
Abstract
Despite clinical guidelines for the management of traumatic brain injury (TBI), evidence-based rehabilitation programmes and large-scale studies evaluating rehabilitation provision and outcomes remain limited. This study aimed to (1) describe rehabilitation services delivered to patients admitted to the intensive care unit (ICU) after TBI, (2) examine associations between rehabilitation support and functional outcome, emotional distress, and TBI-specific health-related quality of life (HRQoL) at 12 months post-injury, and (3) assess the stability of outcomes at 3, 6, and 12 months post-injury. Data were obtained from the CENTER-TBI study. Participants were adults (≥18 years) admitted to the ICU who reported rehabilitation use and completed follow-up assessments. Functional outcome was assessed using the Glasgow Outcome Scale–Extended (GOSE), emotional distress using the Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder scale (GAD-7), and HRQoL using the Quality of Life after Brain Injury–Overall Scale (QOLIBRI-OS). The study included 661 patients (72.3% male; mean age 46.7 years). At 12-month post-injury, 87% achieved favorable recovery (GOSE 5–8), with mild depressive symptoms, minimal anxiety, and a mean QOLIBRI-OS score of 65.7. Rehabilitation provision increased from 30.6% at 3 months to 51.3% at 12 months. Early rehabilitation was most common among patients with mild TBI, while rehabilitation provision for those with moderate and severe TBI increased over time. Nevertheless, approximately half of patients with moderate-to-severe TBI did not receive rehabilitation within the first-year post-injury. Delayed initiation of rehabilitation, older age, lower education, unemployment, greater injury severity, and road traffic-related injuries were associated with poorer functional outcomes and lower HRQoL. Pre-injury psychiatric disorders predicted higher emotional distress. Functional recovery and HRQoL improved over time, whereas emotional distress remained relatively stable. Despite increasing rehabilitation provision, substantial gaps in access persist, particularly for patients with moderate and severe TBI. Early and well-coordinated rehabilitation remains essential to optimize recovery and long-term quality of life after TBI.
Keywords
Introduction
Traumatic brain injury (TBI) is a leading cause of long-term disability worldwide, frequently resulting in persistent physical, cognitive, and emotional impairments that contribute to behavioral and psychosocial difficulties, vocational limitations, and reduced quality of life.1,2 Addressing these multifaceted consequences necessitates comprehensive rehabilitation that integrates medical, allied health, and social care services. 3 Effective rehabilitation systems are characterized by accessible, well-coordinated, multidisciplinary care to meet the complex needs of individuals after TBI. 4 Although evidence supports the benefits of early, integrated rehabilitation for all TBI severities,5–7 many patients with severe TBI do not receive multidisciplinary rehabilitation services after the early in-hospital medical care.8,9 Following discharge from inpatient rehabilitation and throughout the post-acute phase, physical therapy remains the most frequently utilized service, despite reports of unmet needs in cognitive and psychological rehabilitation.10,11
Understanding the factors that influence recovery during the first year after TBI is crucial for timely and appropriate delivery of rehabilitation services. This period is key for neurological and functional recovery, as neuroplastic processes are most active and responsive to targeted interventions.12,13 Recovery trajectories vary substantially across individuals, reflecting the interplay of biological, psychological, and environmental factors. Key determinants, including age, injury severity, and pre-injury health status, interact with psychosocial and contextual variables such as social support, access to specialized rehabilitation, and socioeconomic conditions.14,15 Furthermore, cognitive, emotional, and behavioral sequelae can significantly influence an individual’s ability to engage in and benefit from rehabilitation. 16 A comprehensive understanding of these factors is essential for developing targeted, evidence-based rehabilitation strategies that optimize outcomes and promote successful community reintegration. 3
Although several clinical guidelines address the acute management of TBI,17,18 evidence-based recommendations for rehabilitation remain limited. 19 Consequently, large-scale studies are needed to evaluate the availability, accessibility, and impact of specific rehabilitation services across the continuum of care. 20 Given that service utilization and needs vary according to injury severity, this study focuses on patients admitted to Intensive Care Units (ICUs), a cohort characterized by relatively homogeneous acute care demands and potentially comparable rehabilitation requirements. Findings from such investigations are essential for informing and advancing the development of integrated, patient-centered models of care that can more effectively support recovery following severe and complex TBI. 21
The aims of this study were, first, to describe the delivery of rehabilitation services provided to a cohort of patients admitted to the ICU with TBI; second, to examine the relationship between rehabilitation support and outcomes, including functional status, emotional distress, and TBI-specific health-related quality of life (HRQoL) 12 months post-injury, while controlling for sociodemographic characteristics, premorbid conditions, and injury-related factors; and third, to assess the stability of functional outcomes, emotional distress and HRQoL over time, based on repeated assessments at 3-, 6-, and 12-months post-injury.
Methods
Participants and procedure
This was a multicenter, prospective, observational cohort study using data from the ICU stratum of the CENTER-TBI project (ClinicalTrials.gov ID NCT02210221) that recruited participants after TBI between December 2014 and December 2017. The core sample consists of 4,509 patients, with inclusion criteria of a clinical diagnosis of TBI of any severity, a clinical indication for computed tomography (CT) scan, presentation of TBI within 24 hours of injury, and no severe pre-existing neurological disorders. All patients were attended in the emergency room (ER) and, depending on their needs, were admitted to hospital ward (ADM), ICU, or discharged. Follow-up assessments were conducted up to 24 months post-injury. This study included ICU-admitted patients aged 18 or older who reported whether they had received or not received rehabilitation services and completed outcome (GOSE, PHQ-9, GAD-7, QOLIBRI-OS) assessments 12 months after injury.
The CENTER-TBI study (EC grant 602150) was conducted in accordance with relevant EU laws and those of the countries where the recruiting sites were located. Ethical approval was obtained for each recruiting site (see https://www.center-tbi.eu/project/ethical-approval for details), and all patients and/or legal guardian/next of kin signed informed consent.
Data and instruments
Sociodemographic, premorbid, and injury‐related data
The following sociodemographic data were collected at study enrollment: sex (female or male), age (continuous), education (continuous and dichotomized at median value ≥ 13 years), living situation (living alone or not), and employment status before injury (employed: full- and part-time employed, on sick leave, or in special/sheltered employment; unemployed: looking for work or unable to work; and other (retired, student, or homemaker).
Pre-injury psychiatric diseases (yes or no) were collected by self-report. The premorbid somatic health status was defined according to the American Society of Anesthesiologists Physical Status Classification System (ASA): healthy, mild systemic disease, severe systemic disease, and severe systemic disease with a constant threat to life. 22 The last two categories were merged into “severe systemic disease” due to low number of cases.
Injury-related information was collected at the time of recruitment. CT abnormalities (yes or no) were recorded, and the cause of injury was categorized into road traffic incident, fall, and violent/other (e.g., non-intentional injury, act of mass violence, and suicide attempt). TBI severity was determined by the Glasgow Coma Scale (GCS) (scores 3–8: severe, 9–12: moderate, 13–15: mild) at admission, 23 Abbreviated Injury Scale (AIS) ≥ 3 determined as severe brain injury) 24 and Injury Severity Score (ISS) ≥ 15 determined as major overall trauma). 25 Transitions between the emergency room (ER), intensive care unit (ICU), neurological hospital ward (WN), home (HO), rehabilitation (RE), other ward (WO), and other facilities (OT), were recorded. The most frequent transition of care (TOC) pathways, including more than 10 cases were defined, and TOCs with fewer than 10 patients were aggregated and termed Other. The number of transitions, and the end-point of the TOC defined as the last transition destination were also recorded (home, rehabilitation, other hospital, other). 26
Rehabilitation services
Data on whether patients received any inpatient-and/or out-patient rehabilitation services within the first 12 months after injury (1 = yes; 0 = no) were extracted from the study’s follow-up charts. In addition, information on the type of services received was categorized into the following: physical therapy, occupational therapy, speech therapy, therapeutic recreation, cognitive remediation, vocational services, psychological services, nursing services, comprehensive day treatment, peer mentoring, social work/case management, independent living training, home health, or other. Since multiple choices were possible, the services were categorized into three groups: no help, at least for one domain, or at least for two domains. Patients were asked to indicate rehabilitation service onset (within 1 month, between 1 and 3 months, or later than 3 months after injury).
Outcome instruments
The Glasgow Outcome Scale—Extended (GOSE) was used to assess patients’ functional recovery status. The GOSE is a structured clinician-administered interview designed to evaluate functional recovery after TBI on an eight-point scale (1: dead; 2: vegetative state; 3/4: lower/upper severe disability; 5/6: lower/upper moderate disability; 7/8: lower/upper good recovery). 27 In addition to the interview, the GOSE questionnaire (GOSE-Q) was administered. GOSE-Q is a structured proxy or self-report version of the scale that can be completed by patients or their relatives. In this study, missing clinician-rated GOSE data was replaced by GOSE-Q responses or clinical ratings. Since GOSE-Q does not distinguish between vegetative state and lower severe disability, GOSE levels 2 and 3 were collapsed into one category (2 or 3). For analytic purposes, the following categories were further merged: severe disability (2 to 4), moderate disability (5 to 6), and good recovery (7 to 8).
