
Abstract
Introduction
Extensive macular atrophy with associated pseudodrusen (EMAP) is a rare retinal disease first described by Hamel and colleagues 1 in 2009. EMAP is characterized by symmetric macular atrophy occurring bilaterally, with the vertical axis being larger than the horizontal, as well as pseudodrusen, which is spread throughout the retina. Sporadically, a pavingstone pattern of degeneration appears in the far periphery. The progression of the atrophy is rapid, and significant visual loss occurs in the early stages of the disease, as previously reported by Querques et al. 2 In the initial case series described by Hamel et al, the scotopic and photopic electroretinography responses were reduced in patients diagnosed with EMAP, and none of the patients showed signs of choroidal neovascularization (CNV). 1
This entity is particularly relevant as a differential diagnosis of age-related macular degeneration (AMD), which is one of the most prevalent retinal diseases, with an estimated prevalence of 1.4 per 1000 individuals ages 60 years and older. 3 EMAP differs from AMD in that it affects a younger age group, with onset around the age of 45 years, and there is an absence of hard and soft drusen, a typical feature of AMD. Both CNV and subretinal neovascularization are well described in exudative cases of AMD. Neovascularization primarily arises as a result of hypoxia, which triggers the upregulation of vascular endothelial growth factor (VEGF) and other angiogenic factors.
The use of antiangiogenic agents in patients with CNV or subretinal neovascularization is based on the pivotal role of VEGF in the development of these conditions. 4 Anti-VEGF agents, such as bevacizumab, ranibizumab, and aflibercept, work by directly inhibiting VEGF, thereby reducing both neovascular growth and vascular leakage. This process helps prevent further retinal damage, leading to stabilization or even improvement of vision. 5 In the initial series reported by Hamel et al, 1 none of the patients diagnosed as having EMAP showed signs of CNV.
There is a reported association of EMAP with a history of rheumatic fever and the use of benzathine penicillin. 6 In this report, we present a case series of patients diagnosed with EMAP who developed CNV, the largest case series described to date. We focused on the patients’ demographics, visual function, and medical history, including a history of rheumatic fever and morphologic features of CNV.
Methods
This study was approved by the institutional ethics and research committee of H.Olhos Paulista. All patients provided written informed consent upon admission to the clinic. The research was conducted as a retrospective analysis of medical records. No additional interventions or data collection were performed beyond standard clinical practice.
A total of 87 patients with EMAP were evaluated at our clinic. Patient records were retrospectively reviewed to determine study eligibility. Chart screening was performed by ophthalmologists in their first year of retina fellowship. Patients evaluated between 2011 and 2024 were considered for inclusion. The diagnosis and categorization of EMAP were determined by 2 experienced retina specialists, who based their evaluation on several key factors: early-onset geographic atrophy, the presence of pseudodrusen, peripheral retinal degeneration presenting in a pavingstone pattern, and a history of rheumatic fever and/or prolonged use of benzathine penicillin. Patients were excluded if they had a genetic test positive for AMD or if they exhibited typical drusen along with geographic atrophy with a later onset (particularly in individuals older than age 65 years) and had no history of rheumatic fever or benzathine penicillin use. These criteria were applied to clearly distinguish EMAP from typical AMD, ensuring the accuracy of the study population.
Among the cases screened, 15 eyes of 10 patients presented with CNV (Table 1). These patients were assessed by 2 experienced retina specialists and underwent widefield fundus photography, fundus autofluorescence imaging (Optos; Silverstone), and/or optical coherence tomography (OCT) (Cirrus 6000; Zeiss) or OCT angiography (OCTA) (Spectralis HRA; Heidelberg Engineering).
