
Abstract
Keywords
Introduction
The Centers for Medicare & Medicaid Services (CMS) determine physician reimbursement rates based on a variety of factors, including estimated physician work, practice expenses, professional liability insurance, and budget. After adjusting for inflation, Medicare reimbursements have been shown to have decreased across multiple subspecialties over time, including neurosurgery, 1 general surgery, 2 reconstructive microsurgery, 3 and orthopedics. 4 Likewise, Medicare reimbursements for common vitreoretinal procedures have been declining over the years. 5 Performing retinal detachment repair has been shown to be associated with a significant opportunity cost for the vitreoretinal surgeon. 6
The purpose of the current analysis was to compare Medicare physician reimbursements for the most common vitreoretinal surgeries against the potential reimbursements the physician could have generated by managing patients in the office during the equivalent time within the 90-day global period.
Methods
A theoretical model was designed using TreeAgePro (TreeAge Software, LLC). No human subjects were involved; therefore, institutional review board approval was not required. The study complied with all local and federal laws.
Physician reimbursement rates in the United States are calculated by CMS based on the sum of the estimated physician work, professional liability insurance, and practice expenses, each of which are assigned separate relative value units (RVUs). The physician work component is based on time and work intensity, reflecting the technical skill, physical effort, mental effort and judgment, and stress from the patient risks involved. 7 The current analysis focused on the physician perspective; thus, practice expenses (eg, staffing, equipment, rent, and professional liability insurance) were not included.
CMS defines the global period of every surgical procedure with a specified preservice, intraservice, and postservice time along with an allocated number of postoperative visits. Preservice time includes pre-evaluation time, pre-positioning time, and preservice scrub/dress/wait time, and each of these components is assigned a time allocation by CMS. The pre-evaluation includes tasks such as obtaining consent, coordinating surgery, and surgical planning that can be performed before surgery in the clinic as well as by nonphysician staff; therefore, to be conservative, these were excluded from the model. The remainder of the preservice tasks (ie, pre-positioning and preservice scrub/dress/wait) along with immediate postservice patient counseling were grouped in this model as immediate perioperative care. The intraservice time consisted of the surgical operating time (ie, skin-to-skin incision time), as defined by CMS. 8 The number of postoperative visits in the global period is defined by CMS for each surgical code.
The model estimated the potential office-based work RVUs (wRVUs) that could have been generated during the global period for surgery by adding the equivalent wRVUs that could have been generated during the equivalent perioperative, intraservice, and postoperative periods based on the following formula:

In the modeling of perioperative-equivalent and intraservice-equivalent office work, the average clinic wRVUs per encounter and the interquartile ranges (IQRs) were based on 2021 data from the Vestrum Healthcare Retinal Database (Vestrum Health, LLC), which consists of data harvested from electronic medical records of 2.04 million patients of 289 retina specialists from 63 geographically diverse practices throughout the US. The aggregated real-world data were analyzed to identify the total wRVUs (inclusive of all evaluation and management [E/M] codes, imaging, procedures, diagnostic testing, etc) coded into the database from January 1, 2021, through December 31, 2021, along with the total number of patient encounters in the same period, which were used to identify the mean and IQRs of wRVUs coded per encounter. The number of office patient encounters per hour was modeled with assumptions and were varied.
The postoperative modeling was based on the potential office productivity that could have been generated instead of the postoperative visits that were included in the global period for surgery. In contrast to the valuation for perioperative and intraservice work, which accounted for all potential office-based work that could have been performed during that time, the valuation for postoperative visits was based on E/M codes for established patient examination visits only (CPT 99211-5, 92012, 92014). New-patient visits were excluded because the physician work associated with postoperative visits was assumed to more closely resemble established patient visits. Ancillary wRVUs from diagnostic testing and procedures were excluded because they could be billed separately in the global period.
The opportunity cost associated with surgery was expressed as a percentage of potential office-based productivity (ie, opportunity cost = 1 − (CMS-allocated wRVUs for surgery)/(potential office-based wRVUs).
