
Abstract
Introduction
Retinal pigment epithelium (RPE) tears were first described by Hoskin et al in 1981. 1 The precise mechanisms underlying RPE tear formation remain unclear. Two principal hypotheses have been proposed: hydrostatic and mechanical. In the hydrostatic model, a pigment epithelial detachment (PED) reaches a critical height of approximately 500 µm, at which point intralesional hydrostatic pressure exceeds the tensile strength of the RPE intercellular adhesions, resulting in a tear.2,3 In the mechanical model, contraction of an underlying choroidal neovascular membrane (CNV)—either spontaneous or after antivascular endothelial growth factor therapy—generates shear stress at the junction of the detached and adherent RPE, leading to tearing.3,4
RPE tears most commonly occur in the setting of CNV secondary to age-related macular degeneration, classically after antivascular endothelial growth factor therapy or photodynamic therapy; however, they may also develop spontaneously. 5 Other associations include central serous chorioretinopathy (CSCR), massive subretinal hemorrhage, ocular trauma, and Vogt–Koyanagi–Harada disease.2,6,7 A limited number of case reports have identified RPE tears occurring secondary to exudation in the context of hypertensive choroidopathy.8–10 In these reports, the tears were noted to originate at or near the macula.
In this report, we describe a unique case of a massive RPE tear following an acute hypertensive emergency superimposed on chronic CSCR. We also review the literature on RPE tears associated with hypertensive choroidopathy and discuss the underlying pathophysiologic mechanisms.
Case Report
A 55-year-old man with a history of systemic hypertension and iron deficiency anemia presented to the Wills Eye Emergency Department with a 24-hour history of acute vision loss in the right eye. On presentation, his blood pressure was 215/130 mm Hg, requiring emergent admission for blood pressure control. He reported nonadherence to his prescribed amlodipine for 3 days. Initial examination revealed a visual acuity (VA) of counting fingers (CF) in both eyes. Intraocular pressure was 14 mm Hg in the right eye and 15 mm Hg in the left eye. Anterior segment examination demonstrated clear media with 1+ nuclear sclerotic cataracts in both eyes and no anterior chamber inflammation.
Posterior segment examination of the right eye revealed a macula-off serous retinal detachment extending from 3 to 10 o’clock with shifting subretinal fluid (SRF). In the left eye, examination demonstrated macular scarring and a serous retinal detachment extending from 4 to 9 o’clock, also with shifting fluid. Scleral depression examination revealed no identifiable retinal breaks in either eye. Retinal vessels in both eyes showed copper wiring and increased tortuosity. The patient’s hypertension was successfully controlled over 3 days with amlodipine and hydralazine, and he was subsequently discharged in stable condition.
At 1-week follow-up in the retina clinic, a history and review of systems were obtained, and multimodal imaging was performed. The patient reported a prior evaluation by an ophthalmologist 10 years earlier for presumed bilateral “retinal detachments,” for which focal laser treatment was performed with subsequent visual improvement. The review of systems was unremarkable. He denied immunocompromised status and exogenous steroid use, including topical and inhaled corticosteroids as well as anabolic-androgenic steroids. Laboratory evaluation from the recent inpatient admission, including complete blood count, complete metabolic panel, rapid plasma reagin, fluorescent treponemal antibody absorption, angiotensin-converting enzyme, and lysozyme levels, was unremarkable. Chest radiography was also unremarkable.
Best-corrected VA was CF at 1 foot in the right eye and CF at 4 feet in the left eye. Intraocular pressure was 11 mm Hg in the right eye and 13 mm Hg in the left eye. Posterior segment examination demonstrated improved inferior serous retinal detachments (Figure 1, A–D). Optical coherence tomography (OCT) of both eyes demonstrated SRF associated with PEDs, with marked choroidal thickening, focal RPE attenuation, and RPE atrophy, indicating chronic fluid leakage from the choroid (Figure 2). A massive RPE tear was noted in the right eye, extending from the temporal periphery through the macula, with a rolled RPE flap displaced superotemporally. In the left eye, 2 smaller RPE tears were present in the temporal macula. An intravitreal faricimab injection was administered in the left eye.
