
Abstract
Background:
It remains controversial if intravenous thrombolysis (IVT) prior to mechanical thrombectomy (MTE) is superior to MTE alone in patients with acute ischemic stroke caused by large vessel occlusion. We aim to compare functional outcomes, mortality, reperfusion, and intracranial hemorrhage rates in bridging therapy (IVT prior thrombectomy) and MTE alone groups within 6 h from symptom onset.
Materials and Methods:
Consecutive hospitalized patients (September 2017 and July 2018) with acute large artery occlusion within the anterior cerebral circulation eligible for MTE with or without prior IVT were included. A modified Rankin Scale score of 0 to 2 was considered as good functional outcome at 90 days. Successful reperfusion was defined as a Thrombolysis in Cerebral Infarction scale of 2b to 3.
Results:
Of the 124 patients included, 56 (45.2%) received bridging therapy and 68 (54.8%) received MTE alone. Patients receiving bridging therapy were younger (median, 56 vs 63, P = .045) and had shorter onset-to-groin time (median, 270 vs 370 min, P < .001) than those receiving MTE alone. Successful reperfusion rate was significantly greater in the bridging therapy group (87.5% vs 72.1%, P = 0.03). There were no statistically significant differences between the 2 groups in functional independence (bridging 58.9% vs 75.0%, P = 0.07), mortality at 90 days (bridging 14.3% vs 7.4%, P = 0.22), parenchymal hematoma type 2 (bridging 3.6% vs 2.9%, P > .99), and any hemorrhage (bridging 42.3% vs 26.5%, P = 0.07).
Conclusion:
Compared to MTE alone, bridging therapy with IVT improved the reperfusion rate but not other outcomes. Further clinical trials are needed to confirm our findings.
Introduction
In 2015, 5 randomized studies demonstrated superior efficacy of endovascular thrombectomy over standard medical care in patients with acute ischemic stroke (AIS) caused by large vessel occlusion (LVO) of the anterior circulation. 1 Thereafter, endovascular intervention has been approved for routine treatment in clinical practice. 1 Before 2015, only one drug, recombinant tissue plasminogen activator (rt-PA), was approved for use in selected patients within 4.5 h of stroke onset in Europe and within 3 h in the United States. 2 In 2014, a pooled analysis from 5 randomized control trials (RCTs) of intravenous rt-PA showed favorable treatment effects until 4.5 h from symptoms onset, regardless of age and National Institutes of Health Stroke Scale (NIHSS). 3 However, the rt-PA therapy increases the risk of intracranial hemorrhage (ICH) in those with the following factors: high blood glucose, early infarct sign, hyperdense artery sign, age ≥ 75, NIHSS ≥ 10. 4 The incidence of symptomatic ICH in patients who were administered IV rt-PA before mechanical thrombectomy (MTE) are higher than in those without receiving rt-PA, particularly in those with a large ischemic core.5, 6 Intravenous thrombolysis (IVT) may result in the fragmentation of the thrombus, potentially reduce the efficacy of MTE from achieving complete reperfusion of distal vessels, and delay start of the MTE procedure. IVT is a costly therapy. 7 In addition, in the HERMES (highly effective reperfusion evaluated in multiple endovascular stroke trials) collaboration, only 7.6% of patients achieved recanalization with IVT prior to the endovascular procedure. 1 Furthermore, for large thrombi, rt-PA has poor recanalization, with nearly 0% if the size of thrombi is ≥10 mm. 8 More than 85% of patients in these 5 trials were treated with IVT before randomly assigned to receive either MTE or standard care. 1 Only a small proportion of patients with LVO were recanalized successfully, suggesting that early recanalization in response to IVT is uncommon. 9
Despite its low rate of recanalization, IVT could positively influence the clinical outcome after MTE by enhancing the fibrinolytic process, increasing the speed and likelihood of successful reperfusion with MTE, reducing the required number of passes with a stent retriever, and decreasing the frequency of microvascular thrombosis. 10 In addition, achieving recanalization is not always possible with MTE, and such patients may still benefit from IVT. 10 In particular, for some patients, with distal occlusions, IVT alone may result in recanalization, averting the need for combining IVT and MTE.