Demographic and Clinical Characteristics of Patients with Extensive Macular Atrophy With Pseudodrusen and Choroidal Neovascularization (10 Patients, 15 Eyes). a
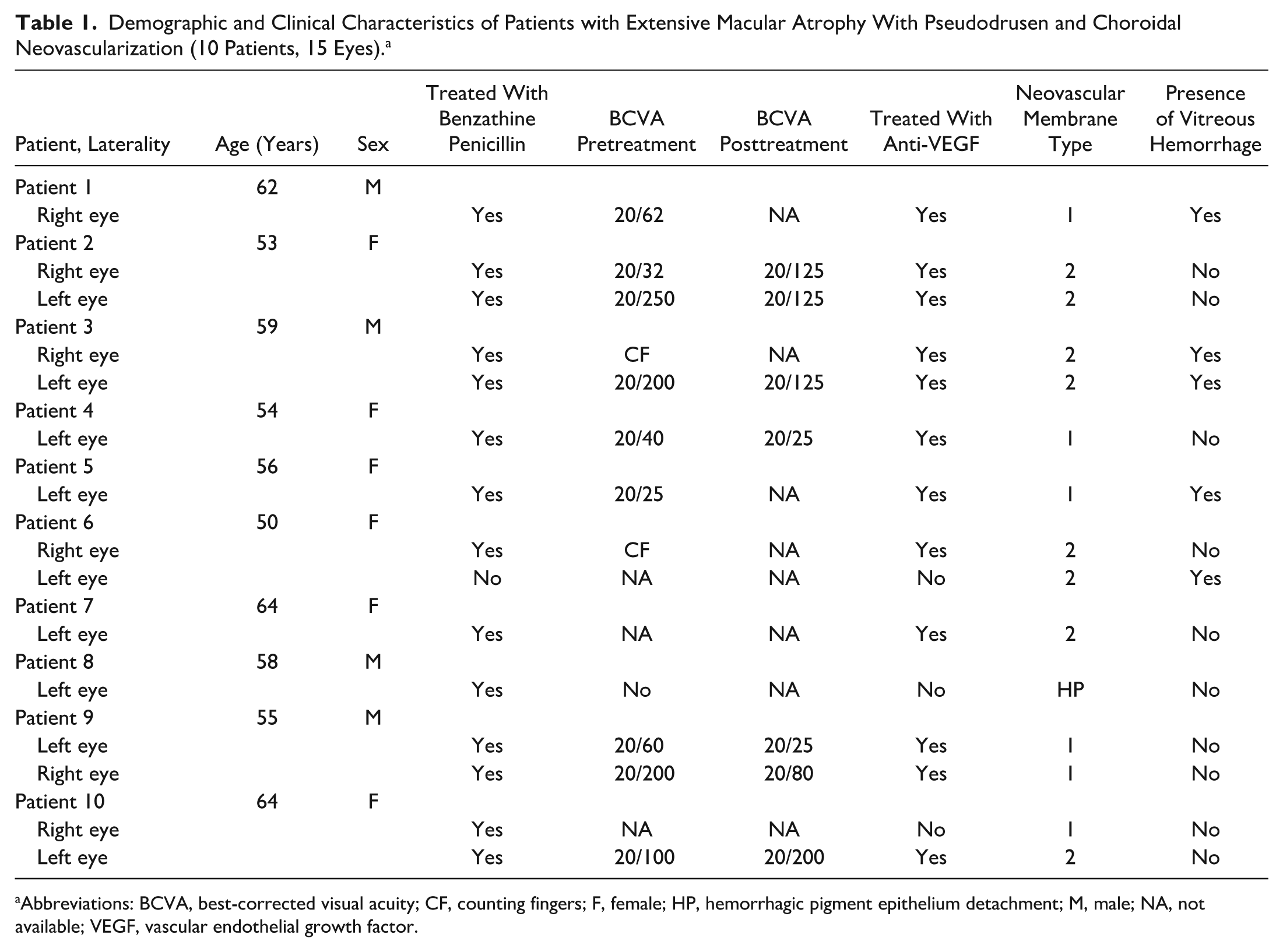
Abbreviations: BCVA, best-corrected visual acuity; CF, counting fingers; F, female; HP, hemorrhagic pigment epithelium detachment; M, male; NA, not available; VEGF, vascular endothelial growth factor.
Results
Among the 10 patients presenting with CNV, 3 were male, and 7 were female, and the mean age at the initial visit was 57 years (range, 50–64 years). All patients had a history of rheumatic fever in childhood. Of the 10 patients, 4 had documented information regarding the duration of penicillin treatment (mean duration of use 13 years). Notably, because of the prolonged treatment duration and the young age of the patients at the time of treatment, specifying the exact number of doses administered to each patient was challenging.
Of the 10 patients included in the analysis, 9 had documented information regarding the use of anti-VEGF medications. The majority of eyes (7 eyes, 7 patients) were treated exclusively with aflibercept. Since EMAP is a rare disease, there is no robust scientific evidence or studies suggesting that aflibercept should be used preferentially over other anti-VEGF agents. In this context, the more frequent use of aflibercept as a treatment choice likely reflects the individual preference of the treating surgeon, rather than being based on definitive clinical guidelines. Two eyes (2 patients) were treated with ranibizumab. One of these patients received ranibizumab in combination with aflibercept and faricimab, possibly reflecting therapeutic adjustments based on the individual patient’s responses.
