
Abstract
Purpose:
To evaluate long-term outcomes of in-office laser barricade for large (≥2 clock hours) rhegmatogenous retinal detachments (RRDs) and to report the frequency of additional laser treatment or pars plana vitrectomy (PPV).
Methods:
A retrospective chart review was performed of patients treated between 2015 and 2023 at a retina-only private practice in Chicago, Illinois. Included cases were eyes with fundus diagram–confirmed RRDs involving ≥2 clock hours of circumference, and ≥3 months of follow-up. Procedure success was defined as RRD management without requiring PPV.
Results:
Seventy-six eyes of 72 patients (mean ± SD age, 52.1 ± 17.7 years) were analyzed, with a mean follow-up of 38.6 months. RRD size was a mean ± SD 2.9 ± 1.1 clock hours (range, 2–6). Mean best-corrected visual acuity (BCVA) was 20/31 at baseline and 20/30 at final follow-up. Procedure success rate was 92.1%, with 6 eyes (7.9%) requiring PPV. Thirteen eyes (17.1%) required additional laser barricade. Eyes with phakic lens status, worse baseline BCVA, vitreous hemorrhage, or baseline posterior vitreous detachment were more likely to require PPV, though these associations did not reach statistical significance (P = .06–.08). Laser barricade was performed on same day of diagnosis in 47 eyes (61.8%) and delayed by ≥1 day in 29 eyes (38.2%). Same-day treatment trended toward a higher need for PPV (P = .08 vs delayed treatment).
Conclusions:
In-office laser barricade is an effective treatment for RRDs spanning ≥2 clock hours, with a 92.1% long-term success rate. Patients not requiring same-day intervention may achieve excellent outcomes with laser barricade alone.
Introduction
A rhegmatogenous retinal detachment (RRD) is a sight-threatening condition that occurs when a retinal break allows fluid to accumulate underneath the neurosensory retina, leading to its separation from the underlying retinal pigment epithelium.1,2 RRDs can be managed using several approaches, including pars plana vitrectomy (PPV) with or without scleral buckling, scleral buckling alone, pneumatic retinopexy, laser barricade, or, in select cases, observation. 3 PPV is a surgical procedure in which the vitreous humor is removed and replaced with gas to reattach the retina. 4 For smaller RRDs, in-office laser barricade is a less-invasive alternative. This procedure involves applying multiple rows of laser burns around the retinal detachment, sealing the retina and preventing further fluid accumulation. 5 Laser barricade offers several advantages, including avoidance of more invasive surgery and its associated postoperative complications, while still providing long-term stability, 6 a high success rate, 7 and preservation of visual acuity. 7
Most case series investigating in-office laser barricade for RRDs have focused on detachments measuring <2 clock hours of circumference.5,8,9 However, a presentation with subretinal fluid spanning only 1 clock hour may represent a large tear with fluid rather than a true RRD. 10 The success of larger detachments treated with laser barricade alone has not been well defined, though it is a routine procedure done in clinic to avoid surgical interventions in patients for various reasons. Having success rates defined can help appropriately counsel patients regarding risks and benefits of treatment options.
The purpose of this study is to evaluate the long-term visual and anatomic outcomes of in-office laser barricade treatment in patients with RRDs measuring 2 or more clock hours and report the frequency of additional laser treatment or the subsequent need for PPV. To avoid including cases with large tears or holes with a small amount of fluid, our study specifically identified cases of RRDs measuring 2 or more clock hours, thereby ensuring the inclusion of true RRDs. Additionally, we assessed outcomes over long follow-up periods, ranging from 3 months to more than 5 years, to evaluate long-term outcomes and potential complications. Through these findings, we aim to further define the role of in-office laser barricade in the management of larger RRDs and provide guidance for clinical decision-making in this patient population.
Methods
This retrospective chart review included patients from a large retina-only private practice in Chicago, Illinois. Patient data were collected over an 8-year period from March 2015 to July 2023 from 15 retina specialists. The study was determined to be exempt from formal review by the medical center’s Institutional Review Board and Ethics Committee, as it met the exemption criteria involving the collection of research data for subjects who could not be identified directly or through linked identifiers. This study was conducted according to the principles of the Declaration of Helsinki, regulations, and guidelines.