Emotional distress was assessed using the Patient Health Questionnaire (PHQ-9) and the Generalized Anxiety Disorder seven-item scale (GAD-7). The PHQ-9 is a nine-item questionnaire that measures depressive symptoms within the last 2 weeks. Items are scored from 0 (not at all) to 3 (nearly every day), yielding a total score ranging from 0 to 27, with higher scores reflecting greater symptom severity. Standard cut-off points are 0–4 no-symptoms, 5–9 mild, 10–19 moderate, and 20–27 severe symptoms. 28
The GAD-7 is a seven-item questionnaire that evaluates anxiety symptoms over the last 2 weeks. Items are scored from 0 (not at all) to 3 (nearly every day), yielding a total score ranging from 0 to 21, with higher scores reflecting greater symptom severity. Conventional cut-off values are 0–4 minimal, 5–9 mild, 10–14 moderate, and 15–21 severe symptoms. 29 For this study, the moderate and severe categories of each scale were combined due to the limited sample size in these groups.
Health-related quality of life was measured using the Quality of Life after Brain Injury-Overall Scale (QOLIBRI-OS). 30 The QOLIBRI-OS is a six-item measure specifically designed to capture the health-related quality of life in domains of functioning relevant for individuals after TBI. Each item is rated on a five-point Likert scale ranging from “not at all satisfied” (1) to “very satisfied” (5). Item scores are converted to a percentage score (0–100), with higher scores reflecting better satisfaction with health-related quality of life. For this study, the following cut-off points were used: poor (0–52), average (53–80), and high satisfaction (>81). 31
Statistical analysis
Descriptive statistics were used to characterize the cohort. For continuous variables, the mean, standard deviation, median, minimum, and maximum were reported; for categorical variables, absolute and relative frequencies were provided.
The proportion of missing data across independent variables ranged from <1% (rehabilitation services) to 33% (rehabilitation onset). Little’s Missing Completely At Random (MCAR) test indicated that missing data were not missing completely at random (χ2 = 2561.76, df = 560, p < .001). Thus, missing-at-random (MAR) was assumed, and missing values in predictor variables were handled with multivariate imputation by chained equations (MICE), using methods aligned with variable type. Outcome variables (GOSE, PHQ-9, GAD-7, and QOLIBRI-OS) were not imputed; analyses include only individuals with completed outcome measures at 12 months. A total of 10 imputed datasets were generated, and imputation diagnostics compared observed vs. imputed distributions and examined strip plots across imputations to detect anomalies.
For each 12-month outcome (GOSE, GAD-7, PHQ-9, and QOLIBRI-OS), ordinal regression models were fitted. The full candidate set included age, sex, education, living alone, employment status, psychiatric history, injury cause, AIS, ISS > 15, number of TOC, care end-point, rehabilitation services, time to rehabilitation support, and baseline GCS. The primary analysis applied an exhaustive all-subsets strategy for proportional-odds models. From an initial set of
All analyses were performed in R (version 4.4.1) using parallel computation on a Windows system. Missing data were handled using multivariate imputation by chained equations (MICE package 32 ), while ordinal regressions were conducted using the Modern Applied Statistics with S (MASS) 33 and ordinal 34 packages. Ordinal regression and related analyses were conducted using the following R packages: MASS, 33 ordinal, 34 and mice. 32
Results
Sample description
The total sample applicable to analyses consisted of 661 patients (Fig. 1). The majority were male (72.3%), with a mean age of 46.7 years (SD = 17.7) and an average of 13.7 (SD = 4.01) years of education. The most prevalent TBI severity levels were mild (n = 289) and severe (n = 249). Road traffic accidents (47.8%) and falls (37.1%) predominantly caused injuries. At 12 months post TBI, most participants (87.3%) showed a favorable recovery (GOSE 5–8), with mild depressive symptoms (Mean = 5.72; SD = 5.64), minimal anxiety symptoms (Mean = 3.85; SD = 4.45), and a mean QOLIBRI-OS score of 65.7 (SD = 22.5) (see Fig. 1 for the participants’ flow diagram) and Table 1 for Sociodemographic, preinjury and clinical characteristics of the sample.
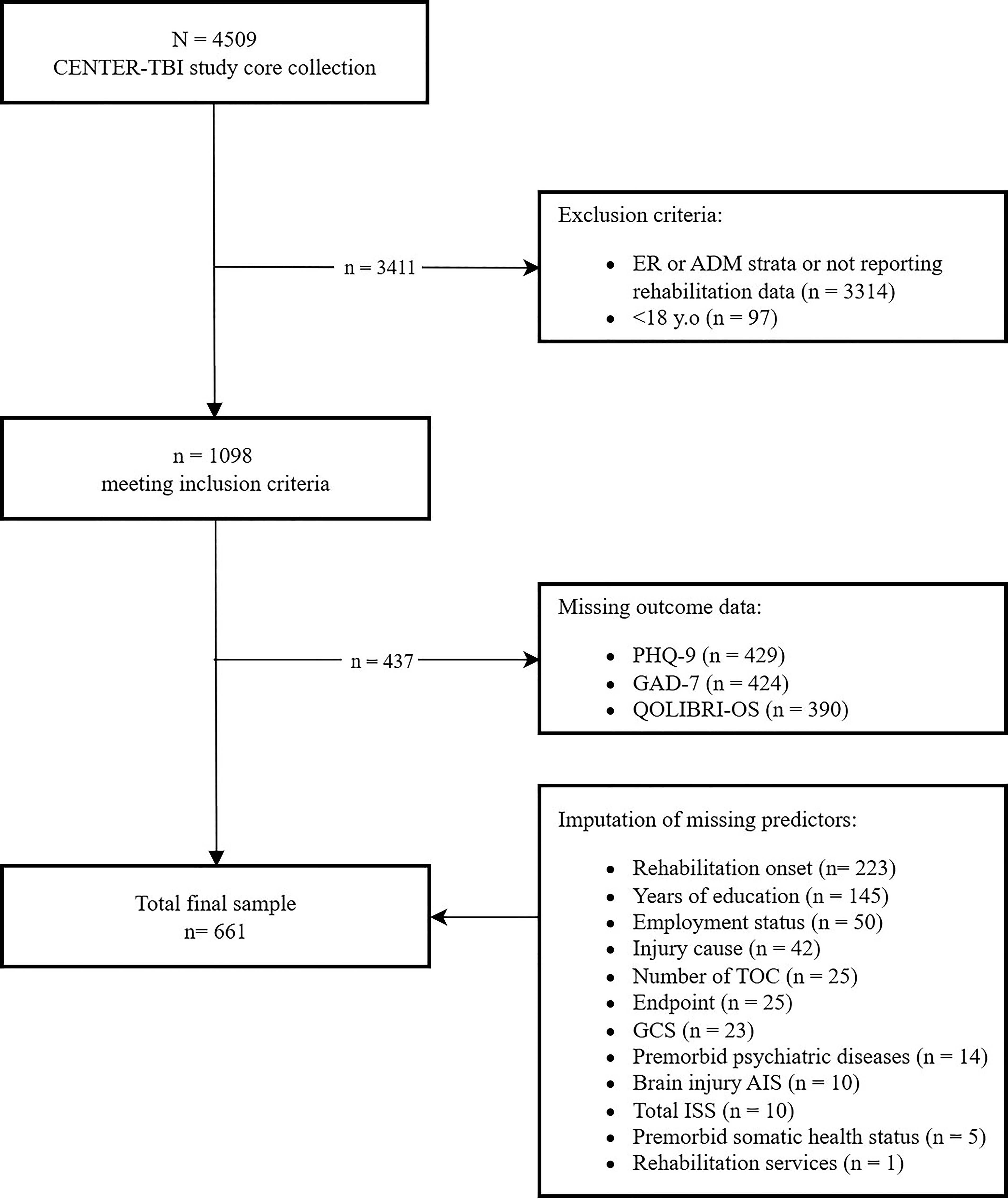
Participants’ flow diagram. Note. Emergency Room (ER); Hospital Ward Admission (ADM); Injury Severity Score (ISS); Abbreviated Injury Scale (AIS); Transition of Care (TOC); the Patient Health Questionnaire nine-item scale (PHQ-9); the Generalized Anxiety Disorder seven-item scale (GAD-7); the Quality Of Life After Brain Injury-Overall Scale (QOLIBRI-OS).
Excluded participants did not significantly differ from those included in analyses regarding age, sex, preinjury ASA, AIS, ISS, or GCS at admission. However, participants included in the study were more likely to have more years of education (p = 0.001), to be employed (p = 0.005), to live with someone (p = 0.007), to have no preinjury psychiatric history (p = 0.002), and to present abnormal CT findings (p = 0.004; see Supplementary Appendix SA4).
Rehabilitation services following ICU admission for TBI patients
Rehabilitation services were documented in 37.4% (n = 247) of the total TBI patients during the first year after the injury. Most patients reported receiving these services within the first month (27.4%, n = 181) or between the first and third months (28.7%, n = 190) after injury.