Regarding the number of injections administered over the study period, complete information was available for 10 eyes. The mean number of injections per eye was 8, with a minimum of 1 application recorded and a maximum of 18. Information about the number of visits for each patient was also collected for a total of 10 eyes. The number of visits varied significantly, ranging from a minimum of 3 visits to more than 100 visits for 1 patient. The mean number of visits was ~27; other recorded values included 16 visits for 2 patients, and 35 visits for 3 patients.
In this study, we analyzed the classification of neovascular membranes in the 15 eyes affected. The CNV classification into type 1 or type 2 was determined based on OCT and OCTA findings obtained at the initial visit, when CNV was first detected.
The classification of CNV into type 1 or type 2 followed the criteria established by Spaide et al 7 , with subsequent confirmation using OCTA and multimodal imaging (Figure 1, A–L). Type 1 CNV (occult) was defined as sub–retinal pigment epithelium (sub-RPE) neovascular proliferation, typically presenting on OCTA as an ill-defined, low-flow vascular network beneath the RPE. Type 2 CNV (classic) was identified as neovascularization in the subretinal space above the RPE, appearing as a well-defined, high-flow lesion with loops and a dense capillary network in the outer retina.
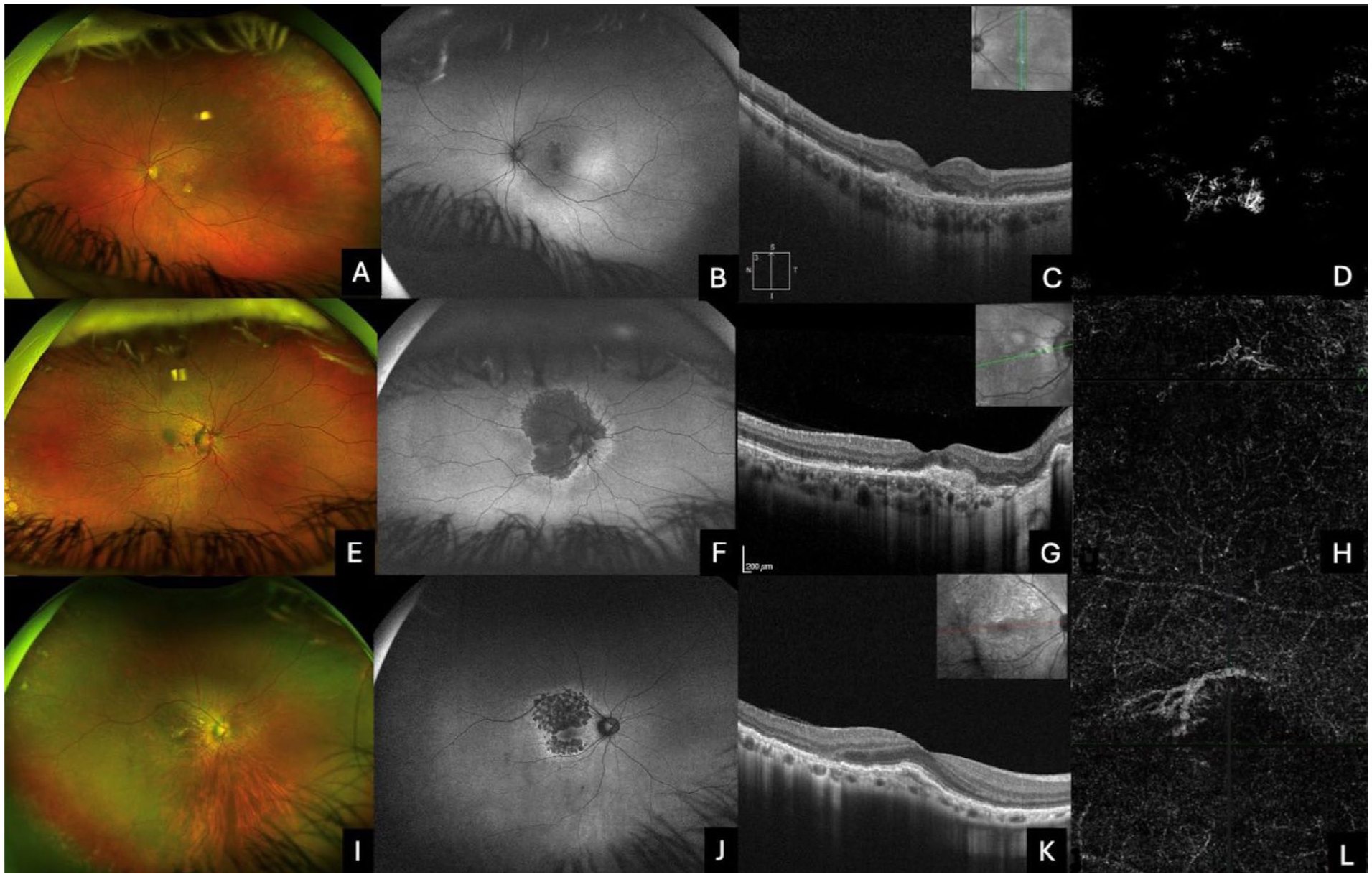
Characteristics of extensive macular atrophy with pseudodrusen and choroidal neovascularization in (A–D) left eye of patient 6, (E–H) right eye of patient 10, and (I–L) right eye of patient 2. (A, E, I) Fundus photographs show features of macular atrophy. (B, F, J) Corresponding autofluorescence images show extensive hypoautofluorescence bordered by areas of hyperautofluorescence in the macula. (C, G, K) Optical coherence tomography (OCT) demonstrates the presence of a subretinal fibrovascular lesion, indicative of either a (C) type 2 neovascular membrane or (G, K) type 1 neovascular membrane. (D, H, L) OCT angiography confirms these findings in the outer retina/choriocapillaris layer.
