
Abstract
Background:
Autistic adults have an increased risk of suicidal thoughts and behaviors, yet little is known about how those supporting them identify or discuss suicide risk. Research suggests that autistic individuals experience unique risk factors, including autistic burnout, sensory overload, and difficulties accessing appropriate mental health support. Despite their elevated risk, autistic individuals are often overlooked in suicide prevention strategies, and their needs are poorly understood in clinical practice.
Methods:
We used semistructured interviews and focus groups to explore how suicidal thoughts and behaviors are identified and discussed with autistic adults. Participants (N = 15) included parents of autistic adults, voluntary sector staff, and health care professionals. We analyzed the collected data using grounded theory methodology, ensuring an in-depth understanding of participant experiences and the generation of a theoretical model.
Results:
We found that conversations about suicidal thoughts and behaviors occurred when autistic individuals were overwhelmed, often triggered by routine changes, interpersonal difficulties, sensory overload, or barriers in navigating support systems. Participants described that they sought to provide a safe environment, demonstrating autism knowledge, engaging in problem-free talk, and considering sensory needs. Risk identification was often based on direct disclosure or targeted questioning. Supporters engaged in immediate responses (e.g., sensory regulation, reassurance, structured problem-solving) and collaboratively developed accessible safety plans, incorporating the individual’s focused interests. Risk assessment was an ongoing parallel process.
Conclusion:
Our research highlights the need for autism-informed approaches to responding to suicide, recommending that supporters recognize triggers such as sensory overload and disrupted routines. Communication should use clear language, structured conversations, and visual or written aids where helpful. Safe environments can be created by considering sensory needs and building trust through problem-free talk. Safety planning must be practical, personalized, and coproduced. Finally, clinicians require autism-specific training so that suicide prevention strategies are effectively tailored.
Community Brief
Why is this an important issue?
Autistic adults face a higher risk of experiencing suicidal feelings or dying by suicide compared with the general population. However, carers, health care staff, and volunteers often struggle to identify and discuss these feelings effectively. Without this understanding, we may miss opportunities to offer meaningful support and reduce risk.
What was the purpose of this study?
We explored how supporters recognize suicidality in autistic adults and approach conversations about these feelings. Our goal was to develop a framework to help supporters identify distress and respond effectively.
What did we do?
We conducted interviews and focus groups with 15 participants, including carers, voluntary sector workers, and health care staff. Each participant had previously discussed suicidal feelings or actions with an autistic adult. Using grounded theory methodology (GTM), we analyzed patterns in these conversations to understand key processes.
What did we find?
Our study found that conversations about suicidality with autistic adults work best when:
Autistic individuals feel safe and supported in sharing their feelings. Supporters draw on knowledge about the person’s unique experiences and communication style.
We identified four key processes in these interactions:
Recognizing distress: Identifying when an autistic person feels overwhelmed or at risk. Exploring meaning: Understanding the reasons behind their feelings and what they are trying to communicate. Providing immediate support: Helping to reduce distress in the moment. Planning the next steps: Assisting with long-term support options.
Throughout these steps, supporters also assess risk to ensure the person’s immediate safety.
Why does this matter?
Our findings highlight the need to create safe, judgment-free spaces for discussing suicidality, which contrasts with traditional approaches that focus primarily on clinical assessments. We also emphasize the importance of adapting support strategies to align with autistic individuals’ unique communication styles and needs.
What are the study’s limitations?
Because we focused on supporters’ perspectives, we did not directly capture autistic adults’ experiences. Future research should include their voices to gain a more comprehensive understanding.
How will this research help autistic adults?
By clarifying how to recognize and respond to suicidality in autistic adults, our findings can inform training programs for carers and professionals. We emphasize the need to create supportive environments and adapt interventions to meet autistic people’s specific needs.
Background
Autistic individuals are at a significantly higher risk of suicidal thoughts and behaviors, with research showing increased rates of suicidal ideation, attempts, and completed suicide compared with the general population.1,2 A UK review of coroners’ inquest records found that individuals who died by suicide exhibited significantly higher levels of autistic traits—whether diagnosed or undiagnosed—than would be expected in the general UK population. 3 Identified risk factors include a history of self-harm, 4 familial suicidal thoughts and behaviors, 5 and experiencing abuse, 6 although many of these are also cited in the general population (e.g., abuse; Molnar, Berkman, and Buka, 7 familial suicide; Tidemalm, et al. 8 ). Kõlves et al. 9 found more than 90% of autistic people who attempted or died by suicide had a comorbid psychiatric condition, with Attention Deficit Hyperactivity Disorder (ADHD) cited as the most prevalent. However, the co-occurrence of autism and ADHD did not further increase the risk of suicide compared with autism alone. 9
A cohort study by Kõlves et al. 9 found that protective factors such as older age and higher educational level do not confer the same protection for autistic individuals. Pelton et al. 10 propose that stressors related to being autistic—such as societal pressures, anxiety, and depression—can increase feelings of perceived burdensomeness and thwarted belonging, leading to suicidal desire. Arnold et al. 11 suggested that the stress of navigating a neurotypical world and the need to mask one’s identity may contribute to autistic burnout, which is linked to increased suicidal thoughts and behaviors (including ideation, plans, attempts, and completed suicide). 11 A review by Cleary et al. 12 noted a lack of consistency in demographic variables that could increase suicide risk among autistic individuals, highlighting the complexity of understanding this issue and the “void in the existing research,” with none of the 39 studies included discussing approaches to suicide awareness and prevention for autistic people, and only one was qualitative. Calls have been made to screen for autistic traits in patients presenting with suicidal thoughts and behaviors, and to remove barriers to accessing support. 3 Autistic people have asked for individually tailored mental health support, and described difficulties in accessing appropriate support, 13 particularly since the COVID-19 pandemic. 14 Despite elevated suicide risk in autistic people, research suggests that clinicians are more likely to identify neurotypical people as higher risk. 15 Clinicians reported greater self-efficacy when screening neurotypical clients, used safety planning at similar rates across groups, but considered it more acceptable for neurotypical clients. 15
Recently, there has been some attempt to adapt approaches (including policy, screening measures, psychological theory, training, and resources), to better identify and manage risk of suicide for autistic people with the key approaches, their adaptations and limitations are described below:
This area of research has seen growing interest and publications in the past 7 years as highlighted by a recent systemic review.