It remains controversial if IV rt-PA prior to MTE is superior to MTE alone or not. Until now, there has been no clear evidence on clinical outcomes between those receiving combined MTE and IVT versus those receiving MTE alone. 7 We performed this study to compare functional outcomes, reperfusion rate, ICH, death in AIS patients with anterior circulation LVO who received MTE with or without prior IVT within 6 h.
Methods
Study Design and Patient Enrolment
A prospective cohort study was conducted in the Department of Cerebrovascular Diseases, the 115 People’s Hospital from September 1, 2017 to July 30, 2018. We obtained data from patients with AIS with LVO within 6 h in the anterior circulation whose treatments were aligned with current clinical guidelines. Patients were excluded if they had large infarct cores (the Alberta stroke programme early CT score (ASPECTS); ASPECTS < 7 ), were treated with IVT only, or lost to follow-up at 3 months. All patients were treated following current guidelines. The MTE was performed using a stent retriever. For this study, the institutional research ethics of board of the 115 People’s Hospital decided that no formal assessment was needed because of the observational design of the study and because all patient data were anonymized. The local ethics committee waived the need for patient/caregiver consent.
Safety and Efficacy Outcomes
The primary outcome was 90-days functional independence rate (modified Rankin Scale [mRS] 0-2). Secondary outcomes included rates of successful reperfusion (Thrombolysis in Cerebral Infarction [TICI] 2b-3, defined by modified TICI system), safety defined as ICH by the Safe Implementation of Thrombolysis in Stroke-Monitoring Study (SITS-MOST) criteria, and