
Abstract
Background:
Autistic people can and do become parents, yet they often feel misunderstood. They fear being judged on their parenting abilities by professionals from health care, social care, and even judicial systems, including the risk of unwarranted and disproportionate child protection investigations or interventions. Despite these concerns being frequently reported qualitatively, they have not been investigated with quantitative data.
Methods:
Using a participatory research framework, we co-constructed a clinical vignette and a set of questionnaire items in collaboration with autistic parents to ensure that the materials reflected their lived concerns and priorities. Professionals from health care, social, educational, judicial, and allied health fields, as well as autistic adults, were invited to complete the survey. We compared their perceptions of a fictional autistic mother, before and after diagnostic disclosure, as well as their views on professional competency regarding autism.
Results:
Although professionals do not hold overtly negative views, their perspectives diverge from those of autistic adults. Professionals perceived the fictional mother with high autistic traits more negatively than did autistic adults before knowing the diagnosis. In addition, judicial, medical, and paramedical professionals were less likely to identify autism than autistic adults. However, participants reported that diagnostic disclosure was somewhat reassuring and decreased their concerns about the mother’s psychological needs. Professionals rated their own competency in autism higher than autistic adults did when evaluating the professionals, although most professionals reported needing further training.
Conclusion:
These results provide support for autistic parents’ concerns about stigma. Divergent perspectives between professionals and autistic adults may be partly explained by a “double empathy problem,” where autistic and non-autistic individuals do not share the same reference frame for behavior. The findings underscore the importance of targeted training on autistic parenthood for all professionals, particularly those with minimal prior autism-specific training, to reduce bias and improve understanding.
Community Brief
Why is this an important issue?
Reports from autism organizations, the press, social media, and some research based on interviews with autistic parents suggest that autistic parents may face unfair judgment and discrimination because of their autism. However, there is still very little research measuring this issue. Research is needed to understand and improve professional practices and support for autistic parents.
What was the purpose of this study?
The study aimed to explore differences in how professionals and autistic adults perceive autistic parents and professionals’ knowledge about autism. We were interested in the views of professionals such as doctors, nurses, psychologists, speech therapists, teachers, judges, or police officers. This was examined in France, where understanding and support for autistic people are still limited. The study was motivated by concerns raised by two autistic mothers who are involved in autism organizations and took part in the research project.
What did the researchers do?
Using a participatory approach, in which researchers and autistic mothers worked together, the two autistic mothers helped identify concerns and challenges faced by autistic parents. The researchers and autistic mothers co-created a fictional case of an autistic mother and an online questionnaire. A total of 124 autistic adults and 988 professionals completed the questionnaire.
What were the results and conclusions of the study?
Professionals judged the fictional autistic mother more negatively than autistic adults did. However, participants’ opinions became more positive after learning that the mother was autistic, which was unexpected. Professionals working in medical- or law-related fields were less likely to recognize autistic characteristics than autistic people. Law professionals also had little autism training. Finally, professionals rated their own knowledge about autism more positively than autistic adults did.
What is new or controversial about these findings?
This study is the first to find evidence backing up the concerns of autistic parents about the unfair judgment they sometimes face from doctors, teachers, psychologists, speech therapists, social workers, and law professionals. We found that many professionals may have difficulty recognizing the characteristics of autism and sometimes don’t have enough training to work with autistic people. This was especially true for law professionals, who often make big decisions about children’s safety and well-being.
What are potential weaknesses in the study?
The professionals who took part in the study may have been more familiar with autism than average professionals. Most participants were females. Professionals were grouped into large categories. The study used a non-standard questionnaire and a single fictional case. The study measured participants’ answers to a questionnaire, which may differ from real-life behaviors. All of these limit our understanding of the issue.
How will these findings help autistic adults now or in the future?
These findings provide evidence about how autistic parents are judged by professionals. It also highlights the importance of including autistic people in research to address the questions that are important to them. The results could help improve training for autistic parents, especially in groups with limited autism training, such as law professionals. The results could also help shape policies that support this training.
Introduction
While there is a growing body of research on autistic adults, research on parenthood remains scarce. 1 Even with possibly challenging experiences such as dealing with sensory sensitivities, this research highlights autistic mothers’ efficacy 2 and the enriching aspects of parenting when one is autistic.3–6 Autistic parents usually prioritize their children’s needs above their own and are highly dedicated to their children.1,5,7,8 Qualitatively, autistic parents describe strong bonds 9 and personal experiences that provide a unique understanding of their children, especially if they are also autistic.8,10,11 Mother–child autism trait similarity has been shown to predict better social functioning and well-being in young children. 12 Parenting can also become a passionate interest for some autistic parents, further enhancing their parenting skills. 9
Despite these positive aspects, autistic parents often feel judged in their parenting skills across different settings, including educational and social environments.5,8,13,14 Autistic parents may experience difficulties communicating with health care professionals.5,9,14 They report a lack of understanding and specific training about autism among providers.5,9,15–17 For autistic adults, and therefore also for autistic parents, past experiences of being misunderstood may reinforce the expectation that professionals will not interpret their behavior accurately or provide appropriate support. 18 For example, autistic individuals report that their communication style or expressions of distress are sometimes misinterpreted (e.g., being perceived as anxious, uncooperative, or lacking insight), which can lead professionals to dismiss their concerns. In addition, autistic individuals, and particularly autistic parents, fear being stigmatized when disclosing their autism diagnoses.5,16,19–21 They are particularly concerned that disclosure might change health care professionals’ attitudes and lead to potential involvement of child protection services in their families,5,19,20,22 which could further exacerbate parental and child stress. This concern may stem from the fears that autism-related behaviors (e.g., differences in communication, sensory responses, or parenting style) could be misinterpreted as indicators of parental difficulties or risks to the child.
While no research has specifically examined child protection services interventions with autistic parents, their concerns may be at least partly justified based on findings from studies on parents with intellectual disabilities. Although child protection services’ functioning and decisions vary across countries, 23 several studies have shown that parents with intellectual disabilities are more prone to be involved in child protection investigations and are more likely to face care applications.24,25 They are also at a greater risk of having their children removed from their care compared with other parents, with single mothers with intellectual disabilities being at particularly high risk.24,26–29 While it is still unknown if this also applies to autistic parents beyond anecdotal evidence, as no quantitative research has investigated this question, qualitative research has highlighted that perceived oddness in autistic mothers can trigger unwarranted interventions from social workers. 30 This can be theorized as ‘cognitive marginalization’ of neurodivergent individuals, that is, the devaluation of atypical cognitive styles when assessing parental competence or risk, leading to reduced credibility and unwarranted professional responses.30,31 Indeed, health professionals and social workers may rely on a normative perspective when evaluating autistic parents, potentially reflecting limited autism-specific training.16,17,19,20
On the contrary, autistic people are less likely than non-autistic individuals or those who are not nuclear family members of an autistic person to stigmatize autism. 32 They also have more scientifically based knowledge on autism. 32 Although the profession of the non-autistic participants is not reported, these findings suggest that lived experience of autism may provide greater awareness of autistic characteristics than individuals without specific autism experience or good and appropriate training.
Despite the concerns about the prejudice that autistic parents may face, no research has explored the perspectives of health care providers, social workers, and judicial professionals on autistic parenting, and there is only limited work on adults with other disabilities. For instance, one study of social workers highlighted that assessing the parenting capacity of parents with intellectual disability was perceived as complex. 33 Another study exploring midwives’ perspective on mothers with mental health disorders indicated that they recognized a lack of knowledge and skills to support this specific population. 34 In addition, other studies have shown that providers lack education and expertise to identify and support autistic adults,35–38 suggesting that this gap may be even greater when working with autistic parents.
