
Abstract
Background
With the emergence of haploidentical transplantation, children with sickle cell disease (SCD) are increasingly pursuing hematopoietic stem cell transplantation (HSCT) as a curative treatment approach. However, suboptimal medication adherence remains a persistent challenge in both SCD and HSCT populations. Adherence to complex medication regimens is crucial to reducing the risk of severe complications and early mortality, yet no synthesis has evaluated patterns of adherence among patients with SCD post-HSCT.
Method
We conducted an integrative review, searching PubMed, CINAHL, and PsycINFO from April 2025 to May 2025 for studies measuring medication adherence in children (≤21 years) with SCD and/or HSCT. Studies were included if they reported adherence rates and excluded if they involved adherence interventions or drug development trials.
Results
Eighteen studies met inclusion criteria: 12 addressed SCD and 6 focused on HSCT. No studies specifically examined adherence in patients with SCD post-HSCT. Adherence rates to disease-modifying medications in SCD ranged from 10% to 89%, while post-HSCT adherence ranged from 40% to 73%. Nonadherence was associated with increased complications across both populations.
Discussion
These findings highlight a critical research gap and provide a foundation for targeted adherence interventions. Addressing this gap is essential to advance nursing practice, improve adherence, and optimize clinical outcomes in pediatric hematology and HSCT care.
Keywords
Introduction
Sickle cell disease (SCD) is the most common inherited blood disease in the United States, affecting approximately 100,000 individuals, with a homozygous frequency of 1 in every 300 births (Kavanagh et al., 2022). SCD is characterized by polymerization of hemoglobin S, resulting in stiff, sickle-shaped erythrocytes that obstruct microvascular flow, which causes acute and chronic pain and leads to progressive organ damage (Kavanagh et al., 2022; Piel et al., 2017). Affected individuals may experience significant complications, such as severe infection, acute chest pain, severe anemia, avascular necrosis, acute chest syndrome, stroke, and other organ damage (Boafor et al., 2016; Kavanagh et al., 2022; Piel et al., 2017). SCD is associated with decreased life expectancy, increased comorbidities, and decreased health-related quality of life (Lubeck et al., 2019; Osunkwo et al., 2021).
Disease-modifying therapies, such as penicillin prophylaxis and hydroxyurea, are essential to reduce disease burden and prevent complications in SCD. However, poor medication adherence is a significant challenge (Loiselle et al., 2016; Walsh et al., 2014). Among pediatric patients with chronic illnesses, it is estimated that 50% of medications are not taken as directed, with nonadherence rates as high as 75% in adolescents and young adults (Brown et al., 2016; McGrady & Hommel, 2013; Rapoff, 2010).
The World Health Organization (2003) defines adherence as “the extent to which a person's behavior—taking medication, following a diet, and/or executing lifestyle changes—corresponds with agreed recommendations from a health care provider”. Nonadherence includes behaviors such as intermittently missing doses, overdosing, incorrect timing or frequency of administration, failure to initiate or refill a prescription, or premature discontinuation of therapy (Brown et al., 2016; Morrison et al., 2017). In pediatric and adolescent populations, the most critical determinant of nonadherence is the complexity and duration of treatment regimens (Belaiche et al., 2017; Coleman et al., 2012; Dew et al., 2018). Medication adherence is measured using a variety of methods, including self-report questionnaires, medication possession ratio (MPR), electronic medication adherence monitors, and drug assay levels. Each method has varying degrees of accuracy, which may influence adherence rates. Adherence thresholds may vary by study, but an adherence rate of 80% or higher is typically the benchmark for satisfactory adherence, particularly in chronic disease management (Anders et al., 2016; Kang & Barner, 2020; Subira et al., 2025).
Medication nonadherence is a major public health concern, contributing to an estimated 125,000 deaths and 25% of hospital admissions annually in the United States (Kini & Ho, 2018). The associated cost ranges from $100 to $500 billion annually, representing up to 16% of total U.S. health care expenditures (Iuga & McGuire, 2014; Kini & Ho, 2018; Neiman et al., 2018; Watanabe et al., 2018). Nonadherence is also associated with increased frequency of hospital admissions, increased length of hospitalization, higher readmission rates, and compromised quality of life (McGrady & Pai, 2019; Morrison et al., 2017).
The emergence of haploidentical donor transplantation has increased curative treatment options for SCD, resulting in more children pursuing hematopoietic stem cell transplantation (HSCT). However, individuals undergoing HSCT are also at increased risk of nonadherence due to the complex nature of therapy. Medication nonadherence posttransplant may lead to significant life-threatening complications such as graft-versus-host disease (GVHD), graft rejection, and systemic infections (Morrison et al., 2017; Pai et al., 2018). Individuals may also experience physical and emotional challenges due to transplant-related toxicities and debilitating GVHD that negatively impact quality of life (Nakamura et al., 2019). Many factors may contribute to nonadherence in the posttransplant setting, including the extensive nature of care, ongoing patient symptoms, and medication side effects (McGrady et al., 2014).
