
Abstract
Introduction
Disparities exist in the care of incarcerated patients. These patients have a higher burden of chronic diseases such as hypertension and asthma compared with the general population, and they are at risk for developing substance use disorders, trauma, infectious diseases such as HIV and hepatitis C, and psychiatric disorders.1–3 There are limited published data on ophthalmic care in incarcerated patients.
A recent study investigating adherence to follow-up in patients with glaucoma reported significantly worse follow-up adherence in incarcerated patients compared with nonincarcerated patients. 4 A significant proportion of incarcerated patients with glaucoma were found to have advanced disease, medication nonadherence, and delayed follow-up. 5
Rhegmatogenous retinal detachment (RRD) is a vision-threatening problem that requires urgent attention for optimal outcomes. Risk factors for RRD include myopia, previous intraocular surgery, lattice degeneration, and trauma. Prompt surgical repair is associated with better visual acuity (VA) outcomes. 6
There are few systematic studies on RRD in incarcerated patients, an understudied population in ophthalmology. The University of California, Davis Medical Center is a major referral center for incarcerated patients in Northern California. In this study, we describe the characteristics of incarcerated patients with RRD treated at our institution and report outcomes of surgical repair.
Methods
This case series was conducted at University of California, Davis Health. The study was reviewed and approved by the University of California, Davis Office of Human Research Institutional Review Board (IRB). Patient consent was waived given the retrospective nature of the study.
