
Abstract
Barrett’s esophagus (BE) is the main precursor to esophageal adenocarcinoma (EAC). Guidelines recommend endoscopic surveillance of BE to detect neoplastic progression early to improve health outcomes. It is challenging for physicians to identify BE patients that will progress to high-grade dysplasia (HGD)/EAC, and studies have shown that prevalent disease can be missed by endoscopy/pathology. The tissue systems pathology test (TSP-9) has been validated to risk stratify patients with BE by predicting their risk of progression to HGD/EAC. This report describes the clinical journey of a patient with a diagnosis of non-dysplastic (ND)BE and a high-risk TSP-9 test result, prompting risk-aligned clinical management.
Keywords
Introduction
Barrett’s esophagus (BE) is characterized by replacement of the normal squamous esophageal lining with intestinal metaplasia (IM) and is the main precursor to esophageal adenocarcinoma (EAC), which has a five-year survival rate of only 22%. 1 Clinical management practices that rely on clinicopathologic factors have limited ability to risk stratify patients with BE, and a subset of patients diagnosed with non-dysplastic (ND)BE harbor missed prevalent high-grade dysplasia (HGD)/EAC or progress to HGD/EAC during their guideline-recommended surveillance intervals. 2 Accurate risk stratification is needed to detect patients with NDBE who are at high risk for HGD/EAC to enable risk-aligned management including short-interval surveillance to detect EAC at early treatable stages or early use of endoscopic eradication therapy (EET) to prevent EAC. The tissue systems pathology test (TissueCypher, TSP-9) is a clinically available test, extensively validated in multicenter studies to provide objective risk stratification in patients with BE that outperforms traditional clinicopathologic factors,3 -9 and clinical utility studies have shown that TSP-9 can guide risk-aligned management decisions for patients with BE.10,11 The test provides a risk score (0-10), risk class (low, intermediate or high), and an individualized probability of progression to HGD/EAC within 5 years. This case report describes the utility of the TSP-9 test in guiding risk-aligned management for a patient in surveillance for NDBE at a foregut surgery center.
Case Description
A 67-year-old male with a history of chronic gastroesophageal reflux disease (GERD) presented to the foregut surgery center due to uncontrolled acid reflux symptoms despite use of a proton pump inhibitor and was seeking a second opinion after undergoing esophagogastroduodenoscopy (EGD) at a gastroenterology practice. The patient had no family history of GERD, was a non-smoker, not obese, and had been getting iron transfusions for chronic anemia of unknown origin. A recent upper endoscopy at the gastroenterology practice reported no signs of inflammation and a medium-sized hiatal hernia. The duodenum appeared normal and mild erythema was observed in the gastric mucosa. Histological assessment of a biopsy from the duodenum confirmed normal duodenal mucosa with no diagnostic abnormalities or features suggestive of celiac sprue. The stomach biopsy showed mild chronic gastritis with no intestinal metaplasia (IM), and H. pylori organisms were not detected by immunohistochemistry. No esophageal biopsy was performed during this EGD.
An anti-reflux/fundoplication surgery was initiated to treat acid reflux, at which time the intra-operative EGD revealed a large hiatal hernia and Prague criteria were C0M1 (Figure 1a) and a successful fundoplication was performed. A biopsy at 42 cm showed no IM, while a biopsy at 41 cm showed IM without dysplasia upon internal pathology review, which was consistent with a diagnosis of NDBE. The patient received a high-risk score of 7.1 with a 17% (95% confidence interval 15.1-19.3) probability of progression to HGD/EAC within 5 years (Figure 1b). This level of risk is approximately 2-times greater than the risk associated with confirmed low-grade dysplasia (LGD) for which EET is recommended, 12 which led to a change in management for this patient. The patient was referred back to the referring gastroenterologist for consideration of EET. Instead of EET, the gastroenterologist recommended short-interval surveillance. Due to the high-risk TSP-9 test result, the foregut surgeon requested the patient return 6 months postoperatively for EGD. The EGD revealed intact fundoplication, and again C0M1 columnar lined epithelium was noted without visible lesions. Biopsies at 42 and 41 cm received pathology diagnoses of NDBE and now a new finding of HGD, respectively (Figure 1c). The patient was subsequently referred to a university-specialized Barrett’s program for further management of HGD, including EET to prevent development of EAC in alignment with current society-recommended guidelines for the management of HGD.