While medication adherence has been studied in pediatric SCD and HSCT recipients separately, no studies have examined adherence specifically in SCD patients post-HSCT. Therefore, the purpose of this integrative review was to synthesize current evidence on medication adherence rates among children and adolescents with SCD and/or those who have undergone HSCT. A secondary aim was to understand the effect of medication adherence on clinical outcomes and health care utilization to guide future research and inform clinical practice.
Method
Search Strategy
To conduct a comprehensive and effective integrative literature search, we systematically explored multiple electronic databases (Whittemore & Knafl, 2005). We selected PubMed for its extensive coverage of biomedical literature and CINAHL to uncover valuable nursing research related to medication adherence. We also used PsycINFO due to its comprehensive coverage of psychological research, which offers a significant role in understanding adherence literature. The literature search was conducted from April 2025 to May 2025. Search terms included “adherence,” “compliance,” “bone marrow transplant,” “hematopoietic stem cell transplant,” “stem cell transplant,” “sickle cell disease,” “sickle cell anemia,” “sickle cell disorders,” “hemoglobin SS disease,” “medication compliance,” “medication adherence,” “medication nonadherence,” “medication noncompliance,” “pediatric,” “child,” “adolescent,” “juvenile,” and “youth.” Limitations were the English language and human (not animal) subject research.
Inclusion criteria were (a) original research, (b) measurement of medication adherence, (c) participants undergoing treatment for SCD and/or HSCT, (d) participants ≤21 years old, and (e) publications in English. Exclusion criteria were (a) adherence not reported, (b) studies involving adherence interventions or drug development trials, (c) adherence measurement not related to medication use, (d) non-peer-reviewed reports or abstracts, and (e) systematic reviews or meta-analyses. Given that SCD is a prevalent global health concern, studies conducted outside the United States were included to provide a better understanding of adherence.