Looking at each time point assessment, follow-up charts established that at 3 months, many patients were not receiving rehabilitation (68.1%), particularly in the moderate (75.0%) and severe (80.3%) groups. The mild group had a lower proportion without rehabilitation (55.4%). At 6 months, the proportion of patients not receiving rehabilitation decreased (61.6%) but remained higher in the moderate (67.0%) and severe (72.7%) groups compared with mild (50.5%). At 12 months, 51.3% of patients had received rehabilitation. However, a substantial proportion, particularly in the severe (56.6%) and moderate (43%) groups, did not receive rehabilitation services at this point of time (see Supplementary Appendix SA1).
Physical therapy was the most administered rehabilitation service at 3, 6, and 12 months after injury, although its frequency decreased over time (88%, 84.1%, and 73.5%, respectively). Occupational therapy followed a similar trend, with 32.5% of patients receiving it at 3 months, 33% at 6 months, and 24.5% at 12 months.
In contrast, speech therapy and psychological and cognitive therapy showed an increasing proportion of patients receiving these interventions over time. For example, speech therapy was provided to 23.9% of patients at 3 months, increasing to 26.1% at 6 months, and to 28.4% at 12 months. Psychological therapy also increased, with 19.7% at 3 months, 23.3% at 6 months, and 30.4% at 12 months. Cognitive remediation exhibited the most substantial increase, rising from 15.4% at 3 months to 24.4% and 29.4% at 6- and 12-month post-injury, respectively.
Sociodemographic, injury, and rehabilitation effects on outcomes
Functional status recovery (GOSE)
Individuals with more than 13 years of education (OR = 1.46; 95% CI [1.05–2.02]) and those in other employment situations (OR = 1.58; 95% CI [1.06–2.36]) were more likely to achieve better functional recovery 12 months after TBI than those with less than 13 years of education and employment situation. Poorer functional outcomes one year after injury were associated with older age (OR = 0.99; 95% CI [0.98–1.00]), more severe brain injury (AIS = 3, OR = 0.14; 95% CI [0.04–0.54]; AIS = 4, OR = 0.13; 95% CI [0.03–0.46]; AIS = 5, OR = 0.11; 95% CI [0.03–0.41]), traffic accident as injury cause (OR = 0.55; 95% CI [0.39–0.79]) compared with falls, a higher number of TOC (OR = 0.85; 95% CI [0.76–0.95]), and end-point at another hospital (OR = 0.60; 95% CI [0.39–0.94]) or other setting (OR = 0.24; 95% CI [0.08–0.74]) compared with discharge to home. Receiving rehabilitation at 3, 6, or 12 months after TBI, which likely reflects greater injury severity, was also associated with poorer outcomes (OR = 0.22; 95% CI [0.16–0.32]), as was delayed initiation of rehabilitation based on self-reported data (>3 months after injury; OR = 0.53; 95% CI [0.33–0.84]; see Fig. 2). For more details on the coefficient models, see Supplementary Appendix SA2.
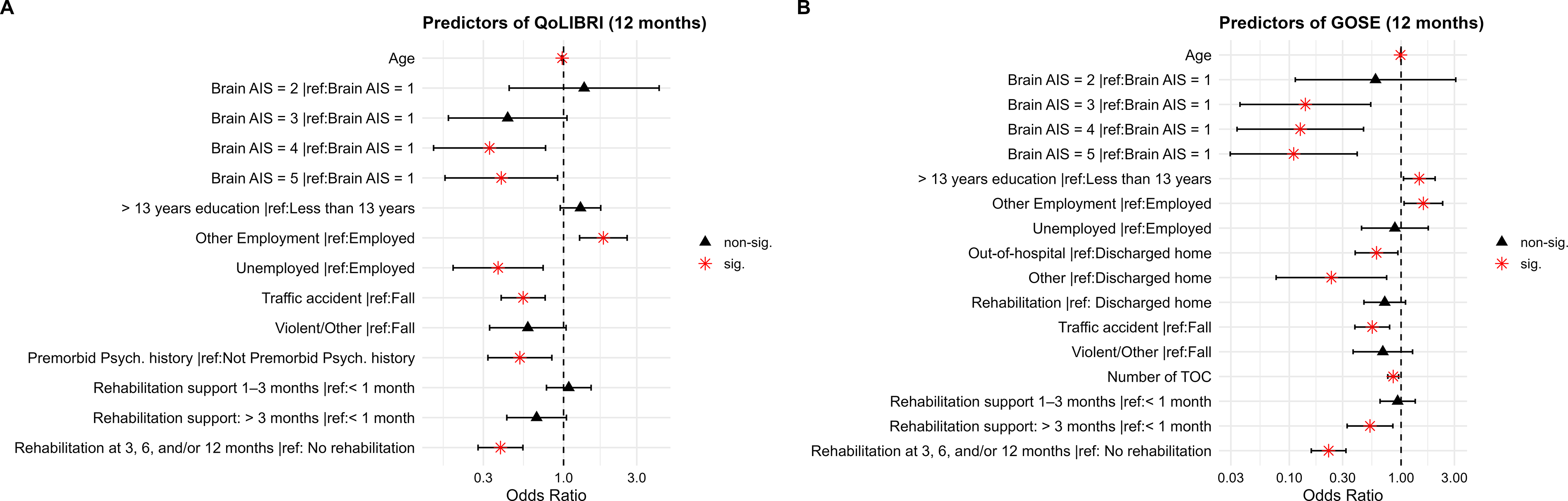
Odds ratios and 95% CIs for the ordinal logistic regression for QOLIBRI-OS (Panel A) and GOSE (Panel B). Note. Abbreviated Injury Scale (AIS); the Quality of Life After Brain Injury-Overall Scale (QOLIBRI-OS).
TBI-specific health-related quality of life outcome (QOLIBRI-OS)
Being in other employment situations (OR = 1.82; 95% CI [1.27–2.6]) emerged as protective factor for health-related quality of life compared with being employed. In contrast, individuals with older age (OR = 0.98; 95% CI [0.97–0.99]), who were unemployed (OR = 0.37; 95% CI [0.19–0.74]) compared with employed, with a history of psychiatric disorder (OR = 0.52; 95% CI [0.32–0.84]), with an AIS score of 4 (OR = 0.33; 95% CI [0.14–0.76]) or 5 (OR = 0.39; 95% CI [0.17–0.91]), with traffic accident as cause of injury (OR = 0.55; 95% CI [0.39–0.76]) compared with falls, and with rehabilitation service received at 3, 6 or 12 months (OR = 0.39; 95% CI [0.28–0.54]) were more likely to present poor health-related quality of life one year after TBI (see Fig. 2).
Emotional distress (PHQ-9 and GAD-7)
Higher odds of experiencing more pronounced anxiety and depression symptomatology at 12 months post injury were found for individuals whose injuries were caused by traffic accident compared with falls (GAD-7: OR = 1.86; 95% CI [1.27–2.72]; PHQ-9: OR = 1.47; 95% CI [1.05–2.05]), those who reported a history of psychiatric disorder (GAD-7: OR = 3.29; 95% CI [1.99–5.44]; PHQ-9: OR = 3.41; 95% CI [2.09–5.55]), and those who received rehabilitation at 3, 6, or 12 months after TBI (GAD-7: OR = 2.36; 95% CI [1.64–3.38]; PHQ-9: OR = 2.22; 95% CI [1.6–3.09]). In addition, compared with employment, unemployment was associated with worse anxiety symptomatology (OR = 2.21; 95% CI [1.16–4.21]), while other employment was associated with better depressive symptomatology (OR = 0.69; 95% CI [0.48–0.99]; see Fig. 3).