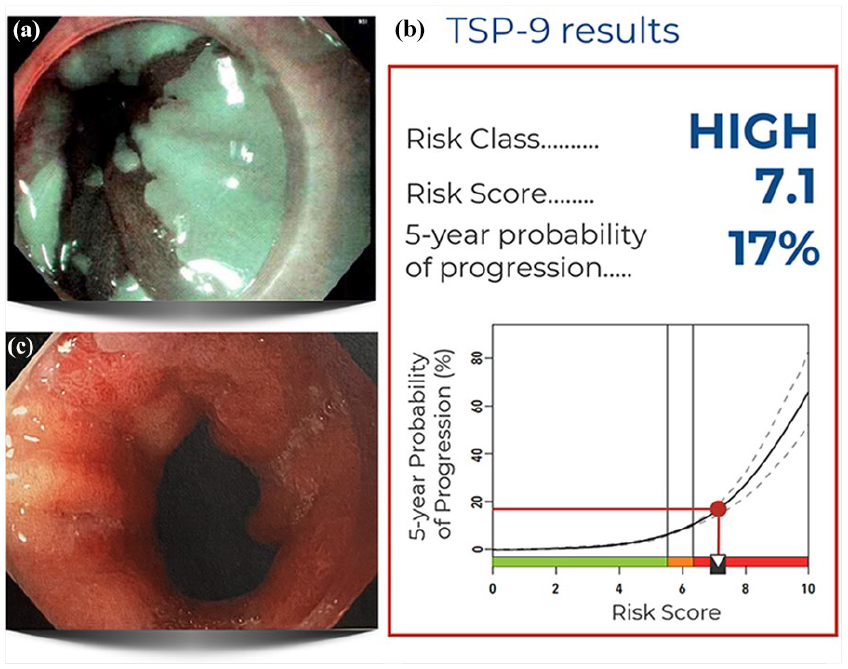
Endoscopic findings and TSP-9 test results: (a) Baseline intra-operative EGD that showed a large hernia and C0M1; biopsies at 42 cm without intestinal metaplasia and biopsies at 41 cm that showed non-dysplastic intestinal metaplasia for which TSP-9 was ordered, (b) TSP-9 results showing that the patient received a result of 7.1, high-risk with a 5-year probability of progression to HGD/EAC of 17% (95% confidence interval 15.1-19.3), and (c) EGD 6 months post-TSP-9 testing showing Prague criteria C0M1 and biopsies at 42 cm that were diagnosed as NDBE and biopsies at 41 cm near the squamocolumnar junction that showed HGD.
Discussion
This communication describes the clinical utility of the TSP-9 test in predicting that a patient with a pathology diagnosis of NDBE was at high-risk for neoplasia, enabling escalation of clinical management. The TSP-9 test was ordered to stratify this patient with NDBE for risk of developing HGD/EAC, consistent with best practice advice in the 2022 American Gastroenterological Association (AGA) BE Clinical Practice Update. 13 The TSP-9 test predicted that this patient was high risk for progression, which led to escalation to short-interval surveillance in 6 months instead of the 3-5 year surveillance interval typically recommended for NDBE. This follow-up EGD performed at the surgical center was deemed a necessary step in patient management, as it is not customary for a direct referral of a patient with NDBE for EET. Pathology review of a biopsy taken at the follow-up endoscopy showed prevalent HGD that was likely missed at the earlier endoscopy. As such, this patient would benefit from intervention with EET, a highly effective strategy to prevent development of EAC. A strength in this case was availability of clinical/pathological data and management plans before and after receiving TSP-9 results, which enabled evaluation of how the TSP-9 test results altered care of the patient. This case highlights the ability of TSP-9 to predict prevalent HGD even if it is not directly sampled by pinch biopsies during endoscopy.
Whereas endoscopic inspection and histologic assessment of esophageal biopsies did not identify that this patient harbored prevalent neoplasia, the TSP-9 test predicted that this patient was high-risk. This enabled risk-aligned management leading to intervention with the goal of preventing EAC. Without the high-risk TSP-9 test result, this NDBE patient would have undergone surveillance at an interval of 3-5 years. During this period, it is very possible that adenocarcinoma would have presented, given that the patient harbored prevalent HGD at the time of biopsy and TSP-9 test.