Among the 15 eyes assessed, a total of 7 eyes (46.7%) were identified as having type 1 neovascular membranes, characterized by sub-RPE vascular proliferation (Figure 1G, 1H, 1K, and 1L). Conversely, 7 eyes (46.7%) demonstrated type 2 neovascular membranes (Figure 1C and 1D), defined by the presence of neovascularization located above the RPE and beneath the neurosensory retina. One eye had no description regarding CNV type.
Conclusions
EMAP is a rare retinal disorder that is primarily characterized by macular atrophy (Figure 1A and 1B, 1E and 1F, and 1I and 1J), which significantly impacts vision and may lead to development of CNV, a clinically important complication. In this retrospective study, we evaluated 87 patients diagnosed with EMAP, focusing on 15 eyes of 10 patients with CNV. Patients underwent widefield fundus photography, autofluorescence imaging, and OCT or OCTA, with the findings revealing type 1 CNV in 46.7% of cases (sub-RPE vascular proliferation) and type 2 CNV in 46.7% of cases (neovascularization above the RPE).
Neovascularization is driven by retinal hypoxia, which upregulates VEGF and other angiogenic factors, contributing to disease progression.2,8 Given the retrospective design and limited sample size of our study, we did not aim to compare the efficacy of specific anti-VEGF agents. The choice of medication was based on individual physician preference, availability, or prior treatment history rather than a standardized protocol. Therefore, we have intentionally refrained from drawing conclusions about the superiority or preference for any particular agent, as our data do not support such comparative analysis.
There are only a few studies in the medical literature that explore the association between CNV and EMAP. The largest case series reported in prior literature was in a study by Kamami-Levy et al, 9 in which CNV in 4 eyes of 3 patients, from a total of 19 cases with confirmed EMAP, was assessed. Similar to our findings, Kamami-Levy et al 9 noted a predominance of the disease in female patients. In our study, 7 of 10 patients were female. All patients in their study developed type 2 neovascular membranes. In our series, 7 eyes (46.7%) exhibited type 1 CNV membrane, also known as occult neovascularization, as confirmed on OCT, while the remaining 7 eyes (46.7%) had type 2 CNV membrane. One eye had no information about the CNV type. To our knowledge, this is the largest retrospective case series published to date on this condition.
Parodi and colleagues 10 described a 55-year-old patient with a juxtafoveal neovascular membrane confirmed by OCT, autofluorescence, and fluorescein angiography. Although the membrane classification was not specified, the authors suggested that its morphology resembled that seen in the wet form of AMD. Romano et al 11 reported a case of a 54-year-old patient with a type 2 neovascular membrane. In our series, all patients had a history of childhood rheumatic fever and use of benzathine penicillin, a finding not mentioned in previous studies describing the presence of neovascularization in EMAP patients.
