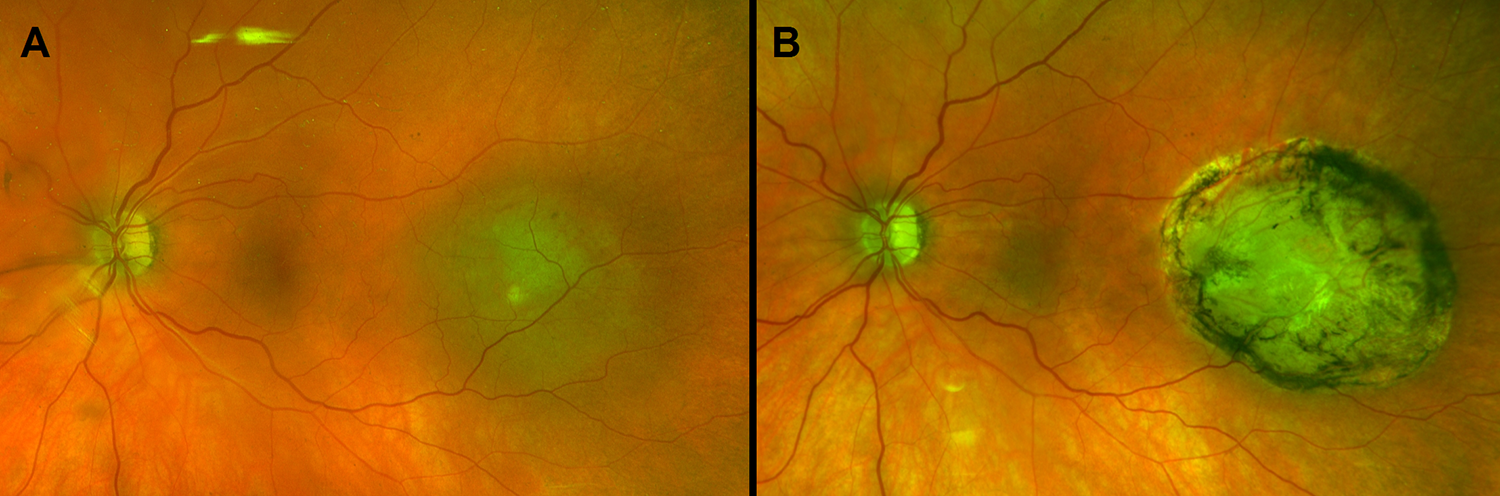
Small choroidal melanoma (A) before treatment and (B) after treatment.
Intravitreal triamcinolone acetonide 4 mg was injected prior to removal of the cannulas. The triamcinolone acetonide that was used was packaged Triesence (Novartis Pharmaceuticals) because this suspension is Food and Drug Administration approved for vitrectomy. No cryotherapy was performed at the cannula sites after removal.
After the FNAB was performed, tumor cells were collected and processed in a standard vial as described by Castle Biosciences, Inc and immediately placed on ice to be shipped overnight.
Results
During the study interval, 226 patients underwent FNAB from January 2012 to January 2015 for uveal melanoma. This study focused on the consecutive case series of patients with small ocular melanoma and a minimum 5-year follow-up. Inclusion criteria selected patients with small choroidal melanoma with an apical height of less than 2.5 mm. Fifty-eight individuals met the small melanoma tumor study inclusion criteria and were analyzed. Minimum follow-up ranged from 60-93 months (Table 1). Mean patient age at diagnosis was 71.4 years (range, 41-91 years). Best-corrected visual acuity (VA) at diagnosis was 20/40 or better in 26 eyes (44.8%), between 20/50 and 20/200 in 31 eyes (53.4%), and worse than 20/200 in 1 eye (1.7%). Best postoperative VA was 20/40 or better in 48 eyes (82.8%) and between 20/50 and 20/200 in the remaining 10 eyes (17.2%).
Demographic Characteristics of Patients (N = 58).
