
Abstract
Keywords
Introduction
Competing economic pressures, such as decreasing reimbursements, increasing cost of staff labor, and anesthesia team shortages have led to concerns about vitreoretinal surgeons’ abilities to perform medically necessary procedures. Surgical reimbursements have been reduced, especially when adjusted for inflation, resulting in negative opportunity costs for the surgeons and the surgery centers.1–4 However, many vitreoretinal conditions such as ruptured globes with intraocular foreign bodies and retinal detachments require urgent surgical repair, and nonsurgical options to prevent vision loss may be limited. Even a delay of a few days could be associated with worse visual outcomes.5–7 During the COVID-19 pandemic, approximately 53% of ophthalmic surgeries performed at academic centers were for urgent vitreoretinal conditions. 8 Unfortunately, there have been anecdotal reports of vitreoretinal surgeons losing access to operating rooms for emergency cases.
The purpose of the study was to assess the extent, possible causes, and potential impact of operating room restrictions on vitreoretinal surgeries in the United States by surveying the members of the American Society of Retina Specialists (ASRS), the world’s largest society of retina specialists. 9
Methods
An electronic survey was sent to 2789 US members of the ASRS from October to November 2025 to assess surgeons’ abilities to access operating rooms. The initial survey questions were developed by the ASRS Operating Room Task Force Committee, then tested and refined by members of the ASRS Health Economics Committee. No patient information was obtained; therefore, institutional board review was not required. The collection of data and analysis complied with all applicable laws.
Subgroup analyses were performed using the socioeconomic statuses of the physicians’ offices and surgery centers zip codes. Economically depressed/lower areas of socioeconomic status were defined as areas where 20% or more of the population met the criteria for the federal poverty level according to the US Census Bureau 10 or had social deprivation indexes above 80. Social deprivation indexes factored in the percentage of the population living in poverty, living in single-parent homes, living in rental units, living in overcrowded housing units, with fewer than 12 years of education, without a car, and unemployed under 65 years of age. 11
Although most patients would likely drive to the nearest surgery center for elective cases, they may need to drive further for emergency cases. The shortest and longest driving distances between surgery centers and the medical offices’ zip codes were calculated with Google Maps and the median values used for comparisons, with the interquartile ranges (IQR) included. Data were assessed for normality. GraphPad (GraphPad Prism 10) and XRealStats (release 9.7.6, Real Statistics Resource Pack Software) were used to calculate Fisher exact and 2-tailed Mann-Whitney U tests. P < .05 was considered statistically significant.
Results
A total of 276 physicians (10%) responded to the survey (Figure 1), the majority of whom were in retina-only private practice (61% [169]), followed by multi-specialty (20% [55]), academics (18% [51]), hospital-based (7% [20]), and other (1% [3]). On average, physicians worked at a median of 2 offices (IQR, 2-3), 86% (238) operated in ambulatory surgery centers, and 84% (233) in hospitals. The majority (63%, 175) performed urgent cases at nights and weekends in the hospitals, with 16% (44) referring to an academic center, 9% (25) operating in ambulatory surgery centers after hours, and 1% (4) referring to another community provider. The proportion of responders from each US region was similar to the geographic distribution of the general ASRS membership (Figure 2). There were more retina-only private practice respondents in the OR survey than in the 2025 ASRS Preferences and Trends Survey (61% vs 44% PAT; P < .001).
