
Abstract
Objectives:
This scoping review aimed to characterize the implementation of telehealth interventions in U.S. K–12 school settings, map how their performance and outcomes have been evaluated across a standardized evaluation taxonomy, and develop a conceptual framework to address gaps in evaluation practice.
Methods:
We conducted a scoping review following Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews guidelines, searching PubMed, CINAHL, Scopus, and Google Scholar for studies published between January 2019 and April 2026. Two reviewers independently screened records and extracted data on study characteristics, intervention types, and evaluation domains. Measures were classified into a standardized taxonomy and synthesized using descriptive mapping and frequency analysis. Framework development was iterative and informed by extracted findings, conceptual review, and integration of existing implementation and evaluation models, alongside policy guidance relevant to school-based telehealth (SBTH).
Results:
A total of 1,217 records were identified, with 22 studies meeting the inclusion criteria. Studies were heterogeneous across service lines and methodologies. Evaluation most frequently focused on access and utilization, satisfaction or acceptability, and implementation outcomes, while health outcomes, cost, academic outcomes, and sustainability were less consistently assessed. Evaluation approaches were fragmented, with limited use of standardized metrics and minimal integration across domains. These findings informed the development of a structured framework spanning Inputs, Implementation Processes, and Outcomes, capturing the relationships between contextual factors, service delivery, and multidimensional performance indicators.
Conclusion:
SBTH appears feasible, acceptable, and capable of improving access to care; however, fragmented evaluation practices limit comparability and policy translation. The proposed framework provides a structured approach to guide comprehensive, longitudinal evaluation and support scalable, integrated telehealth implementation in school settings.
Introduction
The COVID-19 pandemic served as a major catalyst for the rapid expansion of telehealth across the U.S. health system, supported by emergency policy actions and expanded reimbursement that lowered adoption barriers. 1 Nationally representative data indicate a sharp increase in clinician and patient utilization during the pandemic period and sustained use above pre-pandemic baseline. 2 Within K–12 educational settings, widespread disruptions to in-person school-based health service delivery prompted school-based health centers to adopt telehealth modalities to maintain continuity of care and student support services.3,4 School-based telehealth (SBTH) models can deliver a broad range of services, including, but not limited to, primary care, chronic condition monitoring, and behavioral health. 5 They can also reduce time away from class and mitigate logistical barriers such as transportation and caregiver work constraints. 6 Accumulating evidence suggests that SBTH may contribute not only to health service access but also to educationally relevant outcomes by reducing absenteeism, strengthening the rationale for SBTH as a public health and educational strategy.7–9 Beyond acute pandemic response, professional guidance and policy analyses increasingly frame SBTH as a potentially sustainable equity intervention, particularly for rural and medically underserved communities, contingent on supportive reimbursement, infrastructure, and implementation capacity.10–13
Despite growing interest in SBTH, the empirical evidence on its performance, implementation quality, and impacts remains uneven and fragmented. Prior reviews of school telehealth have noted that many programs were implemented with limited evaluation rigor and incomplete reporting of implementation determinants, such as facilities and costs, constraining the ability to draw generalizable inferences for development and sustainability.5,12,14 Moreover, the existing literature exhibits substantial heterogeneity in study designs, service lines, telehealth modalities, and the outcome domains assessed.5,12,14 Furthermore, national data and policy analyses document that the pandemic-era shift accelerated telehealth utilization and altered the operational landscape, underscoring the need for contemporary syntheses that reflect post-pandemic practice realities.2,15,16 Against this backdrop, our review departed from earlier syntheses by restricting scope to recent U.S. K–12 school-based telehealth studies and applying a unified evaluation taxonomy with quantitative mapping of domain and metric frequencies—thereby improving cross-study comparability and illuminating measurement gaps. By focusing on multiple programs within a clearly bounded class of telehealth services, U.S. K–12 SBTH, our approach aims to address a common evidence-synthesis trade-off in telehealth: overly broad reviews obscure program heterogeneity, whereas single-program evaluations limit generalizability.
Therefore, a scoping review focused on recent U.S. empirical studies was conducted to characterize how telehealth interventions had been implemented in K–12 school settings and to map outcomes and performance indicators reported across a standardized evaluation taxonomy. Our primary research question asked how telehealth interventions have been evaluated in U.S. K–12 school settings, that is, which evaluation domains, metrics, and measurement approaches are used, and how frequently each domain is reported across study designs and contexts. By synthesizing these findings, this review sought to inform educators, policymakers, and health care providers about the effectiveness and challenges of integrating telehealth into school health programs, offering insights into future practice and research.