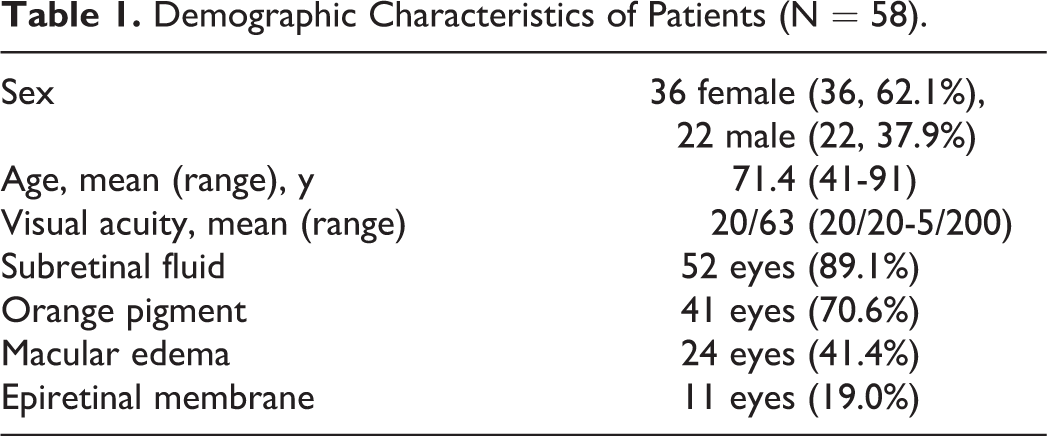
At initial presentation, subretinal fluid was present in 52 eyes (89.1%), macular edema was present in 24 eyes (41.4%), and epiretinal membrane was present in 11 eyes (19.0%). Subretinal fluid and/or macular edema that required intravitreal therapy was present in 21 eyes (36.2%) at any postoperative evaluation. Epiretinal membrane was present in 7 eyes (12.1%) at last evaluation. Traction/rhegmatogenous RD occurred in 1 eye (1.7%) postoperatively. Persistent exudative or tractional detachments occurred in 2 eyes (3.4%). Vitreous hemorrhage occurred in these 2 eyes plus 1 eye alone for a total of 3 eyes (5.2%). No patient with vitreous hemorrhage alone required surgical management. One eye developed a subretinal hemorrhage that was treated with intravitreal antivascular endothelial growth factor therapy and cleared over 4 weeks.
Tumors were located posterior to the equator in 47 patients (81.0%) and anterior to the equator in the remaining 11 patients (19.0%). Mean tumor basal diameter was 10.8 mm (range, 5-15 mm). At diagnosis mean tumor apical height was 1.8 mm (range, 1.0-2.4 mm). Mean postoperative tumor apical height was 1.1 mm (range, 1.0-1.3 mm) at last evaluation.
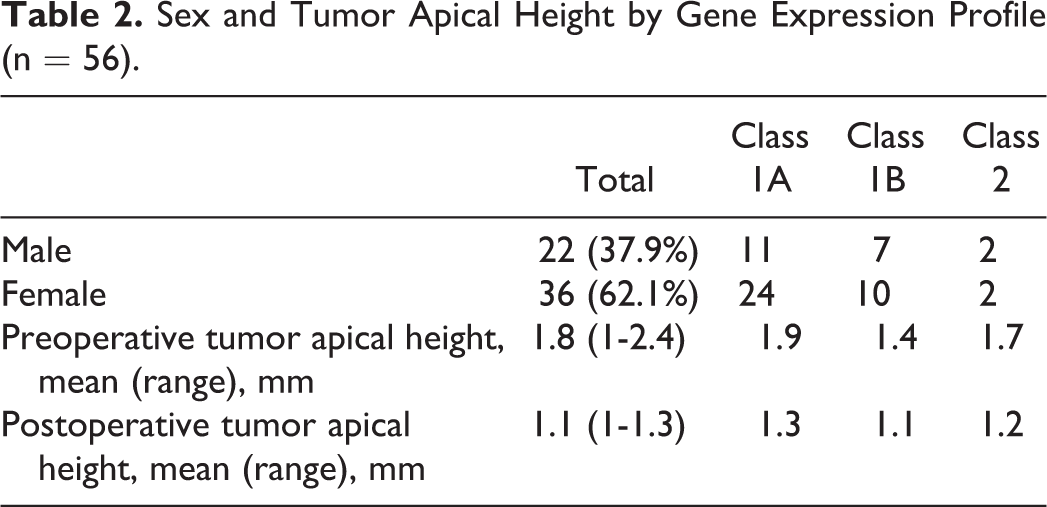
Fifty-six specimens (96.6%) received a molecular classification of either class 2 (4 of 56, 7.1%) or class 1 (52 of 56, 92.8%) (Table 2). Class 1 tumors were further defined as class 1b (17 of 52, 32.7%) or class 1a (35 of 52, 67.3%). Two specimens (3.4%) exhibited multiple gene failure. Excessive fluid biopsy volume was the primary association, with reported multiple gene failure occurring in both specimens. One class 1A tumor (1.7%) required brachytherapy after primary ablative therapy because of recurrent disease. No eyes required enucleation, and no patients developed metastasis during the entire study window.