mortality rate. The collateral grading system was scored on a scale of 0 to 3 as in the ESCAPE (endovascular treatment for small core and anterior circulation proximal occlusion with emphasis on minimizing CT to recanalization times) trial. The follow-up of mRS at 90 days was implemented either through a call or on outpatient visit.
Statistical Analyses
We first analyzed and compared the baseline characteristics, treatment data, functional outcomes using chi-square test, Fisher’s exact test (categorical variables), and the Wilcoxon signed-rank test (continuous variables) when appropriated. Patients were matched 1:1 using propensity score matching (PSM) with age, sex, onset-to-groin time, collateral status, location of the occlusion, baseline ASPECTS, and the NIHSS score as covariates. Caliper width of PSM was 0.2. The 90-days functional independence rate, rate of successful reperfusion, and safety and mortality rates were compared between 2 groups before and after matching. Data were analyzed using R (version 3.6.1-R Core Team [2019]), with 2-tailed P values ≤ .05 considered statistically significant.
Results
Study Population
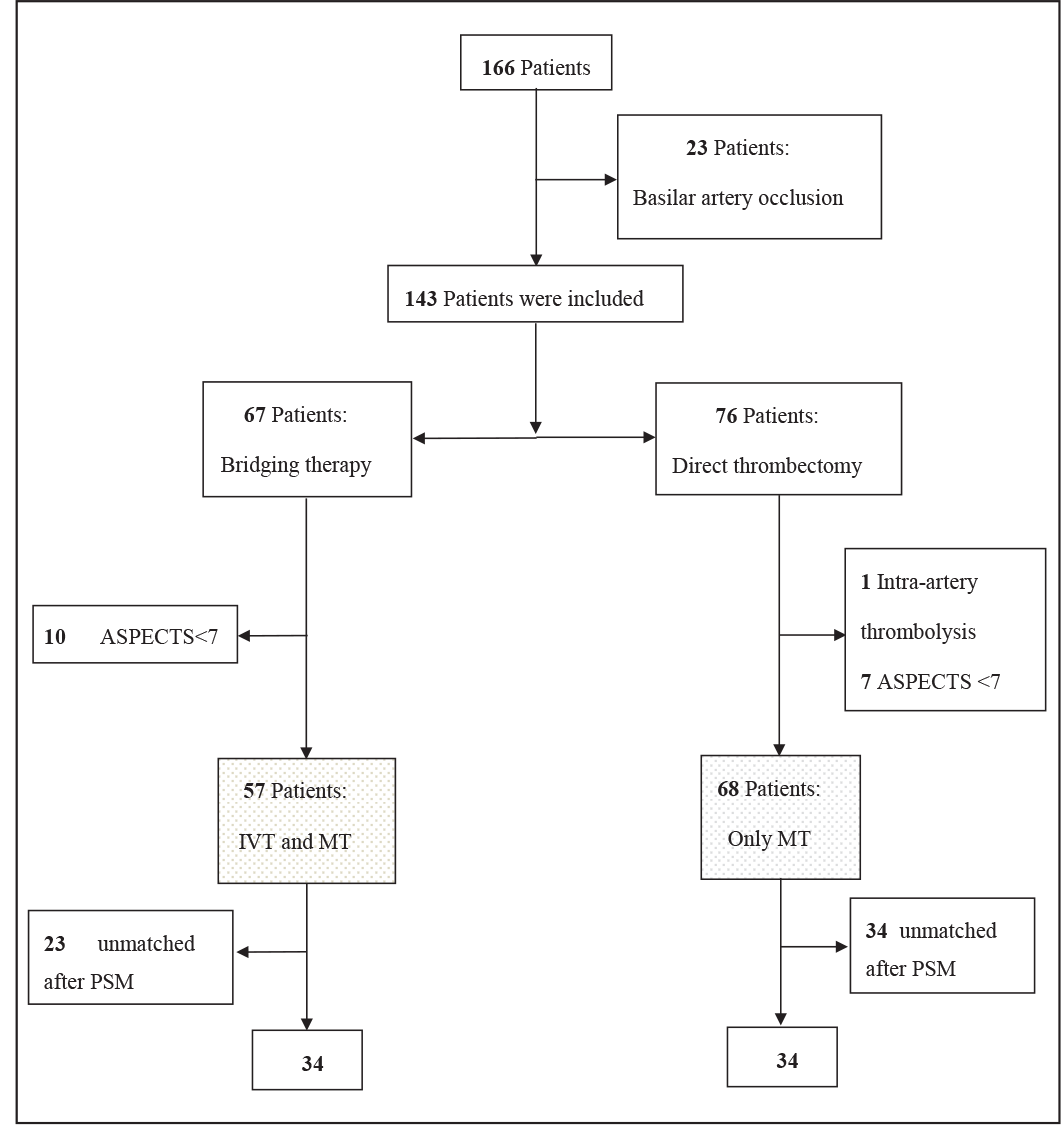
In total, 166 patients were screened. We excluded 23 patients with basilar artery occlusion, 17 patients with large infarct cores (ASPECTS < 7), and 1 patient was treated with intra-arterial thrombolysis. Of 125 enrolled patients with AIS and anterior LVO proven by computed tomography angiography (CTA), magnetic resonance angiography, or digital subtraction angiography (DSA), 57 (45.6%) underwent bridging therapy and 68 (54.4%) were treated with MTE alone. 68 cases (54.4%) were matched using PSM, with 34 patients from each group (Figure 1).