Methods
A comprehensive scoping review was conducted on May 13, 2026, across four major databases: PubMed, CINAHL, Scopus, and Google Scholar, adhering to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines, targeting peer-reviewed studies on SBTH programs published between January 2019 and April 2026.17–21 This time frame reflects the rapid adoption of SBTH during and after the COVID-19 pandemic.3,22 The search employed Medical Subject Headings and free-text terms, including “school-based telehealth,” “digital health,” and “evaluation metrics,” along with Boolean operators to ensure comprehensive coverage (Appendix A1).
Screening and study selection
Search results were imported into Covidence, a web-based systematic review management platform. After duplicate removal, two independent reviewers applied predefined criteria to screen titles and abstracts, retrieving full texts for potentially relevant studies. 23 Discrepancies between reviewers at either stage were resolved through discussion and consensus.
Inclusion and exclusion criteria
Studies were eligible if they met all the following criteria: (1) the setting was a U.S.-based K–12 school environment, including public or private schools; (2) the intervention involved a telehealth, telemedicine, or remote consultation service delivered within the school context such as virtual consultations, teletherapy, tele-mental health services, or remote monitoring accessible to students and/or staff; (3) the evaluation focus included the reporting of defined performance metrics, evaluation indicators, or outcomes, including, but not limited to, access or utilization, cost or efficiency, health or academic outcomes, user satisfaction, and implementation measures such as fidelity or coverage; (4) the study type consisted of empirical research of any design (quantitative, qualitative, or mixed-methods), including pilot implementations, program evaluations, observational studies, or pragmatic trials; (5) the publication period fell between 2019 and 2026, inclusive; (6) the study was published in English; (7) the full text was available through institutional or open-access databases; and (8) the work was published in a peer-reviewed journal or as a formal evaluation report from a credible organization with transparent methodology and clearly described data sources. Exclusion criteria ruled out studies conducted outside the United States, those lacking defined performance indicators, or published prior to 2019.
Outcomes and data extraction
A standardized data extraction form was developed and piloted on a subset of included studies (n = 8). Following the pilot, minor refinements were made to the form including restructuring of categories to account for overlap. The following data were collected: (1) study characteristics, including author, year of publication, geographic location, school setting type, sample size, and population demographics; (2) intervention type and delivery mode, such as synchronous video consultation, asynchronous tele-mental health, remote monitoring, or teletherapy; (3) evaluation domains and specific metrics reported, including cost per student, utilization counts, return-to-class rates, absenteeism, health symptom scales, user satisfaction measures, implementation fidelity, and consent or data governance measures; (4) study design and evaluation methodology, encompassing quantitative, qualitative, or mixed-methods approaches, as well as designs such as cross-sectional, cohort, pre–post, or pilot studies; and (5) key findings corresponding to each evaluation domain.
The outcomes of this review were categorized according to the evaluation domains outlined in the PRISMA extension for Scoping Reviews guidelines. The primary outcome of interest was the distribution, frequency, and type of evaluation domains used to assess SBTH interventions in U.S. K–12 settings. 24 This review, although not centered on hypothesis testing, examined how outcomes were operationalized through reported evaluation domains and measurement metrics in existing studies. Primary outcomes included indicators such as service uptake, utilization volume, follow-up completion, and measures of reach to targeted populations.
In addition, we assessed secondary outcomes pertaining to health indicators, academic outcomes (e.g., absenteeism, return-to-class rates), efficiency and cost (e.g., cost per student or avoided external care expenses), satisfaction/experience, and implementation.
Outcome measures were classified into predefined domains during data extraction and used to organize synthesis in the results. Quantitative and qualitative measures were captured, including validated instruments as reported by the original studies, along with descriptive measurements when available and applicable.
Methodological quality was assessed using the Mixed Methods Appraisal Tool (MMAT), version 2018. 25 The MMAT was selected because the included evidence comprised diverse study designs, including qualitative studies, randomized trials, nonrandomized studies, quantitative descriptive studies, and mixed-methods studies. For each included study, two reviewers first applied the MMAT screening questions and then selected the appropriate MMAT study design category. Each study was appraised using the five criteria corresponding to its design category. Disagreements were resolved through discussion. Studies were not excluded based on MMAT results; rather, appraisal findings were used to contextualize the strength and limitations of the evidence.