45
However, at the time of conducting this research there was so little published on how suicide is identified and discussed with autistic people, we sought to fill this gap, by developing a theoretical understanding of how suicidal thoughts and behavior are identified and discussed with autistic adults. We included both practitioners and informal carers or supporters of autistic people. This approach is important, as the NHS Five Year Forward View
46
notes that nonprofessional carers are central in the delivery of health and social care, with the World Health Organization (WHO) publishing a whole toolkit to ensure that expertise in communities is understood and utilized as part of suicide prevention.
47
Magiati et al.
48
found that 50% of autistic adults required ongoing support from parents or carers, who play a key role in increasing autistic people’s access to mental health services.
37
This research also responds to calls for more qualitative studies in this area.
12
We set the following research questions:
How are carers/supporters and practitioners identifying risk of suicide in autistic adults they support? When risk is identified, how are conversations about suicidal thoughts and behaviors initiated with autistic adults? What areas would a carer/practitioner explore with autistic adults when discussing suicidal thoughts and behaviors?
Methods
Procedures
We completed both one-to-one interviews and focus groups with 15 carers/supporters, NHS staff, and voluntary sector workers to examine the experiences of supporting autistic adults around suicidality. We adopted a constructivist grounded theory methodology (GTM),49,50 following Charmaz and Thornberg’s guidelines 51 to ensure quality and rigor. We chose GTM because, following an open and critical reading of the literature, we identified limited knowledge regarding how these processes unfold with autistic people. A semistructured interview and focus group schedule were developed by the research team, which included clinical psychology and qualitative research expertise (see Supplementary Appendix; further details below). Consistent with the GTM, questions were adapted iteratively as salient issues emerged. Ethical approval was granted by the UK National Health Service (NHS) Research Ethics Service and relevant Research Ethics Committees. All participants provided informed consent, were debriefed, and were offered support resources at multiple points, given the sensitivity of the topic.
Community involvement
Before data collection, we held a patient and public involvement (PPI) consultation with four autistic adults (two men, two women) recruited via the NHS Trust’s PPI service. They reviewed draft research questions and advised on inclusive recruitment, accessible language, and dissemination. Their input led to the inclusion of carers, other supporters, and voluntary sector staff in the sampling strategy and to plans for sharing findings with local NHS teams. We provided feedback to PPI participants on how their suggestions were implemented.
Recruitment and eligibility
Eligible participants had supported an autistic adult (aged 18+, without a learning disability) in the past 24 months and had discussed suicide with that individual. Supporters of autistic people with a learning disability were excluded because autistic adults without learning disability are at highest risk for depression 52 and suicidal thoughts and behaviors 53 ; our aim was to focus on autistic traits rather than support needs linked to learning disability. Carers/supporters were recruited through a voluntary sector support service; health care staff were recruited via services connected to the hosting NHS Trust and local autism organizations.
Professionals who had supported someone who died by suicide in the preceding 12 months, or who were involved in an ongoing investigation into such a death, were excluded from the study. We felt that this exclusion provided an important safeguard for participant well-being, allowing individuals some distance from particularly difficult experiences with this theme. Carers or supporters bereaved by suicide within the last 24 months were also excluded for the same reason. In this case, a longer period of time was considered appropriate given the differing nature of these relationships, and because professionals might have access to employment-based support such as clinical supervision or other therapeutic provision.
In addition, carers or supporters who identified as autistic, or who had a diagnosis of autism at the time the research was conducted, were excluded due to potential risks of rumination and the possible impact this might have had on their well-being. The decision to exclude carers or supporters with a diagnosis of autism was informed by several considerations. At the time this project was being developed (beginning in 2017), there was very little published qualitative research exploring autism in relation to suicidal thoughts and behaviors. As such, there were concerns that autistic people might experience heightened or prolonged focus on distressing thoughts or events, which could increase the risk of emotional distress or exacerbate mental health difficulties. Furthermore, as the project was led by a trainee clinical psychologist, available resources were limited and did not allow for the level of support and accommodations that might have been required to safely and ethically include autistic carers or supporters if difficulties arose during participation. We acknowledge that this exclusion may reflect a neurotypical bias and constitutes a limitation of the research, and we return to consider its implications further in the Discussion section.