Inclusion and Exclusion Criteria
Cases were identified by querying medical records using the Current Procedural Terminology code 67105. Cases were included if they had an RRD treated with in-office laser barricade, a minimum of 3 months of follow-up, and an ophthalmoscopy fundus diagram or descriptive text (that specifically provided clock-hour extent of the RRD) to assess the circumferential width of the detachment. Only RRDs with a minimum of 2 clock hours of circumference were included in the study to ensure that true RRDs were analyzed. Charts lacking an adequate fundus diagram or description of the size of the detachment (clock-hour extent) were excluded. In addition, patients who received intraocular gas bubble (to exclude pneumatic retinopexies) were excluded. Two eyes with fewer than 3 months of follow-up were also excluded.
Laser Barricade
Photocoagulation was delivered using argon laser therapy with either slitlamp or laser indirect ophthalmoscopy. Anesthesia mainly consisted of topical proparacaine, while a limited number of patients were administered subconjunctival lidocaine or retrobulbar block for additional anesthesia. Treatment typically involved 3 or more rows of confluent gray-to-white laser burns applied to the attached area surrounding the RRD out to the ora serrata. However, exact settings were determined by the treating physician at the time of the treatment(s).
Data Extraction and Analysis
Baseline demographic and clinical characteristics of the patients included sex, age, laterality of the RRD, best-corrected visual acuity (BCVA), lens status, and the presence of posterior vitreous detachment (PVD), vitreous hemorrhage (VH), and epiretinal membrane (ERM). Fundus diagrams were reviewed to document the detachment size in clock hours, location (superior or inferior), and types of causative breaks (holes vs tears). Procedural data, including the number of laser spots and laser power (in mW), were collected. Postoperative data included final follow-up VA, duration of follow-up, and the need for additional laser or need for PPV.
