
Abstract
Background
Children with cancer are at increased risk for cognitive and physical suffering from side effects of treatment and disease sequelae. Animal-assisted interactions (AAIs) with canine therapy show strong promise to improve physical and psychosocial outcomes for children newly diagnosed with cancer. Few rigorous studies have focused on the role of AAI for children with relapsed/refractory cancer. The purpose of this study was to evaluate the preliminary efficacy of a randomized controlled trial (RCT) using AAI with children diagnosed with relapsed/refractory cancer for the outcome of health-related quality of life (HRQoL).
Method
This study was a component of a larger mixed-methods RCT in which 30 children (ages 3–17 years) with relapsed/refractory cancer and their caregivers were randomized to receive weekly AAI sessions with a dog and handler or usual care (UC) for 12 weeks during each child's visit to a hospital-based pediatric cancer center.
Results
Mother and child dyads (N = 21) completed the PedsQL 3.0 Cancer Module at both baseline and 12 weeks (nine UC, 12 AAI) required for analyses. None of the changes over time were statistically significant (p > .05); the strongest effects were observed on communication and procedural anxiety.
Discussion
While results were not statistically significant, they suggest AAI demonstrates potential for enhanced HRQoL for children with relapsed/refractory cancer. More research is needed with larger samples and may necessitate the use of a measure designed to capture issues particularly relevant to children with advanced disease.
Introduction
An estimated 500,000 children and adolescents cope with a life-threatening condition (LTC) in the United States (Connor et al., 2017; International Children's Palliative Care Network, 2022). Of the thousands of children and adolescents with an LTC, more than 40,000 undergo cancer treatment at any given time in the United States, with an estimated 14,910 new diagnoses made each year (National Cancer Institute, 2024). Despite gains in survival rates, cancer remains the leading cause of death by disease among children in the United States (National Cancer Institute, 2024). Children with cancer are at increased risk for cognitive and physical suffering, as they often endure debilitating pain and complex symptoms resulting from side effects of treatment, disease sequelae, long-term hospitalization, and isolation (Barrera et al., 2020; Duran et al., 2020; Linder & Hooke, 2019; Momani et al., 2016; Pan et al., 2017; Steineck et al., 2019; Varni et al., 2002). The complexity of these factors compounds the already difficult task children face in effectively coping with their disease, and indicates a continued need for novel and rigorous research focused on mitigating physical distress and improving the health-related quality of life (HRQoL) for pediatric patients with cancer, particularly those with relapsed/refractory cancer.
Animal-assisted interaction (AAI) with canine therapy provides numerous benefits for children newly diagnosed with cancer, such as relaxation and reduced anxiety, exercise or opportunities for positive play, decreased blood pressure and heart rate (markers for anxiety and stress), distraction from pain or worry, unconditional support and acceptance, increased sensory stimulation and opportunities for physical touch, improved social skills that lead to healthy relationships with others, enhanced senses of self-esteem and confidence, and increased motivation to actively participate in the healing process (Chubak et al., 2017; Jennings et al., 2021; McCullough et al., 2017; Silva & Osorio, 2018; Urbanski & Lazenby, 2012). While these findings support the benefits of AAI for youth newly diagnosed with cancer, few rigorous studies have focused on the role of AAI for children with relapsed/refractory cancer. Further research is necessary to determine optimal session protocol, ideal safety standards, and settings in which exposure to animals would be most beneficial to children and adolescents with relapsed/refractory cancer. A conceptual framework, Parent–Child Well-Being Over Time, was designed by some of the authors to illustrate the potential for AAI to promote child and parental well-being during the childhood cancer experience (Figure 1).