Participants
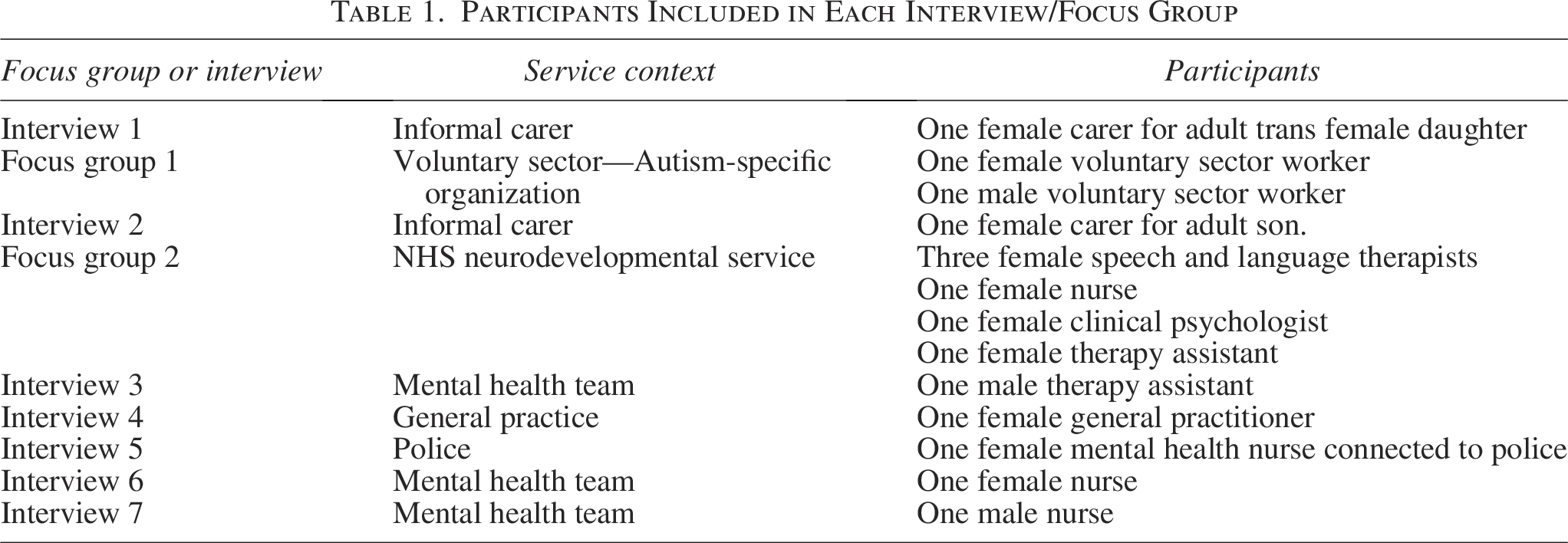
Fifteen participants took part: 2 carers/supporters (both parents), 11 NHS staff, and 2 voluntary sector workers. Two focus groups were conducted (one with voluntary sector staff; one with the NHS neurodevelopmental staff) and seven individual interviews were completed. To protect identities in this small, localized sample, demographic information is presented in aggregate (Table 1).
Participants Included in Each Interview/Focus Group
Interviews and focus groups
Participants chose their preferred format (interview or focus group). All sessions were conducted in person (see Table 1 for composition). Combining focus groups and interviews is both practical and complementary, 54 and offering choice was important given the sensitivity of the topic. One focus group was the voluntary sector staff, and the other was an NHS neurodevelopmental service. Voluntary sector staff and carers/supporters were interviewed at the voluntary organizations’ offices; NHS staff sessions took place in participants’ workplaces.
The interview schedule (Supplementary Appendix) began with introductions and a check-in to gauge well-being and readiness. Eligibility and confidentiality were reviewed, and written information and consent were provided. Core questions addressed how participants identified suicidality in autistic people; how, when, and where conversations about suicide were initiated; and the content of those discussions. Sessions closed with reflections on the interview itself and opportunities to raise concerns. All participants received an information sheet with contact details for support services. The same schedule and well-being check-ins were used for focus groups.
Researcher positioning
The research team did not include autistic members. Recognizing this limitation, we explicitly considered potential biases throughout the study. The lead researcher maintained a reflective diary to track assumptions, values, and motivations, discussed in supervisory meetings. Researcher positionality was a standing agenda item in team discussions to ensure reflexivity during data collection and analysis.
Data analysis
Analysis followed constructivist grounded theory principles,49,50,55 with data collection and analysis proceeding concurrently. Interviews were audio-recorded, transcribed verbatim within 48 hours, and analyzed concurrently with data collection.
The lead researcher began with line-by-line open coding to ensure close engagement with the data, documenting early insights in reflexive memos. After the first four transcripts, coding progressed to sentence level and then paragraph level as familiarity deepened. Substantive coding then grouped codes into categories, refined through constant comparison within and across transcripts.
Analytic rigor was supported through theoretical sampling (whereby emerging insights informed subsequent questioning and recruitment) and sustained memo-writing to capture analytic decisions and theoretical reflections. Relationships between categories were explored iteratively—including testing rival explanations and diagramming conceptual links—to develop a coherent explanatory framework. These were discussed by all three authors in regular project meetings. Data collection ceased at theoretical sufficiency, when no new insights substantively altered the developing theory.
Credibility was enhanced through supervisory review of extracts, codes, and memos, providing opportunities to challenge interpretations and ensure reflexivity. To further strengthen trustworthiness, a summary of the emergent model was shared for member checking: both carers confirmed resonance with their experiences; NHS staff did not respond, possibly due to COVID-19 pressures. Findings were subsequently disseminated to the local NHS and voluntary sector teams, and participants reported that their perspectives had been represented faithfully.