The primary outcome was the proportion of eyes requiring PPV. Secondary outcomes included the proportion of eyes requiring additional laser treatment, the incidence of ERM at final follow-up that was not present prior to laser barricade treatment, and baseline and final VA. The procedure success rate was defined as the percentage of cases in which RRD was successfully managed without the need for PPV. Snellen VA values were converted to logMAR for data analysis. Associations between clinical characteristics and laser treatment success were assessed using univariate analysis and logistic regression. Comparisons of categorical outcomes were conducted using the χ2 test and Fisher exact test. P values less than .05 were considered statistically significant. Results are the mean (±SD) or median (range).
Results
Baseline Patient Characteristics
During the 8-year study period, a total of 76 eyes of 72 patients were analyzed. The baseline demographic and clinical characteristics of the patients are shown in Table 1. The mean age of the patients was 52.1 ± 17.7 years (range, 18–91 years) (Figure 1, C and D). The mean follow-up was 38.6 ± 27.4 months (median, 31 months; range, 3–115 months) (Figure 1, A and B). The mean number of follow-up visits within 6 months was 3.1 ± 2.3.
Baseline Demographic and Clinical Characteristics of Patients With Large RRDs Undergoing Laser Barricade (76 eyes, 72 patients).
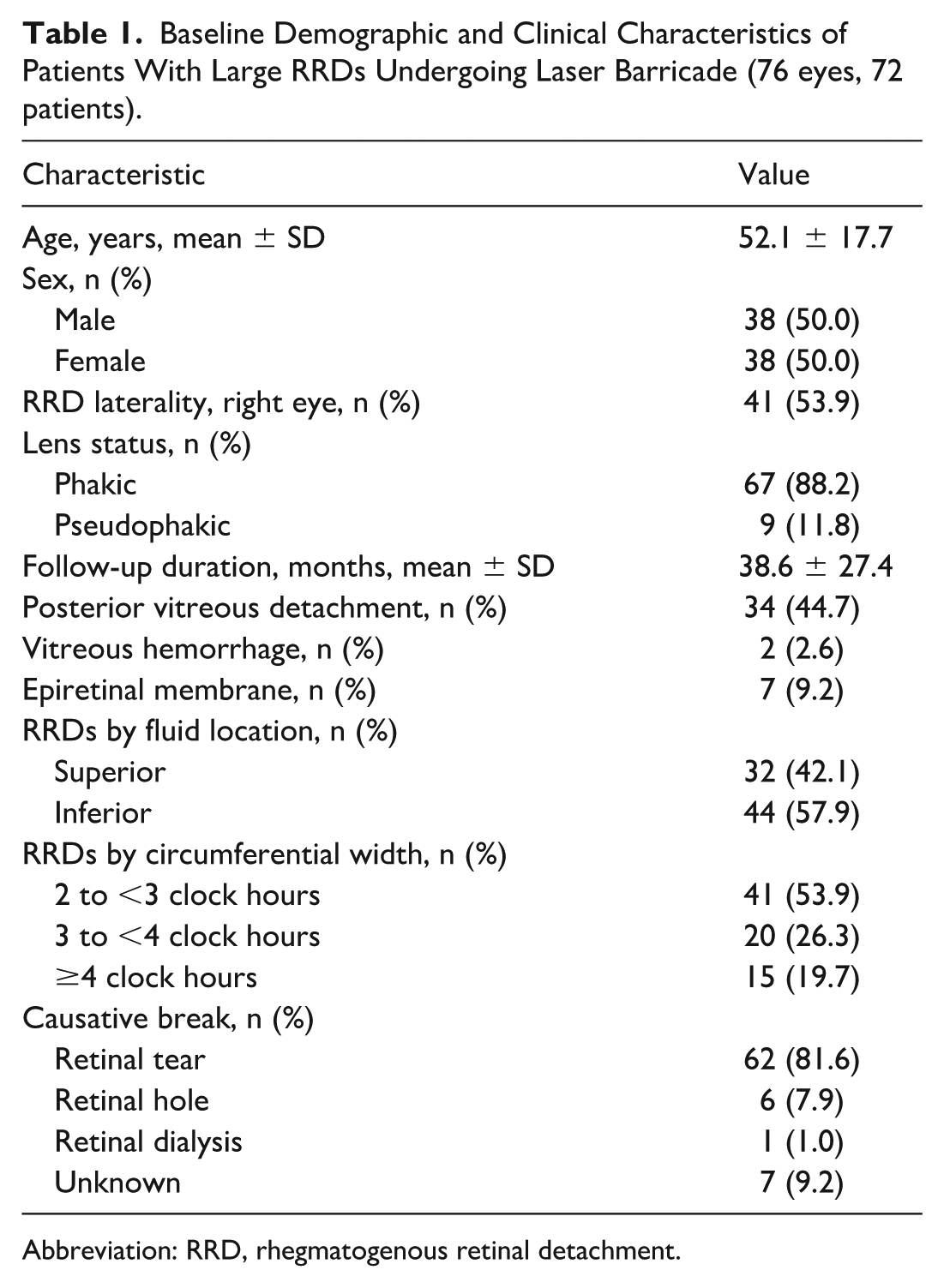
Abbreviation: RRD, rhegmatogenous retinal detachment.
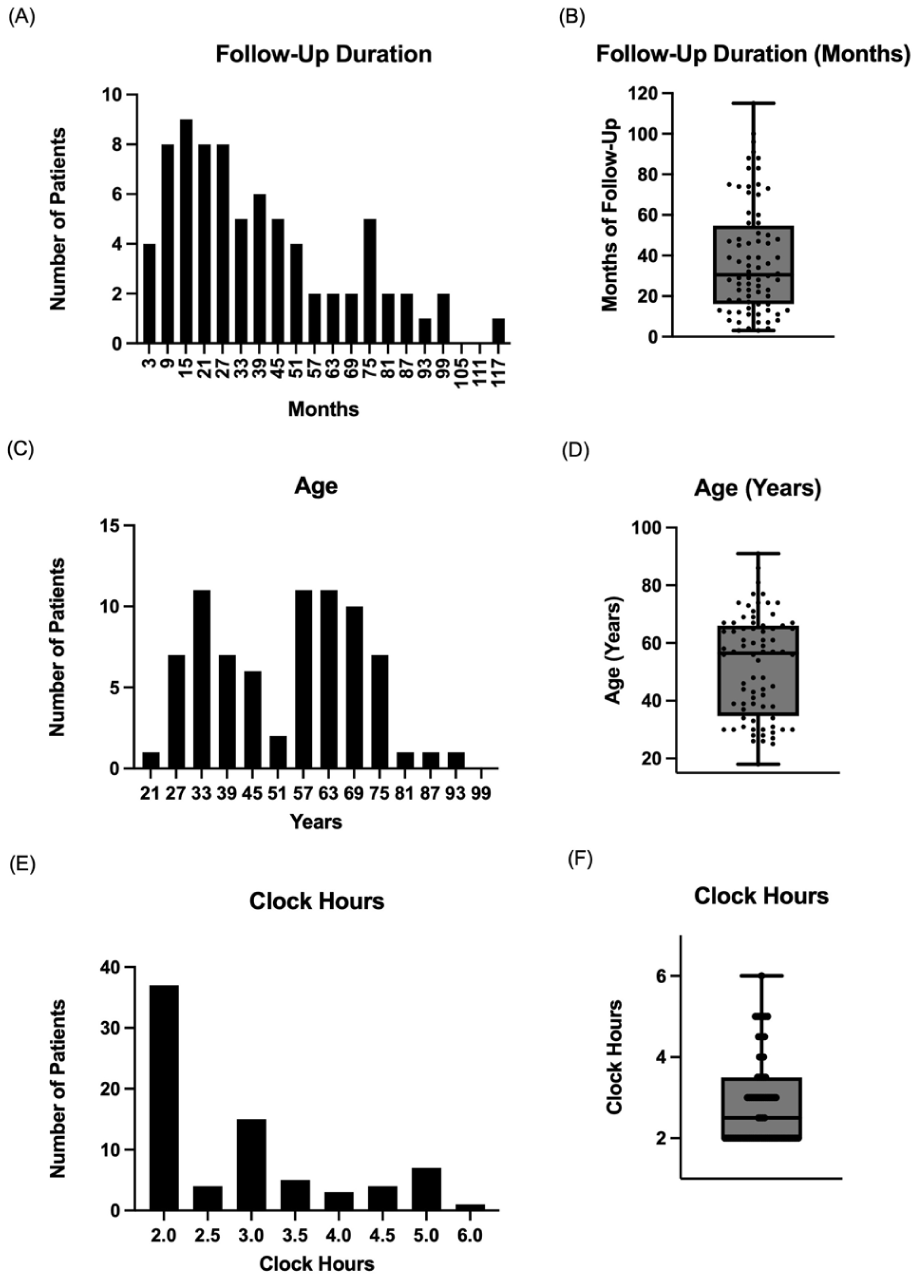
Key study variables, depicted as histograms and box plots, for patients with large rhegmatogenous retinal detachments undergoing laser barricade treatment (76 eyes, 72 patients). Variables include (A and B) follow-up duration evaluated at different times after treatment, represented as 6-month windows centered on the number of patients, and median duration; (C and D) patient ages, represented as 6-year age ranges centered on the number of patients, and median age; (E and F) size of retinal detachments, shown as .5-unit increments of clock hours centered on the number of patients, and median clock hours of circumferential width. Box scatterplots show individual values (dots), median (horizontal line), interquartile ranges (box), and upper and lower ranges (whiskers).