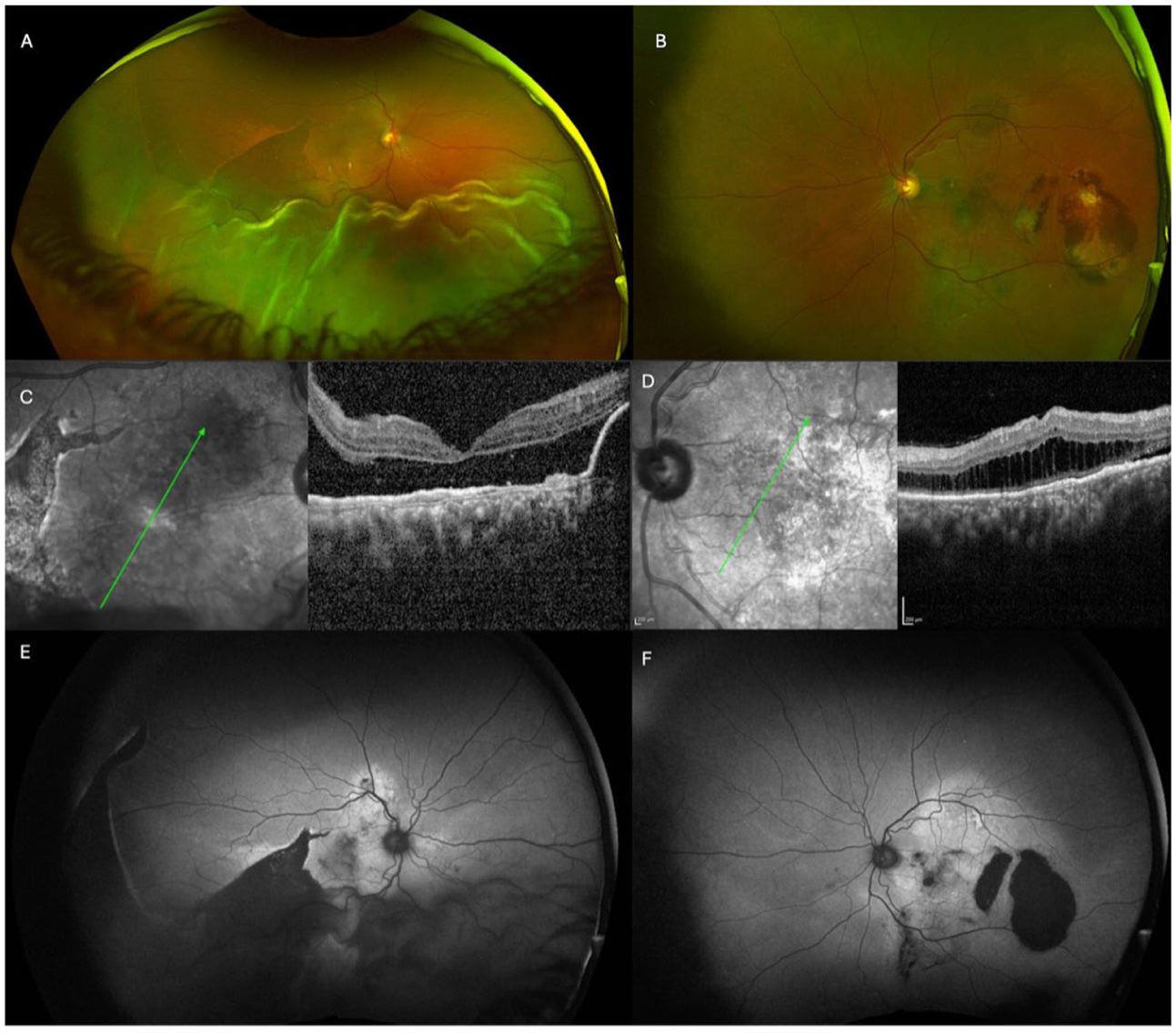
(A) Color fundus photograph of the right eye demonstrating a large retinal pigment epithelium (RPE) tear. (B) Color fundus photograph of the left eye showing an asymmetric RPE tear with multiple areas of RPE atrophy. (C) Oblique optical coherence tomography (OCT) raster of the right eye demonstrating an RPE tear with associated subretinal fluid (SRF). (D) OCT of the left eye showing RPE atrophy and intraretinal fluid with mottling suggestive of a collapsed pigment epithelial detachment. (E) Fundus autofluorescence (FAF) of the right eye highlighting SRF and the RPE tear. (F) FAF of the left eye demonstrating a hyperautofluorescent pattern with focal hypoautofluorescence corresponding to a smaller RPE tear.