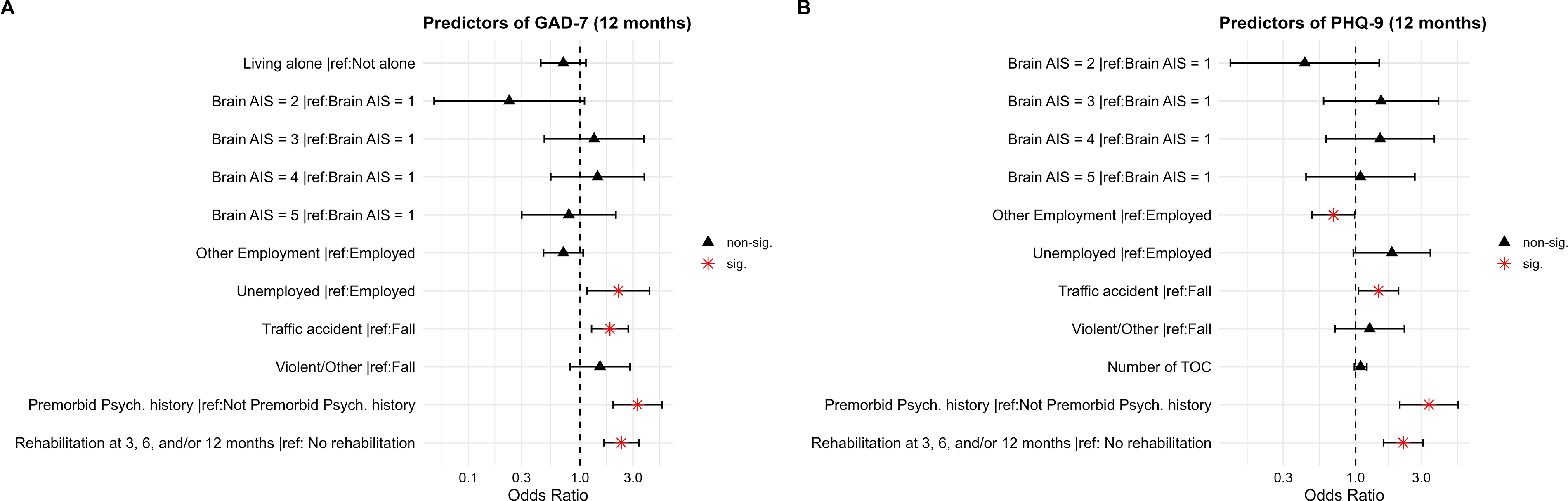
Odds ratios and 95% CIs for the ordinal logistic regression for GAD-7 and PHQ-9 (Panel A and B respectively). Note. Abbreviated Injury Scale (AIS); the Patient Health Questionnaire (PHQ-9); the Generalized Anxiety Disorder seven-item scale (GAD-7).
For all four models, diagnostic checks supported the validity of the proportional-odds assumption and homogeneity of variance. Both the nominal and scale tests were nonsignificant (all
Longitudinal analyses
To examine the stability of these findings over time, additional longitudinal ordinal regression models were estimated for functional outcome, emotional distress, and HRQL, including repeated assessments at 3-, 6-, and 12-months post-injury. For these analysis, 636 individuals were included with completed outcome measures at each time points.
For functional recovery, a significant non-linear effect of time was found (β = –11.95), showing that the probability of achieving good functional recovery increased over time, whereas moderate levels declined. The probability of maintaining severe disability remained low throughout the follow-up period. Patients with older age were more likely to present poorer GOSE scores (β = –0.02), while those with more than 13 years of education (β = 0.70) and in other employment situation (β = 0.56) compared with employment had a higher likelihood of achieving better scores. Among injury characteristics, road traffic accident (β = –0.98) and violence/other (β = –0.91) as the cause of injury reported worse functional recovery after 12 months post-injury. Similarly, injury severity measured with AIS was also associated with worse recovery (AIS 3 = β = –2.23; AIS 4 = β = –2.15; AIS 5 = β = –2.80). Regarding rehabilitation factors, higher number of TOC (β = –0.26) was related to lower functional recovery, as well as those discharged to rehabilitation units (β = –0.78) or other destination (β = –2.65) compared with patients discharged home. Moreover, receiving rehabilitation services was linked to lower functional recovery (β = –2.52), particularly when self-reported rehabilitation initiation occurred between 1 and 3 months (β = –0.98) and later than 3 months post-injury (β = –1.25).
A significant nonlinear effect of time on health-related quality of life was found (β = −4.89), suggesting that the probability of reporting poor and high QOLIBRI-OS levels decreased over time, while the likelihood of reporting average levels of quality of life remained relatively stable. Among sociodemographic variables, older age was associated with poorer QOLIBRI-OS scores (β = –0.03); those who were employed maintained better health-related quality of life compared with those unemployed (β = –1.14), while those in other employment situations had better health-related quality of life compared with those in employment situation (β = 0.59). Moreover, participants with a history of psychiatric disorder (β = –1.20) and road traffic accident (β = –1.023) compared with falls as the cause of injury reported worse scores across time. Likewise, those who received rehabilitation services at any point of the follow-up (3, 6, or 12 months after TBI) showed lower QOLIBRI-OS scores (β = –1.25), particularly when self-reported rehabilitation was initiated later than 3 months post-injury (β = –0.79) (see Fig. 4).
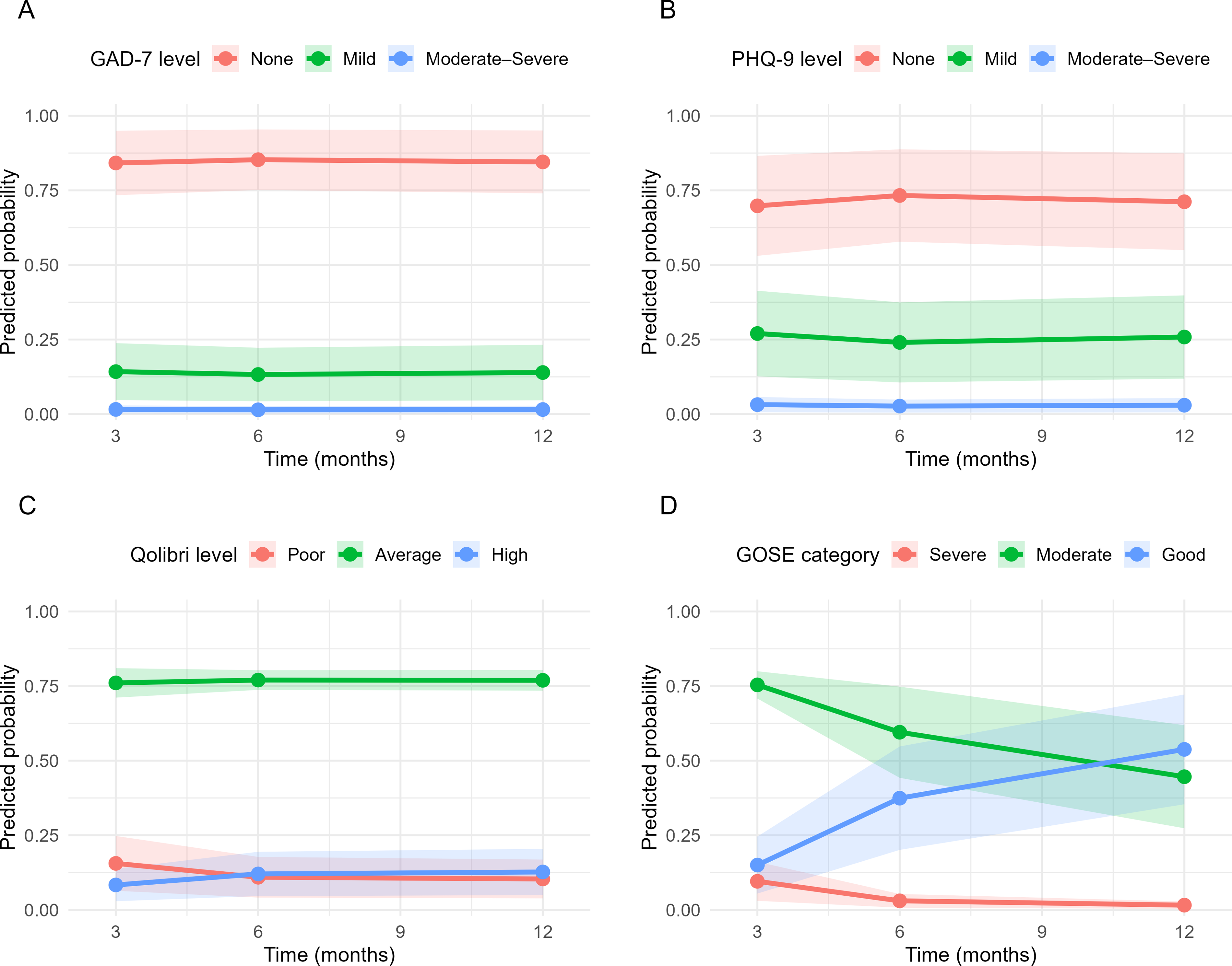
Predicted probabilities of anxiety, depression, health-related quality of life, and functional outcomes over time. Note. The Generalized Anxiety Disorder seven-item scale (GAD-7) (Panel A); The Patient Health Questionnaire (PHQ-9) (Panel B); the Quality of Life After Brain Injury—Overall Scale (QOLIBRI-AS) (Panel C); Glasgow Outcome Scale-Extended (Panel D). Shaded areas represent 95% confidence intervals.
Finally, regarding anxiety (GAD-7) and depression (PHQ-9), no significant time effect or time interactions were observed. For more details on regression analyses results, see Supplementary Appendix SA3.
To evaluate the robustness of our findings under different missingness assumptions, we conducted a sensitivity analysis, repeating the exhaustive variable selection procedure on complete cases only (n = 292) and comparing the results against the primary multiply imputed analysis (n = 636). Predictor overlap ranged from 33.3% to 75.0% across outcomes, and in all four outcomes the predictors retained under complete-case analysis constituted a strict subset of those identified in the imputed models (data not shown).
Discussion
This study describes the provision of rehabilitation services to a large cohort of patients after TBI admitted to the ICU and investigates associations between rehabilitation provision and functional outcomes, emotional distress, and TBI-specific HRQoL 12 months post-injury while controlling for sociodemographic, premorbid conditions, and injury-related factors. The study also examined the stability of these outcomes at 3, 6, and 12 months following injury.
