
Abstract
We report a case of acute pseudo–progressive supranuclear palsy caused by a paramedian thalamopeduncular infarct. The patient presented with a sudden vertical gaze palsy, staring look, and postural instability, mimicking progressive supranuclear palsy. Magnetic resonance imaging showed an acute medial thalamic infarct extending into the midbrain, confirming a vascular etiology.
A 52-year-old male with a history of hypertension and smoking presented with a sudden onset of dizziness, gait instability, and recurrent falls. There was no prior history of neurological disease, and the symptoms evolved acutely over a few hours.
On examination, the patient was conscious, alert, and oriented, with preserved higher-mental functions. Neurological examination revealed a characteristic staring expression (Figure 1A), impaired vertical gaze (both upward and downward), absent convergence (Figure 1B), and sluggish pupillary reactions. Horizontal eye movements were preserved. The vestibulo-ocular reflex was intact, suggesting a supranuclear gaze palsy. No skew deviation was observed.
(A) Showing Staring Look. (B) Nine Gaze Images Showing Impaired Vertical Gaze Upward More Than Downward Gaze, with Minimal Bilateral Horizontal Gaze Involvement with Absent Convergence.

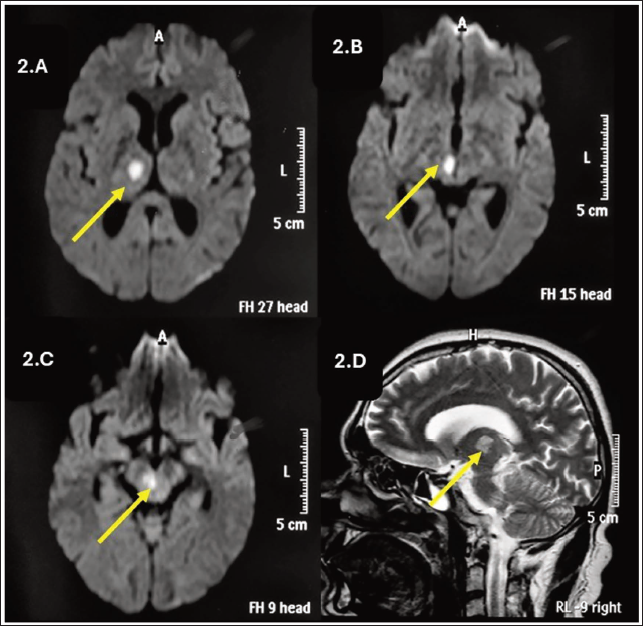
Motor examination showed normal muscle tone and power in all limbs, with no rigidity, bradykinesia, or axial rigidity. Deep tendon reflexes were normal, and plantar responses were bilaterally flexor. There were no features of parkinsonism. These findings were consistent with a progressive supranuclear palsy (PSP) mimic rather than diagnostic of PSP. Magnetic resonance imaging of the brain with diffusion-weighted imaging showed an acute infarct involving the right (unilateral) medial thalamus extending into the rostral midbrain (Figure 2A-2D), consistent with a paramedian thalamopeduncular stroke. The vascular territory likely involved the paramedian branches of the posterior cerebral artery supplying the thalamo-mesencephalic region. No bilateral involvement was noted. Vascular imaging (magnetic resonance angiography) did not reveal large vessel occlusion or basilar artery thrombosis. The patient was managed with antiplatelet therapy and supportive care, showing partial improvement in eye movements over follow-up. Over a follow-up period of 4 weeks, there was an improvement in vertical gaze and convergence, along with better gait stability, allowing independent ambulation.
(A-C) Axial Diffusion-weighted Imaging (DWI) of the Brain Showing Acute Infarct Involving Medial Thalamus Extending to Midbrain. (D) T2 Sagittal Section Showing T2 Hyperintensity Extending from Thalamus to Midbrain.
Discussion
The clinical picture is explained by the involvement of vertical gaze centers in the rostral midbrain, including the rostral interstitial nucleus of the medial longitudinal fasciculus, interstitial nucleus of Cajal, and posterior commissure.1, 2 Infarction affecting these structures disrupts supranuclear control of vertical eye movements, resulting in vertical gaze palsy and impaired convergence. According to established criteria, PSP is a chronic neurodegenerative disorder characterized by progressive vertical gaze palsy, postural instability, and parkinsonism. In contrast, the present case demonstrated an acute onset, absence of parkinsonian features, and clear radiological evidence of a focal vascular lesion, supporting a PSP mimic rather than true PSP.
The differential diagnosis of acute vertical gaze palsy includes Parinaud syndrome (dorsal midbrain syndrome), top-of-the-basilar artery syndrome, Wernicke’s encephalopathy, and other midbrain infarctions. The absence of encephalopathy, nutritional deficiency, and lack of bilateral or diffuse involvement helped exclude these conditions. This case highlights that medial thalamic and midbrain infarction can present as an acute “pseudo-PSP” syndrome. Unlike degenerative PSP, which has an insidious onset and progressive course, vascular PSP mimics present acutely and may show partial recovery.
Conclusion
This case highlights that infarction of the medial thalamus and rostral midbrain can present as an acute “pseudo-PSP” syndrome, and should be considered in patients with sudden PSP-like features.
Footnotes
Declaration of Conflicting Interests
The authors declared no conflict of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval for the study was obtained from the Institutional Ethics Committee, and informed consent was obtained from all participants.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.