In the model for office-based productivity, the reference physician was assumed to manage an average of 40 patients per 8 hours of office-based care and used the mean Vestrum-derived wRVU per encounter and mean wRVU per examination. A lower volume clinician was modeled as seeing 30 patients over 8 hours and used the lower IQR of Vestrum-derived wRVU per encounter and wRVU per examination. A higher volume clinician was modeled as seeing 50 patients over 8 hours with the upper value of the IQR for Vestrum-derived wRVU per encounter and wRVU per examination. A lower productivity clinician and a higher productivity clinician were also modeled according to the above parameters independent of the number of patients seen per day.
To determine the top 10 most common single CPT vitreoretinal surgeries, the 2021 Part B National Summary Data file was used. 9 Trauma and lens cases were excluded because these surgeries may be associated with multiple procedural codes and can be performed by both anterior segment surgeons and posterior segment surgeons. Weighted averages were determined by multiplying the relative proportions of the top 10 most common vitreoretinal surgeries by the average wRVU per CPT code.
Threshold Analyses
Threshold analyses were performed to identify the surgical intraservice time that would render the lost office-based productivity equal to Medicare reimbursements for the reference case and for lower productivity and higher productivity clinicians. Threshold times were obtained by subtracting the perioperative and postoperative wRVUs that could have been generated in the office from the Medicare physician reimbursements for each CPT code, then dividing the remaining wRVUs by the average wRVUs per clinic minute.
Probability Sensitivity Analyses
Probability sensitivity analyses were performed to assess for uncertainty using Monte Carlo simulations with 100,000 2nd-order parameter samples. The model was assessed through a broad range of surgical and clinical conditions. Clinic volumes were varied from 20 to 80 patients, the perioperative and intraservice times were varied from 50% less to 50% more than Medicare allocations, the average wRVUs from office-based productivity were varied from 50% less to 50% more than Vestrum-derived averages, and the number of postoperative visits were varied from 50% less to 50% more than Medicare allocations.
Results