The present participatory study aims to fill this knowledge gap by comparing professionals’ and autistic individuals’ perceptions related to (i) autistic parenting and potential stigma and (ii) professionals’ competency regarding autism and autistic parents, to identify training needs. Professionals from a range of sectors, including health and social care, education, and the judicial system (because of their involvement in child protection decisions), as well as autistic adults, participated in the study based on a clinical case and a custom questionnaire. This study was divided into four parts to address our main hypotheses. Our first hypothesis was that professionals would hold more negative perceptions than do autistic individuals, on a fictional mother with high autistic traits, without knowing her diagnosis. Our second hypothesis was that autistic adults would be more likely to identify autistic behaviors in the vignette than professionals who are not trained to identify autism. Our third hypothesis was that revealing an autism diagnosis to professionals would increase their negative perceptions, while it would not change those of autistic adults. Finally, our fourth hypothesis was that perceived professional competency regarding autism and autistic parents would be rated more positively by professionals than by autistic adults.
Method
Community involvement
The study design followed a participatory process. Two non-autistic researchers and health professionals first contacted autistic adults to identify research needs regarding autistic parenting. In the first semester of 2021, we established a research group, composed of the two non-autistic researchers and three autistic adults (two autistic mothers of autistic children and one autistic researcher), to discuss these priorities. We held online meetings according to members’ availability. These discussions shaped the research objectives, grounded in the lived experiences, concerns, and needs of autistic parents. Both autistic mothers were also actively involved in autism organizations in France, ensuring broader representation of autistic parents’ perspectives.
The autistic adults were considered co-researchers39,40 and worked in equal partnership with the non-autistic researchers. 41 All members actively contributed to every stage of the project. We made methodological decisions collaboratively: All members contributed to the refinement of the clinical case vignette, questions, and terminology. Given the group’s small size, we reached decisions by consensus. Autistic members were in the majority within the core research group, ensuring a power balance in their favor. All members approved the final questionnaire and protocol before submission to the ethics board, and participated in recruitment through their networks. Three additional researchers with expertise in statistics and/or autism research joined the team for data analysis and interpretation. We then discussed the results collectively, and all members contributed to writing and editing the article, directly or indirectly (by suggesting modification orally), according to their preferences.
Participants
Between August 30, 2023, and July 30, 2024, we recruited 124 autistic adults (104 females at birth; 78% reported having at least one child; see Table 1 for more detailed demographics) from French autism associations and through social media. To be included, participants had to be over 18 years old, not under legal guardianship, and report an autism diagnosis made by a professional according to international criteria. In addition, we included a question on diagnostic status in the survey, and participants who self-identified rather than having a professional diagnosis were excluded in this study (n = 17) to limit ambiguity in group definition and interpretation of the results.
Demographic Characteristics (Sex at Birth, Percentage of Participants Reporting at Least One Child, and Age Range) for Autistic Participants and Professionals in Each Category
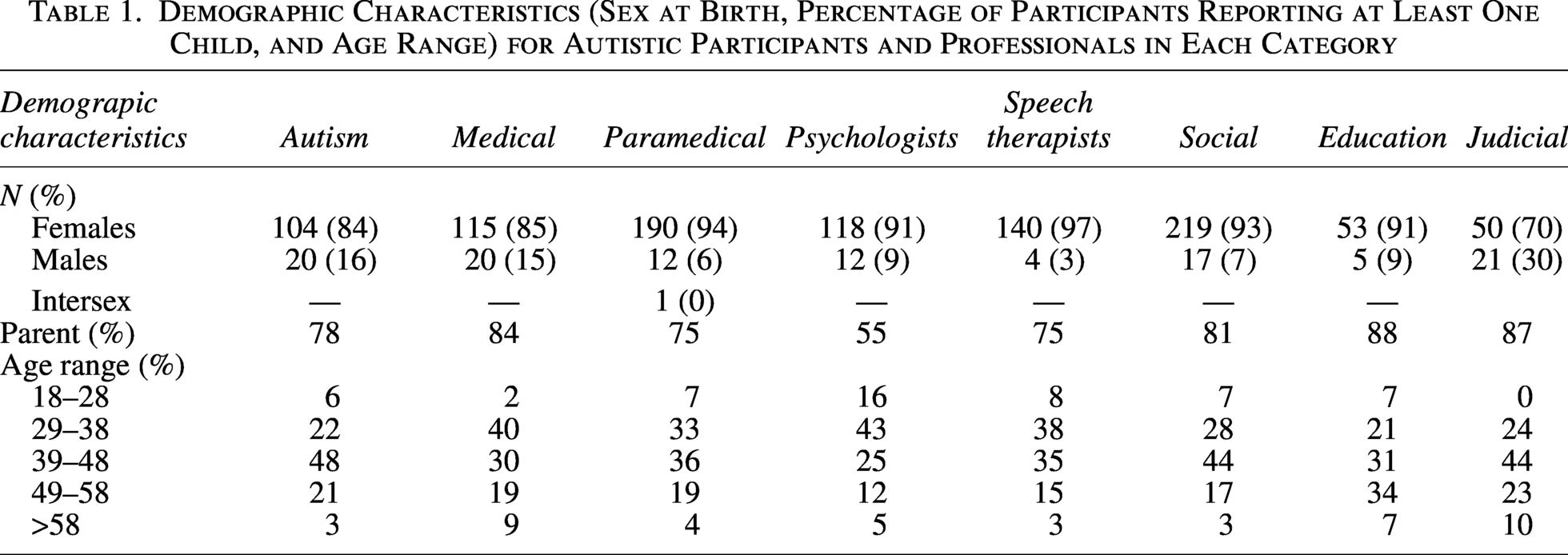
We also recruited 977 professionals (18 years old and above; 885 females at birth, 76% reported having at least one child) from various networks. To allow for clear group comparisons aligned with our hypotheses, the professional group was restricted to non-autistic individuals. They were divided into seven categories based on their current professional occupation: medical (N = 135; psychiatrists N = 50, pediatricians N = 14, general practitioners N = 24, midwives N = 38, other physicians N = 9), judicial (N = 71; magistrates N = 53, police officers N = 18), psychologists (N = 130), education (teachers working in school N = 58), paramedical (N = 203; nurses N = 111, pediatric nurses N = 29, medical assistants N = 2, psychomotor and occupational therapists N = 40, health managers N = 18, physiotherapists N = 2, dietician N = 1), social (N = 236; social and socio-educational professional including educators N = 143, social workers N = 54, community workers N = 20, social/health care managers N = 19), and speech therapists (N = 144). Most professionals may, at some point, face a situation that resembles the one presented in the clinical vignette, either directly or indirectly.
We performed a power analysis using the generalized linear models. The calculated power was greater than 0.8 for the model reported in Hypothesis 1, suggesting that the sample was adequate to detect the observed effects and that the risk of a type II error is low (see the Supplementary Data for details).
Material and procedure
We collected data online using the LimeSurvey platform, which meets data protection and ethical requirements (e.g., GDPR compliance). To reduce the bias regarding the evaluation of the clinical case presented, we described the study as an investigation of parenting needs in adults with physical, sensory, neurodevelopmental, or psychiatric disorders. We provide an English translation of the clinical case and the protocol in the Supplementary Data.
