
Abstract
Purpose:
To describe the clinical features, antimicrobial susceptibilities, and treatment outcomes of acute-onset exogenous Nocardia endophthalmitis following non-cataract surgery.
Methods:
Two cases were retrospectively reviewed.
Results:
Two patients developed acute-onset exogenous endophthalmitis following non-cataract procedures and subsequently underwent multiple surgical interventions. The first patient developed a fulminant infection in the left eye following revision of a glaucoma drainage implant and ultimately progressed to no-light-perception vision, undergoing enucleation. The second patient developed endophthalmitis secondary to infectious scleritis in the right eye and had a best-corrected visual acuity of 5/200 at last follow-up. Microbiologic analysis identified Nocardia brasiliensis and Nocardia niwae. Both isolates demonstrated susceptibility to amikacin and sulfamethoxazole/trimethoprim, with variable susceptibility to β-lactams and fluoroquinolones.
Conclusions:
Acute-onset exogenous Nocardia endophthalmitis may occur after a variety of ophthalmologic procedures and is associated with a poor visual prognosis despite surgical intervention and targeted antimicrobial therapy. Amikacin and sulfamethoxazole/trimethoprim remain the preferred antimicrobial agents.
Introduction
Nocardia is a rare cause of acute-onset exogenous endophthalmitis, with most reported cases originating from South Asia.1 –5 Although Nocardia endophthalmitis is more commonly described as an endogenous disease in immunocompromised patients, isolated cases of postoperative and posttraumatic exogenous infection have been reported.5,6 Nocardia asteroides is the most commonly identified species associated with endophthalmitis; however, infections caused by several other Nocardia species have also been reported.1,3
Despite these reports, data on the clinical course and antimicrobial susceptibilities of acute-onset exogenous Nocardia endophthalmitis in the United States remain limited, and most postoperative cases have occurred following cataract surgery.1,3 We report 2 cases of acute-onset exogenous Nocardia endophthalmitis following non-cataract ophthalmologic surgeries referred to a tertiary care center, including the first reported case caused by Nocardia niwae.
Case Reports
Case 1
A 44-year-old man was referred for evaluation of a painful, red left eye 6 days after revision of a glaucoma drainage implant. His ocular history was notable for remote cataract extraction with intraocular lens implantation and placement of 2 prior glaucoma drainage implants for primary open-angle glaucoma in the left eye.
On presentation, best-corrected visual acuity (BCVA) was light perception OS and 20/60 OD. Intraocular pressure was 17 mm Hg OS and 16 mm Hg OD, with no afferent pupillary defect noted in either eye. Slitlamp examination of the left eye demonstrated conjunctival injection and exposure of the superotemporal tube, corneal edema, and a mixed layer of hyphema, hypopyon, and fibrin reaction in the anterior chamber. The lens and posterior segment could not be visualized. Point-of-care B-scan ultrasonography demonstrated posterior segment membrane formation.
The patient was diagnosed with acute-onset exogenous endophthalmitis and underwent anterior chamber washout, removal of the glaucoma drainage implants, vitreous aspiration, and intravitreal (IVT) injection of vancomycin 1.0 mg, ceftazidime 2.25 mg, and dexamethasone 0.4 mg.
On postoperative day 2, BCVA remained light perception, and B-scan ultrasonography revealed persistent dense vitreous membranes (Figure 1A). The patient subsequently underwent repeat anterior chamber washout and pars plana vitrectomy (PPV) with fluid–air exchange, endolaser photocoagulation, placement of 1000 cs silicone oil tamponade, and repeat IVT injection of vancomycin 0.5 mg, ceftazidime 1.12 mg, and dexamethasone 0.2 mg. After the second PPV, Gram stain and vitreous cultures from the initial vitreous aspiration, grown on blood, chocolate, and Sabouraud agar, identified Nocardia brasiliensis. Antimicrobial susceptibility testing demonstrated sensitivity to amikacin (minimum inhibitory concentration 1 µg/mL), moxifloxacin (minimum inhibitory concentration 1 µg/mL), and sulfamethoxazole/trimethoprim (minimum inhibitory concentration 0.1 µg/mL), with resistance to ceftriaxone (minimum inhibitory concentration 64 µg/mL).