Clinical trials involving drug development require strict adherence protocols to accurately determine the efficacy and safety of new medications, and adherence-promoting interventions are often included within the study design. Therefore, drug development studies and other adherence intervention research were excluded, as they may overestimate adherence rates that do not accurately represent real-world behaviors.
Pediatric medication adherence research, specifically in SCD and HSCT, is limited. Therefore, to ensure a comprehensive understanding of adherence rates within this specialized area, all relevant reports published through May 2025 were included in the review. To be consistent with most pediatric medication adherence research, children and adolescents up to 21 years of age were included.
The PRISMA flow diagram (Fig. 1) illustrates the record selection process (Page et al., 2021). After removing duplicates, 183 records remained, and of those, 48 were screened in full-text review for eligibility. Among those, 20 articles evaluated adherence interventions and were excluded. An additional 11 reports were removed: 2 included participants older than 21 years, and 9 did not provide medication adherence rates. A hand search of the reference list revealed one seminal study from 1990. In total, 18 studies met inclusion criteria and were included in the final review.
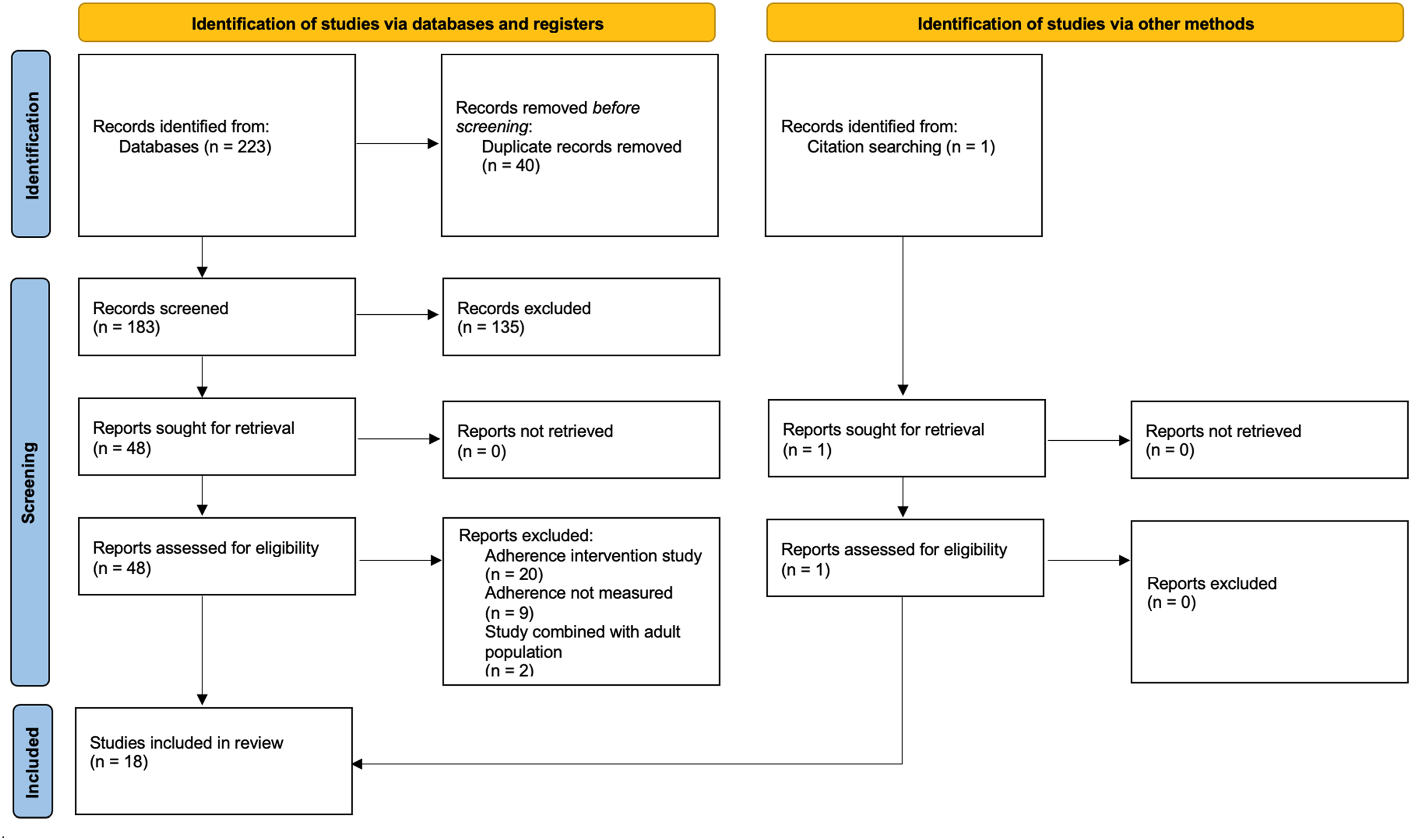
PRISMA Flow Diagram
Results
Twelve out of the 18 studies focused on medication adherence of hydroxyurea and/or penicillin in children and adolescents with SCD (Table 1), while 6 examined adherence following HSCT (Table 2). No studies specifically examined medication adherence in patients with SCD undergoing HSCT.