The most frequently billed single retinal surgeries were 67036, 67039, 67040, 67041, 67042, 67107, 67108, 67113, 67120, and 67121 (Table 1). According to Medicare allocations, the weighted mean immediate perioperative time was 34.65 minutes, the weighted mean intraservice time was 72.65 minutes, and the weighted mean number of postoperative visits was 5.12.
Most Common Billed Single CPT Code Vitreoretinal Surgeries. a
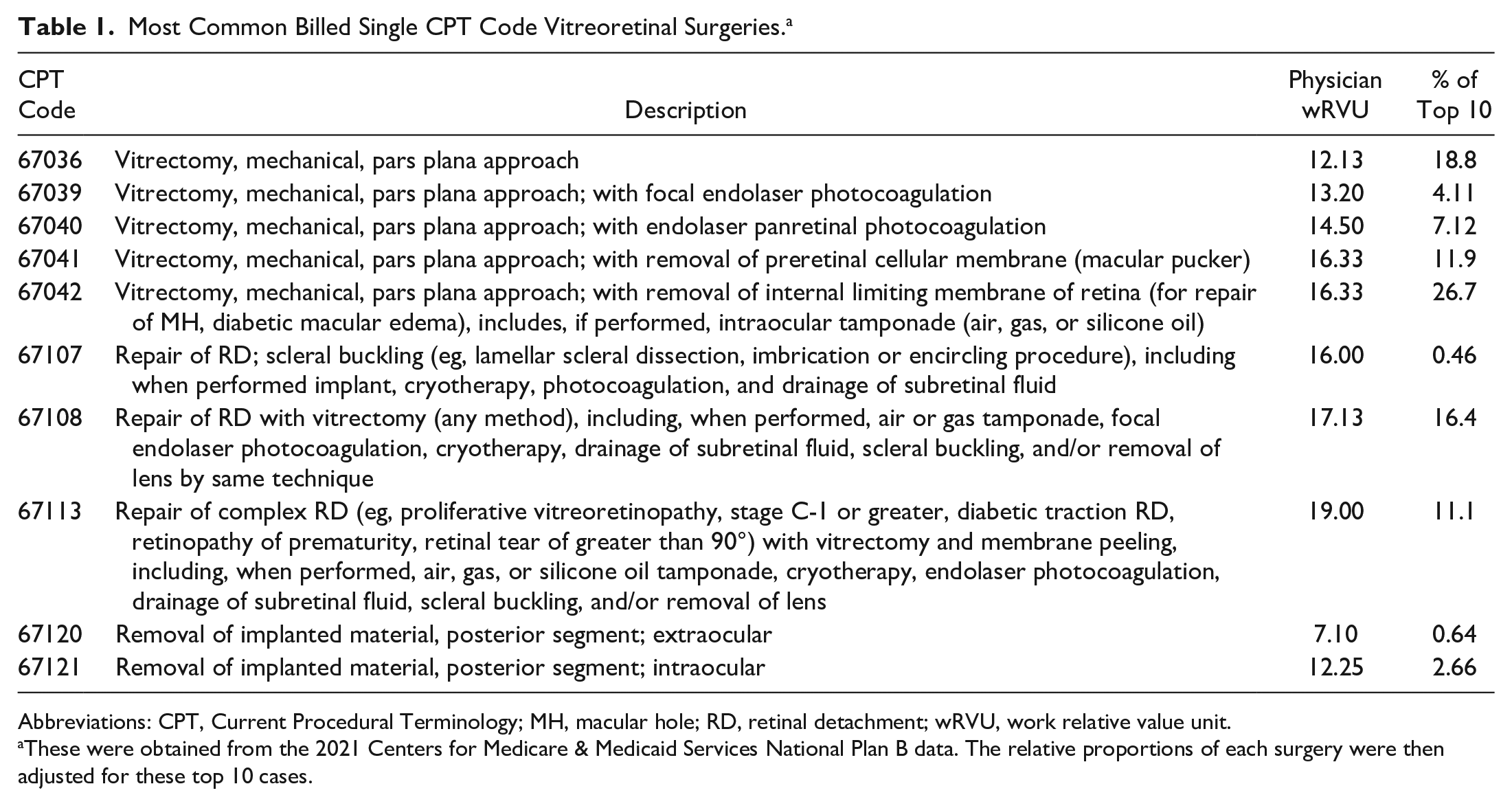
Abbreviations: CPT, Current Procedural Terminology; MH, macular hole; RD, retinal detachment; wRVU, work relative value unit.
These were obtained from the 2021 Centers for Medicare & Medicaid Services National Plan B data. The relative proportions of each surgery were then adjusted for these top 10 cases.
Analysis of the Vestrum database identified a mean of 2.70 wRVUs per office encounter (IQR, 2.44-3.00), which was used to model potential lost office-based productivity during the equivalent perioperative and intraservice period. The lost productivity included all new and established E/M codes of varying levels of intensity along with imaging (eg, optical coherence tomography, fluorescein and/or indocyanine green angiograms, and ultrasounds), diagnostic testing (eg, electroretinograms and visual fields), and office-based procedures (eg, extended ophthalmoscopy; lasers for retinal tears, proliferative diabetic retinopathy, and diabetic macular edema; intravitreal injections; vitreous biopsies; and pneumatic retinopexies).
The Vestrum database also identified a mean of 1.30 wRVUs per any established patient examination visit (IQR, 0.92-1.42), which was used to model potential office-based productivity during the equivalent postoperative 90-day global period.
In the reference case of 40 patients per clinic day, the surgeon could have theoretically generated a weighted average of 30.37 wRVUs (range, 21.35-43.35 wRVUs) in clinic during the equivalent time that they would have been reimbursed a weighted average of 15.63 wRVUs for performing vitreoretinal surgeries and associated care during the 90-day global period. The surgeries therefore represented a weighted average of 49% opportunity cost for the physician (range, 40%-68%). In threshold analyses, the surgeon would have to complete the surgery within a weighted average of 5 minutes to neutralize the opportunity cost of surgery (range, −31-12 minutes). Figure 1 summarizes the weighted averages for Medicare reimbursements compared to potential office-based wRVUs. Figure 2 shows the opportunity cost of surgery compared to the office. Figure 3 compares the threshold surgery times for surgical and office-based reimbursements to equal.