At baseline, 67 eyes (88.2%) were phakic, and 9 eyes (11.8%) were pseudophakic, consisting of 7 with a standard posterior chamber intraocular lens (PCIOL) and 2 with a multifocal PCIOL. The size of the RRDs ranged from 2 clock hours to 6 clock hours, with a mean of 2.9 ± 1.1 clock hours and a median of 2.5 clock hours (interquartile range, 2.0–3.5 clock hours) (Figure 1, E and F). The location of fluid was located superiorly in 32 eyes (42.1%) and inferiorly in 44 eyes (57.9%). There was no significant difference in circumferential width in clock hours between inferior and superior RRDs (P = .49).
At baseline, PVD was identified on clinical examination in 34 (44.7%) of 76 eyes. Optical coherence tomography (OCT) imaging was performed in 38 eyes (50%), of which 16 demonstrated PVD. OCT findings were consistent with the PVD status determined on clinical examination, reflecting 100% concordance between the 2 methods. VH was present in 2 eyes (2.6%). The causative breaks included retinal tears in 62 eyes (81.6%), retinal holes in 6 eyes (7.9%), retinal dialysis in 1 eye (1.0%), and unknown in 7 eyes (9.2%). Lattice degeneration was present in 25 eyes (32.9%). Among eyes with lattice degeneration, 5 required additional laser treatment, and none progressed to require vitrectomy. Approximately 35.5% (27 of 76 eyes) presented with at least 1 symptomatic change. Among those with symptomatic visual changes at baseline, 13 patients (17.1%) reported acute flashes, 17 (22.4%) reported acute floaters, and 5 (6.6%) presented with a peripheral visual field defect. The mean number of laser spots was 592.4 ± 403.2, and the mean laser power was 354.1 ± 164.1 mW. The mean spot size could not be determined, as 30 eyes were treated at the slit lamp and 46 were treated with indirect laser.
