
Abstract
Purpose:
To report a case of acute macular neuroretinopathy in a 22-year-old woman with a history of Adams–Oliver syndrome and associated peripheral retinal vascular anomalies.
Methods:
A single case was reviewed.
Results:
A 22-year-old woman with a history of Adams–Oliver syndrome presented with a central scotoma and was found to have a paracentral outer retinal lesion consistent with acute macular neuroretinopathy. Retinal examination and multimodal imaging revealed peripheral retinal vascular anomalies, including bilateral peripheral telangiectasias, avascular retina, venous shunting, supernumerary branching, and vascular tortuosity, consistent with familial exudative vitreoretinopathy despite negative genetic testing.
Conclusions:
This case expands the ocular spectrum of Adams–Oliver syndrome and highlights the importance of routine ophthalmic surveillance in affected patients.
Introduction
Adams–Oliver syndrome is a rare congenital disorder primarily characterized by aplasia cutis congenita, hypoplasia of the skin, terminal transverse limb defects, and abnormalities of the cardiovascular and central nervous systems.1,2 The majority of cases follow an autosomal dominant inheritance pattern caused by mutations in DLL4, ARHGAP31, RBPJ, and NOTCH1 genes, whereas mutations in EOGT and DOCK6 result in autosomal recessive inheritance.3–5 In addition to familial cases, sporadic occurrences have also been reported. 6 Although the exact pathogenesis of Adams–Oliver syndrome is unclear, impaired vasculogenesis is thought to play a central role and may affect multiple organ systems, including the eyes. 7
While the cutaneous and limb anomalies of Adams–Oliver syndrome are well-documented, ocular involvement remains rarely reported. In a study of 398 patients with Adams–Oliver syndrome, ocular abnormalities were identified in only 18 patients (4.5%). 6
Reported anterior segment manifestations include microphthalmia, congenital cataracts, and glaucoma. 8 Retinal involvement is even rarer, with only a few case reports describing vascular abnormalities such as nonperfusion, neovascularization, fibrovascular proliferation, and, in some cases, retinal detachment.9–11 We herein describe a case of a young woman with Adams–Oliver syndrome who presented with hyperreflectivity of the outer plexiform layer (OPL) and outer nuclear layer (ONL) consistent with acute macular neuroretinopathy (AMN), along with retinal vascular anomalies.
Case Report
A 22-year-old woman with a history of Adams–Oliver syndrome presented for retinal evaluation after a sudden onset of a fixed central scotoma of her left eye 3 days before presentation. She denied any recent viral illness, vaccination, diffuse ischemic insult, ocular trauma, or changes to medication. Her medical history included systemic lupus erythematosus, syncopal episodes, pathologic cutis marmorata telangiectatica congenita, and Adams–Oliver syndrome. The diagnosis of Adams–Oliver syndrome had been established clinically in early infancy based on the presence of an atrial septal defect and bilateral congenital toe hypoplasia. Her medications included chloroquine for systemic lupus erythematosus, oral contraceptive pills, and a history of fludrocortisone use for orthostatic hypotension.
The patient was born at 34 weeks’ gestation and required ventilatory support in the neonatal period. She had no documented diagnosis of retinopathy of prematurity and was regularly monitored for ocular, vascular, and dermatologic manifestations of Adams–Oliver syndrome due to its multisystemic nature.
Ophthalmologic examination revealed a best-corrected visual acuity of 20/20 OU and intraocular pressure within normal limits. Amsler grid testing demonstrated a small paracentral scotoma just temporal to the center of fixation in the left eye. Fundus examination revealed peripheral telangiectatic vessels and vascular dragging in both eyes (Figure 1). Ultra-widefield fluorescein angiography (FA; Optos plc) demonstrated bilateral supernumerary vascular branching, vascular looping and shunting, telangiectasias with scattered microaneurysms, areas of avascular retina, and temporal vascular leakage (Figure 1). Optical coherence tomography (OCT; Spectralis HRA+OCT; Heidelberg Engineering) of the right eye demonstrated thinning of the ONL in the superotemporal macula. OCT through the fovea of the left eye demonstrated a focal band of hyperreflectivity extending vertically from the ONL through the ellipsoid and interdigitation zones, with associated outer retinal disruption, and an additional area of hyperreflectivity involving the outer plexiform layer and ONL (Figure 2). Near-infrared reflectance imaging (Spectralis HRA+OCT; Heidelberg Engineering) of the right eye revealed wedge-shaped lesions corresponding to the OCT findings, while that of the left eye revealed petaloid hyporeflective lesions. Swept-source OCT angiography (Zeiss PLEX Elite 9000; Zeiss) demonstrated areas of flow deficit in the choriocapillaris in both eyes, which were more pronounced in the right eye (Figure 3).