Results
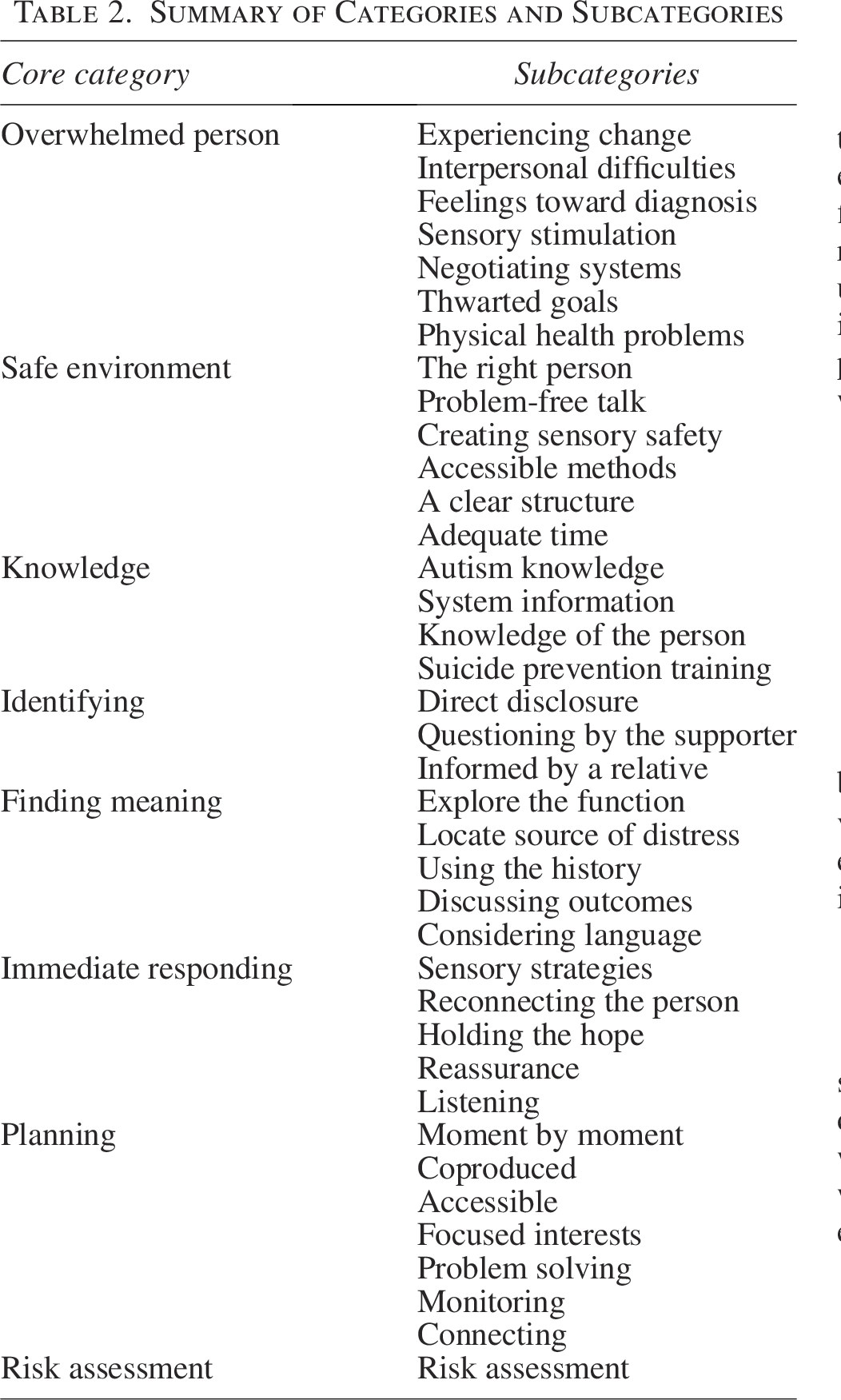
Eight core categories emerged, each with several subcategories, which are summarized in Table 2. These core categories are as follows: Overwhelmed person (e.g., experiencing change, sensory stimulation, interpersonal difficulties), safe environment (e.g., problem-free talk, sensory adjustments), knowledge (autism knowledge, system information), identifying (direct disclosure, targeted questioning), finding meaning (exploring function, locating sources of distress), immediate responding (sensory grounding, reassurance, holding hope), planning (coproduced, accessible safety strategies), and risk assessment (an ongoing, parallel process). These categories are described in detail with supporting quotes below (core categories are in bold, subcategories underlined). Figure 1 conceptualizes the theory and its interactions. The process begins with the overwhelmed autistic person, situated within conditions that create a sense of safety. Within this safe environment, the supporter draws on their knowledge of autism and suicide to guide a sequential process: identifying suicidality, finding meaning in the disclosure, responding in the moment, and planning beyond the encounter. At each stage, the supporter also gathers information that contributes to a continuous process of risk assessment.