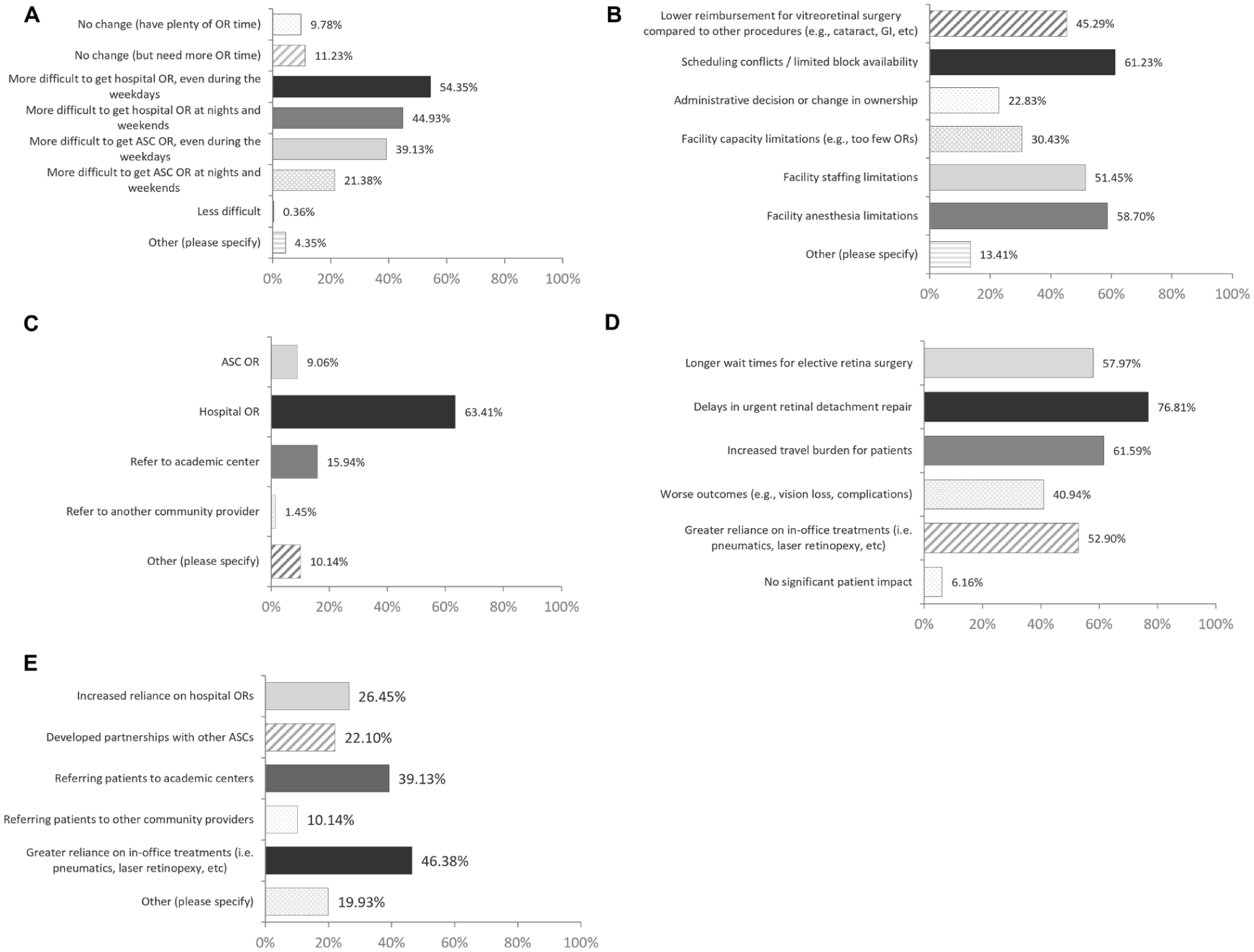
Operating Room Access Survey. (A) Most physicians reported increased difficulty with obtaining operating room time, especially at nights and weekends but also during the weekdays, regardless of their practice setting. (B) A variety of reasons were given for the limited operating room access, most commonly limited block time/scheduling availabilities and anesthesia limitations, followed by anesthesia and staffing limitations. (C) Most physicians performed urgent cases in hospital operating rooms at nights and weekends. (D) Physicians were concerned that operating room limitations would lead to delays in urgent surgical repairs and increased travel burden for patients. (E) Practices have compensated by relying more on in-office procedures and referrals to academic centers.