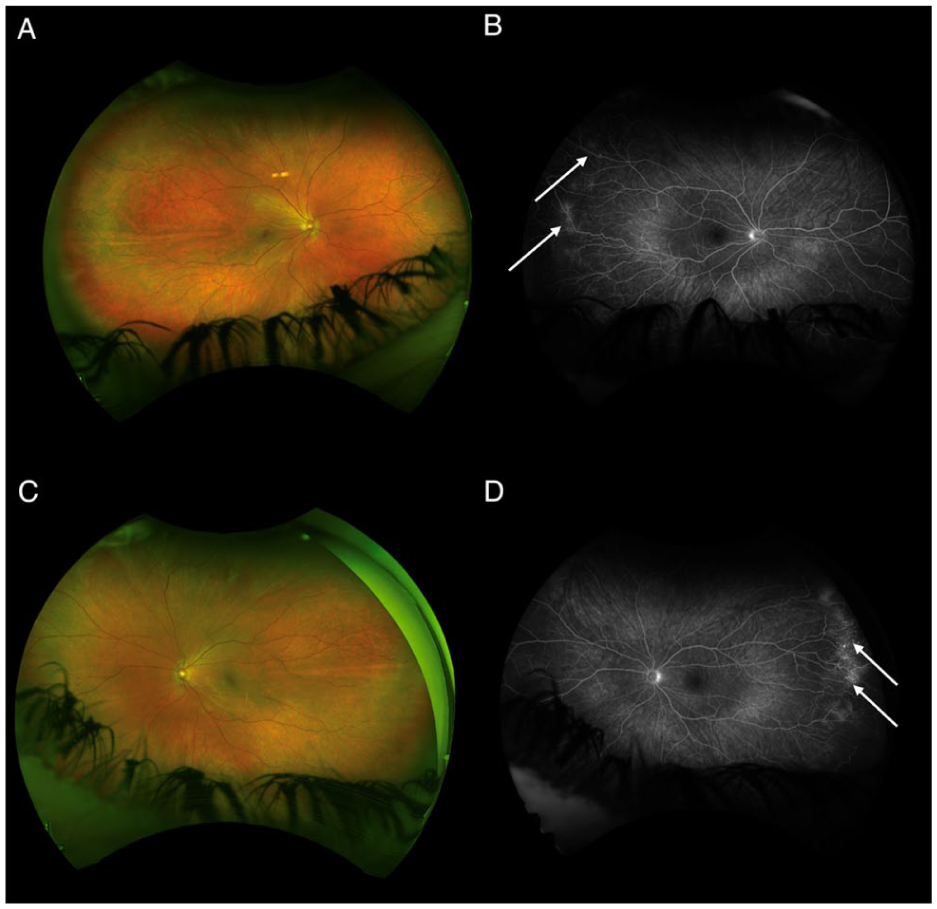
(A, C) Ultra-widefield pseudocolor imaging and (B, D) ultra-widefield fluorescein angiography (FA) images obtained at presentation. Ultra-widefield pseudocolor images demonstrating bilateral optic disc and vascular dragging, tortuosity of the retinal vessels, and peripheral retinal avascularity in both eyes. Ultra-widefield FA reveals abnormal peripheral vasculature, including supernumerary vascular branching, telangiectasias, areas of capillary nonperfusion, and temporal vascular leakage in both eyes (white arrows).