Data analysis, synthesis, and framework development
Data analysis utilized qualitative thematic synthesis and frequency counts of evaluation domains, revealing insights into the operationalization of outcomes across the studies examined. The process aimed at identifying fragmented areas as well as commonalities and gaps in the telehealth evaluation literature. To create the framework, we conducted a conceptual review of the data extracted. Framework development was iterative and collaborative. The research team reviewed existing implementation and evaluation models and identified key constructs related to telehealth evaluation. These elements were progressively synthesized into an integrated conceptual structure. 26 The framework was informed by the policy updates from the U.S. Department of Health and Human Services and 2023 U.S. Centers for Medicare & Medicaid Services, in consultation with the U.S. Department of Education “Guidance on Medicaid and Children’s Health Insurance Program Services in School-Based Settings” further refined through discussions and revisions.16,27 Constructs were reorganized and expanded to capture the relationships between input, implementation processes, and outcome domains relevant to SBTH programs. This process drew insights from both academic and policy literature related to telehealth service delivery in school settings.
Results
After duplicate removal and two-stage screening of titles, abstracts, and full texts, 22 out of 1,217 literature records matched all inclusion criteria (Fig. 1).
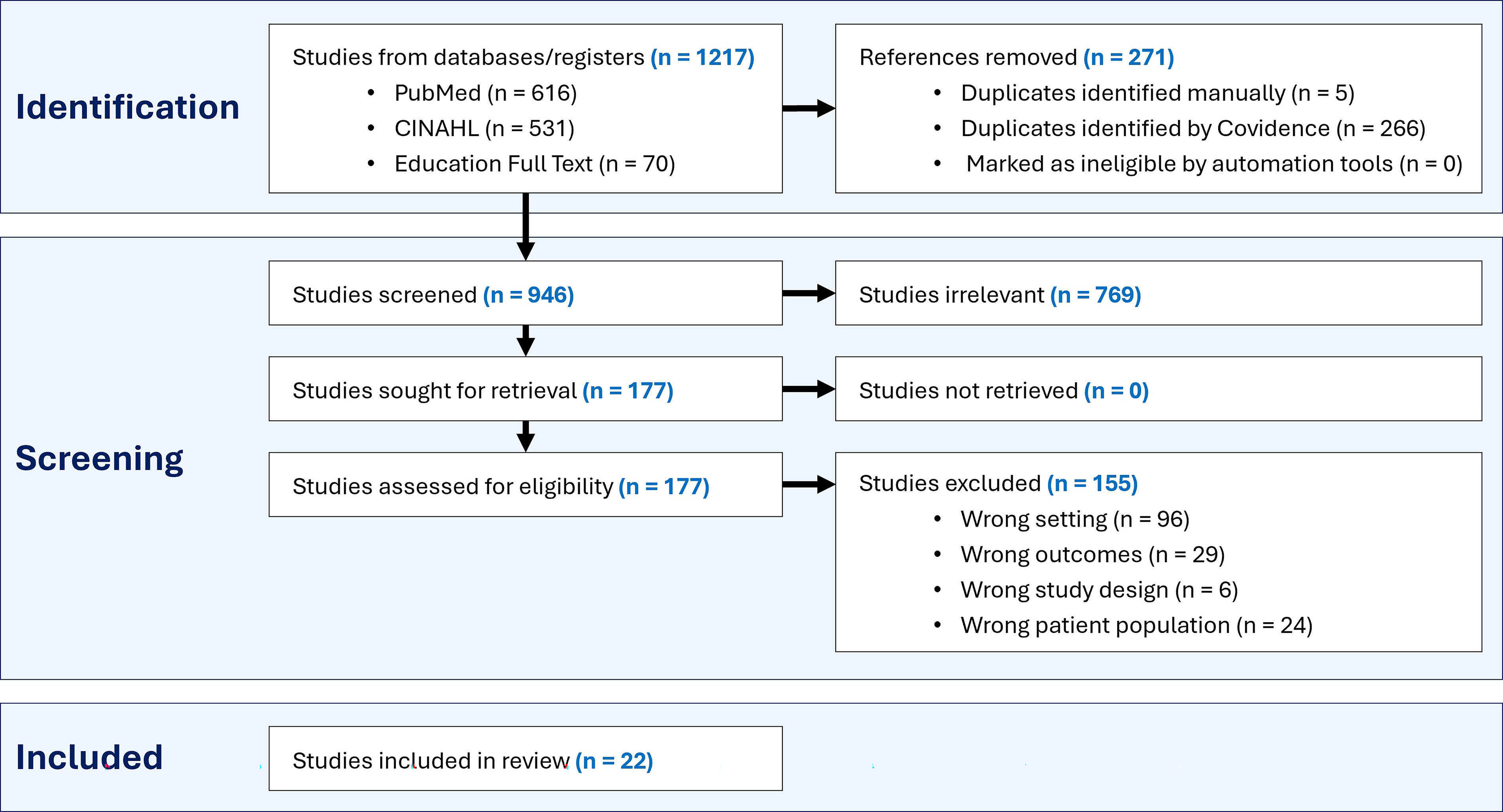
Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews diagram.