Information and consent procedures were co-developed by autistic and non-autistic researchers to ensure accessibility. Participants could withdraw at any time before completing the survey, in which case their data were not recorded. As participation was fully anonymous, data could not be withdrawn after submission, and this was specified to participants. In the first part, after consenting to participate, participants read a clinical vignette describing a woman caring for her sick child in the hospital. We based the case on a clinical vignette by the NICE (National Collaborating Centre for Mental Health, UK, 2012) and modified it for the study’s objectives. We designed the vignette to depict subtle autistic characteristics without clear indicators of neglect or abuse that would directly require child protective service intervention in France. Following the reading, participants used a slider ranging from 0 (total disagreement) to 100 (total agreement), with 50 representing a neutral position, to answer 8 questions regarding the clinical case (Table 2A). The numerical values were not displayed to participants.
Items Presented to the Participants (A) Items Related to the Perception of the Fictional Mother, Presented Before and After the Autism Diagnostic Disclosure; (B) Additional Items Presented After Diagnostic Disclosure; (C) Items Related to the Perception of Professionals’ Competency
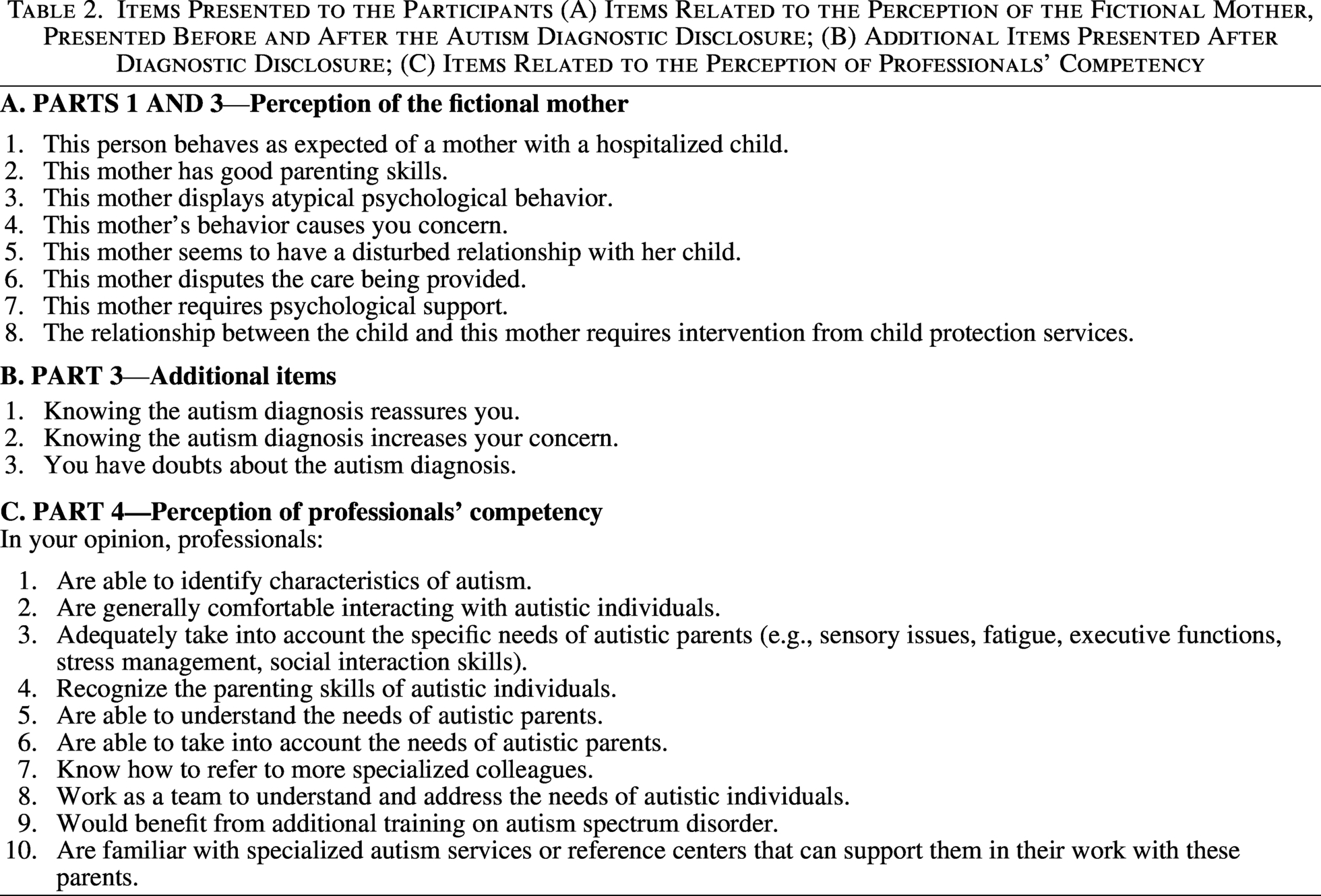
In the second part, participants indicated if the mother or the child’s relationship with the mother suggests a condition or disorder. If yes, participants gave their agreement (Yes/No/I don’t know this disorder) with several conditions, including attachment disorder, depression, autism spectrum disorder, borderline personality disorder, Munchhausen syndrome by proxy, anxiety disorder, schizophrenia, and parental alienation syndrome (as the latter has been often used in French family law 42 ). The terminology used in the questionnaire reflects the wording commonly used in clinical practice in France.
In the third part, after revealing the mother’s autism diagnosis, we presented the same vignette and questions (Table 2A), with three additional items regarding the diagnostic disclosure effect (Table 2B).
Then, we asked socio-demographic questions about age (age range: 18–28, 29–38, 39–48, 49–58, > 58), sex at birth (female, male, intersex), autism diagnosis, employment, and whether participants had received autism-related training of any kind.
Finally, in the fourth part, participants answered questions about their perception of professionals’ competency of autism. We asked professionals to refer to professionals within their own field and autistic individuals to refer to health care professionals. Participants responded using the slider (Table 2C).
All procedures involving human participants complied with the Code of Ethics of the World Medical Association (Declaration of Helsinki), and the study was approved by the local ethics committee (CEREVI/2023/08). No compensation was provided for participation.
Statistical procedure and exploratory factor analysis
We conducted statistical analyses using R software version 4.2.2 43 and Jamovi version 2.6.44. Prior to the main analysis, we performed an exploratory factor analysis (EFA) separately for each of the following parts: perception of the clinical case before the autism diagnosis disclosure, and professional competency regarding autism. We used EFA to reduce the observed items into latent factors, thereby simplifying the questionnaire structure. We recoded reversed items before factor extraction by subtracting each score from one unit above the maximum possible value, ensuring that higher scores consistently reflected the same direction of the underlying construct.
For the analysis of the diagnostic disclosure effect (i.e., same items before and after diagnostic disclosure), we retained the factor structure obtained from the pre-disclosure EFA. We analyzed independently the three additional items specifically designed to assess the diagnostic disclosure effect (i.e., reassure, increase concerns, elicit doubts), without using EFA.
We evaluated sampling adequacy for each EFA using the Kaiser–Meyer–Olkin (KMO) index, with a value >0.60 considered the minimum acceptable threshold. Bartlett’s test of sphericity was required to be statistically significant (p < 0.05). This confirmed the appropriateness of factor analysis. We evaluated internal consistency of each factor using Cronbach’s alpha, with values ≥0.70 considered acceptable for exploratory research and ≥0.80 indicative of good reliability. We retained items when factor loading was ≥0.30, with higher loadings preferred for interpretability.