Sex and Tumor Apical Height by Gene Expression Profile (n = 56).
Discussion
Small uveal melanoma continues to be a challenging diagnosis because of the overlap with atypical uveal nevi. To date, the Collaborative Ocular Melanoma Study (COMS) was the largest randomized controlled trial performed to evaluate uveal melanoma. 11 In the COMS, tumors less than 2.5 mm in apical height were observed.
A total of 188 small uveal melanoma tumors were not treated at the time of study enrollment during the COMS; 46 grew during follow-up to a size that was large enough to be eligible for the COMS clinical trials. 23,24 Of small choroidal melanomas initially managed by observation, 21% demonstrated growth by 2 years and 31% by 5 years. This underscores the risk associated with observation as a primary therapy, because larger tumors have higher risk of metastasis long-term. 2,11,23,24
Nonetheless, observation remains a valid treatment approach for small atypical lesions when close interval follow-up can be maintained. In several studies, observation was safely used with transition to definitive treatment when clinical markers of malignant transformation were observed. In those studies, 5-year melanoma-specific mortality rates varied from 1% to 3%. In the COMS, 10-year mortality rates for small choroidal melanoma were approximately 10%. In that observational study, treatment was performed at the discretion of the treating surgeon with virtually half of the initially observed patients receiving treatment.
A hallmark study performed by Kujala et al in Finland that included 289 individuals found that more than 50% of patients with primary uveal malignant melanoma developed metastasis after 35 years of follow-up. 25 A significant melanoma-related mortality despite treatment of the primary tumor emphasized that uveal melanomas may have metastasized at the time of treatment. Understanding that metastasis is likely to occur early in the disease process is key to understanding why metastasis rates have changed only minimally during the last 3 decades. It is also pivotal for the development of individualized risk-dependent treatments that improve metastasis rates. Fortunately, evolving data have suggested that earlier intervention, approximated by smaller tumor size at the time of definitive treatment, is associated with lower mortality rates. Further understanding of the molecular profile of each individual tumor has suggested that further risk stratification can be performed with tumor genetic profiling.
Multiple studies have shown that specific mutations in chromosomes 3, 6, and 8 are associated with posterior uveal melanoma. 19 Recent studies have shown that mutation in the BAP1 gene is associated with increased risk of metastasis in patients with uveal melanoma. 18 Monosomy 3 has also been associated with increased malignant potential in uveal melanoma. 19
One approach to molecular studies has grouped uveal melanoma into prognostic classes based on GEP. 20 The Castle Biosciences, Inc assay stratified tumors into 3 different classes: 1A, 1B, and 2. Patients with these classes of tumors have a 2% (class 1A), 11% (class 1B), and 72% (class 2) incidence of metastasis at 5 years. 21 GEP classification is currently used for patient education, screening protocols, enrollment in clinical trials, and prophylactic therapy (eg, valproic acid and ipilimumab oral treatment). However, no consensus among ocular oncologists exists regarding the timing and/or approach to tumor biopsy.