These publications, spanning from 2019 to 2026, reflect a period of rapid evolution in the U.S. K–12 telehealth landscape, shifting from emergency pandemic response to formalized, integrated models of care. The evidence base is geographically diverse, covering over 20 states, and methodologically varied, including quantitative randomized controlled trials (n = 3), quantitative nonrandomized studies (n = 2), quantitative descriptive studies (n = 6), qualitative studies (n = 5), and mixed-methods studies (n = 6). Methodological quality varied from high (n = 8), moderate-to-high (n = 3), moderate (n = 7), low-to-moderate (n = 2), and low (n = 2). The most common limitations were small participant or site samples, lack of comparison groups, limited representativeness, and incomplete reporting of measurement validity or qualitative rigor. The full MMAT table is presented in Appendix A3.
The search identified diverse U.S. empirical studies between 2019 and 2026 on K–12 school-based telehealth interventions, spanning over 20 states and a range of urban, suburban, rural, and underserved populations. Methodologies varied from qualitative interviews and cross-sectional surveys to randomized controlled trials.
Evaluation domains reported
Across studies, evaluation focused on multiple domains, although reporting was uneven. Evaluation focused primarily on access, utilization, and satisfaction. Rigorous assessment of health outcomes, cost-efficiency, and academic impact was less common, with minimal data reported on long-term sustainability or program reach. Table 1 depicts the characteristics of reviewed articles, and more detailed information is presented in Appendix A2.
Overview of Included Studies and Key Findings

BP, blood pressure; ECHO, Extension for Community Healthcare Outcomes; ED, emergency department; SBHCs, school-based health centers; VR, virtual reality.
Access and utilization
Consistently reported findings included improved care access. Telehealth in school settings increased service reach or follow-up, especially in rural or high-need populations. A key example is Alaska’s telemedicine hearing screenings, which achieved significantly higher 9-month follow-up rates (68.5%) than standard primary care referral communities (32.1%; 95% confidence interval: 6.8–45.3; p = 0.002).28,29 Although not quantified or statistically tested, descriptive program evaluations of school-based telepsychiatry reported reduced perceived wait times. 36
National and multisite studies highlighted telehealth’s role in service expansion. School-Based Health Alliance Census shows telehealth adoption among U.S. school-based health centers increased from 7% to 19% between 2007 and 2017, led by rural and hospital-sponsored sites. 47 During and after the COVID-19 pandemic, qualitative studies demonstrated that telehealth ensured continuity of care during school closures and transitions back to hybrid in-person models.31,33,37
Health and functional outcomes
While fewer studies evaluated clinical effectiveness, results were generally favorable. School-based telemedicine reduced systolic blood pressure in hypertensive adolescents, and integrated models—combining video visits with remote monitoring—improved asthma management for low-income and underserved students.30,37,42,43 In the Telemedicine Enhanced Asthma Management–Uniting Providers (TEAM-UP) randomized clinical trial, adding telemedicine consultations with asthma specialists to school-based directly observed therapy significantly increased symptom-free days and reduced asthma-related emergency department or hospital visits and school absenteeism compared with enhanced usual care. 43 These asthma programs also demonstrated potential efficiency benefits, with prior economic modeling estimating program cost of approximately $344 per child annually, often offset by reduced emergency department visits and absenteeism.30,37,42 Functional outcomes for occupational therapy and speech-language pathology were comparable to in-person care when interventions were tailored to school contexts and providers received specific training.38,39,41 National surveys found that 80% of occupational therapy practitioners would use telehealth after training, despite 89% having no experience, highlighting the importance of workforce preparation in achieving equivalent functional outcomes.38,48 These studies suggest that structured, condition-specific, integrated SBTH can improve clinical management and access.