For each questionnaire, we analyzed factor scores derived from the EFA using a generalized linear model with a gamma distribution and an identity link function, chosen to account for the non-Gaussian distribution of the response variables. The models included respondent categories (education, judicial, medical, paramedical, psychologist, social, speech therapist, autism) and EFA factors as predictors. For the analysis of the diagnostic disclosure effect, we included a time factor (before vs. after) as an additional predictor. We reported results with χ2 values from likelihood ratio tests, degrees of freedom (df), and corresponding p-values for each effect. We conducted post hoc analyses using Bonferroni correction and reported effect sizes for significant interactions using Eta squared (η2). We reported only post hoc comparisons relevant to the hypotheses in the main text and provided other pairwise comparisons in the Supplementary Data for completeness. In addition, we conducted a logistic regression to examine diagnostic opinion, with the binary outcome coded as 0 (non-autism diagnosis) and 1 (autism diagnosis). The respondent category was entered as the predictor. Model results are reported using χ2 statistics, df, and associated p-values. Although data on professionals’ autism-specific training were collected, they were not included as a predictor in the model to preserve model parsimony and interpretability; training was therefore described and considered in the interpretation of the results.
Results
Professionals would hold more negative perceptions than do autistic individuals, on a fictional autistic mother, without knowing her diagnosis.
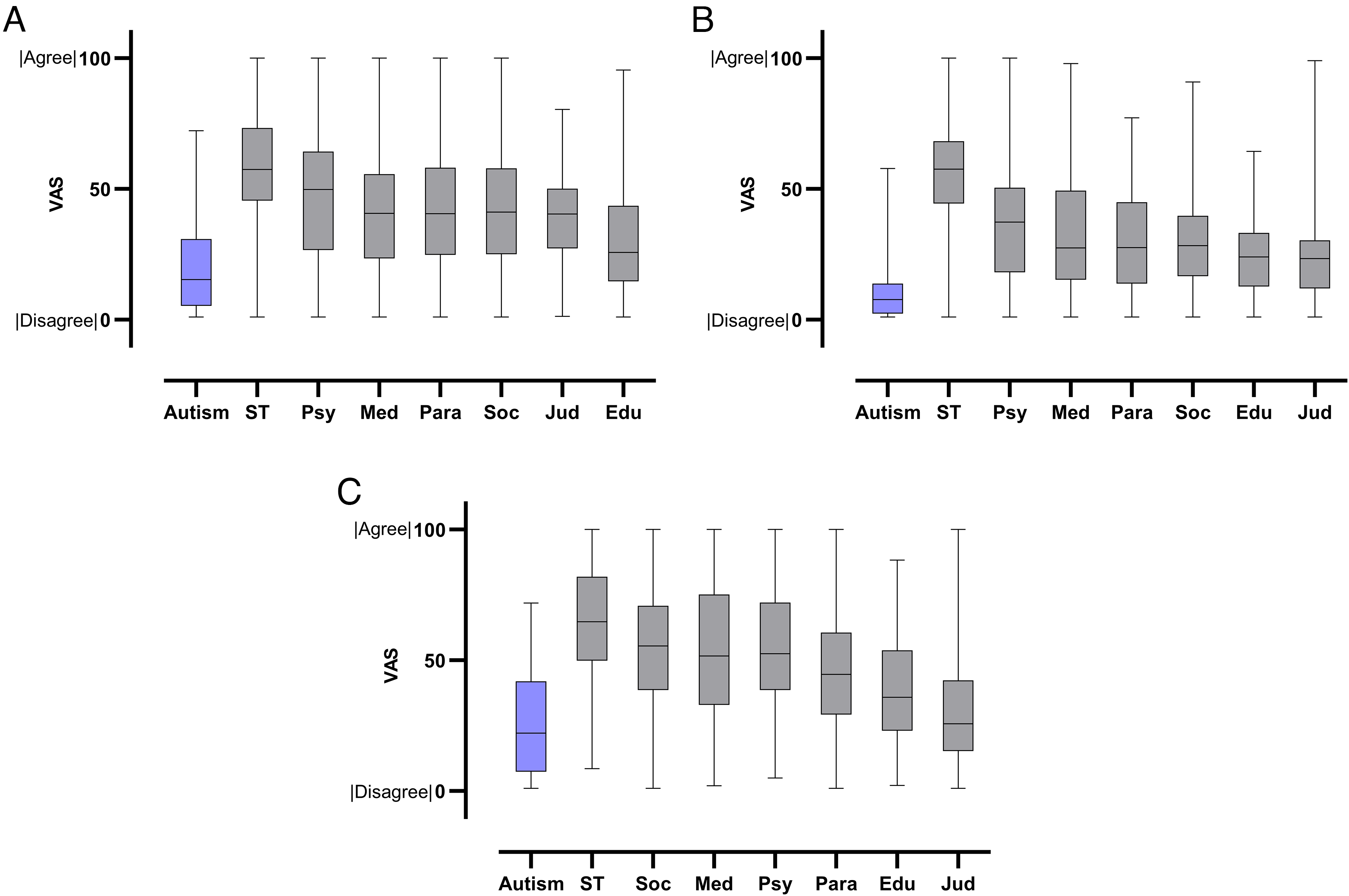
The EFA on the perception of the clinical case indicated excellent sampling adequacy (KMO = 0.86) and a significant Bartlett’s test (p < 0.05), confirming that the data were suitable for factor extraction. Internal consistency was good (Cronbach’s alpha = 0.81). The EFA supported a two-factor structure (with Item 1 removed because it did not load on any factor): adjusted mother–child relationship (Factor 1; items 2, 5, 6, and 8) and maternal psychological concerns (Factor 2; items 3, 4, and 7). Higher factor scores reflect more negative perceptions. Specifically, higher scores on Factor 1 indicate a less-adjusted mother–child relationship, whereas higher scores on Factor 2 indicate greater concerns about maternal psychological needs. Factor scores were then entered into the generalized linear model as described in the Method section. The model revealed significant main effects of respondent categories (χ2(7) = 533.23, p < 0.001, η2 = 0.02), factors (χ2(2) = 1452.05, p < 0.001, η2 = 0.35), and categories × factors interaction (χ2(14) = 140.29, p < 0.001, η2 = 0.032).
Factor 1: Adjusted mother–child relationship
Post hoc pairwise comparisons (Fig. 1A) revealed that autistic adults reported significantly lower agreement with statements indicating a non-adjusted mother–child relationship (M = 9.06, SE = 0.55) than all professional groups (education: M = 26.76, SE = 2.36; judicial: M = 33.70, SE = 2.69; medical: M = 28.23, SE = 1.64; paramedical: M = 23.60, SE = 1.12; psychologist: M = 21.15, SE = 1.25; social: M = 24.44, SE = 1.07; speech therapists: M = 28.77, SE = 1.62; all p < 0.014).