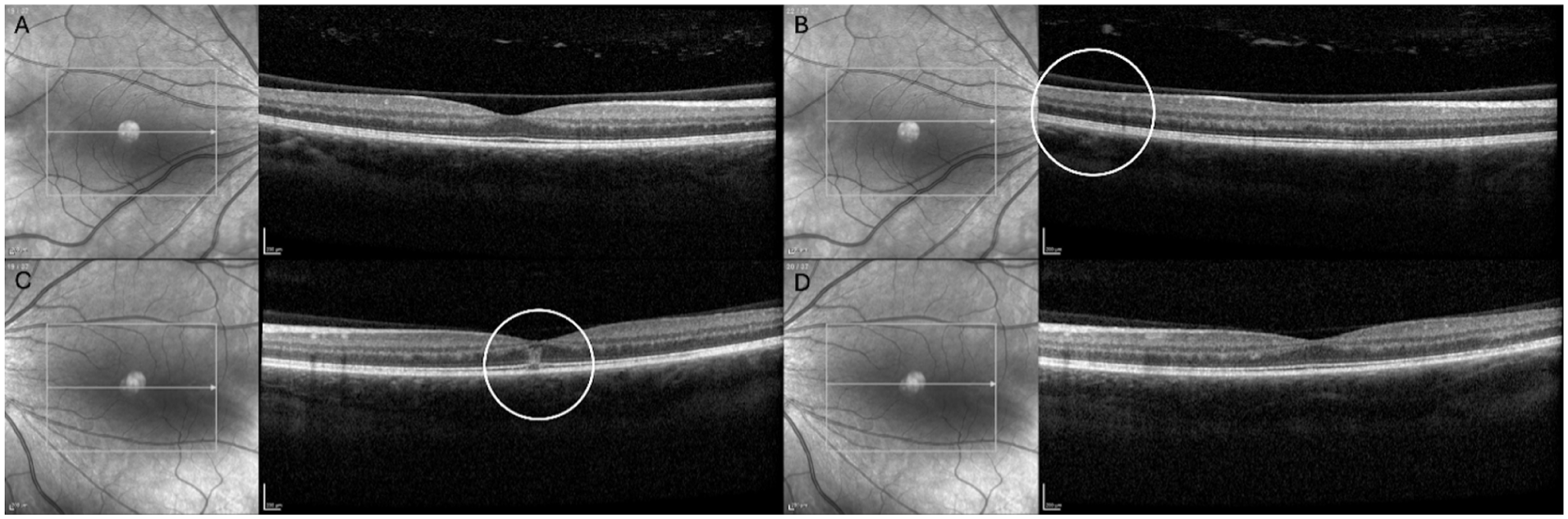
Optical coherence tomography (OCT) images of the macula obtained at presentation. (A) The foveal OCT scan of the right eye appears normal. (B) In the superotemporal macula of the right eye, focal thinning of the outer nuclear layer (ONL) is observed (white circle). (C) OCT through the fovea of the left eye demonstrating a hyperreflective band involving the ONL with associated disruption of the ellipsoid zone (EZ) and interdigitation zone (white circle). (D) An additional lesion in the left eye showing increased hyperreflectivity of the outer plexiform layer and ONL, with attenuation of the underlying EZ.
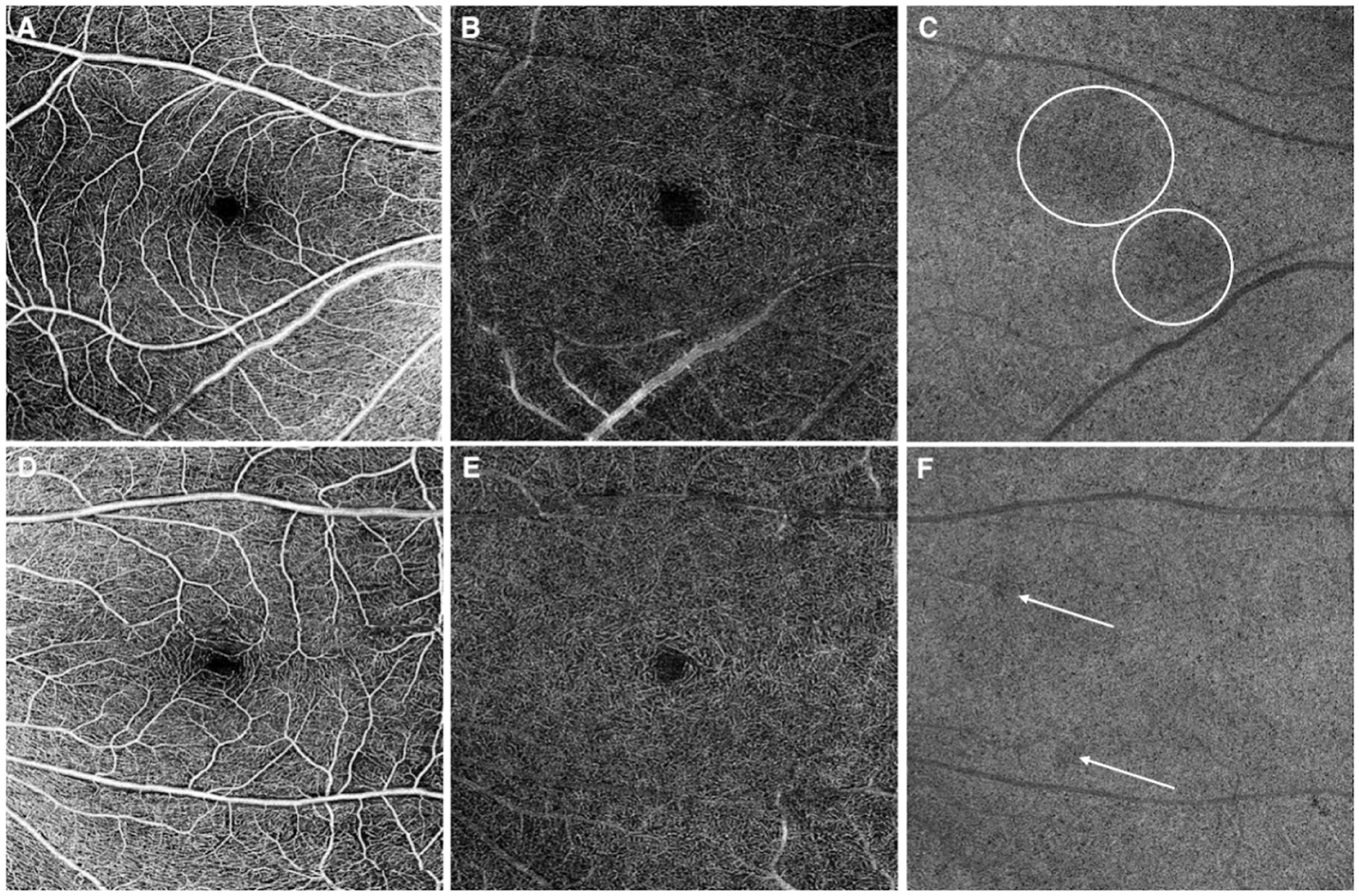
Macular 6 × 6-mm swept-source optical coherence tomography angiography scans obtained at presentation. (A, D) Superficial capillary plexus images demonstrating a small, irregular foveal avascular zone in both eyes. (B, E) The deep capillary plexuses appear intact in both eyes. (C) En face choriocapillaris images of the right eye revealing 2 large, wedge-shaped flow deficits (white circles) corresponding to areas of hyporeflectivity on near-infrared reflectance imaging. (F) The left eye demonstrating subtle, smaller flow deficits (white arrows).
At the 1-year follow-up, FA revealed persistent areas of late vascular leakage, which were managed with observation. Genetic testing for genes associated with Adams–Oliver syndrome and familial exudative vitreoretinopathy (FEVR) showed no pathogenic or likely pathogenic variants. However, a variant of uncertain significance was detected in the VCAN gene. At 2 years of follow-up, the patient’s central scotoma had resolved spontaneously, accompanied by resolution of hyperreflectivity of the OPL and ONL, without any intervention.
Conclusions