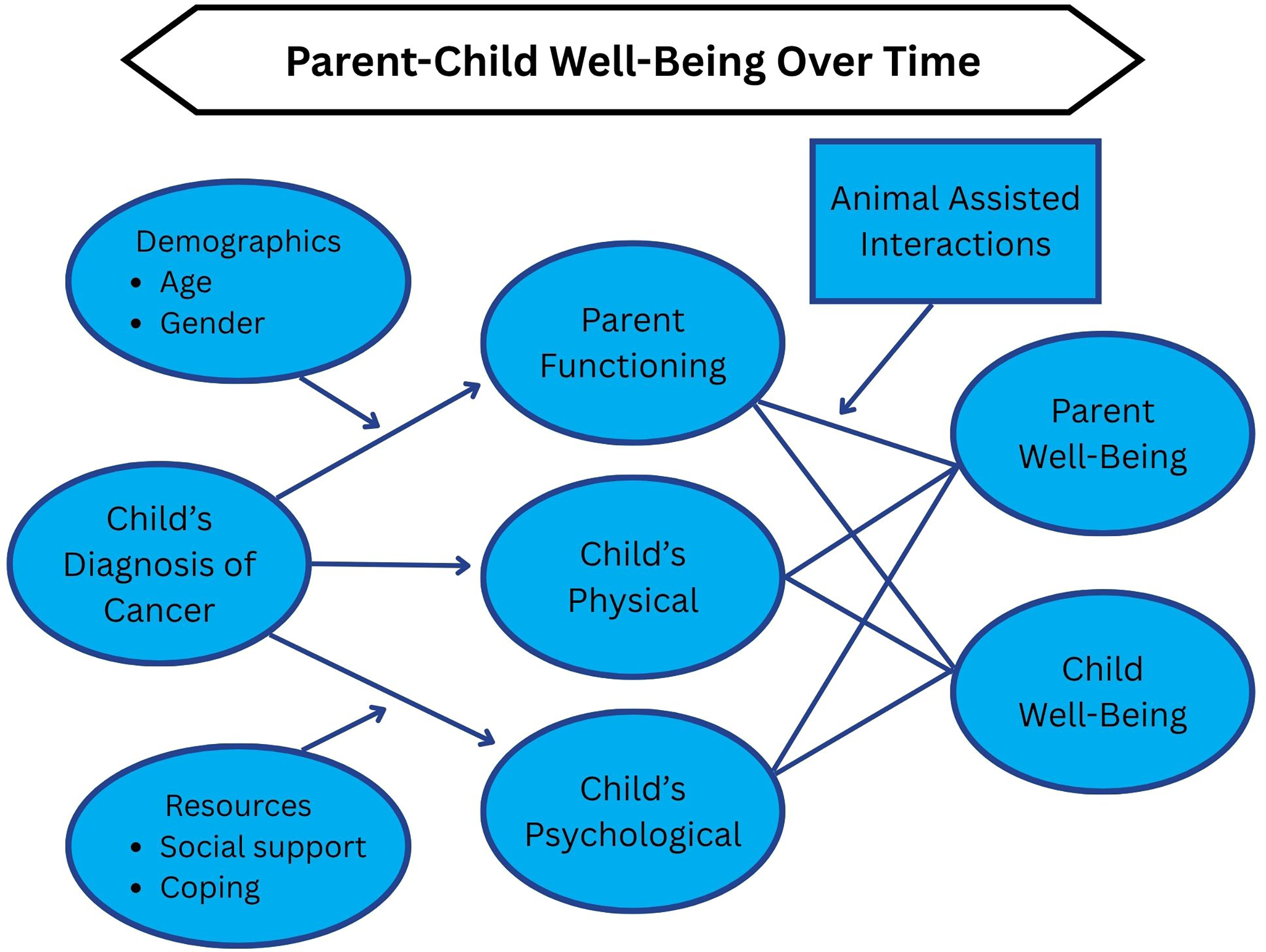
Conceptual Framework: Parent–Child Well-Being Over Time.
The focus of this study is on the preliminary efficacy of AAI sessions for the outcomes of HRQoL. We hypothesized that, compared to usual care (UC), children with relapsed/refractory cancer who receive AAI will have improved HRQoL throughout the course of the study period compared to patients who do not receive AAI.
Method
Design
This study was a component of a larger mixed-methods randomized controlled trial (RCT) conducted at a single institution in the southeastern United States that included children (ages 3–17 years) with relapsed/refractory cancer and their caregivers. Participants were randomized to receive weekly AAI sessions with a dog and handler or to UC for 12 weeks during each child's visit to a large hospital-based pediatric cancer center in the southeastern United States.
This study reports quantitative HRQoL findings from the Pediatric Quality of Life Inventory (PedsQL™) Cancer Module. An important outcome in pediatric cancer treatment is HRQoL, arguably the most important outcome during and following cancer treatment (Varni & Limbers, 2009). HRQoL is defined as the impact of disease and its treatment on the patient's self-perceptions of functioning in a variety of domains (Varni et al., 1998). The PedsQL Cancer Module was developed as the result of an extensive iterative process beginning in the mid-1990s and has been widely used as an HRQoL outcome measure in pediatric cancer research, clinical trials, and clinical practice. It was developed as a problem-focused conceptual model to measure HRQoL with a goal to guide biomedical and biobehavioral treatment interventions. The PedsQL Cancer Module is multidimensional and includes physical functioning and the psychosocial dimensions of emotional, social, and role functioning. It measures HRQoL using child self-reports and parent-proxy reports, with instruments for all age groups, beginning with parent-proxy only for ages 2–4 years. The number of items for different age groups differs slightly, but for children 8 years and older, the measure consists of 27 items and eight scales: Pain and Hurt (two items), Nausea (five items), Procedural Anxiety (three items), Treatment Anxiety (three items), Worry (three items), Cognitive Problems (five items), Perceived Physical Appearance (three items), and Communication (three items). It is scored on a 5-point scale: 0 (never), 1 (almost never), 2 (sometimes), 3 (often), and 4 (almost always). Items are reverse-scored and linearly transformed to a 0–100 scale (0 = 100); higher scores indicate better HRQoL.
Participants
This study was approved by the institutional review board, the Scientific Review Committee, and the Animal Care and Use Committee. After trained research assistants obtained informed consents and assents from all participants meeting the study inclusion/exclusion criteria, participants were randomized (1:1) via the use of a computer-generated, permuted block program to either the AAI group or the UC group.
For this study, inclusion criteria for children were (a) ages of 5–17 years, (b) diagnosed with advanced cancer as defined by any stage of relapsed or refractory cancer in their medical record, and (c) able to understand English to complete consents, AAI, and surveys. Inclusion criteria for caregivers were (a) primary caregiver as determined by the parent who brings the child to >50% of their clinic visits and (b) able to understand English to complete consents, AAI, and surveys. Exclusion criteria for both children and caregivers included a cognitive impairment as documented by the healthcare team or a reported fear of or allergies to canines. In this study, all participating primary caregivers were mothers. No significant differences were observed between the characteristics of the participants randomized to the two study groups (p > .30). Child demographics are presented in Table 1; mother demographics are found in Table 2.