Satisfaction and acceptability
Although satisfaction measurement approaches varied widely, high levels of satisfaction and acceptability were commonly reported among students, families, clinicians, and school staff. Tele-mental health, behavioral parent training, and telementoring models were well-received and useful.34,35,44,45 These findings support SBTH reports during the COVID-19 pandemic, which found that individual tele-mental health encounters were acceptable and useful for maintaining continuity of care, especially when in-person services were disrupted. 7
Caregivers and workers also accepted interventions well. A study on telehealth behavioral parent training for Attention-Deficit/Hyperactivity Disorder (ADHD) found high usability and acceptability among parents (System Usability Scale score >68), sustained engagement (mean session attendance = 94.6%), and clinically meaningful symptom improvement (ω2 = 0.36). 35 In a national mixed-methods evaluation of Project ECHO (Extension for Community Healthcare Outcomes) telementoring for school personnel supporting return-to-learn after mild traumatic brain injury, 97% of participants were satisfied, and knowledge scores increased from 44.8% pre-training to 86.9% post-training, demonstrating the acceptability of tele-education models for distributed school-based teams. 44
A pre–post feasibility study of a school-based virtual reality (VR) exercise program for mobility-impaired students found 83% attendance compared with 27% at home. VR-based activity was popular with students, suggesting that on-site facilitation is crucial to engagement. 46
Acceptance was not universal. A cross-sectional survey of occupational therapy and speech-language pathology clinicians during the COVID-19 pandemic found that telehealth utilization increased sharply (from 8.3% pre-pandemic to 62.5%), but 40% remained concerned that virtual care was not equivalent to in-person services, citing insufficient training (49%) and limited technology access (45%). 39
Many qualitative studies raised concerns about privacy, stigma, and the perceived equivalence of virtual and in-person services, especially for social-emotional or group-based interventions.7,34,47 Children preferred text-based communication, while caregivers preferred phone or video communication in some situations. 37
Implementation, feasibility, and infrastructure
Challenges primarily involved workflow integration, technology access, and workforce readiness. Key barriers to sustainability included a lack of electronic medical record integration, time-intensive setup, and school schedule disruptions. 24 Training emerged as a critical feasibility determinant, particularly for therapy providers with minimal pre-pandemic telehealth experience.35,38,39,41,44,45 Success consistently depended on on-site champions, administrative support, and clear protocols for consent, privacy, and data governance.27,36
Efficiency, cost, and sustainability
Only a small number of studies formally evaluated cost or efficiency outcomes. Where reported, findings suggested that SBTH could be financially viable under real-world conditions. Economic modeling of asthma telemedicine programs indicated that operating costs could be offset by reductions in emergency department utilization and school absenteeism.24,37,42
Summary of evidence gaps
Overall, the evidence base demonstrates that SBTH is feasible, acceptable, and capable of improving access to services across diverse settings. However, the review revealed substantial fragmentation in evaluation approaches, limited use of standardized metrics, and a relative scarcity of studies assessing long-term outcomes, costs, equity impacts, and sustainability. These gaps constrain cross-study comparison and underscore the need for more rigorous and comprehensive evaluation frameworks.
Introducing the conceptual framework for evaluating school-based telehealth programs