Laser barricade treatment was administered on the same day of diagnosis in 47 eyes (61.8% of eyes), while 29 eyes (38.2%) underwent treatment after a delay of at least 1 day. Among delayed cases, the mean time to laser barricade was 16.2 ± 16.2 days. In the delayed group, 10.3% (3 of 29 eyes) required additional laser treatment, and no eyes required surgery. In comparison, in the same-day treatment group, 21.3% (10 of 47 eyes) required additional laser treatment, and 12.8% (6 of 47 eyes) required surgery. There was no significant difference in the need for additional laser treatment between same-day treatment and delayed treatment groups (P = .36). A higher need for PPV was seen in the same-day treatment group compared with the delayed-treatment group, which trended toward significance (P = .08).
Outcomes of Laser Barricade
The laser-only success rate was 92.1% (70 of 76 eyes), with 6 eyes (7.9%) requiring a PPV (Table 2). The mean baseline BCVA was 20/31 (range, 20/20 to counting fingers [CF] at 1 foot), and the mean final BCVA was 20/30 (range, 20/20 to CF at 2 ft). Among the 6 eyes requiring PPV, 4 eyes required PPV due to symptomatic progression of RRD, and in the remaining 2 eyes, PPV was planned at the time of initial laser. The 6 eyes that underwent a single PPV procedure demonstrated a 100% anatomic reattachment rate at 1 year postoperatively.
Anatomic and Visual Outcomes of Retinal Barricade in Patients With Large RRDs (76 eyes, 72 patients).
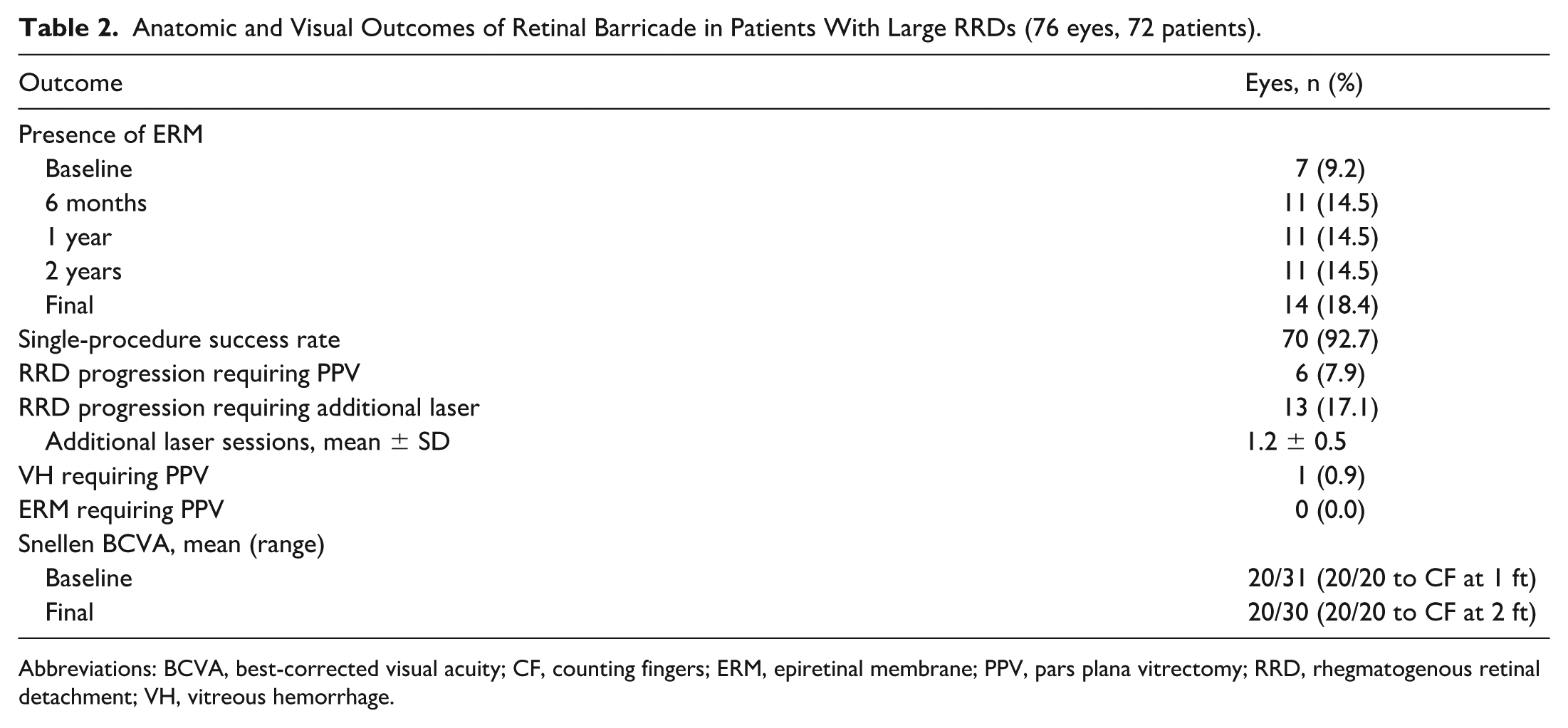
Abbreviations: BCVA, best-corrected visual acuity; CF, counting fingers; ERM, epiretinal membrane; PPV, pars plana vitrectomy; RRD, rhegmatogenous retinal detachment; VH, vitreous hemorrhage.
