
Abstract
This article states the need to decolonize the theories, policies, and practices that dominate health, and reflects on the necessity for a new epistemology built from the Global South. This allows rethinking health with a new categorical framework, which incorporates socially determined health and life, with the optic of reaching the highest conceivable degree of living well/well-living. We put forth that the epistemic bases of epidemiology and the implementation of health systems tend to reproduce a coloniality of power and of established health knowledge. Health systems are viewed as an accumulation of reforms based on theories and policies of the Global North imposed on Latin America and the Caribbean. These systems have been built as bureaucratic, biomedicalized, treatment-oriented, and commercialized health systems that are perceived as external to societies and that reproduce mistreatment, violence, and racism. We make the argument to rethink, remake, and decolonize the theories and practices that govern both epidemiology and health systems, and, from the South, develop strategic processes for building health sovereignty as the vision for the reconstruction of hope and social justice.
Keywords
Background
This article expands the concept that health is socially determined 1 to build a new framework for understanding epidemiology and health systems, especially from the vantage point of the twenty-first century Global South. That health is socially determined rather than a contextless physical and mental state of being follows from the tenets of critical epidemiology 2 advanced by Breihl and other theoreticians in Latin America over the past decades. Socially determined health is one of the three central categories 3 of critical epidemiology 4 along with social reproduction and society-nature “eco-metabolism”, 5 which describes the flows of energy, materials, and waste products that maintain or degrade nature and society—metabolismo sociedad-naturaleza in Spanish. 6
Socioculturally determined health should not be confused with social determinants of health, which focuses on the materiality of health-impacting community conditions and policies rather than explicit social processes. Applying this broader concept helps us understand and confront the social legacy of colonialism on health systems, public health, and epidemiology in Latin America. Underpinning this legacy is an enduring colonial epistemology, which we strive to upend with a new epistemology that will help us chart a decolonized future with our own theories, policies and practice.
Rather that stating a theory, its postulates, and modeling of social relations, policies, economics, and health systems, we leverage the category of socially determined health to explain the internal logic, means, and historical context by which colonialism propagates its epistemological dominance over Latin America. This approach also supports thinking of new ways to transform current system categories and linking understanding to action. Socially determined health as a theoretical framework of critical epidemiology is widely recognized (but less applied) in Latin America than in Europe, where its theoretical basis has not attracted the same degree of interest or development.
First, we describe four dimensions of critical thinking of health from the South. Second, we provide a detailed examination of how the epistemological foundation of current health systems and epidemiology has been conditioned and even adversely impacted by modern scientific thought 7 which reinforces deep asymmetries of coloniality, dependence, and hierarchies anchored to geopolitical power, information and technical expertise.
Critical Latin American thought in health encompasses four processes that we weave together: epistemology, geopolitics, ethics, and action orientation. In the first, we assert that population health is a social-cultural process that is overshadowed by colonial and racial legacies and by capitalism as it has played out from dominant centers (i.e., Europe) to the periphery (former colonies) and ecologically through the world. This raises uncomfortable questions of how we release ourselves from these legacies and create space for a holistic vision of health, policies, and health sovereignty against a backdrop of obstacles and the desire to collectively create living well/good living for Latin American societies and communities. The concept of socially determined health stands in opposition to the dominant Eurocentric theories of international development, conventional definitions of well-being, and the notion of “progress” in the health arena.8,9 Decolonizing the prevailing theories, policies, and practice challenges a perceived universal order in which the “scientific community” normalizes “science” which provides the West's accepted knowledge of health/disease process, and, in turn, is reproduced and internalized in the Global South.
The hegemonic predominance of the framework of tropical medicine with colonial overtones, the biomedical model of health focused on individual diagnosis and treatment (individual pathophysiological repair;10,11), a public health focused on functionalism, and an Anglo Saxon/Eurocentric epidemiology are embedded in the world of academia, health ministries, schools of public health, and in the theory, policies, and organization of health systems. This epistemological framework, which some take as all-encompassing in their academic and professional lives, poses a significant obstacle to considering epistemologies other than “population pathology”. 12 The State directs unilateral action toward the object “society,” and it mobilizes health workers and technicians as the State's agents to carry out a bureaucratic positivist order in which medical care institutions and the population are objects to be controlled and surveilled. The State, in exercising its exclusive power, projects its ideology for the scientific and technical basis of risk and disease prevention of a population, as if it were only a sum of individuals.
These norms and functions become a blind spot for rethinking a critical theory of health from the South that embodies theory, methodology and policy of critical epidemiology, and remaking health systems in regions such as Latin America and the Caribbean, which bear the burden of historical Eurocentric and Pan American health doctrines.