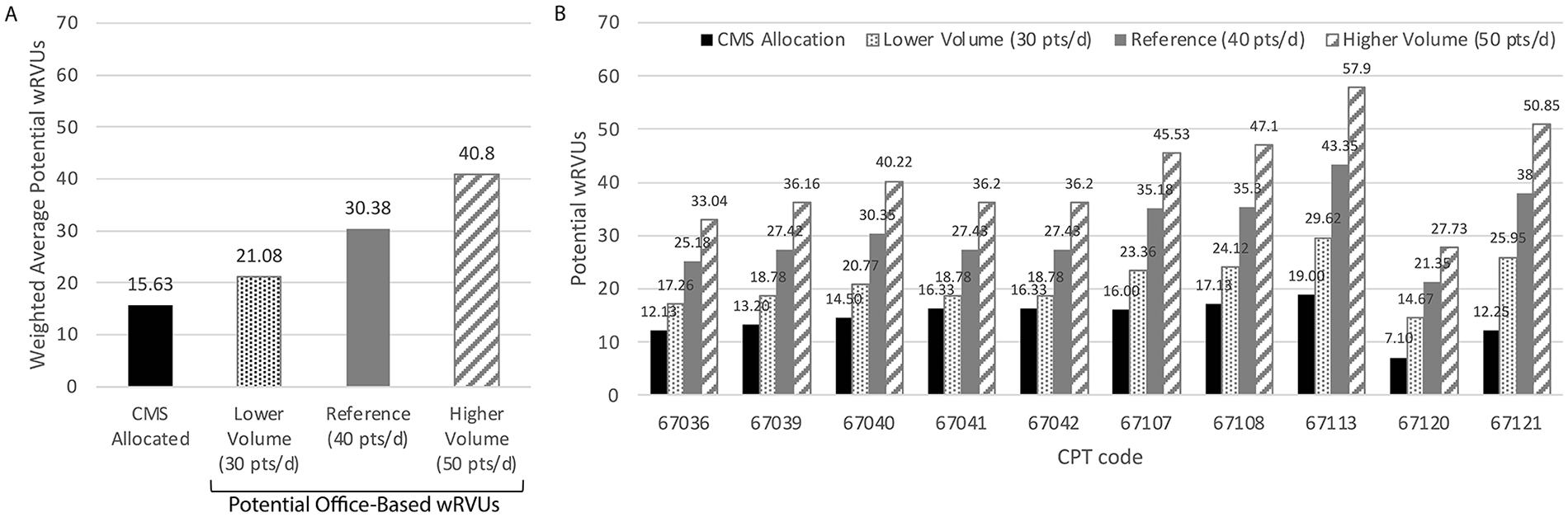
Comparison of vitreoretinal surgery reimbursement with potential office-based reimbursements. The weighted average of surgical reimbursements in wRVUs was less than potential wRVUs that could have been generated in the office during the equivalent time in the 90-day global period by the reference physician as well as a lower volume physician and higher volume physician. For each CPT code, the Medicare reimbursements were less than the potential office-based reimbursements that could have been generated in the global period.