Regarding antiangiogenic treatment, 7 eyes (46.7%) in our series were treated exclusively with aflibercept, 1 eye (6.7%) with ranibizumab alone, and 1 eye (6.7%) with a combination of aflibercept, ranibizumab, and faricimab, while 3 eyes (20%) had incomplete treatment information from other centers. The other 3 eyes did not receive treatment. In the study by Kamami-Levy et al, 9 2 patients received ranibizumab injections, which resolved membrane activity but did not improve visual acuity; 1 patient underwent focal laser therapy, followed by ranibizumab injection, resulting in a slight improvement in visual acuity. In the study by Romano et al, 11 after a patient received 1 bevacizumab injection, visual acuity improved from 20/400 to 20/200 with stability at 2 months. In the study by Parodi and Querques, 10 7 bevacizumab injections were administered, though no final visual acuity was reported. Those authors suggested that antiangiogenic medication could stabilize the ocular condition. In our series, visual improvement was observed in 5 eyes (33.3%). An eye treated with aflibercept demonstrated an improvement in visual acuity from 20/200 to 20/125. Another eye, which received combination treatment with aflibercept, ranibizumab, and faricimab, showed an improvement from 20/40 to 20/32. Furthermore, 2 eyes treated exclusively with aflibercept experienced gains in visual acuity, improving from 20/200 to 20/80 and from 20/60 to 20/25, respectively. An additional eye treated solely with aflibercept improved from 20/200 to 20/100. Two eyes (13.3%) experienced worsening visual acuity, with 1 eye (treated with ranibizumab alone) worsening from 20/62 to 20/125, and another eye (with unknown medication) worsening from 20/32 to 20/125. No improvement or deterioration in visual acuity was noted for the remaining patients.
The relationship between rheumatic fever and EMAP, though not conclusively defined, points to a possible autoimmune influence on EMAP’s onset. Studies have shown that rheumatic fever, an inflammatory condition arising from streptococcal infections, may lead to antibodies that mistakenly attack retinal tissue due to similar epitopes between streptococcal antigens and retinal structures.
In our retrospective case series, a history of rheumatic fever and prolonged use of benzathine penicillin were assessed via chart review. All 10 individuals who developed CNV reported taking benzathine penicillin as prophylaxis for rheumatic fever—a practice commonly prescribed to prevent recurrent streptococcal infections and mitigate the risk of cardiac involvement. Although patient recall was the primary source of this information, and no official documentation was available to confirm treatment details, 5 patients reported a duration of treatment averaging 13 years. In the remaining 5 patients, duration was not specified in the medical records.
In a Brazilian cohort, a high proportion of EMAP patients had previous rheumatic fever and long-term benzathine penicillin treatment, suggesting a possible link that merits additional investigation. While more research is required to confirm causation, these findings imply that a history of rheumatic fever might be a risk factor for EMAP, potentially driven by immune system cross-reactivity and inflammation. 6
The distribution of neovascular membrane types observed in this study, with 7 eyes (46.7%) exhibiting type 1 neovascularization and 7 eyes (46.7%) presenting type 2, aligns with existing literature on CNV classifications. Type 1 CNV, also known as occult neovascularization, is characterized by neovascular growth beneath the RPE, while type 2 CNV, or classic neovascularization, involves neovascularization that penetrates the RPE into the subretinal space. 12 The equal distribution of these types in our case series underscores the heterogeneity of CNV presentations and highlights the importance of OCT and OCTA to accurately identify and differentiate these subtypes. Accurate classification can help us understand the possible prognostic indicators, given that type 1 and type 2 CNV may respond differently to treatment modalities.13,14
This study has limitations, as expected, because of its retrospective analysis of imaging and clinical data, leading to incomplete information regarding visual acuity and the specific anti-VEGF drugs used for some patients. Additionally, although multimodal imaging was available for all patients, the imaging equipment used was not consistent across cases. Another limitation is the patients’ mean age of 57 years, and the onset of rheumatic fever in childhood, which may have affected the accuracy of recalling medical history and treatment details.
These findings demonstrate that EMAP can evolve to both CNV and retinal neovascularization. To the best of our knowledge, this retrospective study represents the largest case series of CNV in patients with EMAP reported to date in the literature. Given the potential of CNV to significantly worsen visual acuity and, consequently, the quality of life for EMAP patients, we understand that patients must be followed up for this complication and carefully considered in clinical management.
Footnotes
Authors’ Note
All resources utilized in the execution of this work were provided by the authors. The authors affirm their responsibility for the accuracy, validity, and integrity of the content presented.
Ethical Approval
This study was approved by the institutional ethics and research committee of H.Olhos Paulista under the CAAE number 79745424.6.0000.9867.
Statement of Informed Consent
All patients provided written informed consent upon admission to the clinic. The research was conducted as a retrospective analysis of medical records. No additional interventions or data collection were performed beyond standard clinical practice.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of AI Assistance
Artificial intelligence (AI) was utilized during the preparation of this manuscript to assist in text revision. Specifically, the AI tool provided support in refining the language, improving grammar, and enhancing the structural coherence of the text to ensure clarity and adherence to high academic standards. Importantly, no substantive alterations were made to the scientific content, methodology, results, or conclusions presented. The authors remain fully accountable for the accuracy, validity, and integrity of all the information and interpretations contained in the article. The utilization of AI in the editorial process was in alignment with ethical standards, ensuring transparency and consistency in manuscript preparation.