While NDBE biopsies lack morphologic changes consistent with dysplasia that can be observed on hematoxylin and eosin-stained slides, NDBE mucosa harbor molecular and cellular changes associated with an increased risk of prevalent neoplasia or future progression. Multiple clinical validation studies have shown that the TSP-9 test can detect these high-risk molecular and cellular changes in patients with NDBE and thereby predict whether patients are harboring prevalent neoplasia.4,8 Studies have also shown that the TSP-9 test can predict incident progression to HGD/EAC within 5 years.3,5 -8 These studies have demonstrated that NDBE patients who receive TSP-9 high-risk results progress to HGD/EAC at a rate similar to or even higher than the rate observed in patients with expert-confirmed LGD.5,6,8 As current gastroenterology society guidelines recommend EET or short-interval surveillance for patients with confirmed LGD,12,14 high-risk patients with NDBE identified by the TSP-9 test may benefit from management similar to patients with LGD based on their progression risk.
The TSP-9 result prompted a shortened surveillance window that enabled the detection of HGD, highlighting its utility in identifying patients that benefit from the escalation of care. EET is more effective in preventing EAC when used at earlier stages, 15 and EET could have been initiated shortly after the TSP-9 high-risk result was received for the NDBE biopsy to maximize the effectiveness of EET. Although EET is not recommended routinely for patients with NDBE, the latest AGA guidelines note that there are high-risk subsets of patients with NDBE who would benefit from EET as a preventative measure, and that these high-risk patients may be identified by TSP-9. 14 Additionally, patients with NDBE typically require fewer sessions than patients with dysplasia to achieve complete eradication of IM, indicating that early use of EET in high-risk patients can improve healthcare resource utilization and patient quality of life. 15
These findings align with previous studies demonstrating the clinical utility of the TSP-9 test in guiding risk-aligned management decisions, including escalation of care for patients who receive high-risk results and de-escalation to reduce over-treatment in low-risk patients. The TSP-9 test has gained significant clinical adoption, and a recent real-world evidence study of 8,080 patients from 505 clinical sites showed that the TSP-9 test identified high-/intermediate-risk BE patients in all evaluated clinicopathologic subsets, including patients with lower-risk clinical factors such as patients with NDBE, short-segment BE and female patients, and also patients with higher-risk clinical factors such as LGD or indefinite for dysplasia, long-segment BE and male sex. 11 The overall rate of progression in the NDBE population is low at approximately 0.63%/year. 2 However, these patients represent the majority of patients undergoing endoscopic surveillance for BE each year in the United States, 6 indicating that the NDBE population harbors the majority of patients who have prevalent HGD/EAC or will progress to HGD/EAC in the future. Early identification of these high-risk patients with NDBE by TSP-9 and escalated management, including EET, could significantly decrease the incidence and mortality of EAC. Conversely, the TSP-9 test identifies approximately 83% of BE patients as low-risk for progression, 11 which can help to reduce the overuse of endoscopy.
In conclusion, the TSP-9 test provided clinically actionable risk results in a BE patient with missed HGD, which resulted in escalation of care to prevent progression to EAC. The TSP-9 test predicted this patient was high-risk when endoscopic inspection and histopathology were unable to identify that this patient was harboring prevalent HGD. This case report highlights the clinical utility of TSP-9 and the need for early and accurate risk stratification for patients with NDBE to enable physicians and patients to make shared management decisions that are aligned with risk of progression to HGD/EAC.
Footnotes
Abbreviations
AGA, American Gastroenterological Association; BE, Barrett’s esophagus; EAC, esophageal adenocarcinoma; EET, endoscopic eradication therapy; EGD, esophagogastroduodenoscopy; GERD, gastroesophageal reflux disease; HGD, high-grade dysplasia; IM, intestinal metaplasia; LGD, low-grade dysplasia; NDBE, non-dysplastic Barrett’s esophagus; TSP-9, tissue systems pathology test.
Author Contributions
P.W.: Conceptualization, investigation, resources, visualization, writing – original draft. R.B.: Conceptualization, investigation, resources, visualization, writing – review and editing.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: P.W. is a consultant for Medtronic, TeleBio, ConMed, Lucid Biosciences, Intuitive, BD Interventional, Castle Biosciences, Inc., Stryker, Johnson and Johnson, and Woodworth Surgical, LLC. He is a committee representative of the American Foregut Society. R. B. is a consultant for Castle Biosciences, Inc., Lucid Diagnostics, TelaBio, Medtronic, Johnson & Johnson, and BD Interventional.
Ethical Approval
Ethical approval is not required for this manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent to participate
Informed consent to participate was obtained verbally.
Consent for publication
Informed consent for publication was obtained verbally.
Use of Artificial Intelligence
No artificial intelligence (AI) was used in the preparation of this manuscript.