Demographic Characteristics of Child With Cancer by Study Group (N = 21)
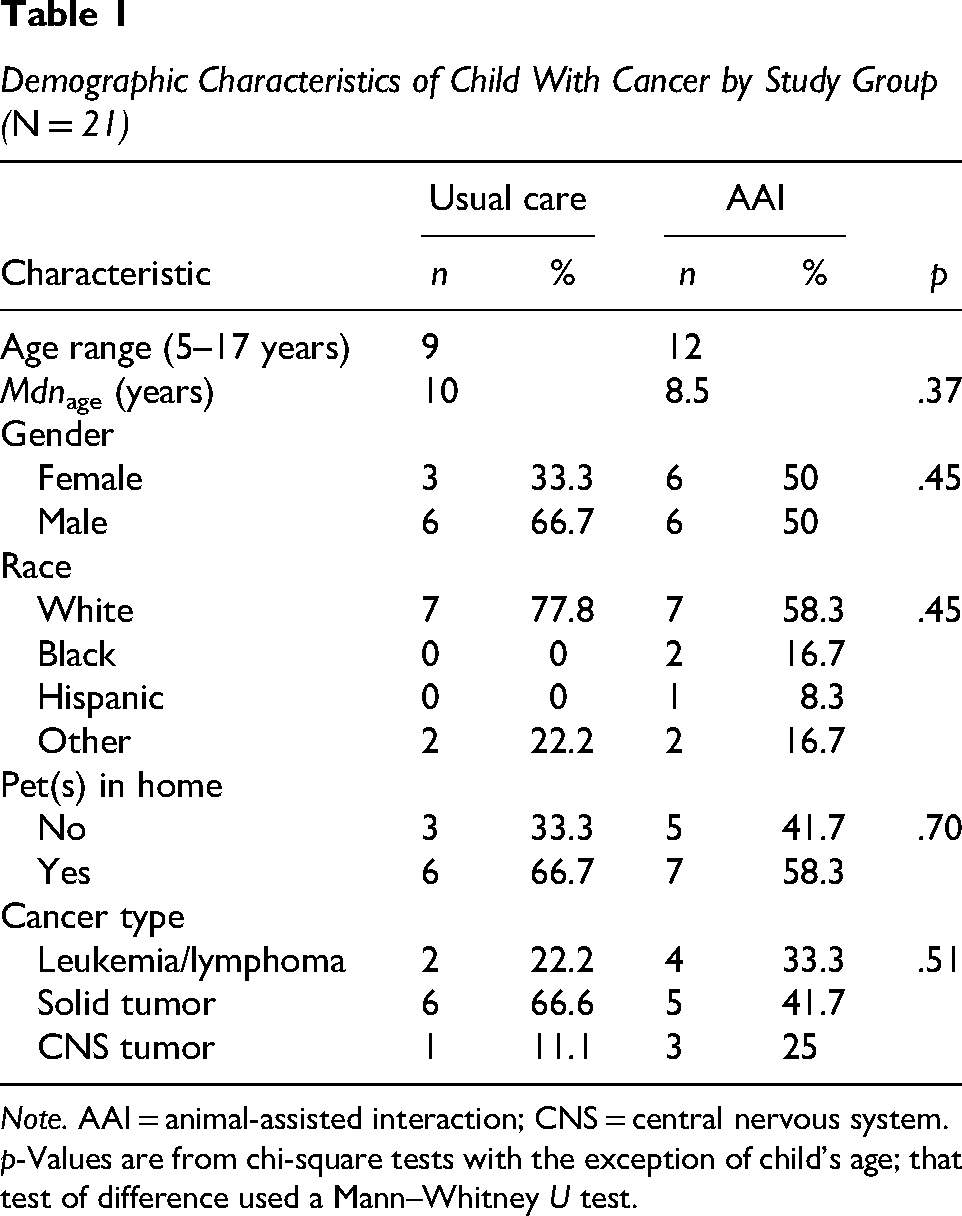
Note. AAI = animal-assisted interaction; CNS = central nervous system.
p-Values are from chi-square tests with the exception of child's age; that test of difference used a Mann–Whitney U test.
Demographic Characteristics of Mothers by Study Group (N = 21)
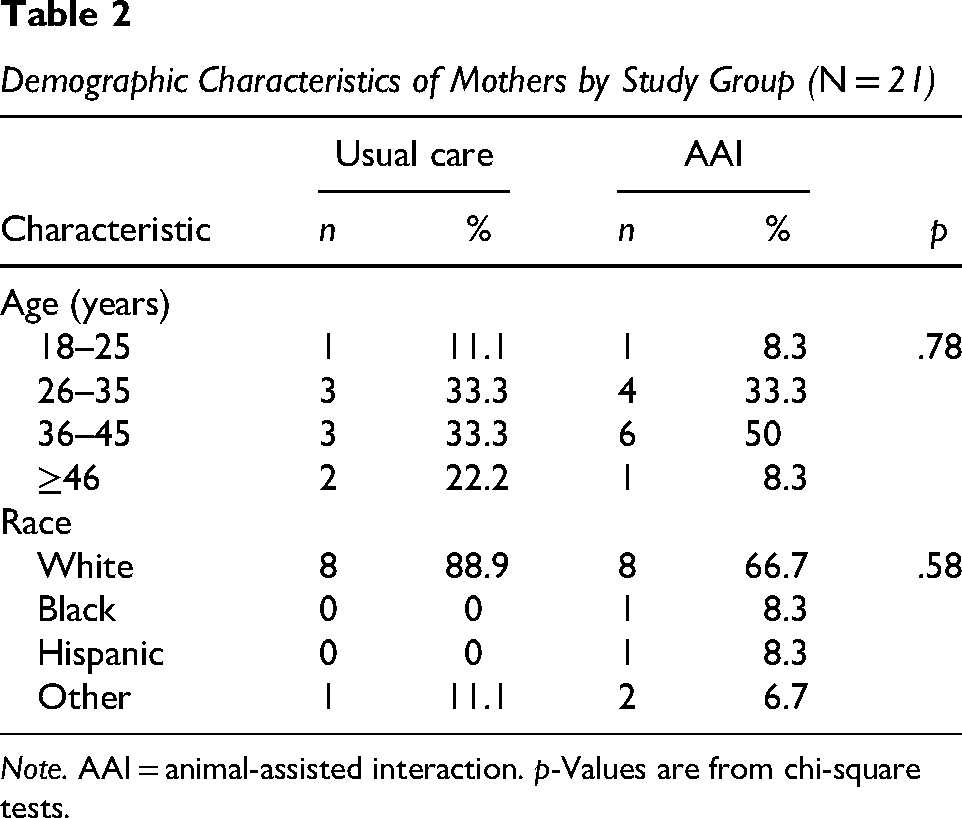
Note. AAI = animal-assisted interaction. p-Values are from chi-square tests.