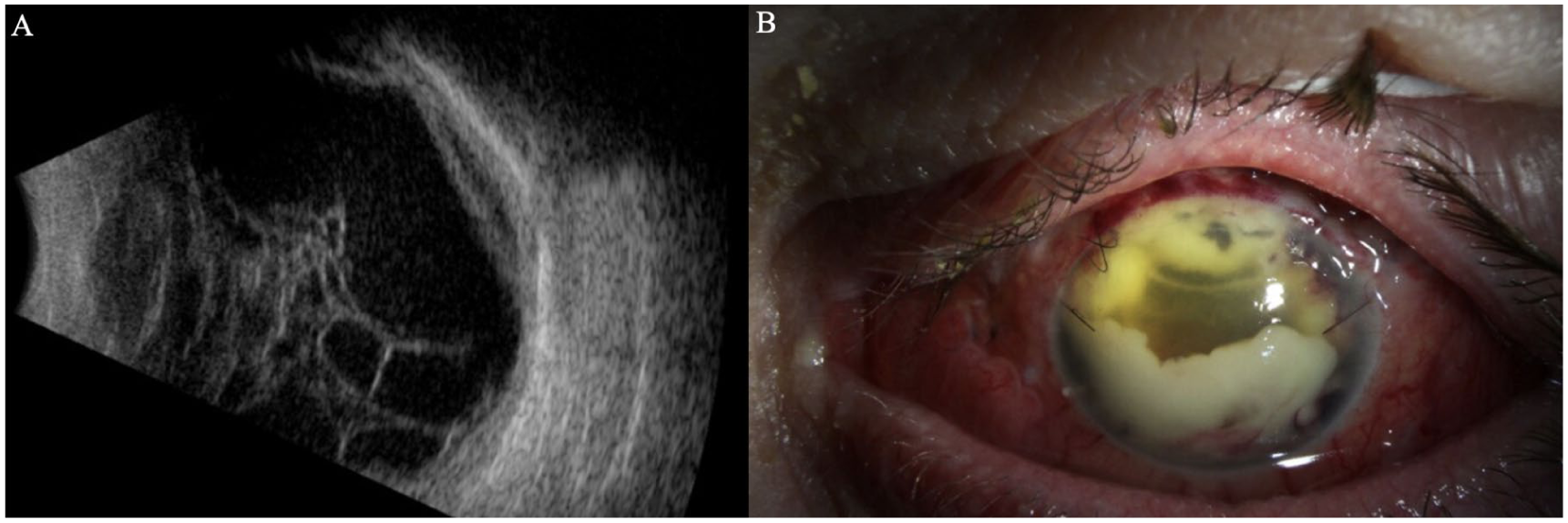
(A) B-scan ultrasonography of the left eye of Patient 1 demonstrating persistent dense vitreous membranes 2 days after anterior chamber washout, removal of the glaucoma drainage implants, vitreous aspiration, and intravitreal injection of vancomycin, ceftazidime, and dexamethasone. (B) Slitlamp image of the left eye obtained 2 weeks after pars plana vitrectomy demonstrating diffuse subconjunctival hemorrhage, corneal edema with nylon sutures, and a mixed layer of hypopyon and hyphema.
Because of progression to no-light-perception vision and worsening ocular pain (Figure 1B), the patient ultimately underwent enucleation.
Case 2
A 69-year-old immunocompetent man was referred for evaluation of a painful, red right eye for 3 days following removal of an extruded scleral buckle 1 month earlier. His ocular history was significant for rhegmatogenous retinal detachment repair in the right eye 10 years earlier and remote cataract extraction with intraocular lens implantation in both eyes. On presentation, BCVA was 20/70 OD and 20/20 OS. Examination revealed isolated inferonasal conjunctival injection and engorged vessels with few cells in the anterior chamber (Figure 2A). B-scan ultrasonography demonstrated an attached and flat retina without significant vitreous opacities (Figure 2B). The patient was treated with hourly fortified topical vancomycin 25 mg/mL and tobramycin 14 mg/mL.

Clinical course of Patient 2. (A) Slitlamp photograph of the right eye at presentation demonstrating focal inferonasal conjunctival injection and engorged episcleral vessels. (B) B-scan ultrasonography demonstrating no significant vitreous opacities and an attached retina. (C) Slitlamp photograph obtained on postoperative day 2 demonstrating an area of inferonasal scleral thinning and whitening covered by amniotic membrane. (D) Slitlamp photograph obtained at postoperative month 1 demonstrating diffuse conjunctival injection and a dense pupillary membrane. (E) Slitlamp photograph obtained at postoperative month 2 demonstrating white and quiet conjunctiva, and resolution of the pupillary membrane and aphakia. (F) Optical coherence tomography of the macula demonstrating diffuse retinal thinning and choroidal folds.