Comparisons of Baseline Characteristics and Outcomes
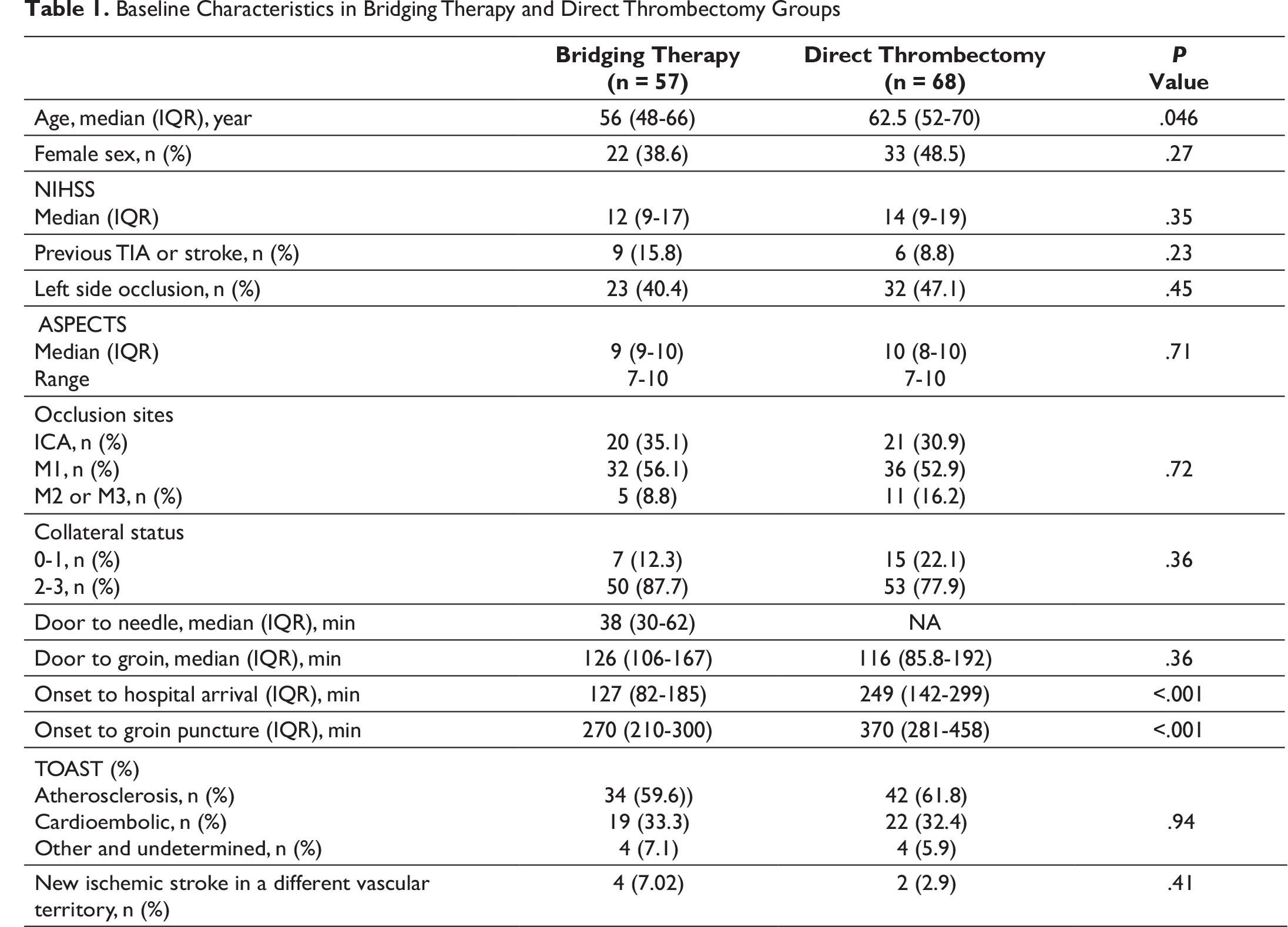
Our univariate analyses showed no statistical differences in the baseline characteristics between 2 groups in the NIHSS on admission, prior history of stroke or a transient ischemic attack (TIA), ASPECTS score, collateral status, location of the occlusion, and onset-to-groin puncture time. However, the patients who underwent bridging therapy were younger than those who underwent MTE alone (56 and 62.5, P = .046). The onset-to-admission time between 2 groups was significantly different (median, 127 and 249 min, P < .001; Table 1).