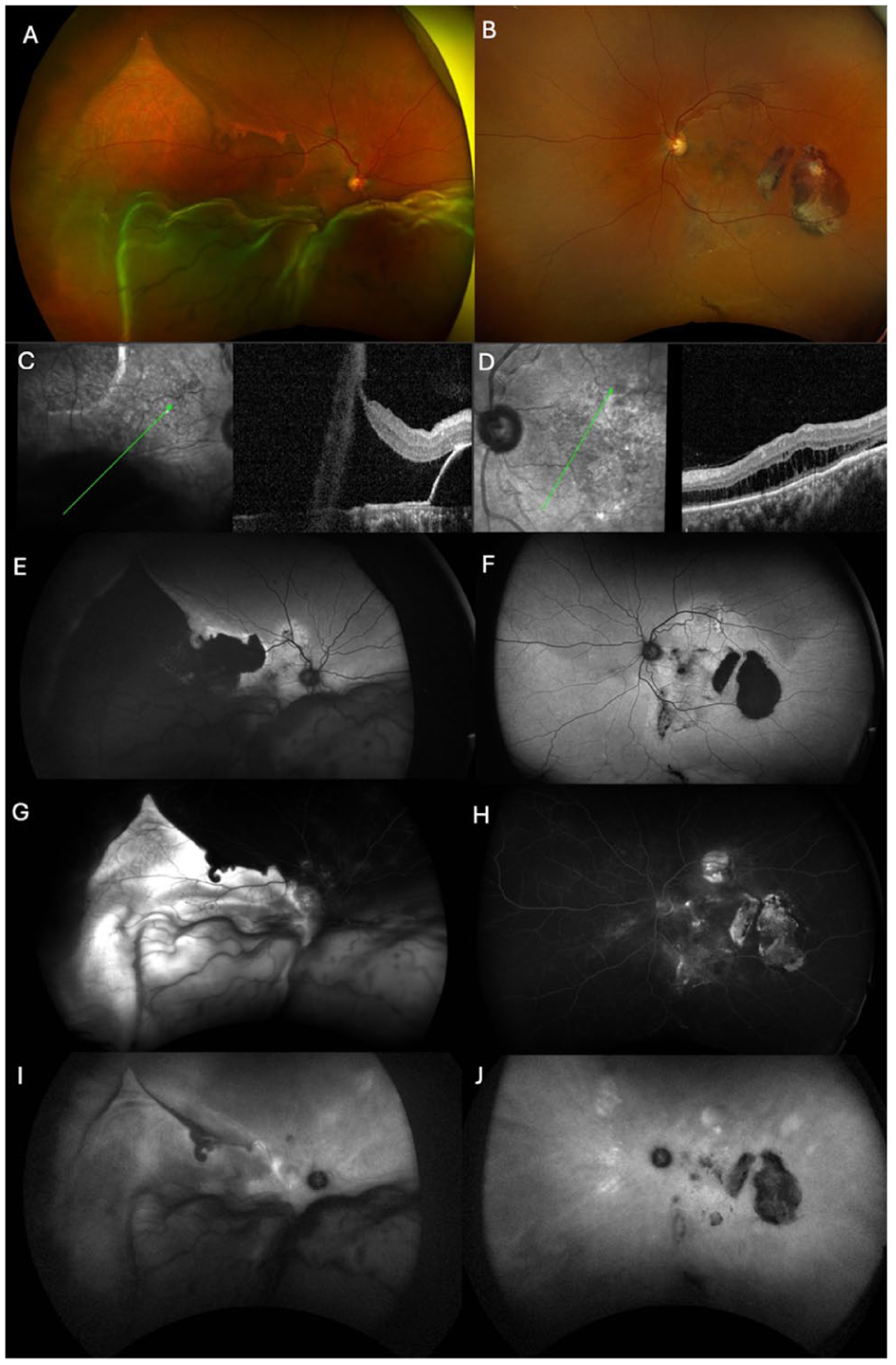
(A) Color fundus photograph of the right eye demonstrating progression and scrolling of the retinal pigment epithelium (RPE) tear. (B) Color fundus photograph of the left eye showing a stable appearance. (C) Oblique optical coherence tomography (OCT) raster of the right eye showing progression of the RPE tear with increased subretinal fluid. (D) OCT of the left eye showing improvement in intraretinal fluid after treatment. (E) Fundus autofluorescence (FAF) of the right eye highlighting the progression of the RPE tear. (F) FAF of the left eye demonstrating stable findings. (G, H) Fluorescein angiography (early phase) demonstrating a hyperfluorescent window defect corresponding to areas of RPE loss. (I, J) Indocyanine green angiography demonstrating increased visualization of underlying choroidal vessels in areas of RPE detachment.
At the 4-week follow-up, VA remained CF in both eyes. OCT demonstrated a stable macular appearance in the right eye and interval improvement in SRF in the left eye. Posterior segment examination of the left eye demonstrated stable findings. In contrast, examination of the right eye revealed progression of the RPE tear with further scrolling, resulting in substantial areas of denuded RPE involving both the macula and peripheral retina (Figure 2). Fundus autofluorescence revealed a large hypoautofluorescent area, confirming the absence of RPE. Fluorescein angiography showed a corresponding early-phase hyperfluorescent window defect (Figure 2, E and F). Indocyanine green angiography revealed increased visualization of underlying choroidal vessels in areas of RPE detachment (Figure 2, G and H). In addition, multifocal areas of late leakage were noted in both eyes on indocyanine green angiography, likely corresponding to patchy areas of RPE atrophy (Figure 2, G and H). The patient was subsequently lost to follow-up.