AAIs Versus UC
AAIs consisted of a registered handler/canine team who spent approximately 15 min with the treatment group during each child's potentially anxiety-provoking visits to the hospital or clinic. At each visit, participants chose activities to engage in with the dog, such as having the dog do tricks, talking to the dog, petting the dog, and/or feeding treats to the dog. The AAI group continued to receive access to UC in addition to AAI.
Children in the UC group were exposed to the same conditions without the intensive dog therapy intervention during the study. UC, or typical treatment for oncology patients in this children's hospital, consists of play therapy facilitated by child life, social work interventions, physical therapy, pastoral care visits, and sessions with child psychologists as needed.
Data Collection
Data collection took place between February 2019 and June 2021, primarily during the COVID-19 pandemic. All study activities, including procedures and data collection, occurred in a private room in a large hospital-based pediatric cancer center in the southeastern United States during each clinic visit or during hospitalization. Sessions coincided with children’s and families’ scheduled medical appointments. Data collection included baseline and monthly surveys entered confidentially into electronic tables over a 12-week period. Demographic and clinical characteristics were also assessed at baseline (Tables 1 and 2). Study data were collected and managed using Research Electronic Data Capture (REDCap) tools (Harris et al., 2009). REDCap is a secure, web-based software platform designed to support data capture for research studies, providing (a) an intuitive interface for validated data capture; (b) audit trails for tracking data manipulation and export procedures; (c) automated export procedures for seamless data downloads to common statistical packages; and (d) procedures for data integration and interoperability with external sources (Harris et al., 2019).
Data Analysis
Data analyses were conducted using IBM SPSS Statistics (Version 28). Nominal and ordinal categorical variables were summarized using frequency distributions. Due to the small sample size and skewness, medians, interquartile ranges, and ranges were used for summarizing the continuous age and PedsQL score distributions. Mann–Whitney U and chi-square tests of independence were conducted to compare the demographic and clinical characteristics of the participants in the two study data analysis groups at baseline. Generalized linear models that included the respective scores after the first clinic visit as a covariate were used to assess the effects of AAI on the PedsQL scores for both children and parent-proxy reports. Cohen's d effect statistics were generated from the adjusted study group regression coefficients on each of the PedsQL scores. While effect sizes were the primary focus of this preliminary study, interpretations of statistical significance maintained a maximum alpha of .05 (p < .05).
Results
Of the 31 participant dyads assessed for eligibility, 30 (96%) were randomized; 21 (67%) completed the study. Participant enrollment, allocation, follow-up, and analysis are displayed in the Consolidated Standards of Reporting Trials (CONSORT) flowchart (Figure 2). Twenty-one caregiver and child dyads completed the PedsQL Cancer Module at both baseline and 12 weeks (nine UC, 12 AAI) required for analyses.