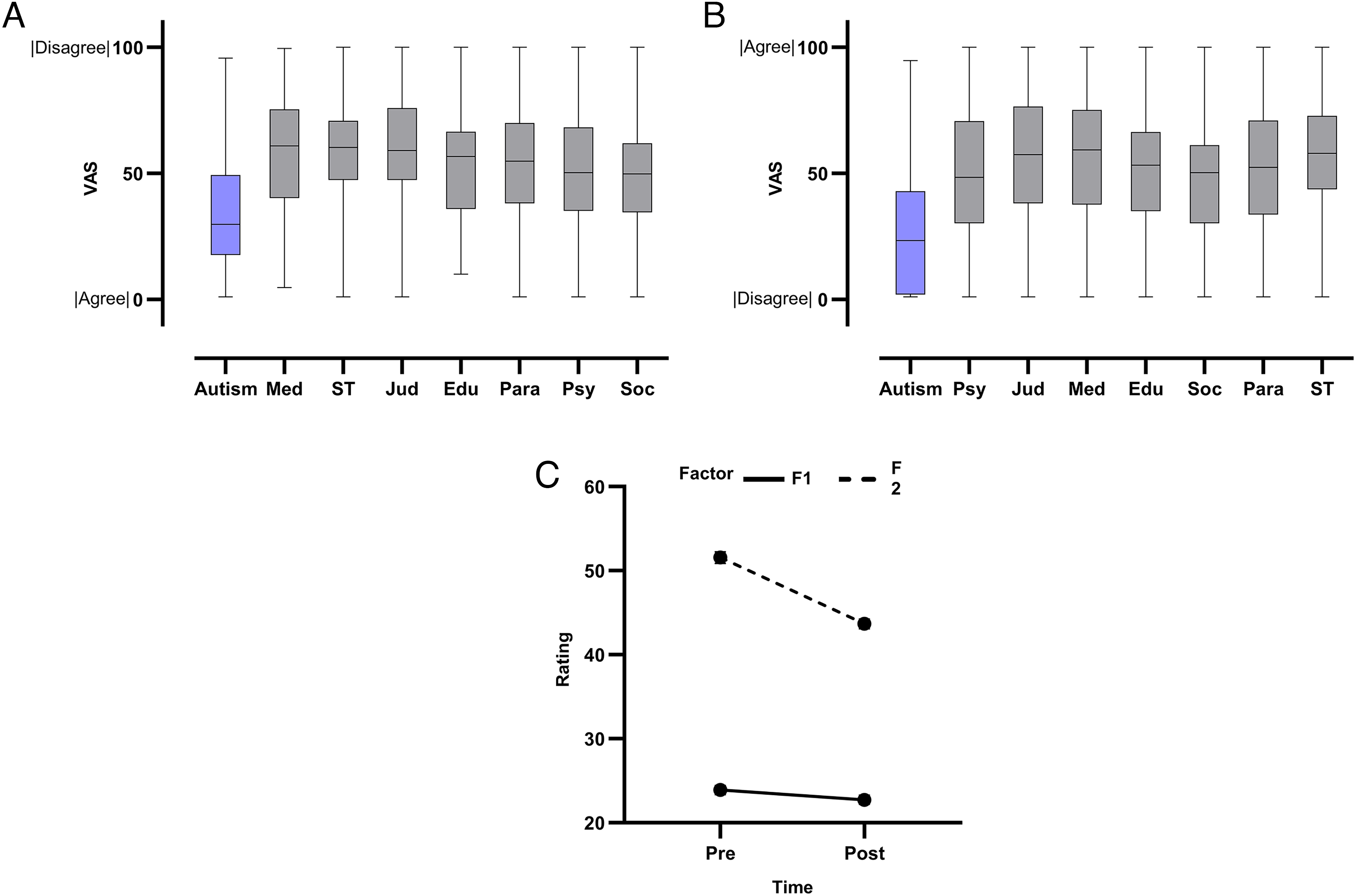
Participants’ perceptions of the clinical case before and after diagnosis disclosure (higher scores reflect more negative evaluations). Pre-diagnosis perception by category:
Factor 2: Maternal psychological concerns
Post hoc pairwise comparisons (Fig. 1B) revealed that autistic adults expressed significantly lower concerns about maternal behavior and her psychological needs (M = 34.05, SE = 1.92) than all professional groups (education: M = 53.51, SE = 4.41; judicial: M = 57.59, SE = 4.29; medical: M = 58.62, SE = 3.17; paramedical: M = 52.83, SE = 2.33; psychologist: M = 51.44, SE = 2.83; social: M = 49.23, SE = 2.01; speech therapist: M = 58.33, SE = 3.05; all p < 0.001). Autistic adults would be more likely to identify autistic behaviors in the vignette than professionals that are not trained to autism.
Logistic regression analysis revealed that the respondent category significantly correlated with diagnostic opinions. The Omnibus test showed that the model was statistically significant (χ2 = 55.8, df = 7, p < 0.001; Nagelkerke R2 = 0.15).
Details of the diagnoses suggested by participants are represented in Figure 2. Post hoc comparisons indicated that autistic adults were significantly more likely to consider autism as a potential diagnosis than judicial (OR = 0.013, p = 0.001), medical (OR = 0.026, p = 0.012), and paramedical professionals (OR = 0.028, p = 0.015). Judicial professionals were less likely to consider autism as a potential diagnosis than psychologists (OR = 0.20, p = 0.017) and speech therapists (OR = 0.24; p = 0.033). No other pairwise comparisons remained significant after correction.
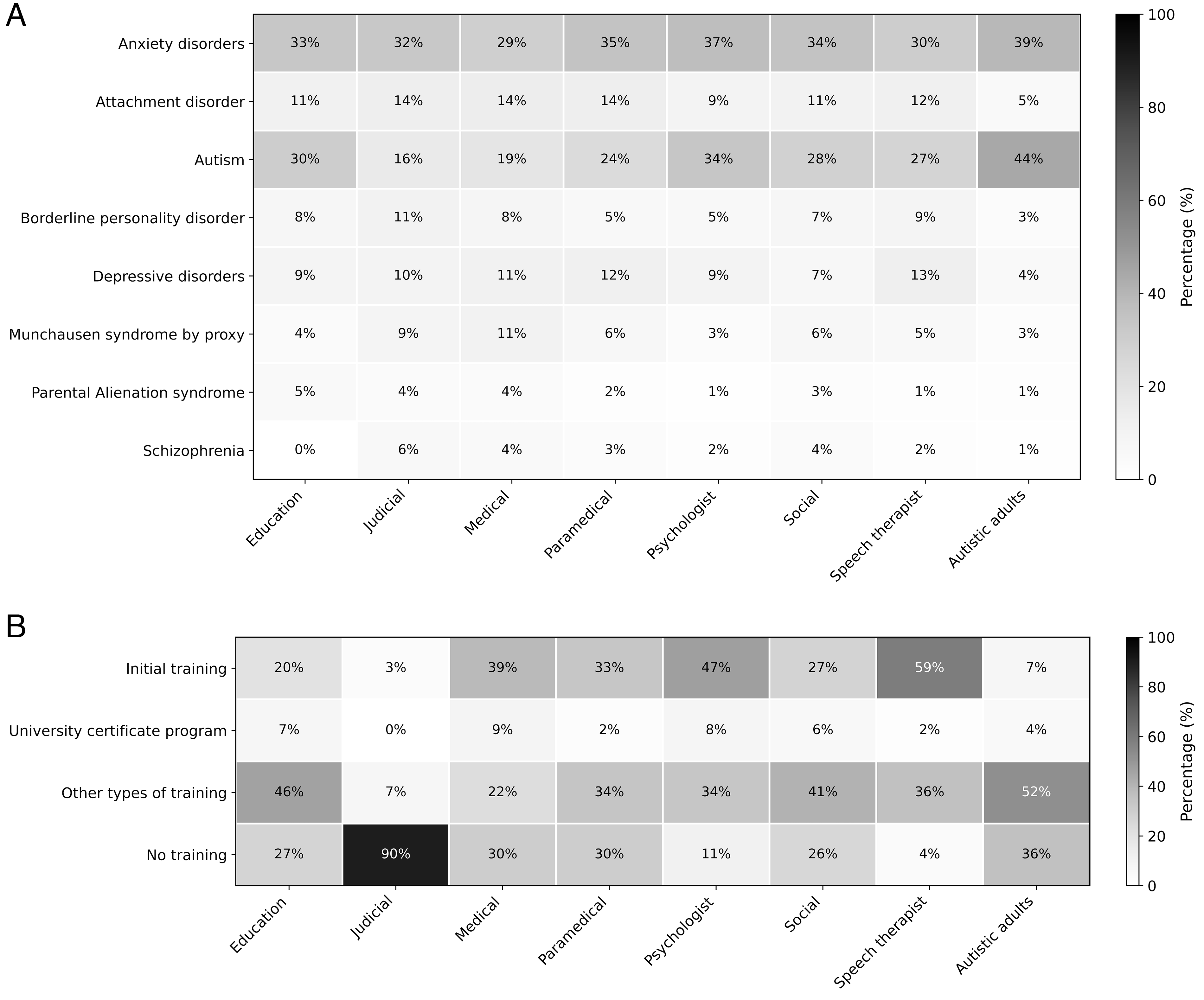
Diagnostic hypotheses and autism training profiles across professional groups.