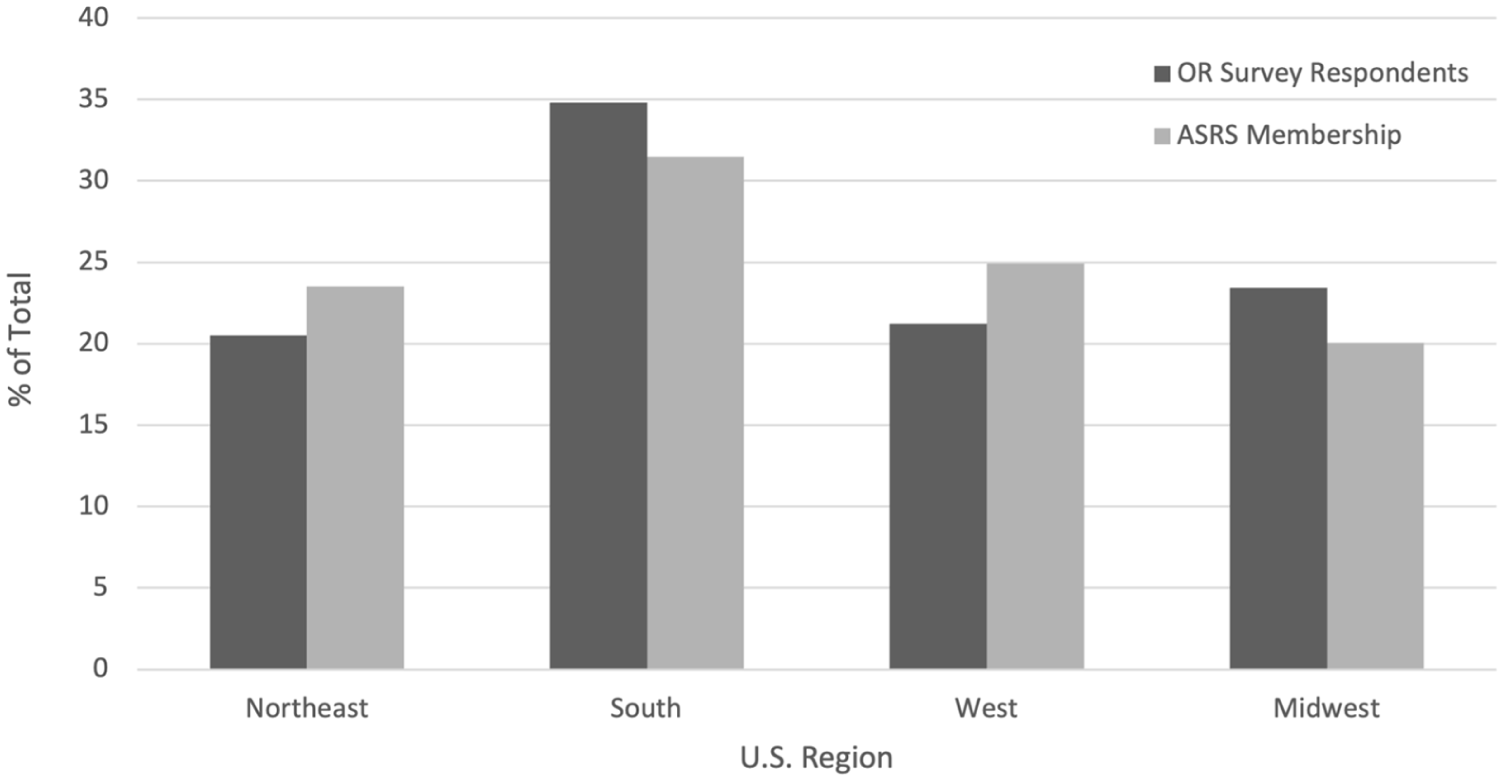
Regions covered by the Operating Room Access Survey. The proportion of regions that reported operating room restrictions was similar to those of the overall American Society of Retina Specialists membership (P < .69).
Approximately 90% of physicians (n = 248) responded that it has become increasingly difficult to obtain sufficient operating room time. The margin of error for the survey was 3.4%. Approximately 54% (150) reported increased difficulty accessing hospital operating rooms even during the weekdays, 45% (124) reported increased difficulty with hospital operating rooms at nights and weekends, 39% (108) had increased difficulty accessing ambulatory surgery center operating rooms even during the weekdays, and 21% (59) had increased difficulty with ambulatory surgery center operating rooms at nights and weekends. Of the 27 people (10%) who stated that they had plenty of block time with no change in availability and 1 person (0.4%) stating they had less difficulty obtaining operating room time, 12 (43%) had at least partial ownership in the surgery center. There was no statistically significant difference in the likelihood of reporting less difficulty with operating room access between those who did or did not have partial ownership in a surgery center (P < .99). Most physicians (99%) were concerned that they would continue to lose operating room access in hospitals and ambulatory surgery centers, both at nights and weekends and during the weekdays. Eleven vitreoretinal surgeons (4%) wrote in that they had no operating room access at all in hospitals or ambulatory surgery centers at nights and over the weekends, even for emergency cases.