Summary of Categories and Subcategories
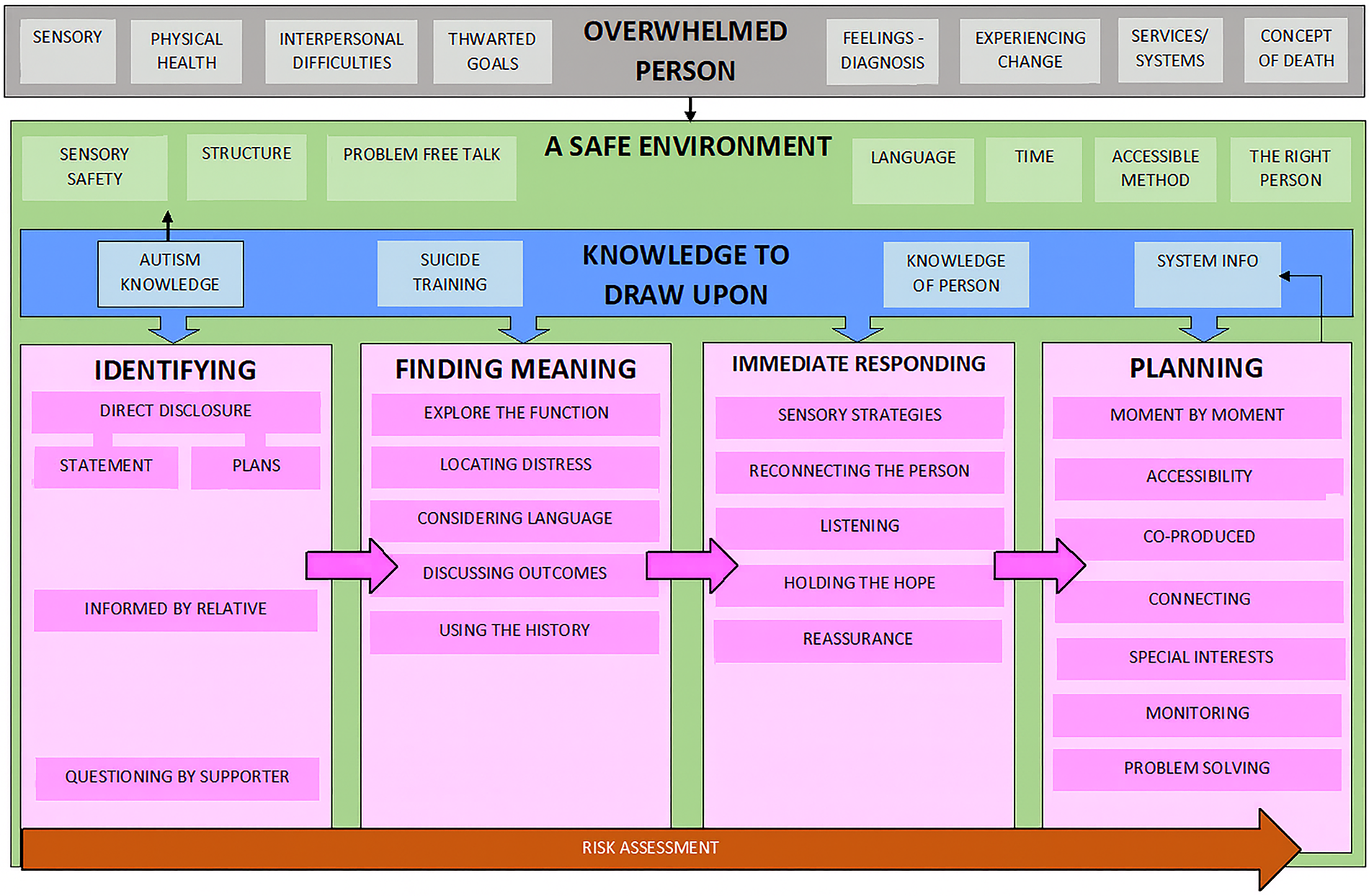
A model illustrating how suicidal thoughts and behaviors are identified and discussed with autistic adults. The process begins with the overwhelmed autistic person, situated within conditions that foster safety. Supporters then draw on their knowledge to guide identification, meaning-making, immediate responding, and planning, while risk assessment runs continuously across all stages.
Overwhelmed person
Participants described that suicidal thoughts and actions were often initiated and identified when the autistic person was overwhelmed, and there were a number of antecedents identified that could contribute to this overwhelm.
Her suicidal thoughts and behaviours will increase in Christmas holidays and summer holidays… her routine changes. It can be as simple as I cut my hair, and look different, and that sent her into spiral. (GP)
Interpersonal events are huge. Being misunderstood or criticised. (Nurse)
Thinking that she’s not popular and that she’s made enemies. (Carer to daughter)
The autistic person’s
It will often be related to having had a new diagnosis, they think they don’t fit in to society. (Voluntary sector worker)
When money is being cut… going through that process. That is one of the main triggers. (Voluntary sector worker)
Not being able to understand the system… Which then builds up into there’s no point in carrying on, because you’re not going to help me. (Therapy assistant)
A lot of trauma from unsatisfactory contact with services, where they’d been labelled as difficult. (Nurse)
Most participants shared examples of autistic individuals being overwhelmed by
Frustration around the sensory side. I can’t cope within this environment. (Therapy assistant)
She had been through a year at university, and failed… she’d always been told that she could have an academic career. (Carer to daughter)
He wanted to join the Navy, but they wouldn’t have him because of his autism. (Carer to son)
A lot of people have significant physical difference. Pain, fatigue, gut issues, and that kind of thing. (Speech and language therapist)
Safe environment
Creating a safe environment for the autistic person to talk allowed them to build trust and feel relaxed. This helped to “disarm the performance” (as stated by a speech and language therapist) or any masking behavior. Conversations had taken place because the supporter was “
The fact… that someone has heard them enough to say “Yeah, you are this highly sensitive person, and you don’t just have to be that stereotypical male… You can see that performance undoing a little as you ask the questions. (Nurse)
I might ask “what do you enjoy doing?”… “I remember once you talked about that videogame” … We can use that. (Voluntary sector worker)
We ask “are the lights alright,” “is the sound OK?” I think that is an instant “you get me.” (Voluntary sector worker)
While face-to-face conversations were the main method described, participants also discussed using
Maybe a diagram or something…. I might do a rating of numbers. (Nurse)
Providing
Say so what we’ll do first is talk about our services, then talk about your life…. I can see people getting more relaxed, “right, now I know what to expect.” (Voluntary sector worker)
You can do a lot in 15 minutes… If I’ve got someone who is distressed or I need more time, I overrun, … or I can schedule more time to see them. (GP)
Knowledge
All aspects of the conversation, from creating the safe environment to the four stages of responding, are informed by having knowledge to draw upon.