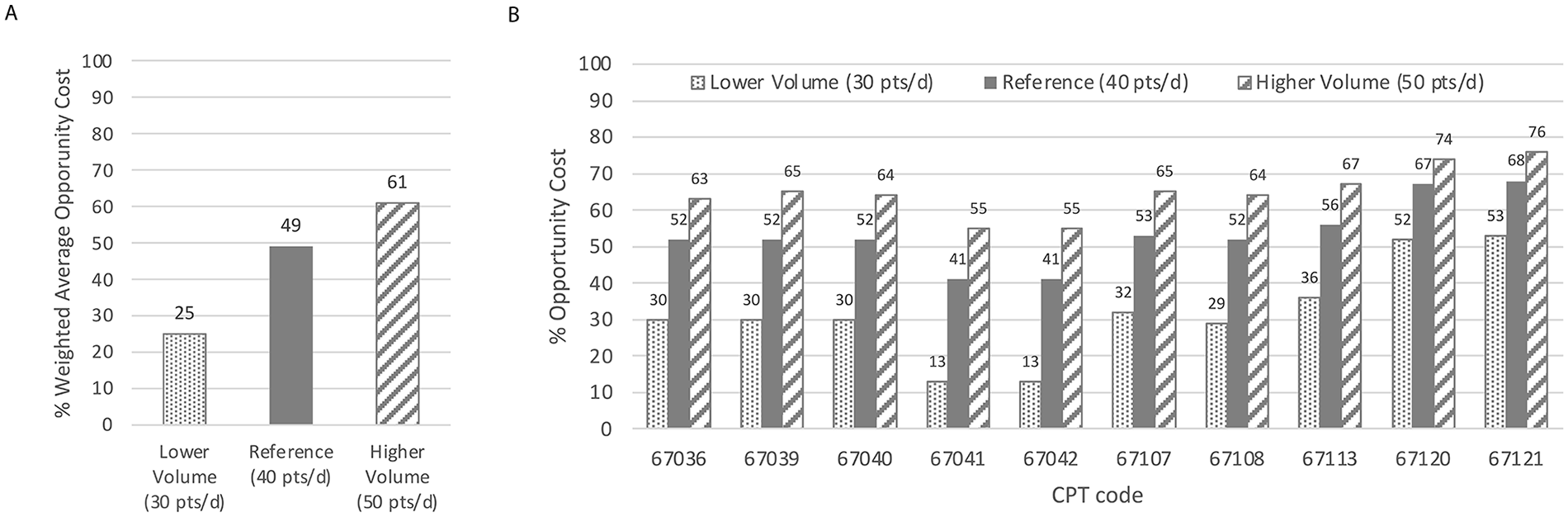
Opportunity cost of surgery. There was a significant opportunity cost (expressed as percentage of potential office-based productivity) for the physician performing the (A) weighted average of the 10 most common vitreoretinal surgeries and (B) for each individual surgery by CPT code for all modeled physicians.
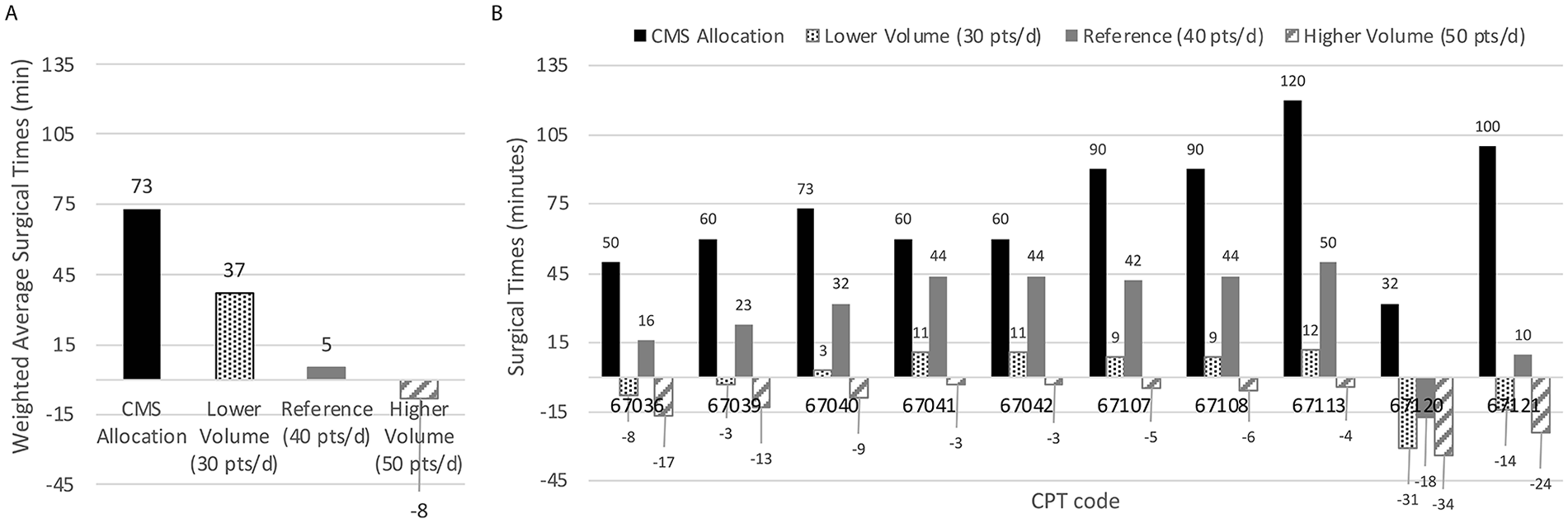
Threshold surgical times. Medicare-allocated intraservice times were greater than (A) the modeled weighted average threshold times for surgical reimbursements to equal clinic reimbursements for the 10 most common surgeries and (B) for each individual CPT code.