The most common reasons for operating room access issues were limited block time/scheduling conflicts (61% [169]), facility anesthesia limitations (59% [162]), facility staffing limitations (51% [142]), lower reimbursements for vitreoretinal surgeries compared with other procedures (45% [125]), facility capacity limitations (30% [84]), and administrative decisions or changes in ownership (23% [63]). More than half (56% [156]) of physicians reported that financial considerations were either explicitly stated or likely to have contributed to restricting retina cases.
The majority of respondents (94% [259]) believed that restricted operating room access impacted patient care, leading to delays for urgent retinal detachment repair (77% [212]), increased travel burden for patients (62% [170]), longer wait times for elective cases (58% [160]), greater reliance on in-office treatments (53% [146]), and worse patient outcomes (41% [113]). Practices have compensated by relying more on in-office procedures (46% [128]), referring to academic centers (39% [108]), relying more on hospital operating rooms (26% [73]), and developing partnerships with ambulatory surgery centers (22% [61]).
Two hundred fifty-six surgeons (93%) took call, with most (77% [198]) taking call for their hospitals or emergency rooms either directly (52% [102]) or indirectly (34% [68]). There was no difference in the likelihood of reporting increased difficulty in accessing operating rooms whether hospital calls were taken directly (P=.16) or indirectly (P = .55).
University-Based vs Private, Hospital-Based, and Public Companies
A similar proportion of surgeons in academics/university-based practices (85%) reported difficulty accessing the operating room compared with those in private practice, hospital-based, or public companies (85% vs 90%; P = .33). University-based physicians were more likely to report a greater reliance on hospital operating rooms (45% vs 28%; P = .014), less likely to refer to academic centers (16% vs 44%; P = .011), and more likely to take direct or indirect call compared with those not in academics (98% vs 62%; P < .001). There was a similar proportion of university-based physicians practicing in lower and higher socioeconomic areas (P = .43).
Surgeons in private practice, hospital-based practices, and public companies were more likely to think that operating room restrictions were from lower relative reimbursements (16% academics vs 52% none-academics; P < .001) and administrative decisions or changes in ownership (10% vs 26%; P = .015). They were more likely to report that surgery centers mentioned case costs (8% academics vs 39% nonacademics; P < .001), case reimbursements (12% vs 47%; P < .001), insurance coverage (4% vs 23%; P = .013), and financial considerations (31% vs 62%; P < .001) as factors for restricting operating room access. In addition, they were more likely to report difficulty accessing ambulatory surgery centers at nights and weekends (8% academics vs 24% nonacademics; P = .011) and during the weekdays (16% vs 44%; P = .077). They were more likely to try to develop partnerships with ambulatory surgery centers to adapt to the restrictions (10% vs 25%; P = .024), were more concerned about losing further operating room access in the future (25% vs 43%; P = .026), and were less likely to think access to ambulatory surgery centers would improve at nights and weekends in the future (6% vs 0%; P = .061).
Lower Socioeconomic Areas vs Higher Socioeconomic Areas
One hundred eleven physicians (40%) had clinical offices that were in lower socioeconomic areas (51% primary clinics [57/111], 62% secondary offices [66/106]). Those in lower socioeconomic areas were more likely to report referrals to academic centers as an adaptation to operating room restrictions (47% vs 34%; P = .042) and were more likely to report insurance coverage/insurance spread as a reason for restricted operating room access (26% vs 15%; P = .026).
Eighty-three physicians (31%) operated in ambulatory surgery centers (16% [39/238]) or hospitals (28% [63/228]) in lower socioeconomic areas. The majority (87%) of the surgery centers without operating room restrictions were located in higher socioeconomic areas; only 1 of 20 ambulatory surgery centers (5%) and 4 of 14 hospitals (29%) without reported operating room limitations were in lower socioeconomic areas.
Driving Distances to Surgery Centers
Physicians operated at an average (± SD) of 1.11 ± 0.76 ambulatory surgery centers and 0.99 ± 0.71 hospitals. Approximately 26% (62/236) of physicians operated in an ambulatory surgery center in a different zip code from their office, and 32% (72/225) in a hospital in a different zip code. The median driving distance between the zip codes from the physician’s office to the surgery center was approximately 10.5 miles (IQR, 0-17.5 miles for the ambulatory surgery center, IQR, 0-19.5 for the hospital; P = .97). There was no difference in driving distances between the practice and surgery center for physicians who did or did not report difficulty with operating room access (P = .69 for ambulatory surgery centers and P = .15 for hospitals). Offices in lower socioeconomic areas were located farther from surgical centers (median of 19 vs 9 miles for ambulatory surgery centers, P < .001, and 17 vs 9 miles for hospitals, P < .001).