SBTH programs operate within complex health care, educational, and policy environments that influence how services are implemented and how outcomes are realized. Building on findings from our scoping review and informed by existing implementation science models, we developed a conceptual framework (Fig. 2). 49
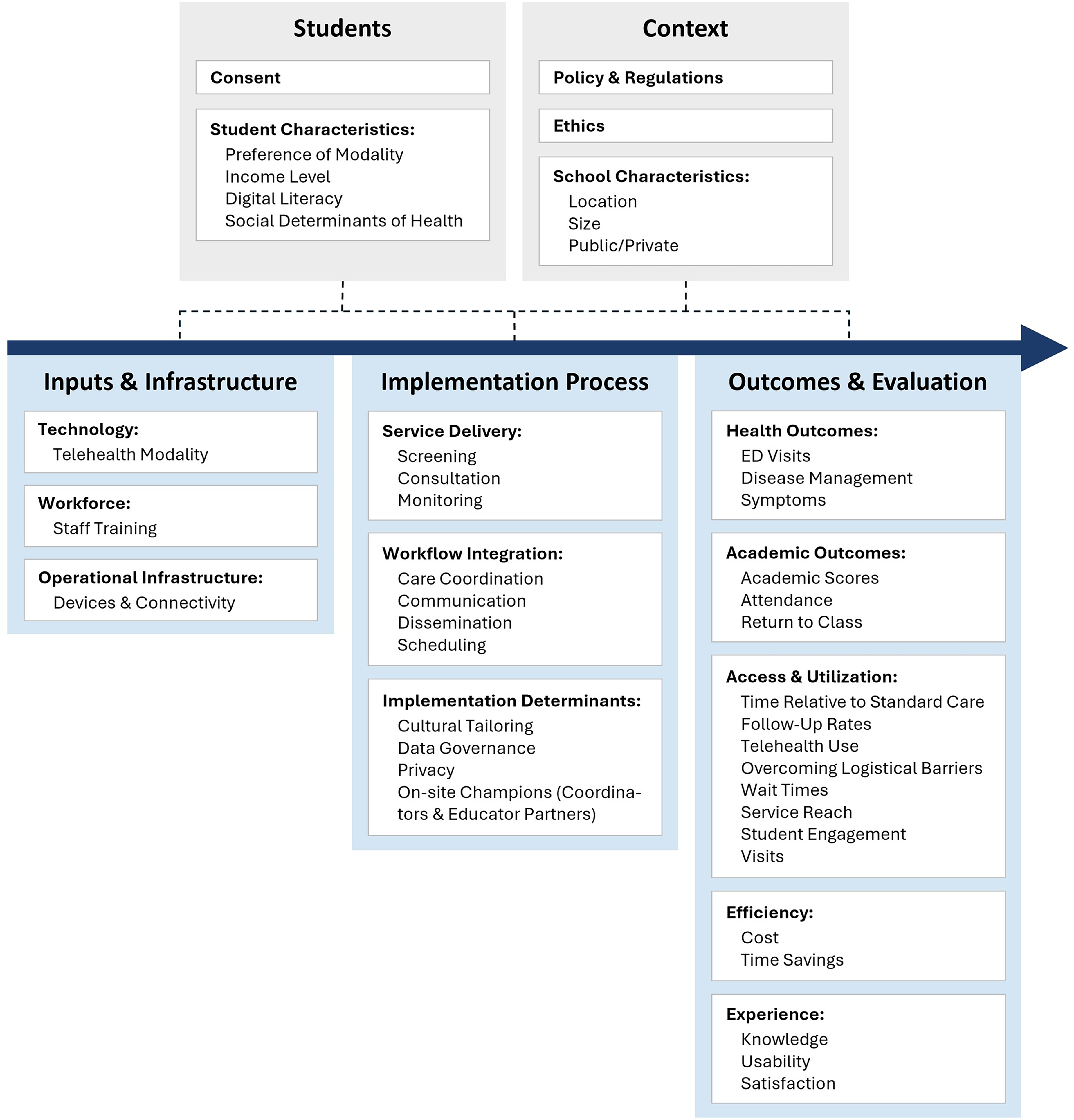
Conceptual framework for evaluating school-based telehealth programs.
The framework synthesizes key domains identified across the literature and organizes them into an integrated structure that captures the relationships between (1) program inputs, (2) implementation processes, and (3) multidimensional outcome domains. The upper portion of the framework captures student-level and contextual factors. At the student level, participation in SBTH is mediated by consent processes and individual characteristics, including modality preference, income level, digital literacy, and broader social determinants of health. These characteristics influence both the feasibility of telehealth engagement and the likelihood that students will benefit from remote health care services.
In parallel, the framework highlights the broader contextual environment in which SBTH programs operate. Policy and regulatory structures shape reimbursement mechanisms, program eligibility, and operational constraints, while ethical considerations, such as privacy protections and responsible data use, govern how telehealth services are delivered within school settings. Institutional characteristics of schools further contribute to this context. Factors such as geographic location, school size, and whether a school is public or private can influence resource availability, infrastructure capacity, and the organization of school health services.
Together, these contextual and student-level elements create the structural conditions that influence program design, implementation feasibility, and eventual outcomes; therefore must be considered when evaluating integrated SBTH initiatives. By situating these domains within a broader implementation context, the framework provides a structured approach for understanding how telehealth interventions translate into measurable outcomes in school settings. In the sections that follow, we describe the individual components of the framework and discuss implications for SBTH evaluation, implementation, and policy translation.
Discussion
The findings demonstrate that SBTH offers meaningful benefits across multiple domains, with persistent challenges related to evaluation rigor and implementation consistency. In parallel, studies often assessed isolated components of SBTH programs without capturing the full continuum from infrastructure readiness to service delivery and downstream impact. In contrast to the emerging data that supports value addition through integrated SBTH, the review revealed substantial fragmentation in evaluation practices.
Additionally, key implementation domains including feasibility, fidelity, training uptake, workflow integration (e.g., between teachers, school nurses, parents, and telehealth providers), and data governance were among the least frequently assessed metrics. Consent and data governance, in particular, were rarely operationalized as measurable performance indicators despite their critical relevance. The capacity of SBTH programs to systematically monitor compliance with federal and state regulations is essential for effective integration. Additionally, from an implementation lens, the absence of standardized, measurable governance indicators constrains adoption, erodes stakeholder trust—particularly among parents and school systems—, and may limit reimbursement eligibility.
To address the gaps identified in this scoping review, our proposed structured SBTH evaluation framework spans across three core domains: Inputs, Implementation, and Outcomes.