Adherence in Pediatric Sickle Cell Disease by Medication Type
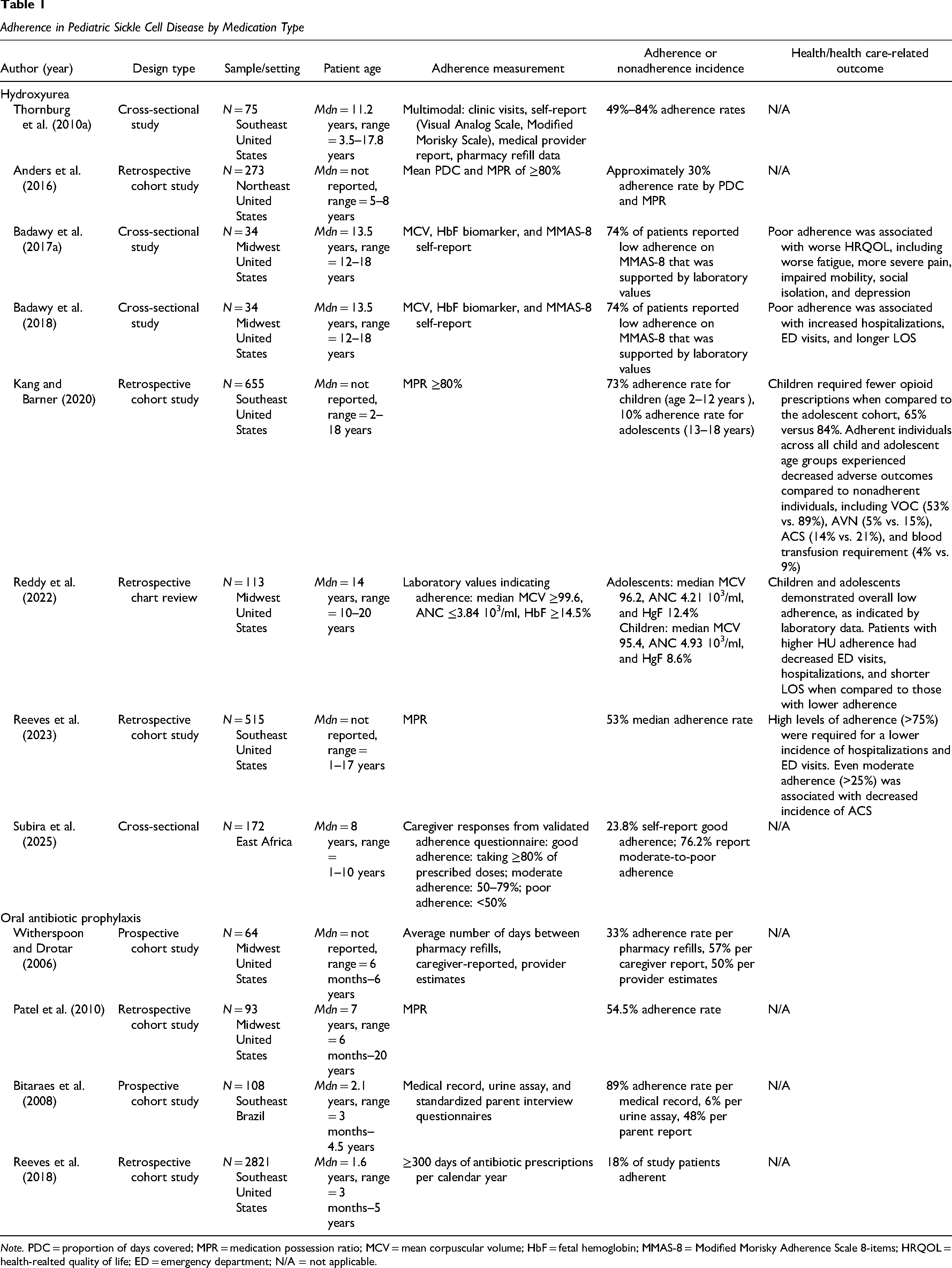
Note. PDC = proportion of days covered; MPR = medication possession ratio; MCV = mean corpuscular volume; HbF = fetal hemoglobin; MMAS-8 = Modified Morisky Adherence Scale 8-items; HRQOL = health-realted quality of life; ED = emergency department; N/A = not applicable.
Medication Adherence in Pediatric Stem Cell Transplantation
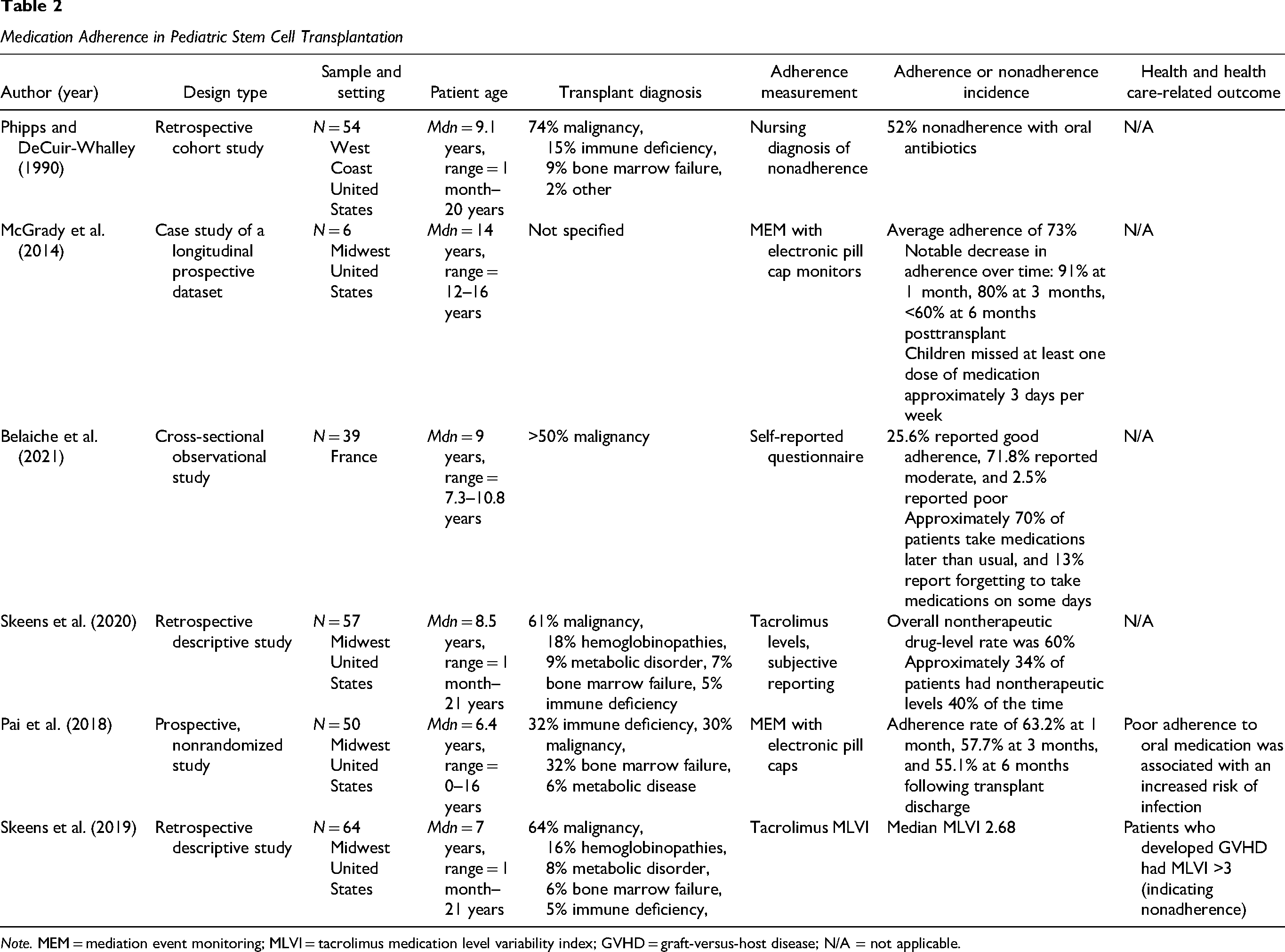
Note. MEM = mediation event monitoring; MLVI = tacrolimus medication level variability index; GVHD = graft-versus-host disease; N/A = not applicable.
Study Characteristics
Setting
Most studies (83%) were conducted in the United States. Two studies of medication adherence among children with SCD were conducted outside the United States. Subira et al. (2025) evaluated hydroxyurea adherence in East Africa, and Bitaraes et al. (2008) examined penicillin adherence in Brazil. One study on posttransplant adherence was conducted in France by the Francophone Society of Bone Marrow Transplantation and Cellular Therapy (Belaiche et al., 2021).
Sample
Sample size varied widely across studies. In the SCD studies, sample size ranged from 34 to 28,271 participants (Badawy et al., 2017a; Badawy et al., 2018; Reeves et al., 2018). Studies involving HSCT generally included smaller cohorts, ranging from six participants in McGrady et al. (2014) to 64 in Skeens et al. (2019). Both SCD and HSCT studies included participants across the pediatric and adolescent lifespan (1 month to 21 years old). Among the six HSCT studies, only two reported including patients with hemoglobinopathy as the transplant diagnosis; however, it is unclear whether these participants had a confirmed SCD diagnosis (Skeens et al., 2019; Skeens et al., 2020).
Design