In univariate analysis, RRD requiring PPV was correlated with worse baseline BCVA (P = .07) and lens status at presentation (P = .06) (Table 3). In logistic regression models, RD requiring PPV was associated with the presence of PVD at presentation (P = .081), VH (P = .08), and phakic lens status at presentation (P = .06), although none of these associations were statistically significant.
Univariate Analysis of Associations of Categorical Characteristics With PPV Status in Patients With Large RRDs Undergoing Laser Barricade.
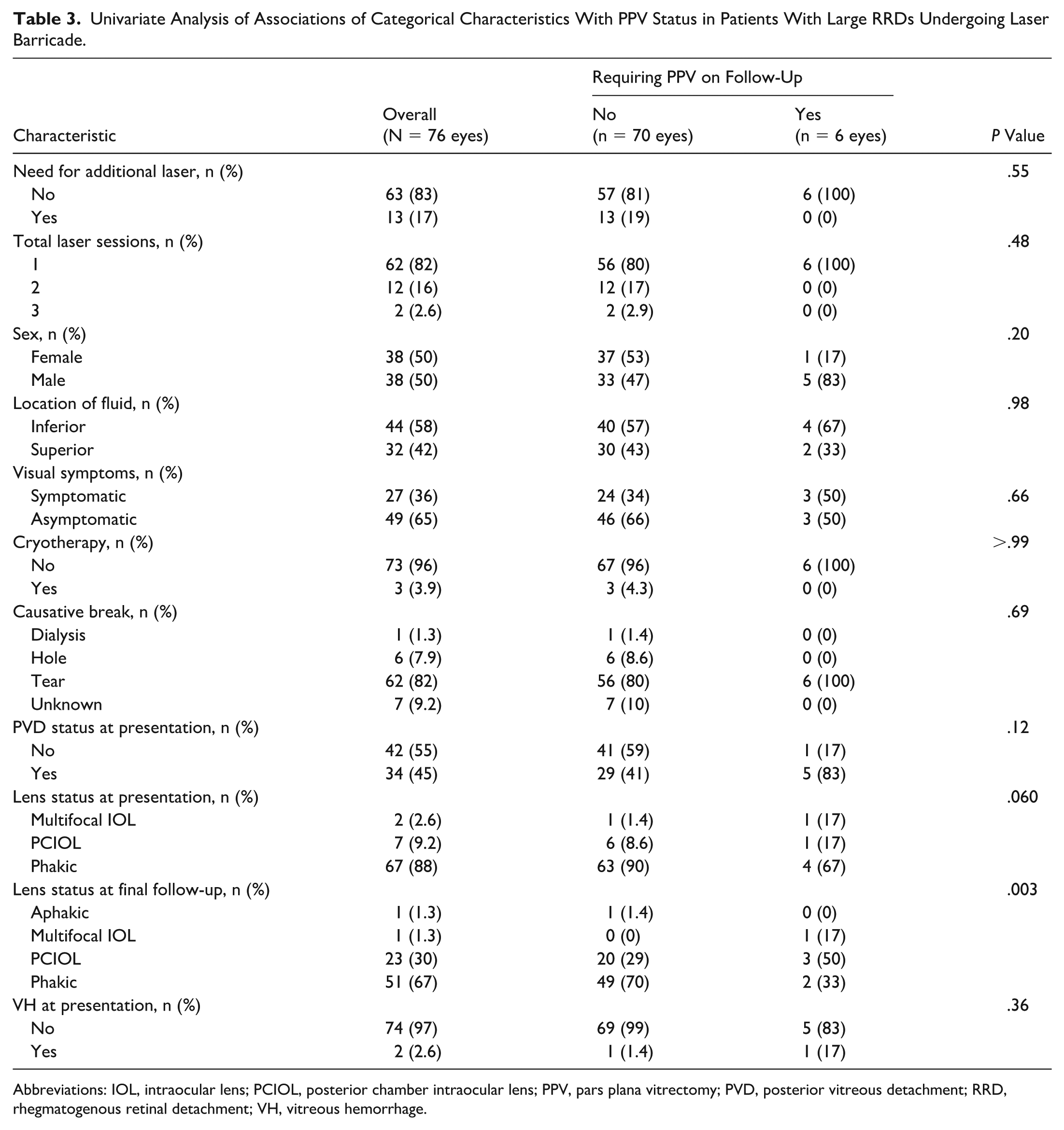
Abbreviations: IOL, intraocular lens; PCIOL, posterior chamber intraocular lens; PPV, pars plana vitrectomy; PVD, posterior vitreous detachment; RRD, rhegmatogenous retinal detachment; VH, vitreous hemorrhage.