The electronic medical record (EMR) was used to identify incarcerated patients seen at the Department of Ophthalmology & Vision Science between January 1, 2012, and December 1, 2022, who underwent retinal detachment repair. These patients were identified by insurance status, as they are insured by the Department of Corrections in the State of California.
International Classification of Diseases (ICD) codes were used to identify incarcerated patients who underwent vitrectomy, scleral buckling, combined vitrectomy and scleral buckling, or pneumatic retinopexy. Medical records were reviewed to confirm diagnosis of RRD and attempted repair by one of the aforementioned surgical procedures. Demographic and clinical characteristics were collected. Single-surgery success was defined as successful reattachment of the retina for a minimum of 3 months following a single surgical procedure.
Paired t tests were performed to compare means for paired samples. Fisher exact tests were performed to determine associations between categorical variables. Statistical significance was set at P ≤ .05. Mean values are ± SD. Statistical analysis was performed using Stata version 17.0 (StataCorp).
Results
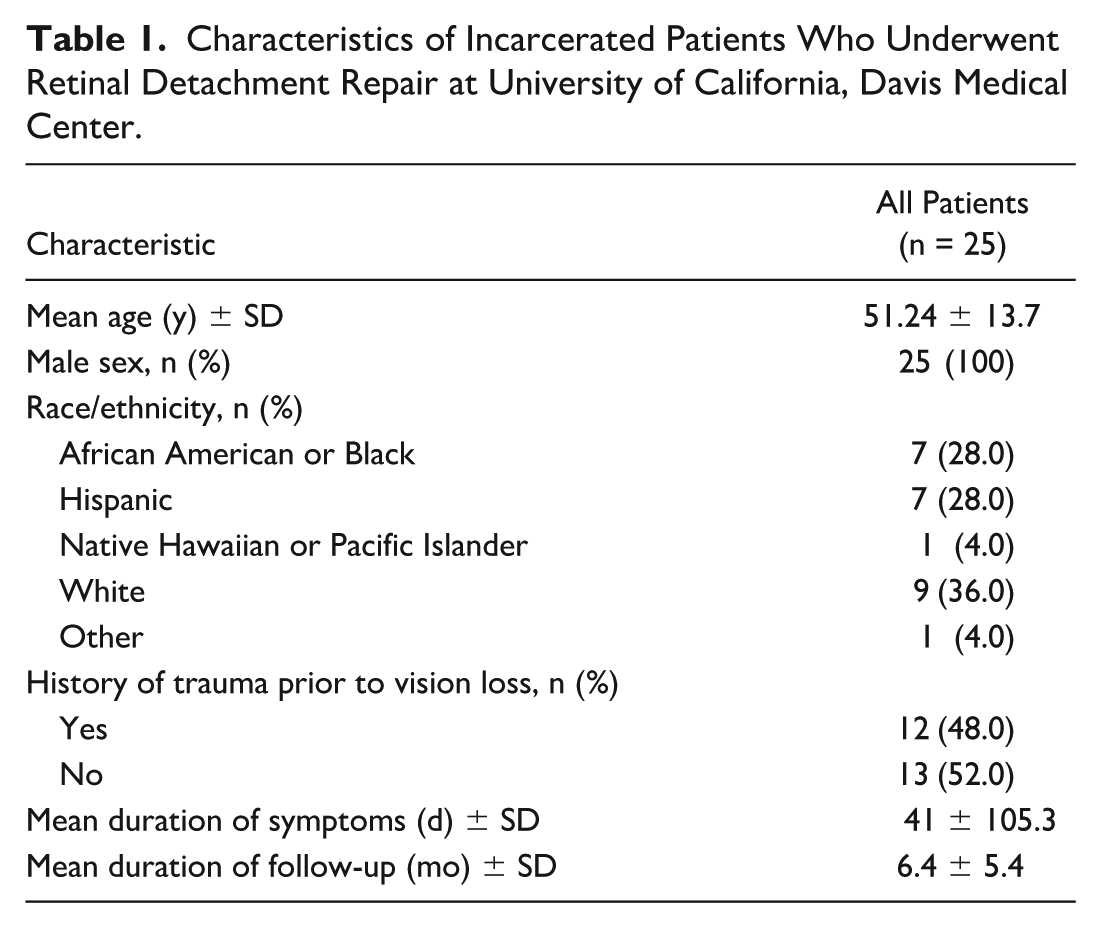
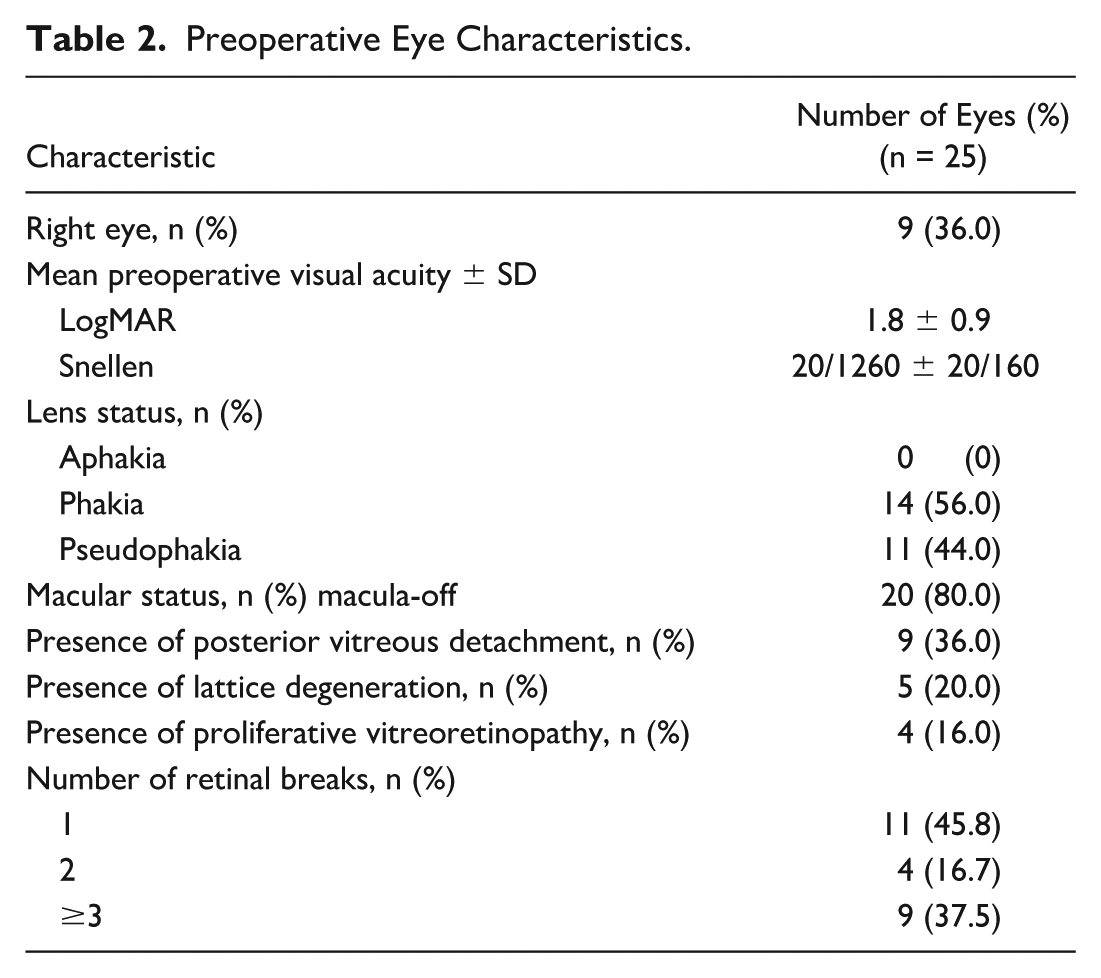
Twenty-five eyes of 25 patients were included in this study. All (100%) were male, and mean age was 51.2 ± 13.7 years. Mean follow-up was 6.4 ± 5.4 months. On average, 2.88 appointments were missed by each patient. Patient characteristics are described in Table 1, and preoperative eye characteristics are described in Table 2. Three patients in this group had scleral buckle as primary surgery, while 5 patients had intraoperative retinectomy.