Consistent with findings from other CENTER-TBI studies, the TBI profile in this cohort differs substantially from that reported in earlier observational research. Participants were, on average, older, with a median age of 50 years, and exhibited a higher burden of comorbidities. Furthermore, notable discrepancies emerged between traditional TBI severity classifications based on the GCS and the actual care pathways: patients with GCS scores of 13–15 (mild TBI) accounted for more than one-third of ICU admissions. 35 This divergence suggests that contemporary clinical decision-making regarding ICU admission extends beyond GCS-defined injury severity and increasingly reflects a broader consideration of patient-related factors such as age, comorbid conditions, and injury complexity.
The proportion of participants receiving rehabilitation services in this study increased progressively during the first-year post-injury, rising from 30.6% at 3 months to 51.3% at 12 months. Notably, the highest proportion of rehabilitation services was reported among individuals with GCS 13–15 during the first three months (42.9%). This trend likely reflects positive prognostic expectations and fewer medical complications in individuals with milder brain injuries, allowing for earlier initiation of rehabilitation interventions. 36 In contrast, there was a marked increase in rehabilitation service provision among those with GCS 9–12 and GCS 3–8 between 3 and 12 months post-injury from 24% to 51% and from 18.5% to 41%, respectively. The delayed initiation of rehabilitation in these groups may be attributable to greater injury severity and medical complexity, prolonged hospitalization, or extended nursing care needs during the acute recovery phase. 37 Also, cognitive, emotional, and behavioral sequelae can influence an individual’s ability to engage in and benefit from rehabilitation 38 and community participation. 39 Nevertheless, approximately half of the participants with moderate and severe TBIs did not receive any rehabilitation services during the first post-injury year, underscoring existing gaps in access to appropriate care. 9
Consistent with prior research, physical therapy was the most frequently provided rehabilitation service, reflecting its broad availability across health care systems.11,14,40 Occupational therapy, aimed at restoring patients’ independence in activities of daily living, was the second most frequently delivered rehabilitation service, provided to approximately one-third of participants at 3 months post-injury, with a gradual decline observed over subsequent follow-ups. This pattern parallels that of physical therapy and likely reflects the primarily acute and subacute focus of these interventions. In contrast, speech therapy, psychological support, and cognitive remediation were provided to fewer than one-fifth of participants at 3 months, and these remained the least frequently accessed rehabilitation services across all time points. Comparable trends of under-provision have been documented in previous research, despite consistent evidence underscoring the critical role of these therapies in promoting cognitive recovery, emotional adjustment, and overall functional reintegration following TBI.8,14 Encouragingly, an upward trend in the provision of these specialized interventions was observed at 6 and 12 months, likely reflecting their relevance during the post-acute phase, when cognitive and psychological difficulties become more evident. 8 This pattern may also indicate the accumulation of unmet rehabilitation needs over time, which, if not addressed early, can contribute to symptom persistence and chronicity.9,41
Most participants demonstrated favorable overall recovery (GOSE levels of 5–8), low levels of emotional distress, and average HRQoL at 12 months post-injury. However, participants after moderate to severe TBI exhibited significantly poorer functional outcomes compared with those after mild TBI, whereas emotional distress and HRQoL were comparable across severity groups. These findings align with previous research indicating that, although functional limitations are more pronounced with greater injury severity, psychological adjustment and perceived quality of life may depend on broader psychosocial factors such as self-awareness, coping strategies, social support, and individual resilience.15,16
Receiving rehabilitation services, particularly when initiated more than three months post-injury, as well as experiencing a higher number of care transitions, were both indicative of greater injury severity and were associated with poorer functional outcomes, lower HRQoL at 12 months, and less favorable longitudinal recovery trajectories. Prior studies have demonstrated that early initiation of rehabilitation following severe TBI is both clinically beneficial and cost-effective.3,8,42 In contrast, delayed rehabilitation may constrain functional recovery and psychosocial adjustment by missing critical windows for neuroplasticity and early adaptive reorganization.12,13 Moreover, a higher number of TOCs may not only reflect increased injury severity and medical complexity but also point to inefficiencies within the rehabilitation pathway, such as fragmented service delivery, inconsistent follow-up, or delays in accessing specialized rehabilitation. These disruptions can compromise continuity of care and diminish overall treatment efficacy. Therefore, patients with more severe or complex injuries, often including significant extracranial trauma, should be prioritized for timely and intensive rehabilitation interventions to maximize recovery potential. Ultimately, poorer 12-month outcomes among these individuals likely reflect the cumulative burden of injury and the inherently prolonged trajectory of recovery rather than the ineffectiveness of rehabilitation itself.
Older age, lower educational attainment, and unemployment were associated with poorer functional recovery and reduced HRQoL, consistent with previous research.15,43 In addition, sustaining a TBI because of a road traffic accident and experiencing greater injury severity, as reflected by higher AIS scores, were both associated with poorer functional and HRQoL outcomes. This suggests that individuals at risk of incomplete recovery after TBI should receive structured, ongoing follow-up programs for early and long-term multidimensional rehabilitation, integrating therapy of cognitive and emotional problems and community reintegration. A history of pre-injury psychiatric disorders was also associated with less favorable recovery and greater emotional distress, in line with evidence that preexisting conditions are robust predictors of adverse outcomes following TBI. 11 TBI may exacerbate underlying physical or psychological vulnerabilities or create compounded challenges that hinder recovery. 44
Time since injury independently predicted longitudinal changes in most outcomes, except for emotional distress, and interacted with several of the aforementioned factors. The consistency of these associations across both cross-sectional and longitudinal analyses reinforces the robustness of the identified predictors and their clinical utility for outcome monitoring and individualized intervention planning. The lack of temporal change in emotional distress may reflect the early establishment of psychological symptom trajectories following TBI, potentially influenced by pre-injury vulnerabilities, acute stress responses, and limited access to timely psychosocial support. This stability suggests that individuals at risk for persistent emotional difficulties can be identified as early as during the ICU stay, underscoring the importance of systematic screening and early, integrated psychological care to prevent the consolidation of chronic distress and its detrimental effects on recovery and quality of life.
Strength and limitations
The strengths of the present study include its large sample size and broad representation of participating European countries, which together provide a robust overview of rehabilitation service provision for patients with TBI admitted to the ICU. However, the contributing hospitals were mostly specialized trauma centers, which may limit the generalizability of the findings for patients in more local hospitals and those not admitted to the ICU. The combination of the study inclusion criteria and the incompleteness of the follow-up data led to a substantial decrease in the available number of participants in this study. Participants were more likely to have higher educational attainment, live with a spouse or partner, and be employed, sociodemographic characteristics commonly associated with greater health literacy, stronger social support networks, and higher levels of health care engagement. 45 This pattern indicates a probable selection bias toward individuals with more socioeconomic resources, who are more likely to recognize symptoms, seek timely medical care, and navigate complex health care systems. Consequently, participants with social or economic disadvantages who may experience barriers to access, lower help-seeking behavior, and reduced continuity of care are likely underrepresented. Such disparities may limit the generalizability of the findings and highlight the need for targeted efforts to understand and improve rehabilitation access among socially vulnerable TBI populations.
In addition, it remains unclear whether the rehabilitation services reported in this study specifically targeted the consequences of TBI or addressed extracranial injuries. Participants were asked to indicate any rehabilitation support received “because of their injury,” and since physiotherapy was the most frequently reported service, it is possible some of these interventions focused on extracranial injuries rather than TBI-related impairments.
To avoid loss of statistical power, we imputed missing predictor values using the MICE approach for those individuals with completed outcome measures at 12 months. We used models aligned with the nature of the outcomes, which were ordinal. Although computationally expensive, the variable-selection strategy is highly robust, allowing us to evaluate all possible combinations and select the best model based on fit and predictive performance, beyond p-values. However, this approach was applied only to cross-sectional analyses, as no robust strategy yet exists to extend it to longitudinal analyses. As a sensitivity analysis, the selection procedure was repeated on complete cases only, compared with the primary imputed dataset. Predictors retained under complete-case analysis constituted a strict subset of those identified in the imputed models in all four outcomes, indicating that MICE recovered meaningful predictive signal rather than introducing spurious associations. This consistency supports the robustness of the primary variable selection results and the appropriateness of multiple imputations as the primary analytic strategy. No imputation was performed for the outcomes due to insufficient data to support reliable prediction, particularly given that the missingness was likely not at random. A comparison between excluded and included participants indicated that those included were more severely injured, as evidenced by injury-related intracranial findings on CT. Future research should prioritize this vulnerable group—for example, by incorporating proxy ratings—to better understand their needs.