Within the “Implementation Process” domain, our review highlights the growing role of SBTH screening tools as entry points to care rather than stand-alone interventions, emphasizing the importance of approaches that integrate telehealth approaches with traditional in-person health care services rather than serving as a stand-alone or substitutive telehealth service. Across diverse settings, digital screening and education platforms demonstrated the feasibility of embedding health identification and triage processes directly into existing school workflows, aligning closely with “Workflow Integration” components such as care coordination, communication, and scheduling. 50 This integration reduces traditional barriers to early detection and referral. 50
Notably, the observed variability in uptake across screening components underscores that engagement is not ubiquitous; this can be interpreted through the “Students domain (Student Characteristics).” This reveals an important design opportunity: multicomponent and human-centered digital interventions allow students to engage with care through modalities that correspond to their social determinants of health, preferences, digital literacy, and perceived privacy.
Moreover, the effectiveness of integrated SBTH was evident in its capacity to provide accessible and timely care without requiring students to leave school premises, directly linking “Implementation Process” with “Outcomes and Evaluation” components. This was further reflected in a study using qualitative interviews with school-based health center coordinators and educator partners in Oregon, which found that telehealth utilization increased during school closures, although experiences were mixed. 34
From a systems perspective, these findings highlight the interaction between the “Context” domain and “Implementation Process.” The success of SBTH screening efforts suggests a turning point in how schools can function as facilitators to preventive and specialty care in an integrated model, particularly for conditions that are historically under-identified or lost to follow-up. 47 By offering telehealth-enabled screening within familiar educational environments, protocols can create opportunities for early detection, streamlined referral, and reduced disparity in treatment, especially in rural and underserved communities. This also aligns with both social determinants of health and broader “contextual factors” (location, policy, and ethics).
Moreover, our review found that successful telehealth screening and referral programs in schools depended heavily on identifying on-site champions. 36 These findings align closely with the conceptual model of innovation champions, which positions champions as key actors who support implementation fidelity. 51 In SBTH settings, individuals such as school nurses or telehealth coordinators function as these champions. This convergence between empirical findings and implementation theory informed our decision to integrate champions within our framework.
Within the “Outcomes and Evaluation” domain, access and utilization were the most frequently evaluated. Common indicators included encounter volume, visit completion rates, repeat utilization, and reductions in time away from class. These findings support the idea that integrated telehealth can mitigate the logistical barriers associated with traditional in-person care, particularly those related to transportation, caregiver availability, and appointment wait times, which are persistent challenges for school-age populations.44,52 For families, this may ameliorate the burden associated with navigating complex health systems, while for schools, they offer a scalable mechanism to support students’ well-being without requiring substantial resources.31,33
Together, these findings position telehealth-enabled screening within an integrated model not merely as a technological alternative to in-person assessment but as an overhaul of access, with the potential to promote preventive care, strengthen school-health system integration, and foster equitable engagement across student populations, without losing the benefits of in-person services when necessary and warranted in a given clinical scenario.
Efficiency and cost outcomes, mapped to the “Outcomes and Evaluation” domain, further strengthen the case for SBTH as a potentially resource-saving model. Although few studies conducted structured cost analyses, reported indicators consistently pointed toward indirect cost savings, including avoided emergency department visits, reduced transportation expenses, and estimated caregiver productivity gains from minimized work absences. Broader telehealth literature highlighted economic efficiencies driven primarily by reduced nonmedical costs rather than direct reductions in clinical service expenses.53,54 Accordingly, cost was explicitly included as a core component of our framework, to ensure that future evaluations systematically capture both direct and indirect economic impacts. However, the absence of standardized economic analyses limits cross-study comparability and constrains assessment of cost-effectiveness relative to traditional care models. Likewise, health outcomes associated with SBTH were generally favorable but inconsistently measured. Most studies relied on descriptive or program-specific outcome measures rather than validated clinical instruments. This heterogeneity in outcome selection informed our “Outcomes and Evaluation” domain of the conceptual framework, in an effort to enhance reproducibility and enable robust assessment of the magnitude and durability of health impacts attributable to SBTH.7,35,46,55 Academic outcomes, although less frequently assessed, provide an important bridge between health service delivery and educational performance. Few studies extended evaluation to broader academic performance metrics, such as standardized test scores or long-term attendance trajectories. The limited scope and short follow-up periods of these assessments highlight a critical gap in understanding how health service innovations translate into sustained educational benefits. Therefore, academic outcomes were included in our framework to capture the full value proposition of integrated SBTH.
Patient, caregiver, and provider satisfaction with SBTH was generally positive, with high acceptability reported across the limited number of studies that assessed experience-related outcomes. A national survey cited improved practice efficiency and expanded access as key perceived benefits.28,29,33,42 However, satisfaction and acceptability were infrequently measured, and reporting often lacked detail on response rates, subgroup variation, or longitudinal trends, limiting interpretability and generalizability. In response to this, we explicitly incorporated satisfaction and acceptability within “Outcomes and Evaluation” to enable cross-study inference and drive policy translation.