RRD progression requiring an additional laser occurred in 13 eyes (17.1%), with 11 eyes requiring 1 additional session and 2 eyes requiring 2 additional sessions. In both univariate and logistic regression analyses, the need for additional laser treatment was significantly associated with the number of clock hours of RRD circumferential width (P < .001 and P = .001, respectively), and with the number of laser spots (P = .02 and P = .01, respectively). Furthermore, in univariate analysis, lower laser power (in milliwatts) was significantly associated with the need for additional laser treatment (P = .01). Superior vs inferior location of RRD was not significantly associated with the need for additional laser (P = .37) or with the need for PPV (P = .98) (Table 3).
Among the 2 cases with baseline VH, 1 eye required PPV on follow-up. The proportion of patients with ERM was 9.2% (7 eyes) at baseline, increasing to 14.5% of patients (11 eyes) at 6 months, 1 year, and 2 years, and increasing to 18.4% (14 eyes) at the final follow-up. None of the eyes with ERM required PPV at the time of the last follow-up appointment.
Conclusions
RRDs can be treated with a range of treatment modalities, including PPV with or without scleral buckling, scleral buckling alone, pneumatic retinopexy, laser barricade, and observation. 3 For smaller, peripheral RRDs, laser barricade is a reasonable and minimally invasive treatment option. It can also be considered in select patients with significant medical comorbidities in which anesthesia or positioning postoperatively are complicating factors. When clinically appropriate, laser barricade treatment can preclude the need for an operating room. However, laser barricade treatment is not the most common approach to treat an RRD because of its limitations, which include that it does not reattach the retina, does not remove tractional forces caused by the vitreous, and does not improve associated symptomatic visual field defects. Despite these limitations, our study demonstrates that laser barricade remains a viable treatment option, even for larger RRDs.
Previous case series evaluating the effectiveness of in-office laser barricade treatments have largely focused on smaller RRDs involving sizes of <2 clock hours.5,8,9 However, it is important to recognize that a large tear may present with subretinal fluid spanning only 1 clock hour, which may not represent a true retinal detachment, but rather a large tear with associated fluid. To address this, we aimed to analyze cases of large RRDs involving at least 2 clock hours. In our cohort of 76 eyes, although 37 eyes had RRDs of 2.0 clock hours, we did have 39 eyes that had RRDs of between 2.5 clock hours and 6.0 clock hours.
Our results demonstrate that in-office laser barricade is an effective treatment for these larger RRDs. We report excellent visual outcomes, with a mean baseline BCVA of 20/31 and mean final BCVA of 20/30. Over an average follow-up of 38.6 months, we report a high success rate (cases in which RRD was successfully managed without subsequent PPV) of 92.1%. These results are consistent with those reported in previous studies evaluating laser barricade treatment for RRDs. Notably, several key studies did not specify an inclusion criterion that was based on clock-hour extent of RRDs. Xu et al studied 112 eyes with macula-sparing peripheral RRDs that underwent laser demarcation, and reported a procedure success rate of 84.8% during a mean follow-up of 20 months. 5 Similarly, in a study by Al-Mohtaseb et al including macula-sparing peripheral RRDs, the findings showed that 81.4% of 27 eyes treated with laser barricade remained attached without requiring additional treatment during a mean follow-up of 38.4 months. 11 Hwang and Chen reported a procedure success rate of 88.8% (32 of 36 eyes) in teenagers with macula-sparing RRDs, 9 further supporting the effectiveness of laser barricade in select cases.