For a lower volume surgeon who managed an average of 30 patients per day with an average 2.44 wRVUs per clinic visit and had a lower quartile average of 0.92 wRVU for the postoperative visit equivalent, the surgeon could have generated a weighted average of 21.08 wRVUs (range, 14.67-29.62 wRVUs). Surgery represented a weighted average of 25% opportunity cost (range, 13%-52%) for that physician, who would have to complete the surgery with a weighted average of 37 minutes (range: −17 to 50 minutes) for the surgical reimbursements to equal the office-based reimbursements.
For a higher volume surgeon who managed an average of 50 patients per day and had a higher average of 3.00 wRVUs per clinic visit and a higher average of 1.42 wRVUs for the postoperative visit, the physician could have generated a weighted average of 40.80 wRVUs (range, 27.73-57.90 wRVUs) with a weighted mean opportunity cost of 61% (range, 55%-76%). The surgeon would have a weighted average of −8 minutes to complete the surgery to neutralize the cost of surgery (range, −34 to −3 minutes).
Figure 4A shows the linear relationship between the number of patients per clinic day and the potential wRVUs that could have been generated in the clinic. Figure 4B shows the logarithmic increase in opportunity cost with increasing numbers of patients per day. Figure 4C shows the negative logarithmic decrease in threshold surgical times (for surgical reimbursements to equal office-based reimbursements) with increasing numbers of patients per day. Similar trends were seen with low and high clinical productivity as defined by the IQR of RVUs generated per encounter and per examination according to the Vestrum database.
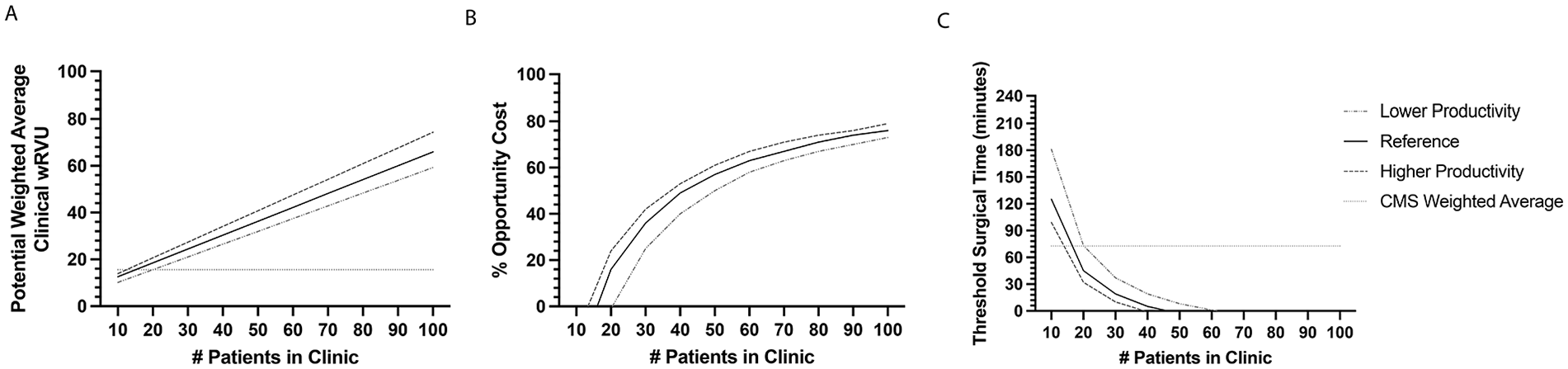
Average wRVU and clinic reimbursements. (A) The relationship between the number of patients per day and the potential clinic wRVU that could have been generated depending on the physician’s productivity per clinical visit. (B) The opportunity cost of surgery relative to clinic reimbursements. (C) The threshold surgery (ie, intraservice) times to neutralize the opportunity cost between surgical and clinical productivity.