In the SCD cohort, two studies employed prospective designs (Bitaraes et al., 2008; Witherspoon & Drotar, 2006). Similarly, within the HSCT cohort, Pai et al. (2018) conducted a prospective nonrandomized study, and McGrady et al. (2014) analyzed a longitudinal prospective dataset. The remaining studies across both cohorts used cross-sectional or retrospective designs.
Medication Adherence in SCD
Overall adherence rates to disease-modifying therapies varied significantly across studies, ranging from 10% to 89%. Variability was also observed across different methods of measuring adherence. Eight studies evaluated hydroxyurea adherence, with publication dates ranging from 2010 through 2025 (Anders et al., 2016; Badawy et al., 2017a; Kang & Barner, 2020; Reddy et al., 2022; Reeves et al., 2023; Subira et al., 2025; Thornburg et al., 2010a). Four studies examined adherence to antibiotic prophylaxis, the most recent of which was published in 2018 (Patel et al., 2010; Reeves et al., 2018; Witherspoon & Drotar, 2006). A range of adherence measurement approaches was reported across the studies and is summarized in Table 1 and described in more detail below.
Hydroxyurea Adherence Rates
Thornburg et al. (2010a) analyzed hydroxyurea adherence rates in 75 children ages 3.5 to 17.8 years using a multimodal assessment of adherence, including number of clinic visits (recommended versus actual), caregiver self-report (via the Modified Morisky Scale and a Visual Analog Scale [VAS]), provider report, and pharmacy refill data. Reported adherence rates ranged from 49% to 84% depending on measurement method. Only 49% of participants refilled a 30-day supply of medication five or more times in a 6-month period with 59% refilling four or more times. Despite this, relatively high levels of adherence were reported through VAS (82%), the Modified Morisky Score (84%), and medical provider estimate (85%). Adherence to scheduled hydroxyurea follow-up clinic visits was 77%.