Adams–Oliver syndrome is a congenital vasculopathy that is most commonly associated with mutations in the Notch signaling pathway, which plays a crucial role in vascular development and pericyte recruitment. 12 Impaired pericyte investment may disrupt normal vascular maturation, resulting in peripheral retinal nonperfusion, capillary dropout, and neovascularization.13,14 These features closely resemble those observed in FEVR, which is typically caused by mutations in the Wnt signaling pathway. Despite differing molecular mechanisms, both the Notch and Wnt signaling pathways play critical roles in vascular development, offering a plausible explanation for the overlapping retinal phenotypes observed in these conditions.
Ocular manifestations of Adams–Oliver syndrome are heterogeneous and less well-defined in the literature. Recent reports have highlighted retinal vascular anomalies resembling those observed in FEVR.15–17 In the present case, peripheral retinal avascularity, telangiectasia, vascular dragging, and abnormal vascular branching identified on clinical examination and FA demonstrated an FEVR-like phenotype despite negative genetic testing. Supporting this association, Wang et al 18 reported that DOCK6-associated Adams–Oliver syndrome can exhibit an FEVR-like vascular phenotype within a cohort of patients with FEVR.
In addition to Adams–Oliver syndrome, our patient was diagnosed with cutis marmorata telangiectatica congenita, a condition that has also been associated with peripheral retinal vascular anomalies on FA. Prior reports have described peripheral nonperfusion, anomalous vascular branching, and abnormal vessel termination in patients with cutis marmorata telangiectatica congenita. 19 As these findings overlap substantially with some of the features observed in our patient, some of the retinal vascular changes could be attributed to cutis marmorata telangiectatica congenita rather than Adams–Oliver syndrome alone. 20 Nevertheless, the coexistence of both disorders complicates attribution of the vascular phenotype to a single underlying condition. Careful assessment of the peripheral retina remains important in such patients to characterize the extent of vascular involvement and guide longitudinal monitoring.