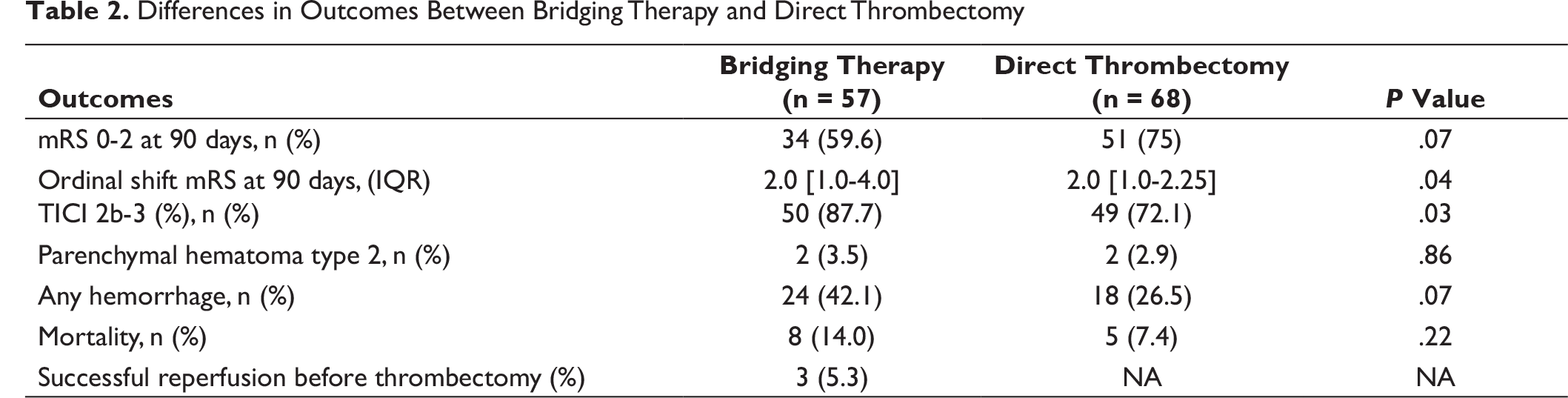
The proportion of patients with functional independence at 90 days was higher in the MTE group than in the bridging therapy group (75.0% vs 59.6%, P = .07), although not statistically significant (Table 2). Successful revascularization rate in the bridging group was significantly higher compared to the MTE group (87.7% vs 72.1%, P = .03).
We found that the rate of parenchymal hematoma type 2 tended to be higher in the bridging therapy group (3.5% vs 2.9%, P > .99), but the difference was not statistically significant. No differences were observed in other types of hemorrhagic transformation and had no significant differences between the 2 groups. Although the mortality rate in the bridging therapy group was higher than in the direct thrombectomy group, the difference was not statistically significant (Table 2).
Flowchart of Patient Selection
Baseline Characteristics in Bridging Therapy and Direct Thrombectomy Groups
Differences in Outcomes Between Bridging Therapy and Direct Thrombectomy
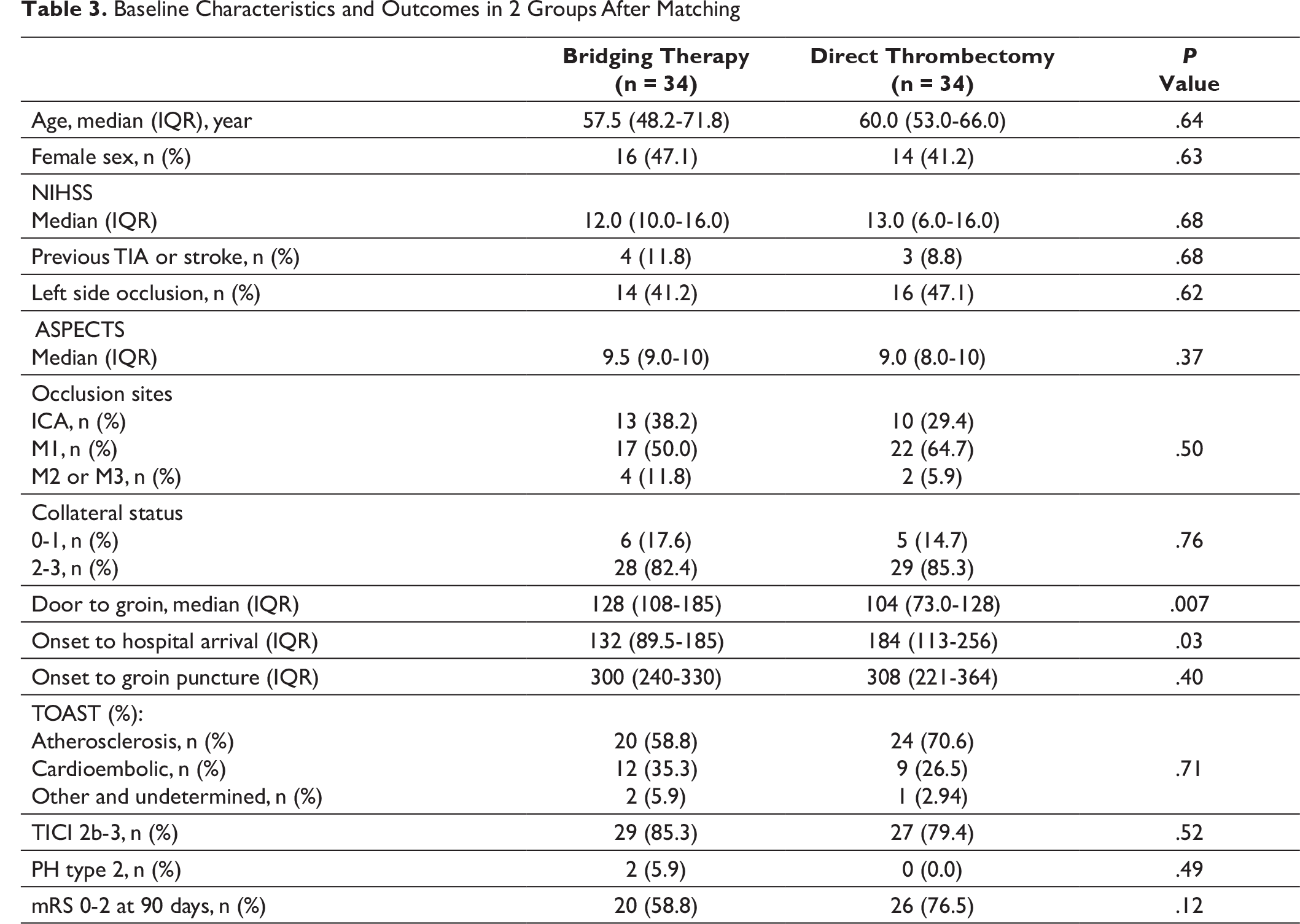
Baseline Characteristics and Outcomes in 2 Groups After Matching
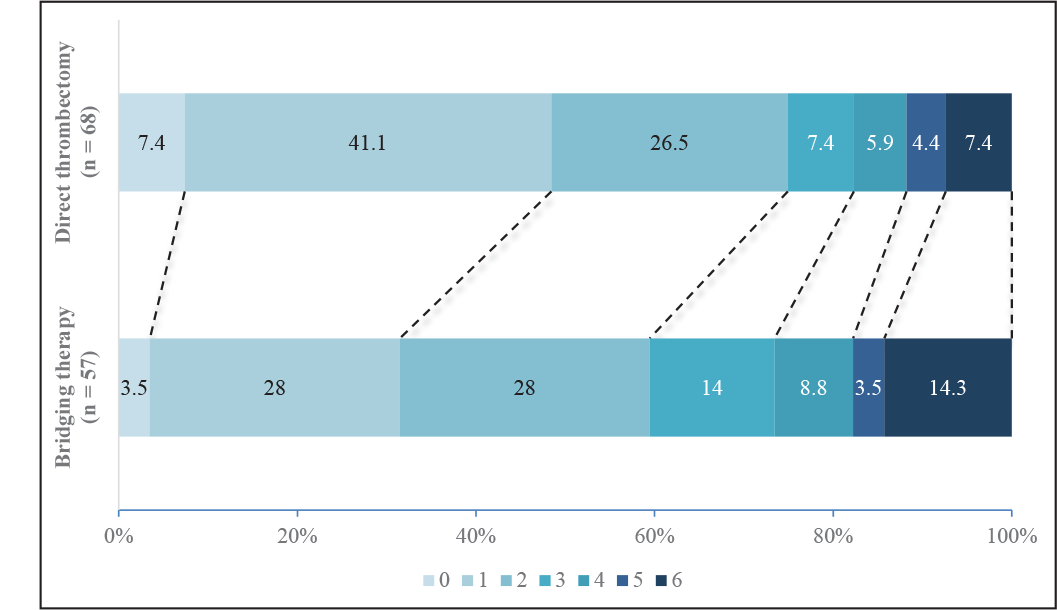
Distributions of mRS Categories in Patients Treated With Bridging Therapy and Direct Thrombectomy Groups
Propensity Score Matching Analysis
After matching, there was no statistically significant difference in baseline characteristics between the 2 groups (Table 3). The 90-days functional independence rate was higher in the direct-MT group, but the difference was not statistically significant (76.5% vs 58.8%, P = .12).