Our study reported symptomatic visual changes in several patients: 13 cases (17.1%) reported acute flashes, 17 cases (22.4%) reported acute floaters, and 5 (6.6%) presented with a peripheral visual field defect. Evaluation of the case series of 27 patients treated with laser demarcation in the study by Al-Mohtaseb et al 11 found that none of the 14 patients who were asymptomatic at baseline experienced symptomatic visual changes over follow-up, compared with 38.5% of patients (5 of 13) who had symptomatic visual changes at baseline. In a case series of 34 eyes in a study by Vrabec and Baumal, the 2 patients who required subsequent treatment after demarcation laser photocoagulation had symptomatic visual changes, which were peripheral scotomas. 12 These studies, along with our findings, suggest that laser barricade treatment may be particularly effective for patients who are asymptomatic with no visual field defect.
All 6 cases in which additional PPV was required were in the same-day treatment group. The need for PPV was higher in the same-day treatment group (12.8%) compared with the delayed treatment group (0%), with the difference approaching statistical significance (P = .08). This suggests a possible trend, such that patients who receive same-day laser barricade treatment may present with more acute, evolving symptoms, which warrants further investigation. In cases of urgent RRDs requiring same-day intervention, PPV may be a more suitable treatment approach than laser barricade. 13
While the presence of PVD, VH, and phakic lens status showed a trend toward association with RRD requiring PPV, these factors did not reach statistical significance. The study by Xu et al 5 also demonstrated that presence of VH was less conducive to laser barrier treatment. Future data may further elucidate these associations and their role in complications, improving outcomes with laser barricade treatment.
Superior RRDs progress more rapidly, and superior breaks are less responsive to laser treatment. 10 However, in our study, the location of fluid was not associated with RRD requiring PPV (P = .98). This may be attributed to the absence of a significant difference in the circumferential width between inferior and superior RRDs (P = .49).
Additional laser treatment was required in 13 eyes (17.1%), with 11 eyes requiring 1 additional session and 2 eyes requiring 2 additional sessions. This was significantly associated with a higher number of clock hours of RRD circumferential width (P = .001). These findings are helpful for setting appropriate patient expectations regarding the potential need for further interventions. Although laser treatment remains a viable option, it is essential to counsel patients that, due to the size of their RRD, additional laser treatment may be necessary to achieve reattachment. Additional laser treatment was also associated with fewer laser spots (P = .012) and lower laser power (P = .010) in the initial laser procedure. This serves as an internal reference point for physicians, suggesting that increasing laser power and adding more laser spots can be a useful strategy to reduce the need for future laser treatments.
One strength of our study is the long-term follow-up, with a mean duration of over 3 years. Additionally, the study included only large RRDs that ranged from 2 clock hours to 6 clock hours in size. Limitations of this study include its retrospective chart review design, as opposed to a randomized controlled trial, which limits our ability to establish causation between variables. Additionally, with the chart review design, we were limited to the terminology used in patient records. For example, “retinal tear” was likely used to describe what we suspect were retinal holes causing the RRDs, especially in the younger subjects who did not have a PVD present. While our study includes a large sample size, additional patient data could provide further insights into associations between clinical characteristics and complications of RRDs. We did not survey patients to determine whether they experienced a visual field defect following the laser treatment, and whether their vision was disrupted by the defect. Furthermore, we relied on the surgeons’ fundus diagrams rather than fundus photography; however, this is unlikely to have significantly affected our results. Detailed fundus drawings represent a standard and routinely used clinical documentation in retinal practice. During the study period (2015–2024), widefield imaging was not uniformly used or available at our institution. As a result, fundus drawings were systematically reviewed to document RRD size and type of causative breaks.
In conclusion, in-office laser barricade treatment is a viable and minimally invasive option for appropriately selected cases of large RRDs. Although typically reserved for smaller or asymptomatic detachments, our findings suggest that laser barricade can be effective even for larger RRDs, demonstrating high long-term success rates and favorable visual outcomes. Patients with VH and/or PVD may require individualized management or closer follow-up due to potential risk factors. Additionally, patients who do not require same-day intervention may achieve excellent outcomes with laser barricade alone. This study contributes to the growing literature supporting laser barricade as a safe and effective treatment for RRDs and highlights areas for further investigation into optimal patient selection, predictors of procedural success, and long-term visual outcomes.
Footnotes
Ethical Considerations
This study was performed after approval from the Rush Institutional Review Board. All tenets of the Declaration of Helsinki were upheld throughout this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Statistical support was provided by Quyen Diep of the Rush Biostatistics Core.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Consent to Participate
Due to its retrospective design, this study was reviewed by the Rush Institutional Review Board and deemed exempt from requiring consent for participation and publication.