Conclusions
Chronic CSCR is characterized by persistent or recurrent serous detachments that cause cumulative damage to the RPE. Over time, the RPE undergoes atrophic changes, with loss of intercellular adhesion and the development of areas of focal weakness. 11 The patient’s reported history of bilateral “retinal detachment” treated with focal laser approximately 10 years earlier, combined with gravitational macular scarring and RPE atrophy, supports a longstanding pachychoroid-driven process. The OCT findings of focal RPE attenuation and choroidal thickening further indicate chronic disease predating the acute presentation. Despite increased choroidal hydrostatic pressure and a high prevalence of PED in chronic CSCR, RPE tears remain uncommon.2,11
Hypertensive choroidopathy may represent a second insult to an already compromised RPE. Severe hypertension causes fibrinoid necrosis of choroidal arterioles and ischemia, leading to rapid accumulation of fluid beneath the RPE and neurosensory retina.8,9,12 In otherwise healthy eyes, the RPE may tolerate such acute hydrostatic stress. However, prior reports have demonstrated RPE tears attributable to hypertensive crisis in some cases.8–10 We speculate that, in our patient, the chronically weakened RPE from longstanding CSCR was unable to tolerate the acute increase in hydrostatic pressure, resulting in a massive tear with progressive scrolling. This may be responsible for the extensive nature of the tear—from the temporal periphery through the macula—which exceeds the extent typically described in hypertension-associated cases alone and suggests that preexisting RPE compromise amplified the severity of damage. The volume of serous SRF in our patient was also substantial. Although neurosensory detachment is common after RPE tears, the presence of substantial SRF may facilitate dissection within the subretinal space, disrupting RPE–photoreceptor adhesion and allowing further propagation of the tear. This process may contribute to the observed superotemporal extension and progressive radial expansion.
Another notable feature in our case is the progressive nature of the tear over time. Most RPE tears reach their maximal extent at onset, with subsequent enlargement of the denuded area primarily attributable to progressive RPE scrolling. 3 We propose that the rapid expansion of SRF, in conjunction with persistent retina–RPE adhesion at the edge of detachment, may lead to propagation of the tear. The neurosensory retina is relatively elastic and mobile, while the RPE is comparatively inelastic; thus, progressive expansion of the detachment likely tears the attached RPE. 13
The marked asymmetry of the RPE tear in this case contrasts with prior reports of acute hypertensive crisis-associated RPE tears, in which bilateral and relatively symmetric involvement has been described.8,9 Torfs and Leys reported a unilateral RPE tear in a case of familial pulmonary artery hypertension, noting CSCR-like changes, including a small serous PED and asymmetric disease; their patient was also taking sildenafil, which the authors theorized may have contributed to CSCR-like changes. Prior CSCR literature similarly suggests that CSCR can asymmetrically affect the RPE, which may predispose to unilateral tear formation. 14
Additional explanation in the case of our patient may relate to the left eye, which showed macular scarring. While this indicates prior damage, such changes may paradoxically indicate areas where the RPE has already undergone fibrotic stabilization, making it more resistant to further tear propagation. Ultimately, the observed asymmetry underscores the importance of both chronic RPE vulnerability and superimposed acute insult occurring in spatial alignment for an RPE tear to develop.
This proposed dual-hit mechanism has important clinical implications. Patients with chronic CSCR may be at heightened risk for severe complications if they develop acute hypertensive choroidopathy. Blood pressure control is critical; however, in patients with underlying pachychoroid spectrum disease, even transient hypertensive episodes may cause irreversible RPE damage. Currently, no consistently effective treatment for RPE tears has been reported, underscoring the importance of prevention and early recognition of this condition.8,9
Footnotes
Ethical Considerations
This case report was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Informed verbal consent was obtained from the patient for publication of this case and any accompanying images.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the J. Arch McNamara, MD Fund for Retina Research and Education.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Xu is a consultant for AbbVie, Apellis Pharmaceuticals, DORC/Zeiss, and Gyroscope/Novartis Pharmaceuticals. Dr. Yonekawa is a consultant for Alcon, Bausch + Lomb, Genentech, Long Bridge Medical, Pykus, Thea, and Versant Health, and receives grant support from EyeBio, Genentech, Kyowa Kirin, Ocugen, and Regeneron. None of the other authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of the article.