The probability sensitivity analyses found that in more than 99% of the clinical scenarios, office-based reimbursements were higher than surgical reimbursements for the same time period, regardless of whether clinic and surgical parameters were varied by 50% and the number of patients varied from 20 to 80.
Conclusions
The most commonly performed vitreoretinal surgeries included a mixture of emergent, urgent, and elective surgeries. In the current study, performing vitreoretinal surgeries represented significant opportunity costs for the physician during the 90-day global period. All surgeries analyzed were associated with opportunity costs, with a weighted average of 49% in the reference case.
The weighted average threshold intraservice time for surgery to equal office-based reimbursement was 5 minutes in the reference case. Threshold times represented a fraction of the total intraservice time allocated by the Relative Value Scale Update Committee (RUC) for these CPT codes and are likely difficult to achieve. In the probability sensitivity analyses, even a 20% to 50% difference in surgical time did not alter the imbalance between surgical reimbursements and clinical reimbursements. A recent review of 108 RUC time estimates across multiple subspecialties found no systematic overestimation or underestimation of the RUC estimated procedural times, with a mean discrepancy of 18.5 minutes (19.8%), 10 suggesting that RUC surgical estimates were relatively accurate.
The disparity between cost and reimbursements for surgery exists in multiple healthcare systems. In the United Kingdom, the direct cost of vitrectomies for macular holes, epiretinal membranes, and vitreomacular traction was higher than the reimbursed costs in 38.6% of cases. 11 In Germany, the cost of more complex inpatient vitrectomies was greater than the reimbursements. 11 In academic ophthalmology departments in the US, the cost of routine vitrectomies was estimated to be $2053.85 more than the Medicare reimbursement. 12
Limitations of the current study include the theoretical nature of the model. The proportion of each vitreoretinal surgery and the average wRVUs may differ based on individual practice patterns. Whenever possible, information was obtained from the large, geographically diverse Vestrum Retinal Healthcare Database to simulate real-world practices; however, coding data may not have reflected actual reimbursements from insurers. The model also assumed that the surgeon would otherwise be in the clinic managing patients; however, the physician could also be returning patient telephone calls, completing uncompensated prior authorization requests, or doing research. The actual average wRVU per clinical visit, the number of patients per hour, and the opportunity cost of surgery may therefore differ from the theoretical reference case.
In addition, the model focused on physician work only and did not include the separately factored costs of professional liability insurance and practice expenses, which each has its own RVU allocation. Practice expenses can account for 45% of total reimbursements, 13 and their impact on the model would depend on their utilization by the practice while the physician is in the operating room instead of the office. The model also did not account for some intangible costs of surgeries, such as the stress and effects on work–life balance, in particular with emergency cases. The model also only applied to uncomplicated surgeries; complications adding to increased operative time and postoperative management would likely further increase the opportunity cost. Hospital and ambulatory surgery center turnover times may vary and differences may also affect the applicability of the model. Furthermore, COVID-19 could have affected the relative proportions of each vitreoretinal surgery performed; however, the probability sensitivity analyses performed with pre-pandemic 2019 data found similar results (data not shown).
In conclusion, performing any of the top 10 most common vitreoretinal surgeries in this model represented a significant opportunity cost for the physician compared with providing office-based patient care. Surgeries were undervalued relative to clinics. Many of the threshold surgical times for surgical reimbursements to equal office-based care might not be achievable. Although physicians are dedicated to providing the best possible medical care to patients, further reductions in surgical reimbursements might potentially disincentive medical students and young physicians from considering a surgical subspecialty and could shift the burden of managing complex cases, such as to academic centers.
Footnotes
Ethical Approval
No human subjects were involved; therefore, institutional review board approval was not required.
Statement of Informed Consent
No human subjects were involved; therefore, informed consent was not required.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.