Discussion
In this single-center observational study in a Vietnamese population, we enrolled 125 AIS patients who underwent stent retriever thrombectomy with or without prior treatment with IVT. Although our findings showed that bridging therapy was associated with significantly higher successful recanalization rate in comparison with MTE alone, there was no difference in functional independence, mortality, and parenchymal hemorrhage type 2 (PH2) hemorrhagic transformations between groups.
The rate of functional independence was higher in the direct thrombectomy group compared to the bridging therapy group (Table 2). For ordinal analysis on the mRS scores, which had a significant difference higher (P = .04), however, these results may be biased by the patient’s baseline characteristics. In a direct thrombectomy group, there was higher baseline ASPECTS score, which has been shown to be associated with good outcomes in clinical trials in patients who undergo reperfusion therapy.11, 12 Also, there were 11 patients in the M2, M3 middle cerebral artery occlusion group with 100% functional independence after 90 days follow-up. In our study, the age of the included patients was lower than that of patients in the randomized clinical trials. 1 Our data showed that our patients were treated on time. Mean door-to-needle time was 38 min, mean door-to-groin time were 126 min in bridging and 116 min in direct thrombectomy group, which was shorter than recommendations from current treatment guidelines. Patients’ functional good outcomes were highly early time-dependent. 1
There was extremely low rate of PH2, which was associated with neurological deterioration and higher mortality, 13 in both groups. This is in line with many clinical trials that have good ASPECTS11, 12 and young patients. 11 Also, the rate of any hemorrhage was lower in the direct thrombectomy group. This may be because of the lack of thrombolysis intravenous usage in this group. Previous studies also showed that bridging therapy was associated with significant higher rate of any hemorrhage.14, 15 This may have contributed to the outcomes of our patients.
In the direct thrombectomy group, although successful reperfusion rate was statistically lower, there was higher functional independence. For those patients, all (11/11) in M2, M3 occlusion achieved functional independence after 3 months, though only 63.6% (7/11) had successful reperfusion. A high rate of good ASPECTS and a trend toward lower ICH was noted in this group. 42.6% (29/68) patients within direct thrombectomy group arrived to the hospital early within the IVT time window. However, among those who had contraindications, there was 72.4% (21/29) with mRS 0 to 2 after 3-month follow-up and 75.9% (22/29) with successful reperfusion.
After adjusting, the data showed that there were no statistical difference in independence functional rate, successful reperfusion, and PH2 rate in the 2 groups (Table 3). The PH2 rate was higher in the patients with bridging therapy than those with MTE alone, although not being statistically significant.