Overall, autistic adults showed the highest likelihood of considering autism as a potential diagnosis, whereas judicial, medical, and paramedical professionals showed the lowest and were also the most likely to suggest a Munchausen syndrome by proxy diagnosis (Fig. 2A). These groups also had the lowest rates of autism-specific training (Fig. 2B), suggesting a descriptive correspondence between training exposure and autism-recognition accuracy. In contrast, psychologists and speech therapists, who were the most frequently trained, displayed higher autism-recognition sensitivity. Revealing an autism diagnosis to professionals would increase their negative perceptions, while it would not change those of autistic adults.
A generalized linear model including time (pre- vs. post-disclosure), category, and factor revealed significant main effects of time (χ2(1) = 60.59, p < 0.001, η2 = 0.01), factor (χ2(2) = 1896.16, p < 0.001, η2 = 0.3), and category (χ2(7) = 473.86, p < 0.001, η2 = 0.1), with autistic people scoring lower than all professional categories (all p < 0.001). The time × factor interaction was also significant (χ2(2) = 32.77, p < 0.001, η2 = 0.003), indicating that changes from pre- to post-disclosure perceptions varied across the two factors (Fig. 1C). In contrast, the time × category interaction was not significant (χ2(7) = 6.13, p = 0.52), suggesting that the overall temporal pattern of pre- to post-disclosure perceptions was relatively consistent across professional groups and autistic individuals. The category × factor interaction did not reach significance (χ2(14) = 3.14, p = 0.051), and the time × category × factor interaction was not significant (χ2(14) = 3.13, p = 0.872). Thus, there was no strong evidence that category-specific effects varied as a function of factor or time. A series of post hoc comparisons was conducted to examine the time × factor interaction.
Factor 1: Adjusted mother–child relationship
For Factor 1 (with lower scores indicating a more adjusted mother–child relationship), post-disclosure scores (M = 22.74, SE = 0.55) were not significantly different than pre-disclosure scores (M = 23.89, SE = 0.54; t(4372) = –1.43, p = 0.15), suggesting that the data do not provide evidence for a change in perceptions of the mother–child relationship after the autism diagnosis disclosure.
Factor 2: Maternal psychological concerns
For Factor 2, post-disclosure scores (M = 43.67, SE = 0.56) were significantly lower than pre-scores (M = 51.56, SE = 0.68; t(4372) = –8.53, p < 0.001). This reflects that participants were less concerned about maternal behavior and her psychological needs after diagnosis disclosure.
In addition, a generalized linear model was conducted to examine responses to the three diagnostic disclosure effects (reassures, raises concerns, and elicits doubts) across professional categories. Omnibus tests revealed no significant main effect of category (χ2 = 5.6, df = 7, p = 0.579), indicating that ratings did not differ between professional groups. However, there was a significant effect of item (χ2 = 43.7, df = 2, p < 0.001, η2 = 0.35) and a significant category × item interaction (χ2 = 224.3, df = 14, p < 0.001, η2 = 0.04), suggesting that the difference between categories varied depending on the diagnostic disclosure effect items.
Item 1: Reassures
Post hoc analyses showed no group differences (all p > 0.05), indicating that participants were rather reassured by the diagnosis.
Item 2: Raises concerns
Autistic adults (M = 4.59, SE = 0.45) scored significantly lower than all professional categories (education: M = 23.93, SE = 1.76; judicial: M = 32.00, SE = 3.96; medical: M = 27.28, SE = 2.45; paramedical: M = 23.72, SE = 1.73; psychologist: M = 17.03, SE = 1.56; social: M = 24.32, SE = 2.63; speech therapist: M = 21.85, SE = 1.90; all p < 0.001), indicating that autistic adults reported fewer concerns than professionals following diagnostic disclosure.
Item 3: Elicits doubts
Autistic adults (M = 5.89, SE = 0.55) scored significantly lower than all professional categories (education: M = 25.47, SE = 3.49; judicial: M = 30.97, SE = 3.83; medical: M = 29.61, SE = 2.66; paramedical: M = 27.49, SE = 2.01; psychologist: M = 25.32, SE = 2.32; social: M = 26.25, SE = 1.78; speech therapists: M = 22.97, SE = 2.00; all p < 0.001), indicating that they expressed fewer doubts regarding the autism diagnosis than professionals. No other pairwise differences among professional groups reached statistical significance after correction. Perceived professional competency regarding autism and autistic parents would differ between professionals and autistic adults.
The EFA on the professional competency questionnaire indicated excellent sampling adequacy (KMO = 0.92) and a significant Bartlett’s test (p < 0.05), confirming that the data were suitable for factor extraction. Internal consistency was good (Cronbach’s alpha = 0.91). The EFA supported a three-factor structure: recognition and support of autistic parents (Factor 1; items 4, 5, and 6), professional skills in autism (Factor 2; items 1, 2, 3, and 9), and networking and specialized guidance (Factor 3; items 7, 8, and 10). Higher factor scores reflect more positive evaluations. The generalized linear model revealed significant effects of respondent category (χ2(7) = 904.0, p < 0.001, η2 = 0.42), factor (χ2(2) = 277.0, p < 0.001, η2 = 0.13), and category × factor interaction (χ2(14) = 103.0, p < 0.001, η2 = 0.05), although this effect was small.
Factor 1: Recognition and support of autistic parents
Post hoc analyses (Fig. 3A) indicated that autistic adults (M = 19.37, SE = 1.04) reported lower perceived recognition and support from health care professionals than the levels reported by professionals when evaluating their own professional groups (education: M = 28.79, SE = 2.23; judicial: M = 39.32, SE = 2.78; medical: M = 41.13, SE = 2.11; paramedical: M = 41.70, SE = 1.74; psychologist: M = 46.63, SE = 2.42; social: M = 42.49, SE = 1.64; speech therapist: M = 57.16, SE = 2.84; all p < 0.001).
Participants’ perceptions of professionals’ competency regarding autism and autistic parents, by participant category.
Factor 2: Professional skills in autism
Post hoc analyses (Fig. 3B) indicated that autistic adults (M = 9.96, SE = 0.53) reported perceiving lower skills in autism among health care professionals than all other groups than the levels reported by professionals when evaluating their own professional groups (education: M = 24.10, SE = 1.87; judicial: M = 23.73, SE = 1.67; medical: M = 34.17, SE = 1.75; paramedical: M = 29.94, SE = 1.24; psychologist: M = 36.38, SE = 1.89; social: M = 29.29, SE = 1.13; speech therapist: M = 55.73, SE = 2.76; all p < 0.001).