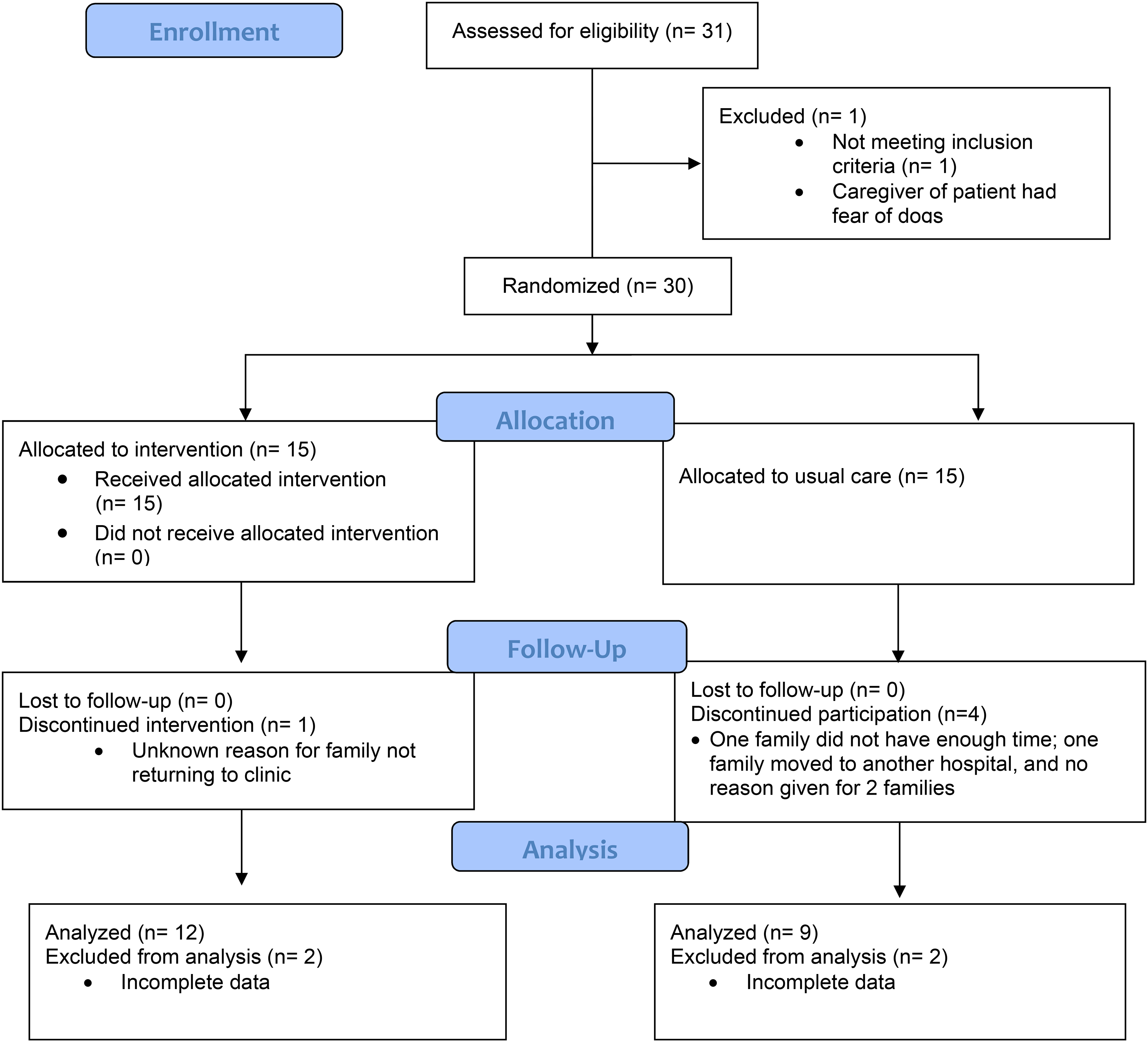
CONSORT Flowchart of Participants in Dyads.
Summaries of the PedsQL Cancer Module scores for child reports and mother proxy reports at baseline, and changes in those scores over the subsequent 12 weeks, are shown in Tables 3 and 4. Controlling for baseline scores, none of the changes over time were statistically significant (p > .05). For the Cancer Module subscales, the strongest effects were observed on communication and procedural anxiety. As illustrated in Figure 3, mothers in both groups perceived their children as having improved communication with healthcare staff and others, while children in both groups reported slightly worsened communication, with a greater worsening in the UC group. As illustrated in Figure 4, mothers in the AAI group perceived that their children had decreased procedural anxiety while mothers in UC reported increased procedural anxiety in their children. Unlike the mothers, though, children in UC reported decreased procedural anxiety, while children in AAI reported increased procedural anxiety. It is important to remember when looking at the slopes in the figures, items on the PedsQL Cancer Module are reverse-scored and linearly transformed to a 0–100 scale (0 = 100); higher scores indicate better HRQoL. In other words, an increasing slope indicates an improvement in HRQoL for that scale.
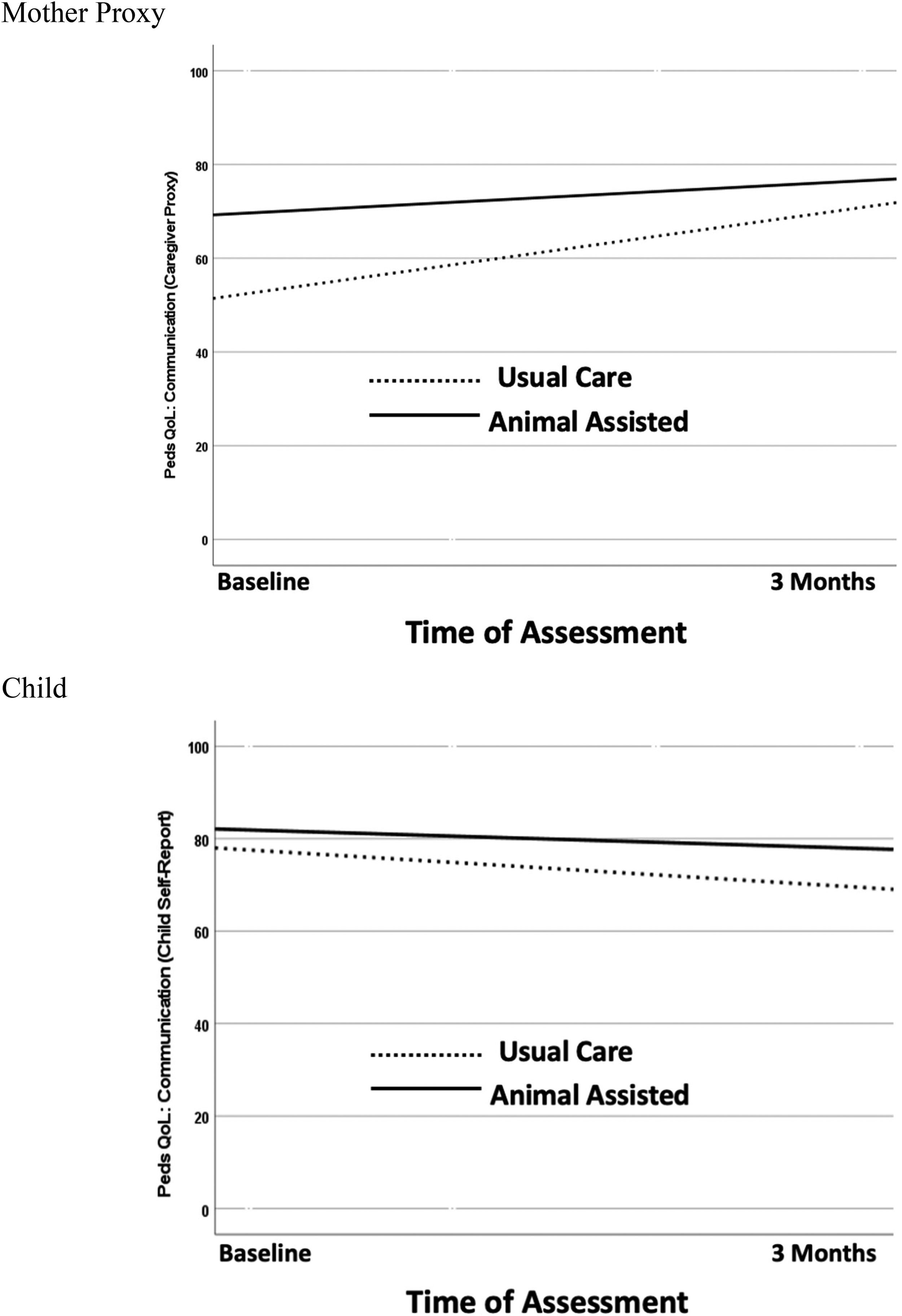
Illustration of Changes in PedsQL Cancer Module Communication Subscale Scores.
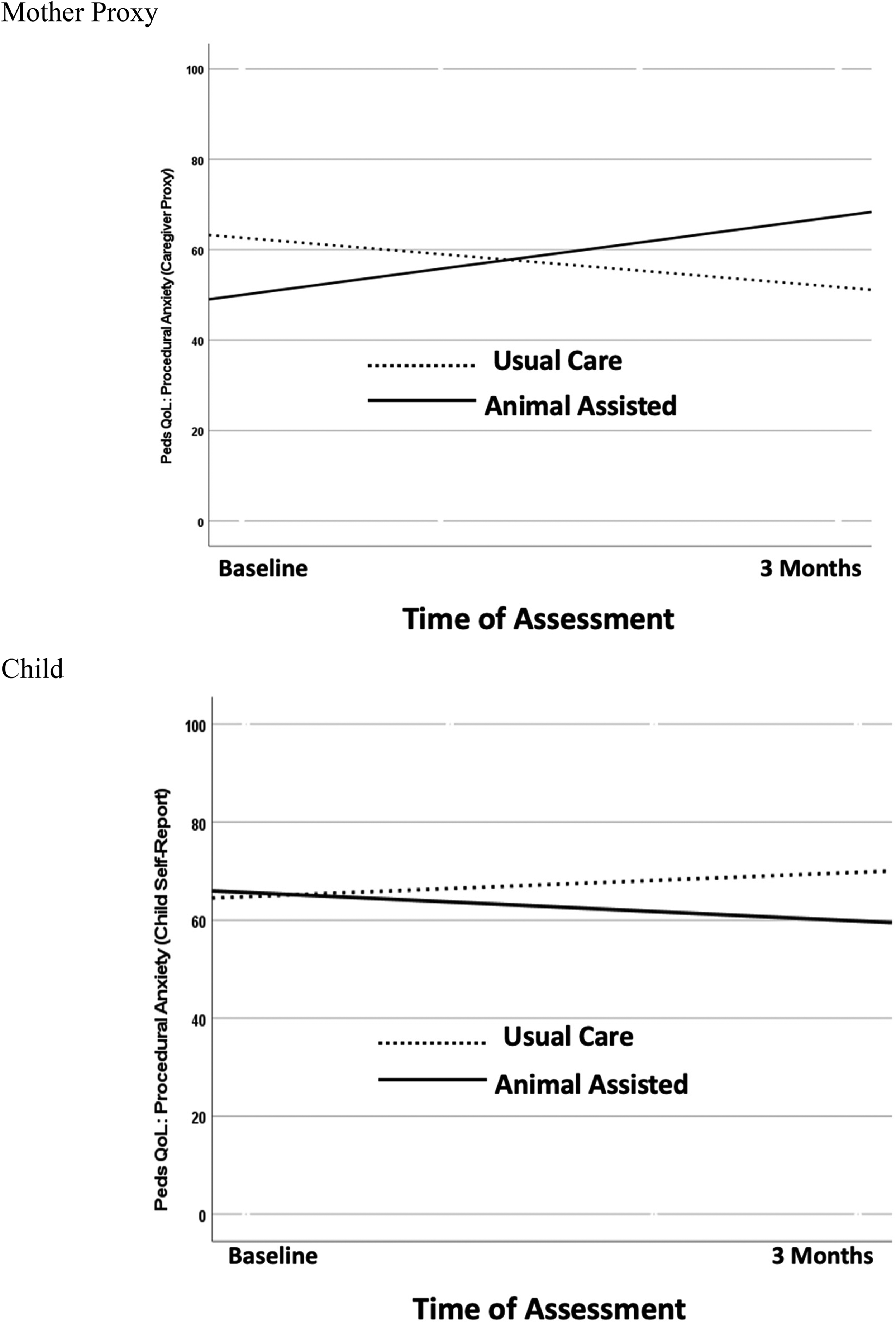
Illustration of Changes in PedsQL Cancer Module Procedural Anxiety Subscale Scores.