Three days later, BCVA declined to hand motion, with worsening ocular pain and fibrin formation in the anterior chamber. The patient was diagnosed with acute-onset exogenous endophthalmitis and underwent vitreous aspiration with IVT injection of vancomycin 1.0 mg, ceftazidime 2.25 mg, and voriconazole 0.1 mg, along with oral moxifloxacin 400 mg twice daily. Vitreous cultures from the initial aspiration, grown on blood, chocolate, and Sabouraud agar, identified Nocardia niwae. Antimicrobial susceptibility testing demonstrated susceptibility to amikacin (minimum inhibitory concentration 1 µg/mL) and sulfamethoxazole/trimethoprim (minimum inhibitory concentration 0.1 µg/mL), susceptibility to ceftriaxone (minimum inhibitory concentration 4 µg/mL), and intermediate susceptibility to moxifloxacin (minimum inhibitory concentration 2 µg/mL).
The patient subsequently underwent PPV, anterior chamber washout, and 2 scleral debridements (Figure 2C). At postoperative month 1 (Figure 2D), a dense pupillary membrane was noted, and the subretinal abscess had enlarged. The patient subsequently underwent a second and third PPV. At postoperative month 2 after the third PPV, visual acuity (VA) stabilized at 5/200 with aphakic correction (Figure 2E). Optical coherence tomography demonstrated diffuse retinal thinning with choroidal folds (Figure 2F).
Conclusions
Visual outcomes in Nocardia endophthalmitis are consistently poor.1,3,4,7 Several case series have been reported from India, including a study by Haripriya et al, 3 in which 79% of eyes had a VA of hand motion or worse, including 46% with light perception vision. Similarly, DeCroos et al 2 reported that 94% of eyes in a 16-patient series had a final VA worse than 20/200, with nearly 50% retaining hand motion vision or worse. This poor prognosis may be attributable to several organism-specific factors, including a propensity for abscess and biofilm formation on intraocular structures, which may limit the efficacy of IVT antibiotics. 8 In addition, Nocardia demonstrates poor vancomycin susceptibility due to its mycolic acid-rich cell wall and exhibits variable susceptibility to β-lactam antibiotics.1,3 Agents such as ceftazidime may provide inconsistent coverage against Nocardia, as reflected in both prior reports and the present susceptibility data.1,3,4 Antibiotic susceptibility patterns and clinical outcomes from previously published case series of Nocardia endophthalmitis are summarized in Table 1.
Published Case Series Describing Antibiotic Susceptibilities and Clinical Outcomes in Endophthalmitis Caused by Nocardia Species.

Abbreviations: CF, counting fingers; HM, hand motion; NLP, no light perception; NR, not reported; TMP-SMX, trimethoprim-sulfamethoxazole; VA, visual acuity.
When infection with a potentially resistant organism is suspected, early surgical intervention may be considered. Welch et al 9 and Choi et al 10 reported that PPV performed within 24 hours, when combined with IVT antibiotics, was associated with improved VA at the final follow-up compared with cases when PPV was delayed. This approach may be particularly relevant in Nocardia-associated endophthalmitis, as PPV and adjunctive procedures may reduce bacterial load by mechanically debulking abscesses and biofilms.
Appropriate antimicrobial selection is also important. Amikacin demonstrates high activity against Nocardia, with reported susceptibility rates ranging from 87.5% to 100% and no documented resistance among isolated case reports from the US.1,3,4,11,12 As demonstrated in the current 2 cases, sulfamethoxazole/trimethoprim is an effective oral therapeutic option. Similarly, Wang et al 13 reported that 92.2% of Nocardia isolates were sensitive to sulfamethoxazole/trimethoprim.
Although amikacin demonstrates high efficacy against Nocardia, repeated IVT administration carries a small risk of macular toxicity. In patients requiring multiple injections, upright head positioning after injection may be considered to reduce repeated aminoglycoside exposure to the macula and mitigate retinal toxicity. 14
Footnotes
Ethical Considerations
This report was conducted in accordance with the principles of the Declaration of Helsinki. Institutional review board approval was obtained.
Consent to Participate
Written informed consent was obtained from the patient(s) and/or guardian(s) before enrolment in the study.
Consent for Publication
Written informed consent was obtained from the patient(s) and/or guardian(s) for publication of this report and any accompanying images.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by an unrestricted grant from Research to Prevent Blindness (No. GR004596-1).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of the article.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.