Anders et al. (2016) evaluated Medicaid data in 273 children with SCD to measure adherence using MPRs and proportion of days covered (PDC) for the therapy period, spanning the first and last fill. The mean PDC in the first year was 56.3%, and only 30% met the ≥80% adherence threshold. More recently, Subira et al. (2025) evaluated 172 children, ages 1 to 10 years, with SCD in East Africa. Adherence was measured by caregiver questionnaire; approximately 24% reported good adherence (≥80% of doses), with 76% reporting moderate to poor adherence.
Hydroxyurea Adherence and Outcomes
Reeves et al. (2023) evaluated hydroxyurea adherence by MPR in children with SCD ages one to 17 years enrolled on Medicaid during 2005–2012. This multistate study included data from Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas. Among the 2,474 children screened, 515 (18.7%) had initiated hydroxyurea therapy. High levels of adherence (>75%) were required for a lower incidence of hospitalizations and emergency department visits. Even moderate adherence (>25%) was associated with decreased incidence of acute chest syndrome (Reeves et al., 2023).
In an evaluation of Texas Medicaid claims from 2011 to 2016, Kang and Barner (2020) reported that children (age 2–12 years) were more adherent to hydroxyurea than adolescents (13–18 years), 73% and 10%, respectively. Children required fewer opioid prescriptions when compared to the adolescent cohort, 65% versus 84% (Kang & Barner, 2020). Adherent individuals across all child and adolescent age groups experienced decreased adverse outcomes than nonadherent individuals, including vaso-occlusive crisis (53% vs. 89%), avascular necrosis (5% vs. 15%), acute chest syndrome (14% vs. 21%), and blood transfusion requirement (4% vs. 9%; Kang & Barner, 2020).
Reddy et al. (2022) completed a 5-year retrospective chart review of 113 children and adolescents with SCD prescribed hydroxyurea therapy. Routine complete blood count and fetal hemoglobin laboratory results measured adherence. Adolescents and children demonstrated overall low levels of adherence. Individuals with higher fetal hemoglobin, higher mean corpuscular volume (MCV), and lower absolute neutrophil count (ANC) (indicating adherence) required fewer emergency department visits and hospitalizations, decreased length of stay, and decreased incidence of chronic pain (Reddy et al., 2022).
Among 34 adolescents with SCD (age 12–18), 75% reported low hydroxyurea adherence on Modified Morisky Adherence Scale 8-items (MMAS-8) self-report that was consistent with laboratory findings (Badawy et al., 2017a; Badawy et al., 2018). Poor adherence was associated with more frequent hospitalizations, emergency department visits, and longer length of stay (Badawy et al., 2018). Patients with increased health utilization also experienced worse fatigue, more severe pain, impaired mobility, and social isolation (Badawy et al., 2018). Poor adherence was also associated with worse health-related quality of life, including worse fatigue, more severe pain, impaired mobility, social isolation, and depression (Badawy et al., 2017a).
Antibiotic Prophylaxis Adherence Rates
In a large study by Reeves et al. (2018) including 2,821 young children (3 months–5 years) with SCD across multiple states, only 18% had >300 days of filled antibiotic pneumococcal prophylaxis. Witherspoon and Drotar (2006) conducted a prospective study involving 64 children with SCD aged 6 months to 6 years. The researchers examined adherence to penicillin using various measurement methods and found the following rates: 57% based on caregiver reports, 50% based on clinical evaluations, and only 33% according to prescription refill monitoring. In a prospective trial including 108 children under 5 years old, Bitaraes et al. (2008) also identified discrepancies in antibiotic adherence across different measurements, with reported adherence rates of 89% from medical record reviews, 56% from urine tests, and 48% per parent reports. Patel et al. (2010) evaluated adherence to a variety of maintenance medications in 93 children and adolescents (≤18 years) with SCD. Among the children who were prescribed penicillin prophylaxis, 55% (n = 62) were considered adherent by demonstrating a MPR ≥75% (Patel et al., 2010). None of the studies included in the review evaluated the effect of antibiotic prophylaxis on health or health care outcomes.
Medication Adherence in Pediatric HSCT
Medication adherence in children and adolescents following HSCT was poor, with reported rates of 40% to 73% (McGrady et al., 2014; Pai et al., 2018; Phipps & DeCuir-Whalley, 1990; Skeens et al., 2020). McGrady et al. (2014) reported on medication adherence among six children (ages 12–18 years) post-HSCT. Data was obtained from a larger, prospective study that examined adherence using medication event monitoring with electronic pill cap monitors. Data from pill bottles were downloaded at four time points (1, 3, 6, and 9 months) following transplant discharge. Researchers found adherence rates to be relatively stable at 91% in the first month following transplant hospital discharge; however, the trend decreased over time to less than 60% at 6 months postdischarge. Participants also missed at least one dose of medication on an average of 3 days per week (McGrady et al., 2014).