Characteristics of Incarcerated Patients Who Underwent Retinal Detachment Repair at University of California, Davis Medical Center.
Preoperative Eye Characteristics.
Sixteen patients (64%) had follow-up of 3 months or more. In this group, logMAR VA improved from a mean of 1.9 ± 0.2 (Snellen equivalent, 20/1600 ± 20/30) preoperatively to a mean of 1.3 ± 0.2 (Snellen equivalent, 20/400 ± 20/30) postoperatively (mean difference, 0.5; P = .034) at last follow-up (mean, 9.4 ± 4.5 months).
Three patients had a macula-on RRD, and VA declined from a mean of 0.5 ± 0.1 (Snellen equivalent, 20/60 ± 20/25) preoperatively to a mean of 1.1 ± 0.5 (Snellen equivalent, 20/250 ± 20/60) postoperatively at last follow-up (mean follow-up, 15 ± 3.6 months); this difference was not statistically significant (mean difference, 0.7; P = .247).
Thirteen patients had a macula-off RRD and VA improved from a mean of 2.2 ± 0.2 (Snellen equivalent, 20/3170 ± 20/30) preoperatively to a mean of 1.4 ± 0.2 (Snellen equivalent, 20/500 ± 20/30) postoperatively (mean difference, 0.8; P = .002) at last follow-up (mean follow-up, 8.1 ± 3.7 months).
Seven of 25 patients had retinal redetachment, and 6 of 7 patients were symptomatic for more than a week, suggesting delayed presentation. Additionally, 4 of these patients had missed appointments prior to their redetachments.
Single-surgery success was achieved in 9 eyes (56.3%) with minimum follow-up of 3 months. Table 3 compares achievement of single-surgery success by surgery type. There was no significant relationship between initial procedure type and single-surgery success (P = .498). Tamponade was utilized in 15 eyes (93.8%).
Single-Surgery Anatomic Success by Surgery Type.

Abbreviations: PPV, pars plana vitrectomy; SB, scleral buckle.