GEP allows molecular classification in very small melanomas. 20,21 It is suggested that as few as 6 of 7 tumor cells may be adequate to obtain molecular tumor profiling with GEP analysis. That technology allows molecular classification of small choroidal melanoma, whereas our surgical approach incorporated definitive tumor treatment while obtaining molecular tumor profiling. 26 This approach of incorporating biopsy classification with definitive tumor treatment focuses on eliminating future progression of tumor genetics, which may occur in the setting of biopsy alone. Further, GEP class 2 tumors may benefit from treatment strategies that incorporate additional tumor treatment, enhanced screening, or potentially adjunctive systemic therapy. GEP class 1 tumors may not require enhanced treatment or screening after initial ablation. In some studies, RD risk associated with choroidal melanoma FNAB is similar to that of eyes following vitrectomy or cataract surgery. 27,28 RD after FNAB may be complex and present with persistent exudative RD, progressive tractional RD, or a combination of these presentations, including development of a rhegmatogenous RD.
The present series reports a low risk for rhegmatogenous RD (1.7%) and vitreous hemorrhage (5.2%) that may be the result of better intraocular pressure control and endolaser cauterization during the biopsy procedure compared with other studies that use nonvitrectomy approaches to biopsy. 22 In contrast, transvitreal biopsy without vitrectomy has been shown to require a second surgical procedure to manage persistent RD or nonclearing vitreous hemorrhage in 3.5% and 5.9% of patients, respectively. 28 In this setting, the surgical approach to both biopsy and definitive treatment, incorporating small-gauge vitrectomy, may have a lower complication than the risk of transvitreal FNAB without either vitrectomy or endolaser. The use of MIVS-controlled vitrectomy to enable removal of tractional alterations at the tumor, endolaser direct tumor ablation, and 25-gauge FNAB followed by intravitreal steroid suppression of postsurgical inflammation may effectively couple early, small-tumor treatment with preservation of anatomic and visual function. This approach has the potential to decrease tumor-associated mortality by moving to an earlier treatment approach without compromising ocular function. 11 -13
In our study, no patient developed metastasis (follow-up, 60-93 months), suggesting that the morbidity associated with early FNAB combined with PPV and endolaser ablation might be lower than the risk of mortality associated with observation.
Definitive endolaser tumor ablation delivered during MIVS enables controlled transvitreal FNAB while relieving tractional forces on the retina and suppressing the inflammatory sequelae of the surgical procedure with triamcinolone acetonide. This surgical approach achieves excellent local tumor control (98.3%) with extended follow-up beyond 5 years (Table 3). Complications related to FNAB using these techniques are rare and may be lower. Most recent studies have not seen any increase in mortality associated with FNAB. 29 However, the risks vs benefits associated with different FNAB techniques are not completely understood. This article documented excellent long-term tumor control, avoiding radiotherapy in all cases. Additionally, compared with a recent study assessing brachytherapy for small choroidal melanoma, this treatment approach yielded nearly identical local control, sparing the patient radiotherapy. 30 For this series, GEP class did not affect tumor control or 5-year risk of metastatic disease.
Entry and Extended Follow-up Outcomes.

Conclusions
Decision-making for management of small melanoma is complex and includes diagnostic accuracy, appropriate treatment, and long-term outcome. In this unique subset of choroidal melanoma, we believe that treatment efficacy must be greater than 90% with local control maintained through a 5-year window. As important as VA is in small-melanoma management, patient survival must always be paramount.
Finally, limitations in our study included the use of a single surgeon (T.G.M.), single institution, retrospective review, and small case series, whereas potential advantages included a single, defined surgical approach, standardized molecular tumor analysis, defined patient inclusion characteristics, and long-term extended follow-up.
Ultimately, additional prospective studies that evaluate FNAB techniques, definitive tumor treatment approaches, morbidity, and mortality are needed to improve our understanding of the long-term outcomes of the treatment of small choroidal melanoma.
The evolution of therapy toward definitively treating small choroidal melanoma at earlier time points must be defined by local tumor control, anatomic and visual functional outcomes, and extended follow-up. Further, future treatments must use definitive molecular tumor analysis that, at this time, remains obtainable only by direct intratumoral biopsy.
Footnotes
Ethical Approval
This report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)–compliant manner.
Statement of Informed Consent
Standard surgical consent was obtained. Per our institutional review board, no study consent was required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health (grant No. P30-EY014801) and an unrestricted grant to the University of Miami from Research to Prevent Blindness.