Factor 3: Networking and specialized guidance
Post hoc analyses (Fig. 3C) showed that autistic adults (M = 25.59, SE = 1.37) reported lower perceived professional coordination and guidance from health care professionals than the levels reported by professionals when evaluating their own professional groups (education: M = 38.78, SE = 3.12; medical: M = 53.44, SE = 2.73; paramedical: M = 45.97, SE = 1.94; psychologists: M = 54.32, SE = 2.84; social workers: M = 55.46, SE = 2.15; speech therapists: M = 64.65, SE = 3.19; all p < 0.001), except the judicial group (M = 29.96, SE = 2.11, p > 0.05).
Discussion
This participatory study examined how autistic adults and non-autistic professionals perceive autistic parenting and professionals’ competency regarding autism in France. Overall, professionals viewed autistic parenting more negatively than autistic adults, who were also generally more accurate at identifying autistic behaviors than several professional categories, particularly when professionals had limited autism-specific training. The disclosure of an autism diagnosis appeared to reduce professionals’ concerns, suggesting that diagnostic information may have a positive effect on professional perceptions. Nevertheless, autistic adults rated professionals as less competent than professionals rated themselves, highlighting a gap between perceived and self-reported competence.
Our first hypothesis was that professionals would hold more negative perceptions of a fictional mother with high autistic traits than autistic adults, in the absence of diagnostic information. This hypothesis was confirmed. Compared with all professional groups, autistic adults perceived less disruption in the mother–child relationship depicted in the vignette and expressed fewer concerns about the mother’s psychological needs. Mean scores among professionals were generally below 50, indicating that their perceptions were not overtly negative and were rather consistent with those of autistic adults. In contrast, mean scores among professionals for the mother’s psychological needs factor were slightly above 50, whereas those of autistic adults were below 50. This indicates that the fictional mother’s behavior was perceived as somewhat atypical and elicited a certain degree of concern among professionals. This partly supports autistic parents’ fear of being judged on atypical behaviors.5,13,14 These findings may reflect the “cognitive marginalization” 31 and cultural differences between autistic people and non-autistic professionals, who do not necessarily share the same behavioral norms or reference points. 44 This aligns with the double- or triple-empathy problem45–47: Autistic adults may perceive the mother’s behaviors as typical within their own normative framework, whereas non-autistic professionals may interpret them as more unexpected, leading to reduced understanding and increased judgment. Importantly, there was high variability in professionals’ responses within each category, potentially reflecting important individual differences in familiarity with autism and in the amount of autism-specific training received.
Our second hypothesis, that autistic adults would be more likely to identify autistic behaviors than professionals without autism-specific training, was partly supported. Autistic adults showed higher odds of suggesting an autism diagnosis than judicial professionals, who had the highest proportion of untrained respondents (∼90%). Autistic adults were also more likely to suggest an autism diagnosis than paramedical and medical professionals. In these professions, about 30% of respondents lacked autism-related training, a proportion comparable to social and education professionals. This gap in training among groups that routinely interact with autistic people and parents is concerning, but consistent with previous research in other countries.48–50 It is particularly worrying for medical doctors, who are the only group authorized to diagnose autism in France. Interestingly, this group was also the most likely to suggest conditions such as Munchausen syndrome by proxy or parental alienation syndrome (15%). However, across all professional groups, such interpretations remained rare, and fewer than 10% of respondents in most groups endorsed these hypotheses. Although analyses of the influence of the type of training were not conducted, it is possible that autism training for medical and paramedical professions more often occurs during initial training in educational and social fields. This may indicate that initial training remains insufficient and based on basic awareness, notably during medical and paramedical school. 51 Indeed, in past research, physicians usually rate their training related to autism as poor or fair.52,53
Our third hypothesis was that revealing an autism diagnosis would increase professionals’ negative views, while leaving autistic adults’ perceptions unchanged. Contrary to this hypothesis, changes between pre- and post-disclosure perceptions did not differ between autistic adults and professionals, although autistic adults consistently held more positive views of the depicted mother than professionals. Importantly, although participants’ perceptions partially shifted following diagnostic disclosure, the direction of this shift was opposite to that expected. Specifically, endorsement of items reflecting a disrupted mother–child relationship (e.g., parenting skills, relationship disruption, disputes over care, or the need for child protection involvement) did not differ significantly between pre- and post-diagnostic disclosure, and participants expressed fewer concerns regarding maternal psychological needs following disclosure. This pattern may reflect a reinterpretation of certain behaviors as typical autistic traits rather than indicators requiring specific intervention. Consistent with these findings, analyses of reassurance-related items indicated that professionals predominantly reported feeling reassured and perceiving no additional concerns following diagnostic disclosure, albeit to a lesser extent than autistic adults. These results align with a scoping review reporting generally positive outcomes of autism diagnosis disclosure when evaluated through vignettes from a non-autistic perspective. 21 Professionals’ reported reassurance may reflect normative expectations of non-discrimination, as well as the belief that diagnostic information facilitates access to appropriate support. Although the same review noted that autistic individuals themselves often report more negative outcomes following diagnostic disclosure, this perspective was not directly examined in the present study and warrants further investigation.
Overall, the present results do not support autistic parents’ concerns that diagnostic disclosure would lead professionals to adopt more negative views or increase their propensity to involve child protective services. On the contrary, they should encourage diagnostic disclosure. However, these findings should be interpreted with caution. First, they may reflect the relatively high proportion of professionals with autism-related training in the sample. Second, responses collected in a survey context are likely to capture explicit, value-driven attitudes and may be influenced by demand characteristics or social desirability, particularly among professionals aware of normative expectations in their field. These explicit attitudes may differ from implicit, stereotype-based attitudes that are more likely to influence behaviors in real-life professional settings.54,55 Indeed, studies examining this discrepancy have found that negative implicit attitudes toward autistic individuals coexist with positive explicit attitudes, underscoring the importance of considering both types of evaluation when interpreting professional judgments. 54
When evaluating doubts elicited by diagnostic disclosure, autistic adults expressed fewer doubts than all professional groups, although mean scores indicated that professionals generally reported low levels of doubt. This contrasts with prior work on disclosure experiences among autistic adults in which many reported not being believed. 56 Differences may stem from the previous study not focusing specifically on disclosure to professionals but instead adopting a broader perspective. Nevertheless, it can also again highlight a potential gap between explicit, value-driven attitudes (e.g., a professional would not explicitly disbelieve a diagnosis made by an expert) and more automatic, stereotype-based evaluations55,57 that may influence real-world behaviors (e.g., struggling to accept a diagnosis when it does not match pre-existing autism stereotypes).
Finally, we hypothesized that perceived professional competency regarding autism and autistic parents would differ between professionals and autistic adults. This hypothesis was supported: Autistic adults perceived lower recognition and support of autistic parents, lower professional skills in autism, and less networking and specialized guidance among health care professionals than the levels reported by professionals themselves when evaluating their own professional groups. However, these results should be interpreted with caution. Autistic participants provided a global evaluation of health care professionals, whereas professionals rated their own specific professional group. As such, these comparisons do not reflect direct group-to-group evaluations and may be influenced by variability in autistic individuals’ experiences across different types of professionals. In addition, comparisons involving non-health-care professions (e.g., education, judicial, social) cannot be directly interpreted, as these groups were not specifically evaluated by autistic participants. More granular assessments would be needed to examine how different professional groups are perceived individually.