Conclusions
Most (90%) of the 276 vitreoretinal surgeons who responded to the ASRS Operating Room Access survey reported difficulty accessing sufficient operating room time. The majority (99%) of surgeons were concerned about further limitations to operating room access. These restrictions were prevalent across the US and its territories. Approximately half of surgeons reported difficulty accessing hospital operating rooms, even during the weekdays and at nights and weekends. Given that many vitreoretinal conditions require time-sensitive repairs to prevent permanent vision loss,5,6 these limitations to accessing operating rooms are increasingly concerning.
Retina surgeons drove to a median of 2 offices and operated at a median of 1 ambulatory surgery center and 1 hospital to increase patient access, with 40% of respondents having an office in a lower socioeconomic area. A quarter to a third of patients still had to travel to a different zip code for their surgeries, possibly due to the availability of surgery centers with specialized equipment and highly trained staff. Patients in lower socioeconomic areas had to drive almost twice as far as those from wealthier neighborhoods. Finding caretakers to drive patients back and forth may be difficult, especially for those with limited financial means. In other surgical specialties (eg, general surgery, neurosurgery, colorectal surgery, cardiothoracic surgery, and cardiovascular surgery), having a lower socioeconomic status and being in more rural areas were associated with lower access to high-volume surgery centers and worse patient outcomes.12–19
The potential reasons for the operating room restrictions are likely multifactorial, including financial reimbursements for retina cases relative to other procedures 20 and staffing deficiencies. The availability of anesthesiology care teams and experienced surgical technicians and nurses were significant factors identified in the present survey. Surgery centers, especially those in lower socioeconomic areas, are facing greater financial strains, and the costs of staffing and performing retinal surgery can exceed current reimbursements, especially for hospitals.4,21–23 Physicians are trying to shift more cases to ambulatory surgery centers, but patient comorbidities or insurances may preclude that option. Doctors have tried to compensate by using more in-office procedures, such as pneumatic retinopexies, but some emergent conditions may not be amenable to nonsurgical options. Physicians can try to perform surgeries before or after clinics at the surgery centers that do allow add-on cases, but these emergency cases could take longer to perform, 2 increasing the direct and indirect costs for the surgeon and surgery center and contributing to physician burnout and fatigue. 24 Sending urgent cases to overburdened academic centers is not a sustainable solution, especially because similar access issues are being encountered at university-based practices. The Centers for Medicare & Medicaid Services could help mitigate the financial concerns by raising facility reimbursements for emergency care and making it more financially acceptable for surgery centers to ensure adequate block time and staff for vitreoretinal cases.
Limitations of the present study include possible survey bias. Physicians who have had more difficulty obtaining operating room access may have been more likely to respond to the survey, especially those in private practice; however, the margin of error for the survey was only 3.4%, and the members were distributed within the US similar to the general ASRS membership. The OR access survey results were also similar to the PAT survey, in which 78% of the 889 US and international ASRS members reported difficulty accessing sufficient operating room time, especially for emergency surgeries. 25 The present study relied on self-identified practice designations and zip codes for the sub-group analyses, but some practices may be hybrid academic/private practice, and some may not have listed all offices or surgery center zip codes. Certain patient care concerns may also be applicable to all physicians, regardless of their practice setting. Because the surveys were anonymous, it was unclear how many separate practices and surgery centers were involved, but the increased difficulty accessing operating rooms appeared to affect areas nationwide. Furthermore, the estimated driving distances and socioeconomic statuses were based on the office and surgery center zip codes; the actual patient driving distances may not fully reflect the transportation burden and socioeconomic status of the patients.
There is increasing nationwide concern regarding the ability for patients with vitreoretinal pathologies to undergo surgeries at both ambulatory surgery centers and hospitals, which could shift the patient burden further toward academic centers, limit patient access to care, lead to treatment delays, and increase barriers to care. The financial disincentives for hospitals and ambulatory surgery centers could be mitigated by increasing the facility and anesthesia reimbursements for retina cases. Other potential policy initiatives include requiring minimum operating room access or allocating dedicated emergency retina operating room time for surgery center licensure. Future studies may help quantify the impact of operating room access on patient outcomes, especially for those in lower socioeconomic areas.
Footnotes
ORCID iDs
Ethical Considerations
Ethical approval was not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data available upon request.