Sulfur hexafluoride (SF6) gas was used in 2 eyes (12.5%), perfluoropropane (C3F8) gas in 9 eyes (56.25%), and silicone oil in 4 eyes (25.0%). No significant relationship was noted between choice of tamponade and single-surgery success (P = .148). All 25 eyes (100%) were attached at last follow-up (mean follow-up, 6.4 ± 5.4 months; range, 0.5-19 months).
Conclusions
Ophthalmology is one of the most requested services by incarcerated patients, a vulnerable and understudied patient population. 7 There are limited published data on clinical outcomes in ophthalmology in these patients. In this study, we describe the clinical characteristics and outcomes of incarcerated patients with RRD treated at our institution, a major referral center for incarcerated patients in Northern California.
We note several outcomes that raise concern. More than one-third of these patients had less than 3 months of follow-up, single-surgery success is lower than what is reported in the general population in other series, and while all patients had retinal reattachment at their final visit, the VA improvement was modest.8,9
Several findings may explain these results. Eighty percent of our patients presented with macula-off RRDs with correspondingly poor VA on presentation. A recent study found improved VA outcomes for macula-off RRDs repaired within 2 to 3 days of macular detachment compared with 4 days or more. 6
On average, the patients in this series presented with more than 40 days of RRD-related symptoms. Nearly 50% reported a history of trauma, and 16% were found to have proliferative vitreoretinopathy—indicating complex RRD—on presentation. These factors likely contributed significantly to the suboptimal outcomes reported in this series.
While incarcerated, patients experience significant challenges in obtaining prompt and adequate care. They may have restricted access to medical services due to limited healthcare providers, infrequent medical visits, or logistical barriers within the facility. Inmates can face long wait times for appointments or delays in receiving medications. 10 The process for requesting medical care can also be very slow, which may also be due to overcrowding. 11
Prisons may also have inadequate medical equipment, which can also compromise the quality of care provided. Additionally, medical consultations in prisons may lack confidentiality, which can discourage inmates from seeking medical attention. In some systems, inmates may have to pay for certain services or medications, which can be a barrier if they cannot afford the costs. 12 A patient experiencing symptoms of retinal detachment may not be seen quickly due to the slow process or may delay seeking care due to concerns of confidentiality or costs.
Following incarceration, ex-offenders face challenges in securing gainful employment, and when employment is secured, most obtain employment in manufacturing (21.66%), construction (19.89%), accommodation and food services (16.62%), and administrative and support services (14.28%). 13 Employment following incarceration has been associated with lower rates of recidivism; in particular, jobs with higher occupational level reduce crime rates among high-risk offenders. 14 It is well known that decreased vision is associated with unemployment. 15 Thus, maintaining adequate vision is likely to help ex-offenders obtain employment and remain out of prison.
This study is limited by the biases inherent to its retrospective nature, reliance on the accuracy of the EMR, and limited sample size, which likely limits our ability to detect differences in outcome between the various procedures performed. The small sample size and limited number of patients with 3 months of follow-up or more limits the generalizability of our results. In addition, while these patients were incarcerated at the time of surgery at our institution, it is possible that some were released from incarceration shortly after surgery and received follow-up care elsewhere, unbeknownst to us. We acknowledge the results may not be representative of all incarcerated patients.
Delayed treatment for vision-threatening diseases, such as retinal detachment, may have negative consequences on ex-offenders’ ability to obtain employment and successfully reintegrate into society. Our results highlight the importance of not only prompt ophthalmology evaluation, but necessary structural changes in the medical correctional system that can improve access to medical care, improve referral time, and adherence to follow-up for this unique patient population. Future studies to better understand the systemic factors that may result in treatment delays for these patients may improve surgical outcomes.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in a Health Insurance Portability and Accountability Act (HIPAA)-compliant manner.
Statement of Informed Consent
The study was reviewed and approved by the University of California, Davis Office of Human Research, Institutional Review Board. Patient consent was waived given the retrospective nature of the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.