Nevertheless, for both the factors related to recognition and support and to professional skills, mean scores for all categories except speech therapists were below 50, indicating low to moderate knowledge and self-efficacy among professionals, consistent with previous literature.35,51,52 Speech therapists were the most confident in their expertise, although their confidence remained moderate. This may reflect their higher likelihood of autism-specific training and frequent early contact with autistic individuals. Indeed, health professionals who are used to providing care to autistic people usually feel more knowledgeable and competent, although still wanting further training. 58
Overall, the results indicate that autistic parents can be judged on their behaviors by professionals, who may sometimes struggle to identify autistic characteristics, potentially due to a lack of training. Diagnostic disclosure may improve professionals’ perceptions, although this effect would need to be confirmed using implicit measures and a more representative sample of professionals. These findings highlight the need for professionals to move away from normative views and reduce stereotypes about autistic behaviors in autistic parents. Behavioral diversity, including distinctive parenting styles, should be recognized and acknowledged. Professionals across health care, social work, and the judicial system need to better distinguish atypical from problematic behaviors and provide more neuroaffirming environments in which autistic parents can be supported and recognized.18,59
Education and direct contact with autistic parents could be proactive strategies to promote positive attitudes among professionals. 60 There is a need to develop training that improves identification of autistic characteristics for all professionals who may assess or support autistic parents. This includes judicial professionals, whose decisions can have a major impact on parents’ lives, yet who are almost never trained in autism. The reduced training of the judicial professionals, including both professionals from the judicial system and police officers, aligns with a previous study specifically focused on police officers. 61 In addition, since initial professional training, for instance in medical school, may be too broad, specialized autism training programs should be implemented for all relevant professionals. Such programs have been associated with improved knowledge and increased self-efficacy in supporting autistic patients among physicians, 62 social workers,63,64 and teachers, although these studies did not specifically address training for working with autistic parents.
Limited real-world exposure to autistic parents may reinforce reliance on societal stereotypes rather than lived experience. 60 Thus, including autistic parents in training could be particularly beneficial. While autism acceptance training using first-person narratives has shown promises in reducing misconceptions among university students, its effect on implicit bias is still limited. 65 Social workers have reported that training delivered by autistic people themselves could be especially helpful, 64 which should thus be prioritized. Developing specialized training for all professionals on autistic parent acceptance, with autistic parents, could, therefore, be particularly valuable. Future research should focus on designing and evaluating such programs to reduce implicit bias toward autistic parents in professional settings.
Limitations and future directions
This study had several limitations. First, as with other online studies, there is a potential bias in participant selection. Despite our efforts to reach a broad professional network, the professionals who participated in the study may be predominantly those who had received training on autism. This may not be representative of the population of French professionals and could explain some of the findings, such as rather positive views on autism or on the diagnosis disclosure. Although grouping professionals into categories was necessary to conduct the analyses, this approach may have obscured meaningful differences between professions (e.g., between police officers, jurists, and lawyers). Some professions were only represented by small sample sizes (e.g., dietitians), limiting the interpretation at a more granular level. Future studies could examine these subgroups separately.
Sex/gender distribution also represents a limitation, as both autistic participants and professionals were predominantly female at birth (autistic participants: 84%; professionals: from 70% in the judicial category to 97% in speech therapists). This represents a source of potential bias, as males and females may be socialized differently and have different social expectations, interpretations, and responses. Nevertheless, these proportions are broadly consistent with the sex/gender distribution typically observed in these professions, suggesting that the sample remains relatively representative in this respect. However, the overrepresentation of females among autistic participants may limit the generalizability of the findings to the broader autistic population.
In addition, only limited socio-demographic variables were collected for ethical considerations. Future research should examine the potential influence of factors such as age, gender, and ethnicity on participants’ responses.
Another limitation is that the questionnaire and clinical case used were not pre-existing validated tools. Instead, they were co-developed by the research team, including autistic parents, to directly address their needs and concerns, as the development of hypotheses was informed by lived experiences of autistic parents. While this participatory approach ensured that the research tools and questions were relevant and meaningful, the lack of formal validation may limit the generalizability of the findings.
In addition, the clinical vignette is necessarily simplified and does not allow for a formal autism diagnosis, as is typical for vignettes. Therefore, participants’ responses reflect perceptions based on a brief scenario rather than a full clinical evaluation. Furthermore, the scenario is set in a health care context, which may be more directly relevant to professionals working in this setting and influence how different professional groups interpret the situation.
Finally, the study relied on a single vignette, which limits the interpretation of the results. In particular, it does not allow us to determine whether the observed group differences are specific to autistic-like behaviors as illustrated in the vignette or reflect other factors. For example, because the clinical case was presented in a medical context, professionals’ responses may reflect greater concern about the psychological adjustment of any parent whose child faces medical issues requiring hospitalization. Observed group differences might also reflect response biases that could be influenced by the female sex of the autistic parent depicted. Specifically, anxiety disorders are more common than autism in the general population,66,67 and females, including autistic females, tend to present higher rates of anxiety and other mental health conditions than males. 68 Moreover, the vignette may have provided clearer evidence of anxiety than autism. Therefore, professionals might have been less likely to indicate autism because anxiety represented a more parsimonious and statistically likely explanation of the behaviors described and because they avoided making assumptions under conditions of uncertainty, rather than because they failed to recognize autistic characteristics. Conversely, autistic participants may also have been more likely to interpret some behaviors as autistic characteristics rather than as reflecting another condition, possibly because of greater familiarity with lived experiences. Given these limitations, the findings should therefore be considered exploratory. Future research could focus on refining and validating the vignette(s) to improve their reliability. Importantly, they should also include a broader range of scenarios (e.g., more neuro-normative behaviors or other specified conditions such as having an anxiety disorder but without autism), vary key characteristics such as the sex and gender of the parent depicted, and examine different contexts to better disentangle the factors driving participants’ perceptions and assess potential response biases.
Finally, as this study was based on questionnaires, it reflects explicit attitudes, which may be more positive than implicit attitudes toward autistic individuals. 54 Future research could consider including implicit measures that might better capture attitudes or behaviors in real-life settings.
Conclusion
The present study provides important quantitative evidence supporting concerns raised by autistic parents in qualitative research, particularly regarding difficulties in being understood by professionals. The findings reveal persisting stigma, gaps in knowledge, and a clear need for targeted training on autistic parenthood across diverse professional groups, including those less directly involved with autism, such as judicial professionals. Effective training should incorporate first-person narratives from autistic parents and aim to foster environments and relationships that acknowledge difference, promote understanding, and provide safe spaces where autistic parents can be appropriately recognized and supported. These results underscore the urgent need for systemic initiatives to enhance professional awareness, improve knowledge and attitude, reduce biases, and strengthen support for autistic parents across health care and social systems.
Authors’ Contributions
A.L.: Conceptualization, methodology, investigation, writing—original draft, supervision, and project administration. W.V.: Data curation, formal analysis, and writing—original draft. M.-C.L.: Methodology and writing—original draft. D.L.: Conceptualization, methodology, investigation, and writing—original draft. M.P.: Conceptualization, methodology, investigation, and writing—original draft. J.B.: Methodology and writing—original draft. M.D.: Conceptualization, methodology, investigation, supervision, and writing—original draft. C.D.: Conceptualization, methodology, investigation, supervision, writing—original draft, and funding acquisition.
Footnotes
Acknowledgment
The authors are grateful to IMind for hosting the study and supporting the project infrastructure.
During the preparation of this work the first author used ChatGPT to perform grammatical checks and to improve readability. After using this tool/service, all authors reviewed and edited the content extensively. We take full responsibility for the content of the published article.
Data Availability
Data is available on request from A.L.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this study.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.