I’m often one of the first people they meet who has autism knowledge. I find a lot of the time I’ll speak to people that have been going through all of this and no one in their life knows about autism, and sometimes the people themselves don’t. (Voluntary sector worker)
It might be through looking through care notes that you know they have ongoing thoughts of suicide. (Nurse)
You have that picture of them as part of a community… you know the area of town they are from, the support systems around… so my contextual picture is a lot more holistic. (GP)
Having accessed
The training was really clear that it only allowed us to ask the question and ask the further question “have you got a plan?” and from there we just pass it on. (Voluntary sector worker)
Identifying
Most participants reported that the discovery of suicidal thoughts and behaviors was the result of a
People with a diagnosis of autism can be quite vocal… That might be the first words that come out of their mouth “I’m suicidal.” (Nurse)
He just burst out with it. He said that there was no point in living, that his life had no meaning. (Carer to son).
Sometimes disclosure was prompted by
There’s a real directness that people appreciate. (Nurse)
A less common route to identification was being
His mum will tell us, and the older lady I mentioned, she lives with her mum so she will often tell us as well. (Nurse)
Finding meaning
A key process to finding meaning was participants making an effort to
And what’s happened? What’s shaken up their world so much that they’re contemplating hurting themselves? (Nurse)
Participants made great effort to
What does suicide mean to you? Do you actually want to be dead forever? Never to be here again. Or you want the arguments with your mum to stop? (Nurse)
Take a history. Understanding when they started, the triggers, how they keep safe. (GP)
I told her that if she tried doing that, she would end up failing, but being ill, and turning, being a vegetable. And that worked. (Carer to daughter)
If you did, you wouldn’t be able to watch that favourite TV programme anymore, … do you realise that you wouldn’t be doing that anymore? (Therapy assistant)
An ongoing assessment of what language they use. How they speak to me, what terms they use. I work it in to that. (Nurse)
Immediate responding
Following the identification of suicidal thoughts and behaviors, and the exploration of their meaning, participants described moving into an immediate response phase—providing support and intervention while the person was still in their presence. Participants emphasized the role of using
Sensory boxes out and exploring those kinds of things. And does that make a difference. And taking breaks, all of that. A coffee… I might do a little grounding — mindfulness practice. (Nurse)
After she’s seen the counsellor, I get her to tell me what the counsellor has said, so I can remind her about it…. That’s a positive strategy. (Carer to daughter)
I said to him that we would hold the hope for him until we could give it back. And we made a picture to show him all the things that were being put in place in the meantime, so he could still hold on to, life. (Voluntary sector worker)
I tell him how important he is to me, that people like him and care about him… That his perception of being useless is wrong, that’s just a feeling, but that’s not an accurate feeling, really he does matter. (Carer to son)
Throughout responding it was felt that
She’d heard something on the internet… It was about cyanide in apple pips, and she convinced herself that if she bought enough apples there would be enough cyanide to kill herself…. What I do now, when she talks about these ideas, I just listen, and I realise it is an expression of the pain she is going through. (Carer to daughter)
Planning
Participants described safety planning with the suicidal person, which was frequently shared with other parts of the system either through contacting another person directly and sharing it, or uploading it to a record system so that it becomes part of the system information held.
Participants described planning as being “
If someone is phoning in a crisis you’re not talking about what you can do in a week’s time, you’re talking about the next hour, the next few hours. (Nurse)
This plan is
You might plan out the next few days, what are you going to eat? Have you got any food at home? Maybe plotting out a timetable if that’s the kind of thing they like… And fill it with meeting basic needs. (Clinical psychologist)
This was central to ensuring that the plan is
And we said “what would you do if you felt unwell?” and he said “oh, I’d ring the doctor,” and there is absolutely no evidence at all that he would do this. (Speech and language therapist)
I leave her with something I’ve written down she’s got it there for where I go and then it’s still permanent? (Speech and language therapist)
Engaging them in activity that they like. Because if you have a tendency to have a loss of identity, then it exacerbates those feelings of not being grounded. (Therapy assistant)
Or if they have a psychiatrist or psychologist, I’ll get permission — “Is it OK for me to make contact with your psychologist?” (Voluntary sector worker)
Something practical, even if it’s small, I think they need to be able to see something happening. (Speech and language therapist)
What can we do now? What do you want to do? Shall we take you home, are we going to go back to A&E? Shall we talk to mum? When are you due to see your care team? What distractions can you use? (Nurse)
Ongoing
Closely supervising him. Because he likes to be on his own at times like this… And it’s basically just making sure there are no more attempts… I ask him how he’s feeling. (Carer to son)
Risk assessment
Throughout the processes described (identifying, finding meaning, responding, planning), participants were assessing risk, which then directly influenced the planning. This was felt to be complete when they had enough information about thoughts, level of intent, suicide plans, history, triggers, and protective factors.