A cross-sectional, multicenter study that included 39 children (7.3–10.8 years), examined medication adherence 3–6 months post-HSCT (Bealaiche et al., 2021). Although the study included both adult and pediatric participants, pediatric data was analyzed and reported separately and was therefore included in this review. Caregivers and/or patients completed a self-reported questionnaire for adherence measurement. Medication adherence was estimated as good in 25.6%, moderate in 71.8%, and poor in 2.5% of patients. Approximately 70% of patients reported taking medication later than usual, and 13% reported not taking medications at all on some days.
In a seminal study by Phipps and DeCuir-Whalley (1990), nonadherence was determined by nursing documentation in a retrospective chart review. Among the 54 children (1 month–20 years) included in the study, 52% were reported as nonadherent with oral antibiotics. Investigators also found the highest incidence of nonadherence in children 2–12 years of age (Phipps & DeCuir-Whalley, 1990). However, additional research by Skeens et al. (2020) reported nontherapeutic immunosuppression levels, indicating nonadherence, most frequently occurring in children 1–5 years old. The retrospective study included 57 children aged 1 month to 21 years. The overall nontherapeutic drug level rate was 60%, and approximately 34% patients had nontherapeutic levels 40% of the time (Skeens et al., 2020).
Only two of the six HSCT studies examined the effect of medication adherence on health outcomes which included the incidence of infection and GVHD (Pai et al., 2018; Skeens et al., 2019). Skeens et al. (2019) used tacrolimus medication level variability index (MLVI) to assess the development of GVHD and hospital readmission. The retrospective study included 64 patients (1 month–21 years) post-HSCT. Patients with elevated MLVI, representing subtherapeutic immune suppression, had a greater incidence of GVHD than those with lower levels (p = .024).
In a prospective nonrandomized study by Pai et al. (2018), including 50 transplant recipients (0–16 years), adherence was measured by electronic cap monitoring. Investigators reported adherence rates of 63.2% at 1 month, 57.7% at 3 months, and 55.1% at 6 months following transplant discharge. Although researchers did not find a relation between adherence and GVHD post-allogeneic HSCT, there was an increased incidence of infection (p = .005) in patients who demonstrated nonadherence (Pai et al., 2018), with the most common documented infection across all time points being gram-positive cocci.
Discussion
This integrative review aimed to comprehensively identify and summarize existing research on medication adherence among pediatric patients with SCD and those undergoing HSCT. Across published literature, suboptimal medication adherence emerged as a persistent and significant challenge in both populations. The overall rates of adherence to medications ranged from 10% to 89% for SCD patients and 40% to 73% for HSCT recipients. Notably, there were no published studies that focused specifically on medication adherence in children with SCD post-HSCT.
Researchers employed various methods to measure adherence, including caregiver self-reports, provider reports, pill counts, electronic monitoring devices, pharmacy refill data, and monitoring of drug assay levels. Adherence rates tended to be higher when measured via self-report, but lower with objective measures such as pharmacy refill or drug assay data (Thornburg et al., 2010a; Witherspoon & Drotar, 2006). This finding is consistent with broader adherence literature, suggesting that both patient and provider reports often overestimate adherence rates (Walsh et al., 2014). This underscores the importance of using objective measures in conjunction with self-reports in adherence research and clinical practice (Shah et al., 2023). Furthermore, the lack of standardized measurement approaches for adherence creates challenges when comparing findings across studies and limits the generalizability of results.
Hydroxyurea has been shown to be effective in reducing the frequency of pain crises, acute chest syndrome, hospitalizations, and the need for red blood cell transfusions (Wang et al., 2011). Adherence rates for hydroxyurea during the landmark clinical trials assessing its efficacy ranged from 74% to 95% (Kinney et al., 1999; Thornburg et al., 2010b; Wang et al., 2011). However, this review found that after the U.S. Food and Drug Administration approved hydroxyurea for use in children, adherence rates dropped significantly, falling as low as 34% to 67% (Alvarez et al., 2009; Anders et al., 2016; Creary et al., 2019). The effectiveness of hydroxyurea in preventing complications associated with SCD may be diminished in real-world applications due to issues with nonadherence (Walsh et al., 2014).
Children with homozygous SCD are at increased risk of developing invasive pneumococcal disease caused by Streptococcus pneumoniae bacteria. This condition is serious and potentially life-threatening, as it can progress rapidly and may lead to death if not treated promptly (Yawn et al., 2014). Children who receive daily penicillin are 84% less likely to develop an infection than those without prophylaxis (Gaston et al., 1986). Experts recommend that children with SCD receive penicillin prophylaxis medication from infancy through the age of 5 (Yawn et al., 2014). Despite over three decades of education and support for antibiotic prophylaxis, our review found adherence rates as low as 18% (Reeves et al., 2018).