Conclusions
This study provides new insights into the delivery and timing of rehabilitation services for patients after TBI admitted to the ICU and their associations with recovery outcomes over the first post-injury year. Despite gradual increases in rehabilitation service provision, many individuals, particularly those after more severe TBIs, did not receive comprehensive care during this critical period. Early initiation of therapy and rehabilitation and improved care coordination appear essential for optimizing functional recovery and HRQoL after TBI. These findings emphasize the importance of systematic follow-up and timely access to specialized rehabilitation for at-risk individuals and support the development of integrated, patient-centered care models to enhance recovery trajectories and long-term outcomes.
Transparency, Rigor, and Reproducibility Summary
CENTER-TBI is pre-registered at clinicaltrials.gov (number NCT02210221). The analysis plan for the current study was presented in a protocol available on: https://www.center-tbi.eu/data/approved-proposals. The sample size was the one available from the ICU stratum of Core study, namely, 2138 patients. After excluding patients with missing data in crucial predictor and outcome variables, 661 subjects were included. Data were labeled using Global Unique Patient Identifier codes. CENTER-TBI included patients between 2014 and 2017. Data were analyzed using R version 4.1.1. All equipment and software used to perform analysis are publicly available from https://www.R-project.org. The key prognostic factors used in the current study are established standards in the TBI field. Statistical analyses were provided by the first three authors. Author D.R. is well-known statistical expert in the field of TBI research and prognostic modeling. Missing data have been handled as reported in the statistical analyses section. Extensive methodology statements of CENTER-TBI are publicly available, as stated and referenced to in the methods. Data and analytic code from this study are available upon reasonable request to the study authors, after approval by the management teams of CENTER-TBI. Deidentified CENTER-TBI data are available to researchers who provide a study proposal for review and approval by the management committee (submitted online at https://www.center-tbi.eu/data). Access and use of CENTER-TBI data require adherence to the CENTER-TBI Data Use Agreement and harmonized procedures for data access requests.
Sociodemographic, Preinjury and Clinical Characteristics of the Sample
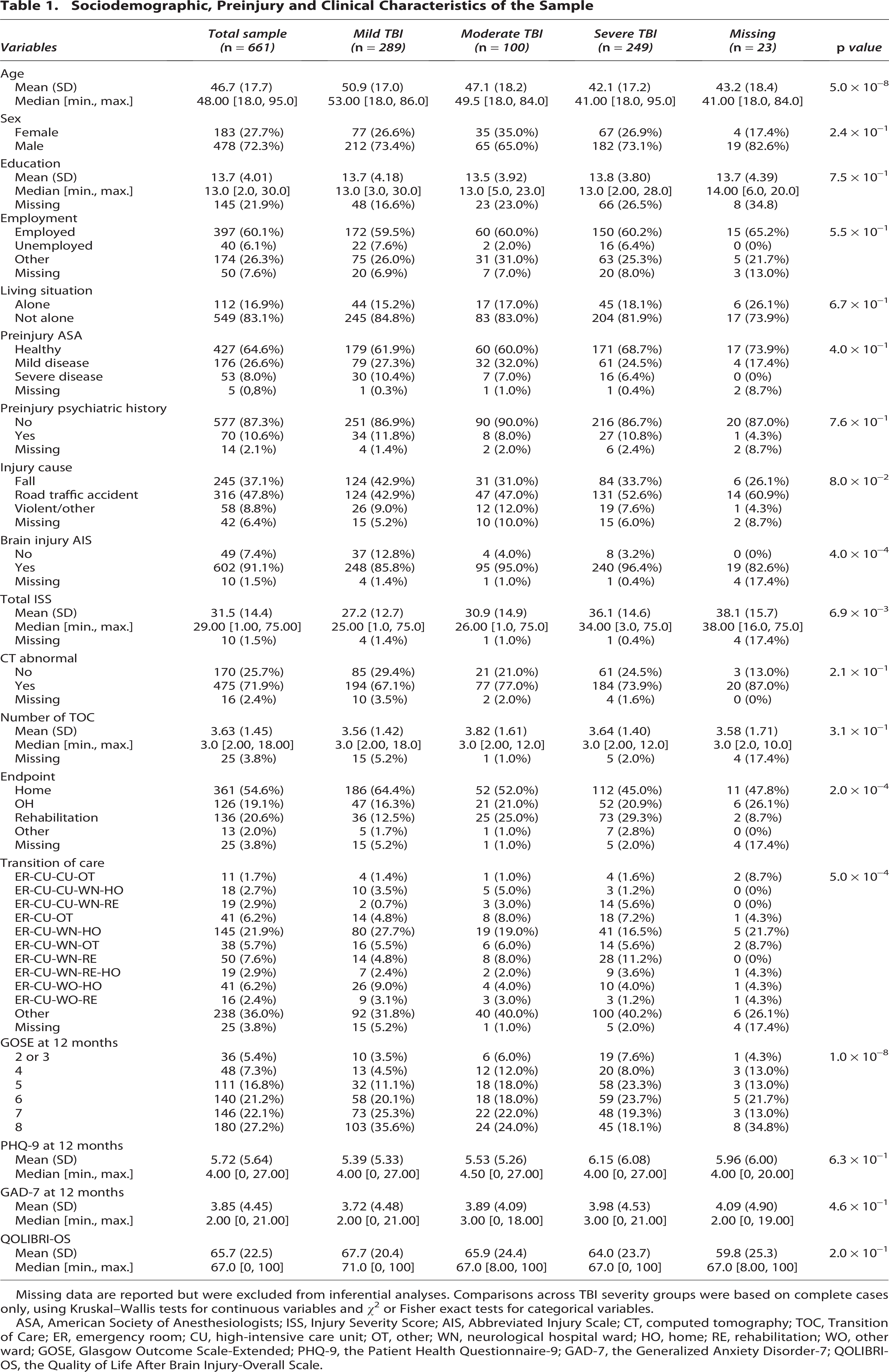
Missing data are reported but were excluded from inferential analyses. Comparisons across TBI severity groups were based on complete cases only, using Kruskal–Wallis tests for continuous variables and χ2 or Fisher exact tests for categorical variables.
ASA, American Society of Anesthesiologists; ISS, Injury Severity Score; AIS, Abbreviated Injury Scale; CT, computed tomography; TOC, Transition of Care; ER, emergency room; CU, high-intensive care unit; OT, other; WN, neurological hospital ward; HO, home; RE, rehabilitation; WO, other ward; GOSE, Glasgow Outcome Scale-Extended; PHQ-9, the Patient Health Questionnaire-9; GAD-7, the Generalized Anxiety Disorder-7; QOLIBRI-OS, the Quality of Life After Brain Injury-Overall Scale.