I feel like I just carry on asking enough questions until I am confident that I can decide what their level of risk is or what my response needs to be. (Clinical psychologist)
Discussion
This study provides a theory for understanding how suicidal thoughts and behaviors are identified and discussed with autistic adults. This addresses a significant knowledge gap by highlighting the conversational strategies, environmental adjustments, and planning processes that were understood by participants to be helpful. The generated theory suggests that supporters often have these conversations when an autistic person is overwhelmed and a safe environment has been established that accommodates their sensory needs. The supporter then draws upon their knowledge of autism, the person, and the system, identifies suicidal thoughts and behaviors via disclosure or questioning, and responds to this by finding meaning, making an immediate response, assessing risk, and developing a safety plan. For researchers, our theory, as presented in Figure 1, provides a framework to guide future studies examining autistic experiences of suicidality and supporter responses. For practitioners, it functions as a visual guide to structure conversations—emphasizing the importance of first establishing safety, drawing on autism knowledge, exploring meaning, and coproducing plans. For policymakers and service designers, the theory can inform training curricula and highlight areas where systemic adjustments (e.g., sensory environments, autism-informed risk assessment approaches) are needed. In this way, the figure translates our findings into a usable resource that bridges research and applied contexts.
Our research demonstrates that autistic individuals experiencing suicidal thoughts and behaviors often report antecedents that align with autistic burnout, such as cumulative stress, sensory overload, and difficulty accessing support. 56 It is important to distinguish autistic burnout from a mental health condition such as depression as the interventions required are different (e.g., behavioral activation would not be recommended for autistic burnout 11 ). This highlights the importance of integrating an understanding of autistic burnout into suicide prevention strategies, ensuring that interventions are tailored to the needs of this population (as set out in the DHSC National Strategy 57 ).
The generated theory is broadly aligned with the stages proposed by models such as Mental Health First Aid 28 (asking directly about suicide, listening nonjudgmentally, giving reassurance, encouraging the person to seek help, and encouraging the use of self-help strategies) but emphasizes the importance of supporters having knowledge of autism. This further supports the recommendations of the NHS Long Term Plan 58 and Department of Health and Social Care’s National Strategy for autistic children, 57 which also advocate for training in autism for health and social care services.
Our findings also provide insight into the applicability of established theories of suicide to autistic individuals. IPTS suggests that perceived burdensomeness and thwarted belongingness drive suicidal ideation, while acquired capability leads to suicidal behavior. However, our research found that while interpersonal difficulties and feelings of not fitting in were common themes, factors such as sensory distress, routine disruption, and difficulty accessing emerged as more immediate triggers. This suggests that existing models may require adaptation to fully capture the autistic experience of suicidal thoughts and behaviors. Similarly, the IMV model highlights entrapment as a key driver of suicide risk; our findings align with this concept, particularly in relation to autistic individuals feeling trapped within inaccessible systems or unsupportive environments. Future research should explore how these models can be refined to more accurately reflect autistic experiences. Our findings align with recent efforts to adapt suicide theory for autistic experiences. Cassidy et al. (2020) 59 expanded the Interpersonal Psychological Theory of Suicide, showing that camouflaging autistic traits is associated with thwarted belongingness and lifetime suicidality, indicating that interpersonal constructs central to IPTS may operate differently where camouflaging is salient. Cassidy et al. (2023) 60 further embedded autistic experiences within the IMV model, finding that camouflaging relates to defeat and entrapment, and that the link between autistic traits and lifetime suicidality is mediated by camouflaging, defeat, and entrapment. Taken together, these extensions support our emphasis on understanding the meaning and function of suicidality in autistic people and the need for assessment approaches that attend to communicative intent, belonging/burdensomeness, and feelings of defeat/entrapment alongside overt risk indicators.
Our findings reinforce the need for autism-specific adaptations to suicide prevention strategies, such as asking about distress in concrete terms and recognizing signs of autistic burnout. Similar to the findings of Goodwin et al., 38 participants reported using safety planning with this population in ways that closely align with the AASP interventions. Goodwin et al. 38 highlight several key adaptations consistent with our findings: safety plans are most effective when they are coproduced with the autistic person and completed with a trusted supporter, developed flexibly and iteratively, and tailored to individual sensory preferences and formatting needs to ensure usability during distress.
Our research also highlights the importance of understanding autistic communication differences in suicide risk assessment, with participants noting that their ability to identify suicidal thoughts and behaviors depended on their knowledge of autism. For example, the double-empathy problem 61 suggests that communication breakdowns between autistic and neurotypical individuals are due to mutual misunderstandings rather than deficits within autistic people, and that being misperceived by the neurotypical majority can have major implications for an autistic individual’s mental health. 62 Such cross-neurotype communication challenges are particularly relevant in suicide prevention, which may mean that autistic individuals’ expressions of distress are not understood fully or that neurotypical carers/supporters and/or professionals may fail to recognize warning signs.
In our findings, the exploration of meaning and function of suicidal thoughts and behaviors emerged as a distinct and important process in conversations between supporters and autistic adults. Participants often tried to discern whether suicidal disclosures reflected a direct desire to die, or whether they served other functions—such as communicating emotional overload, expressing a need for control, or signaling a call for support. This aligns with research indicating that autistic individuals often experience difficulties identifying and describing emotions (alexithymia), which may contribute to challenges in communicating distress. 63 In this context, suicidal thoughts or behaviors may function as a communicative act, particularly when neurotypical supporters misinterpret distress signals—a dynamic that can be understood through the double-empathy problem outlined earlier. Our findings support calls for suicide risk assessments tailored to autistic individuals, which focus less on traditional verbal disclosure and more on behavioral intentions and the individual function of suicidality. 6
Our research highlights the importance of involving carers/supporters in the care of autistic people, particularly in relation to identifying and responding to suicidal thoughts and behaviors. Consistent with findings from Lascelles et al. (2023), 64 carers/supporters often play a key role in monitoring risk and supporting safety plans, while also liaising with professionals. This collaborative approach—where carers/supporters help identify warning signs and reinforce strategies developed with professionals—can improve detection of risk and adherence to safety planning. However, as the review notes, carers/supporters also need timely support and information to manage the emotional toll and maintain their own well-being. Involving carers/supporters appropriately may therefore enhance outcomes for both autistic people and those who support them.