Pediatric Quality of Life Inventory (PedsQL™) Cancer Module Summaries: Child Reports
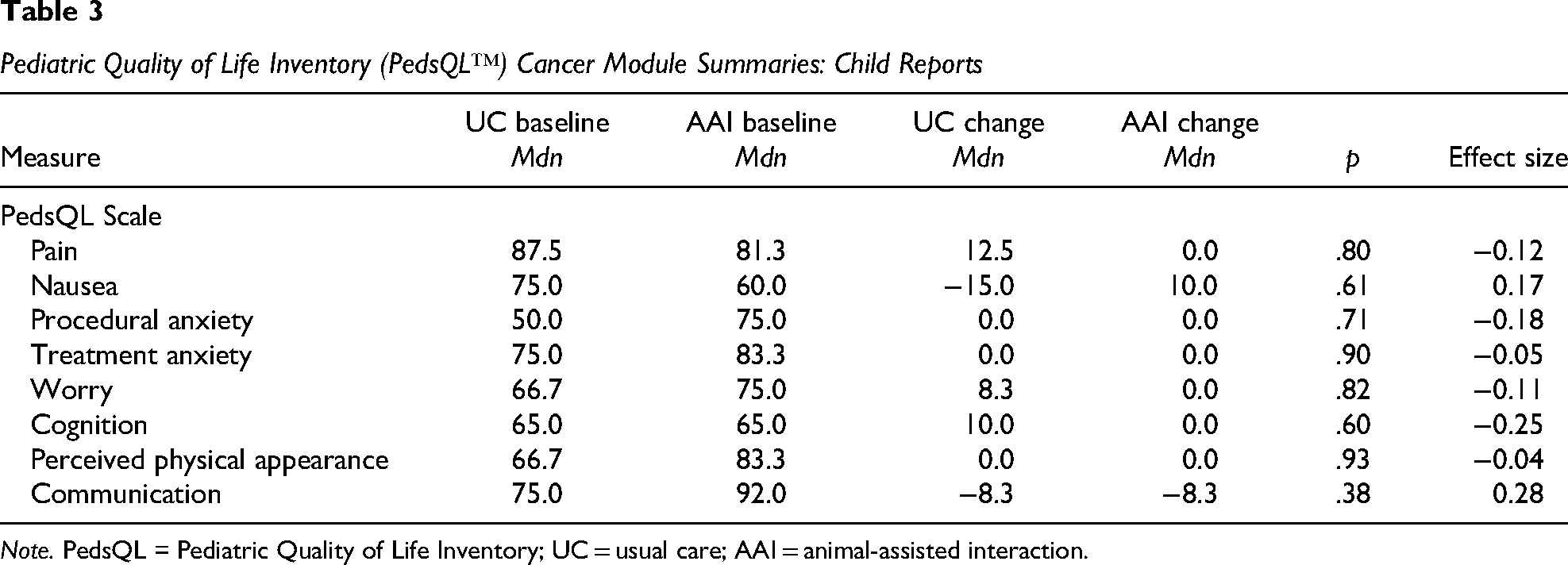
Note. PedsQL = Pediatric Quality of Life Inventory; UC = usual care; AAI = animal-assisted interaction.
Pediatric Quality of Life Inventory (PedsQL™) Cancer Module Summaries: Mother Proxy Reports
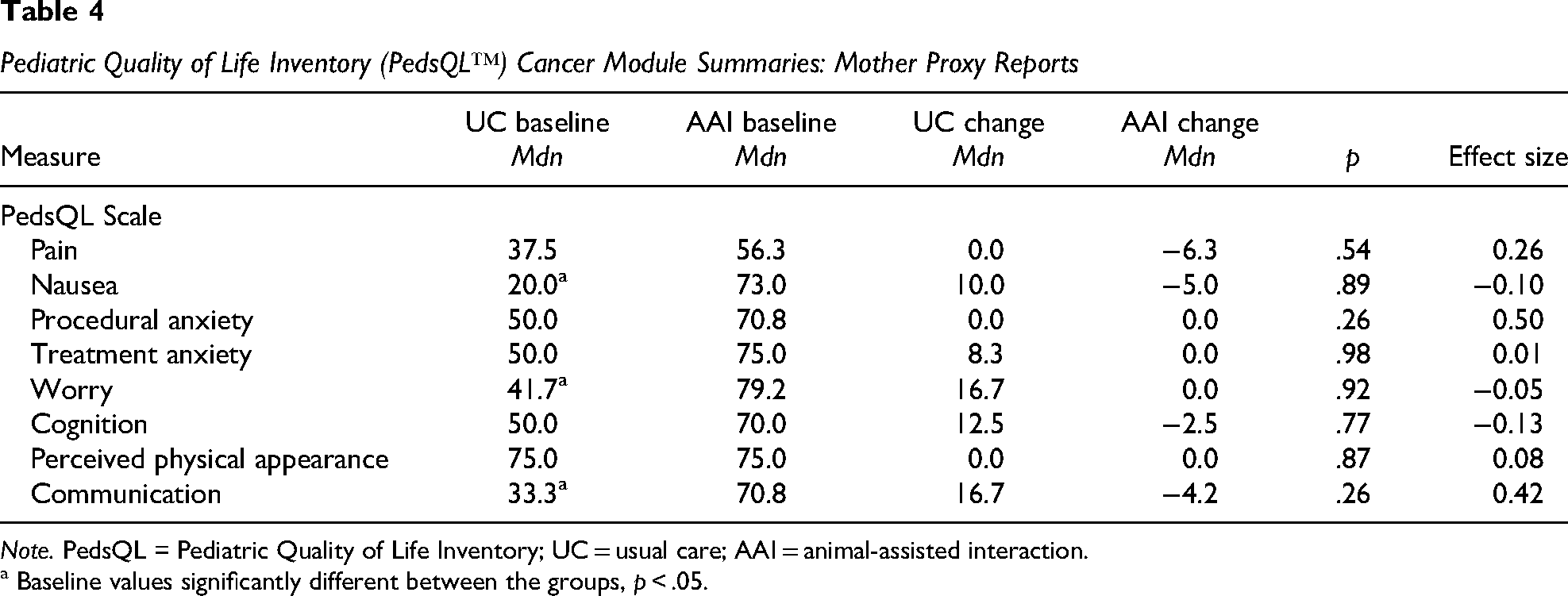
Note. PedsQL = Pediatric Quality of Life Inventory; UC = usual care; AAI = animal-assisted interaction.