Before 2015, IVT was the only approved reperfusion therapy to be used for patients with AIS within 4.5 h. 3 In the ESCAPE trial, only 4.8% (8/165) patients randomly assigned to endovascular thrombectomy group were successful recanalized TICI 2b-3 in the first angiogram. 9 In the MR CLEAN (Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands) trial, this rate was 3.7%. 16 The probability of successful thrombolysis depends on the location of the occlusion whereby the occlusion of the terminal internal carotid artery has worse prognosis than that of the M2 or M3. 17 In our study, full and partial recanalization before MTE were documented in 5.3% (3/57) and 3.5% (2/57), respectively, suggesting that the benefits of IVT preceding MTE remain uncertain, particularly in cases with proximal middle cerebral artery (MCA) and internal carotid artery (ICA) occlusions. There may be new insights gained with Tenecteplase, whereby patients with large LVO were shown to have a significantly higher successful recanalization rate confirmed by the first angiogram, the tenecteplase versus alteplase before endovascular therapy for ischemic stroke (EXTEND-IA TNK) trial. 18 Current guidelines recommend using only noncontrast computed tomography before giving rt-PA, which means that waiting for the evidence of LVO in angiography will delay the onset-to-treatment time. In the worst scenario, reperfusion therapy could be also missed if the endovascular intervention cannot reach the thrombus. In addition, the DIRECT-MT (Thrombectomy in Order to Revascularize Acute Ischemic Stroke Patients with Large Vessel Occlusion Efficiently in Chinese Tertiary Hospitals: A Multicenter Randomized Clinical Trial) study showed no statistical differences in serious adverse events, symptomatic hemorrhage, and death rates between the groups, suggesting safety outcomes of the bridging therapy. 19
The recent study which was conducted by Gamba and colleagues demonstrated that patients receiving combined therapy had higher first-pass success rate and higher recanalization rate compared to those with direct thrombectomy, 20 confirming our study results. In the randomized trial of revascularization with solitaire FR device REVASCAT (randomized trial of revascularization with solitaire FR device versus best medical therapy in the treatment of acute stroke due to anterior circulation large vessel occlusion presenting within eight hours of symptom onset) trial, the efficacy of thrombectomy alone appeared to be better than the combined therapy with prior treatment with thrombolysis, although the difference was not statistically significant. 21 Recently, MTE, the most effective reperfusion therapy, has been demonstrated noninferior to the bridging therapy group in functional outcomes, and overall successful reperfusion on final angiogram. 17 However, another RCT which was presented in ISC 2020 could not prove noninferior of the direct MT therapy in comparison to the bridging therapy. There was a significantly lower rate of any hemorrhage in the direct thrombectomy group (the randomized study of endovascular therapy with versus without intravenous tissue plasminogen activator in acute stroke with ICA and M1 occlusion; SKIP study).
There are several ongoing RCTs worldwide to address this controversial issue. These data from RCTs can help to inform changes in routine clinical practice. However, we should carefully consider skip IVT rt-PA on a case-by-case basis, particularly for patients with ICA occlusion, which was found not effective and posed more risks for symptomatic hemorrhage.
Limitations
This study has a large cohort of AIS patients in a single center that allows us to have enough power to test our hypotheses. We acknowledge the limitations of our study design as a prospective cohort study, not an RCT, with potential bias by onset-to-treatment time in the 2 groups. In addition, our study was limited to the patients with good ASPECTS for both groups. We did not collect data on the recanalization rate on the first angiogram in direct thrombectomy group. In our PSM analysis, differences in characteristics between the 2 groups were adjusted in multivariable models, but the selection bias of this study could not be fully eliminated.
Conclusion
Our study revealed significantly higher successful revascularization rate among patients receiving the bridging therapy (IVT prior to MTE) when compared to those receiving MTE alone. However, compared to direct thrombectomy, bridging therapy did not improve other outcomes including functional independence, mortality, rate of PH2 hemorrhagic transformation, and hemorrhage complications. Further RCTs are needed to confirm our findings.