Many of the factors contributing to suicidal thoughts and behaviors in our study were related to systemic barriers, including difficulties accessing or understanding care, navigating benefits systems, and feeling unsupported within health care settings. Our findings suggest that access to information about autistic people’s needs and experiences is important for professionals responding to suicide, for example, through the use of the digital reasonable adjustment flag on NHS records or tools such as autism passports. 65 These can facilitate supporters to have information about how someone wishes to be supported in a crisis to reduce sensory overwhelm and facilitate communication.40,65
Strengths, limitations, and future research
This study had a number of limitations that could be addressed by further research.
First, autistic individuals themselves were not included as participants, which could be argued constitutes a neurotypical bias in the research. While the study captures the perspectives of those supporting autistic individuals, it does not provide firsthand accounts of how autistic people experience these conversations, what approaches they find most effective, or whether they perceive existing suicide prevention strategies as helpful. Autistic voices are crucial in understanding whether supporters’ assumptions align with autistic individuals’ lived experiences. Since our research was developed and completed, studies have been published that have explored these processes with autistic people themselves, with findings closely aligned with ours. For example, our findings resonate with recent work by Wilson et al., 66 who explored the experiences of 33 autistic adults with histories of suicidal ideation or attempts. They identified the overarching theme of “We don’t know what we don’t know,” alongside four central themes: Communicate with Me, Understand Me, Help Me to Understand Myself, and Support Me—all underpinned by trust and psychological safety. These themes mirror the importance of autism-informed communication, identity validation, and sensory-aware, individualized support identified in our study. Taken together, both studies underscore the need to embed autism-specific knowledge, environmental adjustments, and tailored training into suicide-prevention practice and policy.
Second, the study did not include supporters of autistic individuals bereaved by suicide. The experiences of those bereaved by suicide could provide valuable insights into potential warning signs that may have been missed, challenges in accessing timely support, and whether current risk assessment approaches adequately capture distress in autistic individuals.
In addition, the participant sample was limited in terms of demographic diversity. Most participants were female and British, meaning the findings may not fully reflect the influence of cultural, racial, or gender-related factors on suicide discussions. While women form the majority of the adult social services workforce 67 and are more likely to be carers, 68 the findings cannot reflect how characteristics such as ethnicity and gender might play a role in approaches. One participant was the parent to an autistic and transgender person, and the intersection of identities and how this might affect supporter approaches was not explored in this study. As neurodiversity is elevated in gender-diverse populations, 69 people living at this intersection potentially face additional mental health challenges. 70
Only two carers/supporters, both parents, were able to be recruited for the research. It has been shown that the recruitment of caregivers in research can often be challenging as it requires considerable time for building relationships, aligning values, and establishing trust with these populations. 71 It is perhaps unsurprising that parents were the carers/supporters who responded to recruitment advertisements as autistic adults experience reduced opportunities for employment and may be more likely to live with parents in adulthood compared with other populations. 72 Their addition provided further richness to the theory but may be limited to a parent perspective—other informal carers or supporters might have additional insights.
Finally, data collection occurred during the COVID-19 pandemic, which may have influenced participants’ responses. Increased strain on mental health services and disruptions to usual support systems may have shaped their experiences in ways that differ from the prepandemic or future postpandemic contexts. While this study captures important insights, ongoing research is needed to examine whether suicide prevention strategies continue to evolve in response to changing health care landscapes.
Despite these limitations, this qualitative study provides a foundation for understanding how suicidal thoughts and behaviors are identified and discussed with autistic adults. A major strength of this study is its focus on a rarely explored area—how suicidal thoughts and behaviors are identified and discussed with autistic adults by those who support them. By using in-depth interviews and focus groups, the study captures rich, contextualized insights from NHS professionals, voluntary sector staff, and carer supporters. Many participants were highly attuned to autistic needs, describing communication strategies, sensory adaptations, and planning approaches that align with emerging autism-informed best practice.
Conclusions
Our study provides a theoretical framework for understanding how supporters identify and discuss suicidality with autistic adults. Our findings highlight that these conversations often take place when an autistic person is overwhelmed, triggered by sensory overload, changes in routine, interpersonal difficulties, or barriers to accessing support. Supporters described navigating these discussions by creating a safe environment, drawing on autism-specific knowledge, and using direct and concrete communication.
We identified four key processes in these interactions: Following identification of suicidal thoughts or behavior, supporters then explored meaning by understanding the function of suicidal thoughts, provided immediate support through sensory regulation, reassurance, and structured problem-solving, and planned the next steps with coproduced, accessible safety strategies. Risk assessment remains an ongoing parallel process throughout these steps.
These findings have important implications for practice. Suicide prevention strategies must incorporate autism-informed approaches, ensuring that assessments and interventions account for autistic individuals’ unique needs. Supporters, including clinicians, carers, and voluntary sector staff, should receive training in autism-specific adaptations, such as adjusting communication styles, recognizing distress triggers, and integrating sensory considerations into safety planning. Future research should include autistic individuals’ perspectives to further refine best practices and ensure that interventions align with their lived experiences.
Footnotes
Authorship Confirmation Statement
All the authors contributed to the conceptualization, methodology, analysis, writing, and reviewing and editing of this article. The first researcher completed the interviews and focus groups, transcribing, and led the data analysis.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.