a Baseline values significantly different between the groups, p < .05.
Discussion
Overall, the results of this study demonstrated preliminary efficacy for full-scale testing and implementation of AAI with children with relapsed/refractory cancer. While none of the patterns or effects were statistically significant, it is noteworthy to discuss the trends in the two areas that had the strongest effects. Some differences between self-report and parent-proxy were noted in both AAI and UC groups.
It is not uncommon to have cross-informant variance, or discordance, among child self-reports and parent-proxies, and often the information provided by the child with a chronic health condition is not equivalent to that of the parent-proxy (Cataudella et al., 2014; Varni et al., 1998, 2002). While parent-proxies are needed when a child is either unable or unwilling to complete self-reports, researchers are advised to take caution when interpreting parent-proxy reports, as they may not always accurately reflect what a child is experiencing.
There are arguably many factors that may contribute to these discrepancies, and it raises the question of whether the items on the PedsQL Cancer Module adequately capture areas of concern for young people with relapsed/refractory cancer. For example, the school category may not be relevant for children with advanced cancer since most are not able to attend school due to their health. Issues such as finding meaning and maintaining hope, and existential distress that can arise when there is an increased possibility of death and dying, are not addressed (Cataudella et al., 2014). For example, one of the items on the PedsQL Cancer Module is “worrying that the cancer will reoccur or relapse”; the children in this study were already living with relapsed cancer. Mayland et al. (2022) conducted a scoping review of available tools to measure the quality of dying, death, and end-of-life care for children and young people. They found 11 tools, all of which were proxy assessments; all but 1 were undertaken after death, and only 6 out of 11 had undergone psychometric testing within a pediatric palliative care setting. They called for future research to adapt, refine, and improve existing tools, in particular, to find ways to capture the direct views of the dying child, as they are not captured by existing measures.
Until there is an instrument that may better capture HRQoL issues relevant to children with relapsed/refractory cancer, the addition of qualitative measures to directly assess the child's perceptions is essential to enhance our ability to measure intervention outcomes such as those with AAI. As mentioned, this study was a component of a larger mixed-methods RCT; another component of that trial involved a qualitative study to explore perspectives of children with advanced cancer and their parents on experiences with AAI (Cowfer et al., 2021). Children and their parents were interviewed after their final AAI session; all perceived AAI as advantageous, with the only negative aspect reported as too little time with the dog, suggesting that not only was AAI beneficial but also desired at an even greater level.
Strengths and Limitations
There was a risk of selection bias due to convenience sampling and a small sample size. The limited ethnic diversity may affect generalizability. Fathers were not represented in this study. Having both patient and parent-proxy reports was a strength, but it was also a weakness due to the lack of concordance between parent-proxy and patient reports. Strengths include the fact that this was a longitudinal RCT focused exclusively on children with relapsed/refractory cancer. The results show preliminary efficacy of conducting research with this vulnerable population, and the findings expand the body of knowledge related to the impact of AAI on HRQoL in children with relapsed/refractory cancer.
Implications for Future Research
More research is needed with larger samples and may necessitate the use of a measure designed to capture issues particularly relevant to children with relapsed/refractory cancer and their caregivers, with attention on how children can be better supported in communicating their needs with parents and the healthcare team. Incorporating qualitative measures should be considered for all future studies, as well as examining the benefits of longer or more frequent AAI sessions. AAI studies with children with other LTCs, such as neurodegenerative conditions, cystic fibrosis, muscular dystrophy, and heart disease, are another area for exploration.
Conclusion
Results of this study show preliminary efficacy for full-scale testing and implementation of AAI with children with relapsed/refractory cancer. While results were not statistically significant, they suggest AAI showed potential as an intervention for enhancing HRQoL for children with relapsed/refractory cancer. This study adds evidence to a field with limited published studies and presents opportunities for future research to continue to advance the field, including the need to find better ways to capture patient experiences in this vulnerable population. AAI is a promising intervention for children with relapsed/refractory cancer and their caregivers in the hospital/clinic setting and may be applicable to youth with other LTCs.
Footnotes
Acknowledgments
The authors would like to thank the children, their parents, and providers who graciously agreed to help us learn more, and to the volunteer handler/dog teams who make animal-assisted interventions possible. This study also utilized REDCap for data collection and thus benefited from the National Center for Advancing Translational Science/National Institutes of Health Support.
Funding
The authors disclose the following financial support: the Human Animal Bond Research Institute (Grant No. HAB18-010) and the National Center for Advancing Translational Science/National Institutes of Health Support (Grant No. UL1 TR000445).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.