The proposed framework therefore has important implications for research. Observational studies guided by this framework should collect data across multiple domains of program performance. Because SBTH programs operate within complex socio-technical systems, observational research should incorporate contextual variables such as school characteristics, digital infrastructure, and policy ecosystems. Longitudinal study designs may be of particular importance for evaluating SBTH programs, as many outcomes including health status, service utilization patterns, and academic outcomes can evolve over time. Repeated measures across academic terms or school years may help identify when telehealth interventions produce measurable impacts across cohorts. While challenging, researchers should consider it for SBTH evaluation studies and providers should allow ready access to their data to allow translational research.
Finally, the framework has direct implications for integrated SBTH program implementation. This aligns with federal guidance on telehealth policy and national telehealth planning strategies that require alignment between clinical services, school infrastructure, and reimbursement structures such as Medicaid coverage and administrative claiming mechanisms.11,27
Limitations
This scoping review demonstrates promising evidence for the use of telehealth in delivering health services within K–12 school settings; however, several limitations should be considered when interpreting the findings. First, the substantial heterogeneity in study designs, telehealth modalities, service lines, and evaluation metrics poses a challenge for direct comparison across studies. The wide variation in how core domains such as access, cost, health outcomes, and satisfaction were operationalized limits the ability to draw definitive conclusions regarding relative program effectiveness.
Second, many included studies (n = 7) relied on descriptive or self-reported outcome measures, which may introduce reporting and response biases. The infrequent use of validated clinical instruments and standardized satisfaction tools further constrains the reliability and comparability of reported outcomes. Additionally, most studies focused on short-term or pilot-phase outcomes, which may not fully capture the long-term clinical, educational, or economic impacts of SBTH interventions.
Third, small sample sizes and nonrandomized recruitment methods, such as volunteer-based participation or convenience sampling at the school or district level, may limit generalizability. The extent to which findings can be extrapolated to diverse geographic regions, school types, and student populations, particularly those with varying socioeconomic conditions or technology access, remains uncertain.
Last, this review was limited to U.S.-based studies published between 2019 and 2026, which, while appropriate for capturing pandemic-era and post-pandemic practice realities, may exclude relevant insights from earlier implementation efforts or international models. The reliance on peer-reviewed and formal evaluation reports may also have resulted in publication bias, as unsuccessful or underperforming programs are less likely to be reported.
Recommendations
Future research should aim to address the identified limitations to enhance the rigor, comparability, and policy relevance of integrated SBTH evaluations. In addition, future reviews should explicitly extract and report whether telehealth services are implemented as integrated components of existing school health systems or as stand-alone programs, as this distinction may substantially influence implementation processes, outcomes, and sustainability.
Second, future evaluations should incorporate formal economic analyses, including willingness-to-pay, cost-effectiveness, and cost-utility studies that link telehealth interventions to standardized health and educational outcome measures. These analyses should account not only for direct service costs but also for indirect costs and savings, such as human capital opportunity costs, documentation time, technology maintenance and depreciation, and infrastructure investments.
Greater attention should be given to the systematic measurement of workflow integration, staff training, protocol adherence, adaptation processes, and data governance practices would yield actionable insights into how integrated telehealth programs can be scaled sustainably and ethically within complex school health ecosystems.
Conclusion
Despite ongoing challenges related to technological infrastructure, evaluation fragmentation, and inconsistent measurement practices, SBTH emerges as a promising and adaptable model for delivering accessible, efficient, and student-centered health services within K–12 settings. The reviewed evidence suggests meaningful benefits including access to care, reduced time away from class, indirect cost savings, favorable health outcomes, and high user satisfaction. The current evidence base is constrained by heterogeneity in study designs, limited use of validated instruments, and insufficient attention to implementation fidelity and data governance.
Although this heterogeneity provides challenges for researchers, future research must move toward standardized evaluation frameworks, robust economic analyses, and long-term outcome assessments. Strengthening the methodological rigor and consistency of telehealth evaluations will be essential for informing policy decisions, securing reimbursement support, and guiding scalable implementation strategies. Our hope is that this framework will help generate research and evidence-informed interventions to improve integrated SBTH implementation and sustainment.
Ethical Considerations
This scoping review involved analysis of publicly available, de-identified data from published literature only. No human participants or private data were collected; thus, institutional review board approval was not required.
Footnotes
Acknowledgments
The authors gratefully acknowledge “J.C.,” Clinical Nursing Librarian at the Health Sciences Library, University of North Carolina at Chapel Hill, for her assistance in designing the search strategy for this review.
Author Disclosure Statement
The authors declare they have no conflicts of interest.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.