The near-infrared reflectance and OCT findings of wedge-shaped hyporeflective lesions corresponding to hyperreflective bands in the outer plexiform and outer nuclear layers with associated ellipsoid and interdigitation zone disruption were suggestive of AMN and explained the patient’s central scotoma. AMN is thought to result from ischemia at the level of the deep retinal capillary plexus and is commonly associated with systemic hypotension, vasoconstrictive agents, inflammatory conditions, and other ischemic insults. In some patients, involvement of the choriocapillaris has also been reported, suggesting that both retinal and choroidal ischemia may contribute to the disease process.
The patient’s medical history was remarkable for significant syncopal episodes, including one associated with loss of consciousness and perioral cyanosis, as well as vasomotor disturbances such as shower-induced cutis marmorata, suggesting abnormal capillary and venous vasculature and predisposition to diffuse ischemia. In this case, the FEVR-like retinal vascular compromise and peripheral ischemia may have contributed to localized macular ischemia and subsequent AMN. Although AMN can occur in otherwise healthy young women,21,22 the coexistence of AMN with Adams–Oliver syndrome in this patient suggests a mechanistic link between the vasculopathy of Adams–Oliver syndrome and central macular involvement. The patient’s history of systemic lupus erythematosus is also notable, as autoimmune disorders have been recognized as potential contributors to AMN. 23
In addition, oral contraceptive use has been implicated in the pathogenesis of AMN due to its vasoconstrictive and prothrombotic effects. 21 The development of AMN in this patient was therefore likely multifactorial, with contributions from underlying vasculopathy, systemic lupus erythematosus, and oral contraceptive use. However, a complete hypercoagulability evaluation was not conducted.
It is noteworthy that no causative genetic variant is identified in almost half of individuals with FEVR and in about 40% of those with Adams–Oliver syndrome, underscoring the importance of clinical judgment and multimodal imaging in diagnosis.24–27 Although laser photocoagulation of the avascular peripheral retina was considered, treatment was deferred due to the stability of the retinal findings and the patient’s good treatment compliance. Over 3 years of observation, there was no new exudation, hemorrhage, or vascular leakage. Furthermore, both the patient’s visual symptoms and the associated structural retinal changes gradually resolved, with complete normalization of the macular architecture on imaging 2 years later.
Given the potential for progressive, vision-threatening retinal vascular disease and its associated complications, patients with Adams–Oliver syndrome should undergo an initial comprehensive ophthalmologic evaluation followed by long-term monitoring with ultra-widefield FA, particularly those with Adams–Oliver syndrome who exhibit an FEVR-like phenotype.
In conclusion, this case highlights a unique ocular presentation of AMN occurring in the setting of retinal vasculopathy in a young woman with Adams–Oliver syndrome. It underscores the importance of regular ophthalmologic evaluation in affected patients and highlights the role of abnormal vascular development in the pathogenesis of ocular complications in Adams–Oliver syndrome.
Footnotes
Author Note
Dr. Chaaya and Dr. Adibnia contributed equally to this study.
ORCID iDs
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of patient health information were performed in a Health Insurance Portability and Accountability Act-compliant manner.
Consent to Participate
Informed consent was obtained from the patient for participation in this case report.
Consent for Publication
Verbal informed consent for publication of this case report and accompanying images was obtained from the patient.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Patel is supported by the Retina Innovation Fund, Massachusetts Eye and Ear, Boston, MA; The Simouran Family; and the St. Vincent de Paul Foundation. The funding organizations had no role in the design or conduct of this research. No specific funding was received for the preparation of this case report.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Patel is a consultant for Alcon, Alimera, Allergan, Apellis, Atheneum, Biogen, DORC, EyePoint Pharmaceuticals, Genentech, Gerson Lehrman Group, Inc, Guidepoint, Lifesciences, Regeneron, and Regenxbio. Dr. Miller is a consultant for Alcon, Allergan, Carl Zeiss, Genentech, Sunovion, and Topcon, and receives financial support for research from Adaptive Sensory Technology and Intalight. None of the other authors declared potential conflicts of interest with respect to the research, authorship, and/or publication of the article.