Supplemental Material
sj-docx-1-ntr-10.1177_2689288X261452589 — Supplemental material for Rehabilitation and Outcomes in Patients after Traumatic Brain Injury Admitted to the Intensive Care Unit: Results from the CENTER-TBI Study
Supplemental material, sj-docx-1-ntr-10.1177_2689288X261452589 for Rehabilitation and Outcomes in Patients after Traumatic Brain Injury Admitted to the Intensive Care Unit: Results from the CENTER-TBI Study by Nada Andelic, Diego Rivera, Laiene Olabarrieta-Landa, Mari S. Rasmussen, Emilie I. Howe, Louis Jacob, Philippe Azouvi, Marina Zeldovich, Eirik Helseth, Cathrine Tverdal, John Castro, Torgeir Hellstrøm, Marit V.D. Forslund, Ida Borgen, Ingerid Kleffelgaard, Helene L. Søberg, Unni Sveen, Marianne Løvstad, Solveig L. Hauger, Juan Lu, Simon Beaulieu-Bonneau, Olli Tenovuo, Nicole von Steinbuechel, and Cecilie Røe
Footnotes
Acknowledgments
The CENTER-TBI ICU WP6 participants and ICU ONLY investigators (to be indexed as “Collaborators” in PubMed):
Cecilia Åkerlund (Department of Physiology and Pharmacology, Section of Perioperative Medicine and Intensive Care, Karolinska Institutet, Stockholm, Sweden); Krisztina Amrein (János Szentágothai Research Centre, University of Pécs, Pécs, Hungary); Nada Andelic (Division of Clinical Neuroscience, Department of Physical Medicine and Rehabilitation, Oslo University Hospital and University of Oslo, Oslo, Norway); Lasse Andreassen (Department of Neurosurgery, University Hospital Northern Norway, Tromso, Norway); Audny Anke (Department of Physical Medicine and Rehabilitation, University Hospital Northern Norway, Tromso, Norway); Gérard Audibert (Department of Anesthesiology & Intensive Care, University Hospital Nancy, Nancy, France); Philippe Azouvi (Raymond Poincare hospital, Assistance Publique—Hopitaux de Paris, Paris, France); Maria Luisa Azzolini (Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy); Ronald Bartels (Department of Neurosurgery, Radboud University Medical Center, Nijmegen, The Netherlands); Ronny Beer (Department of Neurology, Neurological Intensive Care Unit, Medical University of Innsbruck, Innsbruck, Austria); Bo-Michael Bellander (Department of Neurosurgery & Anesthesia & intensive care medicine, Karolinska University Hospital, Stockholm, Sweden); Habib Benali (Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France); Maurizio Berardino (Department of Anesthesia & ICU, AOU Città della Salute e della Scienza di Torino—Orthopedic and Trauma Center, Torino, Italy); Luigi Beretta (Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy); Erta Beqiri (NeuroIntensive Care, Niguarda Hospital, Milan, Italy); Morten Blaabjerg (Department of Neurology, Odense University Hospital, Odense, Denmark); Stine Borgen Lund (Department of Public Health and Nursing, Faculty of Medicine and health Sciences, Norwegian University of Science and Technology, NTNU, Trondheim, Norway); Camilla Brorsson (Department of Surgery and Perioperative Science, Umeå University, Umeå, Sweden); Andras Buki (Department of Neurosurgery, Medical School, University of Pécs, Hungary and Neurotrauma Research Group, János Szentágothai Research Centre, University of Pécs, Hungary); Manuel Cabeleira (Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Alessio Caccioppola (Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy); Emiliana Calappi (Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy); Maria Rosa Calvi (Department of Anesthesiology & Intensive Care, S Raffaele University Hospital, Milan, Italy); Peter Cameron (ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia); Guillermo Carbayo Lozano (Department of Neurosurgery, Hospital of Cruces, Bilbao, Spain); Marco Carbonara (Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy); Ana M. Castaño-León (Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain); Simona Cavallo (Department of Anesthesia & ICU, AOU Città della Salute e della Scienza di Torino—Orthopedic and Trauma Center, Torino, Italy); Giorgio Chevallard (NeuroIntensive Care, Niguarda Hospital, Milan, Italy); Arturo Chieregato (NeuroIntensive Care, Niguarda Hospital, Milan, Italy); Giuseppe Citerio (School of Medicine and Surgery, Università Milano Bicocca, Milano, Italy; NeuroIntensive Care Unit, Department Neuroscience, IRCCS Fondazione San Gerardo dei Tintori, Monza, Italy); Hans Clusmann (Department of Neurosurgery, Medical Faculty RWTH Aachen University, Aachen, Germany); Mark Coburn (Department of Anesthesiology and Intensive Care Medicine, University Hospital Bonn, Bonn, Germany); Jonathan Coles (Department of Anesthesia & Neurointensive Care, Cambridge University Hospital NHS Foundation Trust, Cambridge, UK); Jamie D. Cooper (School of Public Health & PM, Monash University and The Alfred Hospital, Melbourne, Victoria, Australia); Marta Correia (Radiology/MRI department, MRC Cognition and Brain Sciences Unit, Cambridge, UK); Endre Czeiter (Department of Neurosurgery, Medical School, University of Pécs, Hungary and Neurotrauma Research Group, János Szentágothai Research Centre, University of Pécs, Hungary); Marek Czosnyka (Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Claire Dahyot-Fizelier (Intensive Care Unit, CHU Poitiers, Potiers, France); Paul Dark (University of Manchester NIHR Biomedical Research Centre, Critical Care Directorate, Salford Royal Hospital NHS Foundation Trust, Salford, UK.); Véronique De Keyser (Department of Neurosurgery, Antwerp University Hospital, Edegem, Belgium); Vincent Degos (Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France); Francesco Della Corte (Department of Anesthesia & Intensive Care, Maggiore Della Carità Hospital, Novara, Italy); Hugo den Boogert (Department of Neurosurgery, Radboud University Medical Center, Nijmegen, The Netherlands); Bart Depreitere (Department of Neurosurgery, University Hospitals Leuven, Leuven, Belgium); Dula Dilvesi (Department of Neurosurgery, Clinical centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia); Abhishek Dixit (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Jens Dreier (Center for Stroke Research Berlin, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany); Guy-Loup Dulière (Intensive Care Unit, CHR Citadelle, Liège, Belgium); Ari Ercole (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Erzsébet Ezer (Department of Anaesthesiology and Intensive Therapy, University of Pécs, Pécs, Hungary); Martin Fabricius (Departments of Neurology, Clinical Neurophysiology and Neuroanesthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark); Kelly Foks (Department of Neurology, Erasmus MC, Rotterdam, the Netherlands); Shirin Frisvold (Department of Anesthesiology and Intensive care, University Hospital Northern Norway, Tromso, Norway); Alex Furmanov (Department of Neurosurgery, Hadassah-hebrew University Medical center, Jerusalem, Israel); Damien Galanaud (Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France); Dashiell Gantner (ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia); Alexandre Ghuysen (Emergency Department, CHU, Liège, Belgium); Lelde Giga (Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia); Jagos Golubovic (Department of Neurosurgery, Clinical centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia); Pedro A. Gomez (Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain); Benjamin Gravesteijn (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Francesca Grossi (Department of Anesthesia & Intensive Care, Maggiore Della Carità Hospital, Novara, Italy); Deepak Gupta (Department of Neurosurgery, Neurosciences Centre & JPN Apex trauma centre, All India Institute of Medical Sciences, New Delhi-110029, India); Iain Haitsma (Department of Neurosurgery, Erasmus MC, Rotterdam, the Netherlands); Raimund Helbok (Department of Neurology, Kepler University Hospital, Johannes Kepler University Linz, Linz, Austria; Clinical Research Institute for Neuroscience, Johannes Kepler University Linz, Linz, Austria); Eirik Helseth (Department of Neurosurgery, Oslo University Hospital, Oslo, Norway); Jilske Huijben (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Peter J. Hutchinson (Division of Neurosurgery, Department of Clinical Neurosciences, Addenbrooke’s Hospital & University of Cambridge, Cambridge, UK); Stefan Jankowski (Neurointensive Care, Sheffield Teaching Hospitals NHS Foundation Trust, Sheffield, UK); Faye Johnson (Salford Royal Hospital NHS Foundation Trust Acute Research Delivery Team, Salford, UK); Mladen Karan (Dep-artment of Neurosurgery, Clinical centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia); Angelos G. Kolias (Division of Neurosurgery, Department of Clinical Neurosciences, Addenbrooke’s Hospital & University of Cambridge, Cambridge, UK); Daniel Kondziella (Departments of Neurology, Clinical Neurophysiology and Neuroan-esthesiology, Region Hovedstaden Rigshospitalet, Copenhagen, Denmark); Evgenios Kornaropoulos (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Lars-Owe Koskinen (Department of Clinical Neuroscience, Neurosurgery, Umeå University, Umeå, Sweden); Noémi Kovács (Hungarian Brain Research Program—Grant No. KTIA_13_NAP-A-II/8, University of Pécs, Pécs, Hungary); Ana Kowark (Department of Anaesthesiology, University Hospital of Aachen, Aachen, Germany); Alfonso Lagares (Department of Neurosurgery, Hospital Universitario 12 de Octubre, Madrid, Spain); Steven Laureys (Cyclotron Research Center, University of Liège, Liège, Belgium); Fiona Lecky (Centre for Urgent and Emergency Care Research \(CURE\); Health Services Research Section, School of Health and Related Research \(ScHARR\); University of Sheffield, Sheffield, UK; Emergency Department, Salford Royal Hospital, Salford UK); Didier Ledoux (Cyclotron Research Center, Univ-ersity of Liège, Liège, Belgium); Aurelie Lejeune (Department of Anesthesiology-Intensive Care, Lille University Hospital, Lille, France); Roger Lightfoot (Department of Anesthesiology & Intensive Care, University Hospitals Southhampton NHS Trust, Southhampton, UK); Hester Lingsma (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Andrew I.R. Maas (Department of Neurosurgery, Antwerp University Hospital, Edegem, Belgium; Department of Translational Neuroscience, Faculty of Medicine and Health Science, University of Antwerp, Antwerp, Belgium); Alex Manara (Intensive Care Unit, Southmead Hospital, Bristol, Bristol, UK); Costanza Martino (Department of Anesthesia & Intensive Care; M. Bufalini Hospital, Cesena, Italy); Hugues Maréchal (Intensive Care Unit, CHR Citadelle, Liège, Belgium); Julia Mattern (Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany); Catherine McMahon (Dep-artment of Neurosurgery, The Walton centre NHS Foundation Trust, Liverpool, UK); David Menon (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Tomas Menovsky (Department of Neurosurgery, Antwerp University Hospital, Edegem, Belgium; Department of Translational Neuroscience, Faculty of Medicine and Health Science, University of Antwerp, Antwerp, Belgium); Benoit Misset (Cyclotron Research Center, University of Liège, Liège, Belgium); Visakh Muraleedharan (Karolinska Institutet, INCF Inter-national Neuroinformatics Coordinating Facility, Stockholm, Sweden); Lynnette Murray (ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia); Ancuta Negru (Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania); David Nelson (Department of Physiology and Pharmacology, Section of Perioperative Medicine and Intensive Care, Karolinska Institutet, Stockholm, Sweden); Virginia Newcombe (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); József Nyirádi (János Szentágothai Research Centre, University of Pécs, Pécs, Hungary); Fabrizio Ortolano (Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy); Jean-François Payen (Department of Anesthesiology & Intensive Care, University Hospital of Grenoble, Grenoble, France); Vincent Perlbarg (Anesthesie-Réanimation, Assistance Publique—Hopitaux de Paris, Paris, France); Paolo Persona (Department of Anesthesia & Intensive Care, Azienda Ospedaliera Università di Padova, Padova, Italy); Wilco Peul (Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands); Anna Piippo-Karjalainen (Department of Neurosurgery, Helsinki University Central Hospital); Horia Ples (Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania); Inigo Pomposo (Department of Neurosurgery, Hospital of Cruces, Bilbao, Spain); Jussi P. Posti (Division of Clinical Neurosciences, Department of Neurosurgery and Turku Brain Injury Centre, Turku University Hospital and University of Turku, Turku, Finland); Louis Puybasset (Department of Anesthesiology and Critical Care, Pitié -Salpêtrière Teaching Hospital, Assistance Publique, Hôpitaux de Paris and University Pierre et Marie Curie, Paris, France); Andreea Radoi (Neurotraumatology and Neurosurgery Research Unit \(UNINN\); Vall d’Hebron Research Institute, Barcelona, Spain); Arminas Ragauskas (Department of Neurosurgery, Kaunas University of technology and Vilnius University, Vilnius, Lithuania); Rahul Raj (Department of Neurosurgery, Helsinki University Central Hospital); Jonathan Rhodes (Department of Anaesthesia, Critical Care & Pain Medicine NHS Lothian & University of Edinburg, Edinburgh, UK); Sophie Richter (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Saulius Rocka (Department of Neurosurgery, Kaunas University of technology and Vilnius University, Vilnius, Lithuania); Cecilie Roe (Department of Physical Medicine and Rehabilitation, Oslo University Hospital/University of Oslo, Oslo, Norway); Olav Roise (Division of Orthopedics, Oslo University Hospital, Oslo, Norway; Institute of Clinical Medicine, Faculty of Medicine, University of Olso, Oslo, Norway); Jeffrey V. Rosenfeld (National Trauma Research Institute, The Alfred Hospital, Monash University, Melbourne, Victoria, Australia); Christina Rosenlund (Department of Neurosurgery, Odense University Hospital, Odense, Denmark); Guy Rosenthal (Department of Neurosurgery, Hadassah-hebrew University Medical center, Jerusalem, Israel); Rolf Rossaint (Department of Anaesthesiology, University Hospital of Aachen, Aachen, Germany); Sandra Rossi (Department of Anesthesia & Intensive Care, Azienda Ospedaliera Università di Padova, Padova, Italy); Juan Sahuquillo (Neurotraumatology and Neurosurgery Research Unit \(UNINN\); Vall d’Hebron Research Institute, Barcelona, Spain); Oddrun Sandrød (Department of Anasthesiology and Intensive Care Medicine, St.Olavs Hospital, Trondheim University Hospital, Trondheim, Norway); Oliver Sakowitz (Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany; Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany); Renan Sanchez-Porras (Klinik für Neurochirurgie, Klinikum Ludwigsburg, Ludwigsburg, Germany); Charlie Sewalt (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Kari Schirmer-Mikalsen (Department of Anasthesiology and Intensive Care Medicine, St.Olavs Hospital, Trondheim University Hospital, Trondheim, Norway; Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology, NTNU, Trondheim, Norway); Rico Frederik Schou (Department of Neuroanesthesia and Neurointensive Care, Odense University Hospital, Odense, Denmark); Peter Smielewski (Brain Physics Lab, Division of Neurosurgery, Dept of Clinical Neurosciences, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Abayomi Sorinola (Department of Neurosurgery, University of Pécs, Pécs, Hungary); Emmanuel Stamatakis (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Ewout W. Steyerberg (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands; Dept. of Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, The Netherlands); Nino Stocchetti (Department of Pathophysiology and Transplantation, Milan University, and Neuroscience ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milano, Italy); Nina Sundström (Department of Radiation Sciences, Biomedical Engineering, Umeå University, Umeå, Sweden); Riikka Takala (Perioperative Services, Intensive Care Medicine and Pain Management, Turku University Hospital and University of Turku, Turku, Finland); Viktória Tamás (Department of Neurosurgery, University of Pécs, Pécs, Hungary); Tomas Tamosuitis (Department of Neurosurgery, Kaunas University of Health Sciences, Kaunas, Lithuania); Olli Tenovuo (Division of Clinical Neurosciences, Department of Neurosurgery and Turku Brain Injury Centre, Turku University Hospital and University of Turku, Turku, Finland); Matt Thomas (Intensive Care Unit, Southmead Hospital, Bristol, Bristol, UK); Dick Tibboel (Intensive Care and Department of Pediatric Surgery, Erasmus Medical Center, Sophia Children’s Hospital, Rotterdam, The Netherlands); Christos Tolias (Department of Neurosurgery, Kings college London, London, UK); Tony Trapani (ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia); Cristina Maria Tudora (Department of Neurosurgery, Emergency County Hospital Timisoara, Timisoara, Romania); Andreas Unterberg (Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany); Peter Vajkoczy (Neurologie, Neurochirurgie und Psychiatrie, Charité – Universitätsmedizin Berlin, Berlin, Germany); Shirley Vallance (ANZIC Research Centre, Monash University, Department of Epidemiology and Preventive Medicine, Melbourne, Victoria, Australia); Egils Valeinis (Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia); Zoltán Vámos (Department of Anaesthesiology and Intensive Therapy, University of Pécs, Pécs, Hungary); Mathieu van der Jagt (Department of Intensive Care Adults, Erasmus MC– University Medical Center Rotterdam, Rotterdam, the Netherlands); Gregory Van der Steen (Department of Neurosurgery, Antwerp University Hospital, Edegem, Belgium); Jeroen T.J.M. van Dijck (Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands); Thomas A. van Essen (Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands); Roel P. J. van Wijk (Dept. of Neurosurgery, Leiden University Medical Center, Leiden, The Netherlands and Dept. of Neurosurgery, Medical Center Haaglanden, The Hague, The Netherlands); Alessia Vargiolu (NeuroIntensive Care Unit, Department Neuroscience, IRCCS Fondazione San Gerardo dei Tintori, Monza, Italy); Emmanuel Vega (Department of Anesthesiology-Intensive Care, Lille University Hospital, Lille, France); Anne Vik (Department of Neuromedicine and Movement Science, Norwegian University of Science and Technology, NTNU, Trondheim, Norway; Department of Neurosurgery, St.Olavs Hospital, Trondheim University Hospital, Trondheim, Norway); Rimantas Vilcinis (Department of Neurosurgery, Kaunas University of Health Sciences, Kaunas, Lithuania); Victor Volovici (Department of Neurosurgery, Erasmus MC, Rotterdam, the Netherlands); Daphne Voormolen (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Petar Vulekovic (Department of Neurosurgery, Clinical centre of Vojvodina, Faculty of Medicine, University of Novi Sad, Novi Sad, Serbia); Eveline Wiegers (Department of Public Health, Erasmus Medical Center-University Medical Center, Rotterdam, The Netherlands); Guy Williams (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Stefan Winzeck (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK); Stefan Wolf (Department of Neurosurgery, Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Berlin, Germany); Alexander Younsi (Department of Neurosurgery, University Hospital Heidelberg, Heidelberg, Germany); Frederick A. Zeiler (Division of Anaesthesia, University of Cambridge, Addenbrooke’s Hospital, Cambridge, UK; Section of Neurosurgery, Department of Surgery, Rady Faculty of Health Sciences, University of Manitoba, Winnipeg, MB, Canada); Agate Ziverte (Neurosurgery clinic, Pauls Stradins Clinical University Hospital, Riga, Latvia); Tommaso Zoerle (Neuro ICU, Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico, Milan, Italy).
Authors’ Contributions
N.A.: Conceptualization, methodology, formal analysis, data curation, and writing—original draft preparation; D.R.: Conceptualization, methodology, formal analysis, data curation, and writing—original draft preparation; L.O.L.: Conceptualization, methodology, formal analysis, data curation, and writing—original draft preparation; writing—review and editing; M.R.: Writing—review and editing; E.I.H.: Conceptualization, resources, and writing—review and editing; L.J.: Conceptualization, resources and writing—review and editing; P.A.: Conceptualization, writing—review and editing; M.Z.: Resources and writing—review and editing; E.H.: Resources and writing—review and editing; C.T.: Resources and writing—review and editing; J.C.: Writing—review and editing; T.H.: Writing—review and editing; M.V.F.: Writing—review and editing; I.B.: Resources and writing—review and editing; I.K.: Writing—review and editing; H.L.S.: Writing—review and editing; M.L.: Writing—review and editing; S.H.: Writing—review and editing; J.L.: Writing—review and editing; S.B.B.: Writing—review and editing; O.T.: Conceptualization, resources, and writing—review and editing; N.S.: Conceptualization, writing—review and editing; C.R.: Conceptualization, resources, supervision, and writing—review and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Data used in the preparation of this article were obtained in the context of CENTER-TBI, a large collaborative project with the support of the European Union 7th Framework program (EC Grant 602150), Hannelore Kohl Stiftung (Germany), OneMind (USA) and from Integra LifeSciences Corporation (USA).
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.