The primary concern for nonadherence in SCD and HSCT is the risk of adverse patient outcomes (Visintini et al., 2023). In this review, medication adherence had significant clinical implications across both populations. Increased adherence to hydroxyurea was associated with a reduction in hospitalization, emergency department visits, and length of stay (Badawy et al., 2018; Reddy et al., 2022; Reeves et al., 2023). Higher levels of adherence were also associated with decreased incidence of adverse health outcomes, including acute chest syndrome, vaso-occlusive crises and avascular necrosis (Kang & Barner, 2020; Reeves et al., 2023). Conversely, poor adherence was correlated with worse health-related quality of life (HRQOL), leading to more severe pain, fatigue, social isolation, and depression (Badawy et al., 2017a).
In the context of HSCT, children and adolescents who demonstrated nonadherence were shown to have a greater incidence of systemic infection and acute GVHD (Pai et al., 2018; Skeens et al., 2019). When individuals with SCD undergo HSCT, they are introduced to additional medications, potential risks, and treatment-related side effects (Kassim & Sharma, 2017). Strict adherence to complex oral medication regimens is necessary to prevent transplant-related complications and optimize outcomes (Morrison et al., 2017; Pai et al., 2018; Visintini et al., 2023). Increasing the complexity of care may cause an even greater risk of medication nonadherence and worse health-related outcomes.
Our review is subject to several important limitations that must be acknowledged. Firstly, we only included studies published in peer-reviewed journals, which may inadvertently exclude valuable research findings from gray literature, conference abstracts, or unpublished studies. Consequently, there may be additional investigations evaluating medication adherence in pediatric SCD and HSCT that we did not consider. Secondly, this review focused only on understanding medication adherence rates. We did not systematically explore the potential barriers and facilitators that impact medication adherence in SCD and HSCT. Several studies have attempted to address barriers to adherence in these patient populations (Chardon et al., 2022; Chardon et al., 2023; Hoegy et al., 2019; King et al., 2023; Badawy et al., 2017b; Curtis et al., 2019). By not addressing these critical factors, we miss the opportunity to provide an understanding of the unique challenges that influence adherence (Adams-Graves & Bronte-Jordan, 2016). Furthermore, we did not evaluate specific interventions designed to enhance medication adherence, which could offer insights into effective strategies and practices. Additionally, the small sample size of the included studies may limit the generalizability and robustness of our findings.
Overall, while our review contributes to the existing literature, further research exploring both the complexities of adherence and the effectiveness of targeted interventions is needed. SCD is distinct from other chronic illnesses due to its significant impact throughout an individual's life, the stigma associated with the disease, and the existing health care disparities (Hodges et al., 2020). Future research on medication adherence in children with SCD undergoing transplant is crucial to providing clinicians with the necessary resources to identify patients at risk for nonadherence and implement strategies to enhance adherence in real-world settings.
Summary
This integrative literature review indicates that children with SCD are at significant risk for medication nonadherence. Adherence to disease-modifying medications is crucial in improving health outcomes and reducing disease-related complications. Similarly, children who undergo HSCT also show nonadherence with immunosuppressive and antimicrobial medications in the acute posttransplant phase. Nonadherence can negatively impact health by increasing the risk of GVHD, infection incidence, and other transplant-related complications. As alternative donor transplantation becomes more accessible for patients with SCD, it is imperative to thoroughly examine medication adherence in this patient population.
Investigating medication adherence is important to provide clinicians with resources to identify patients at risk for nonadherence, recognize potential barriers and facilitators, and implement strategies to improve adherence in real-world applications. Understanding the reasons behind nonadherence, such as socioeconomic factors, psychological barriers, and medication regimen complexity, will enable health care providers to develop targeted interventions for sustained behavior change. By addressing these issues, we can improve adherence rates, enhance patient outcomes, and ultimately provide better quality of care for children with SCD undergoing transplantation.
Footnotes
Ethical Considerations
Ethical approval was not required for this integrative review.
Author Contributions
Misty Evans contributed to the conception of the review, performed a systematic review, prepared the first draft, and incorporated revisions. Samereh Abdoli, Micah Skeens, and Dominique Bulgin critically reviewed the manuscript. Lisa C. Lindley contributed to supervision and also critically reviewed the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Misty Evans has a consulting relationship with Vertex Pharmaceuticals, Jazz Pharmaceuticals, and Alexion Pharmaceuticals. This relationship did not influence the research, preparation, or content of this manuscript.