The reasoning behind public health and functionalist epidemiology stems from the theory, knowledge base, and methods of structural functionalism, which, as espoused by Parsons, 13 underlies causality, stability, and equilibrium of systems. The principles include adaptation, achievement of goals, and the maintenance of guidelines for social integration within and reproduction of the social system. In this framework, social problems, including health problems, are merely functional imbalances—mismatches—that are produced and can be corrected in subsystems. This helps explain the thinking behind public health and its functionalist epidemiology, which always presents itself as a series of corrections or mitigations to control functional imbalances. Instead of transforming processes, it operates through the calculation of risks and as a progression of explanatory frameworks: agent-host environment 14 ; the primacy of socioeconomic factors in health 15 ; equity and health. 16 This type of public health and its epidemiologic expression are reproduced in current cognitive capitalism in its accelerated phase of financial liquidity and social-environmental extraction. Even the discussion of health inequalities between and within nations can be viewed as reductionist simplifications of causality, disconnected and isolated.17–19
Also, seen through the lens of structural functionalism, the plethora of current reports focusing on health inequalities presume that inequalities are merely imbalances that require correction, rather than the result of an underlying determinative process.
We want to clarify that socioculturally determined health is not social determinism, which subordinates biology to social and natural phenomena, but rather it is a complex process of conditions and challenges in quasi-structural problems intertwined at multiple levels inherent to the contemporary world system but with specificity to Abya Yala (meaning Nuestra America/Our America) as a marginalized and dependent periphery of capitalist colonial world system. This framework posits a combination of theories, typologies, language, concepts, and methodologic and analytic approaches entrenched in the institutional knowledge and actions of universities, professional fields, health diplomacy, and public administration that internalize a Eurocentric/Pan American canon to reproduce, copy, assimilate a one-and-only positivist science. Imitation and/or adaptation are central as political-sanitary coloniality.
Expressions and concepts such as well-being, health and development, reforms, health systems based on primary care, models of social welfare, levels of care, public health programs (i.e., categorical programs for specific diseases), essential functions of public health, epidemiologic transition, diseases of development-underdevelopment, the natural history of disease, risk factors, and social determinants of health correspond to an epistemology of health and development theory that follows a transformation of market colonialism to industrial capitalism based on international development, and then to cognitive neoliberalism. Throughout the twentieth century, this epistemology of health was internalized by institutions in the United States, societies at large, epidemiology, and health systems. Dependence produced by the coloniality of thought, knowledge, and action in the field of health and epidemiology is not only an external phenomenon; it also manifests itself in the internal structures and processes of academia, public administration in the health sector, and dominates the culture of societies of the Global South.
The agenda, geopolitics, and actions of liberal global health and Pan American regional health doctrine with its national and local impacts fosters dependence as an intrinsic characteristic in the theory, practice, and policies of epidemiology and health systems. This dependence generates a homogenization of possible pathways and limited understanding of the specifics of the South, and it embodies the international framework for health policy in the periphery.
Intersection of Decolonization and Refounding Health Systems in the Twenty-first Century
Situated at the crossroads of decolonization is a second requirement: birth of a systematic review of the theories, policies, and workings of the State and the health systems in Latin America which were formed and functionalized by development interests from the center to the periphery, by capital, and by the market that enabled a mercantilization of life through a medical-industrial-financial-insurer complex tied to commercial agreements from the United States and corporations of the Global North. This makes the need self-evident to push for self-determination of health sovereignty, policies, and health systems of the South.
The epistemological foundations of health systems in Latin America and the Caribbean tend to reproduce coloniality of power and of institutional knowledge in health systems. This makes health systems an accumulation of reforms of reforms of reforms of organizational and institutional changes from the standpoint of the theories and practices of the Global North. 20 Health becomes a colonial concern with racializing and dehumanizing the lives of indigenous people and African slaves, and is a response that progresses through the beneficence and charity of public health hygiene to: importation of Bismarkian social security; missions of the International Labor Organization in the 1940s; the post-war Beveridge (United Kingdom) model of state-run, universal health care financed by income taxes with universal biomedical care for corporal repair to return to the production process; workers’ compensation linking medical care and indemnification to levels of injury and incapacity; categorical (disease-specific) financing and programming; and the myth of primary care guided by a strategy for impoverished people in the periphery. In general, these efforts, based on the epistemology of social welfare, are additive and present transitions of intertwined global capitalism, colonialism, and modernity. These Eurocentric classes and types of models of social protection, which rest on social theories of the Global North, are held up as universal and cast as referential frameworks of ground zero (they are “universal” models). The latest iteration of neoliberal social protection includes social risk management 21 and structural pluralism 22 promoted by the World Bank and the Inter-American Development Bank with the Pan American Health Organization, which have implemented a molecular expansion of regulated markets of health insurance financial coverage that culminate in universal health coverage. 23 These same health system reforms were and are spaces to parse functions and anchor the regulation of financial coverage markets through systems of insurance. Taken as a whole, these structures and processes converge to produce what we call Frankenstein health systems, which are biomedicalized, bureaucratic, and oriented toward treatment, insurance, and profit. They are perceived to be external to society and reproduce the mistreatment, violence, and structural racism over plurinational and intercultural territories and territorialities, 24 accompanied by epidemiologic and socioenvironmental polarization. None of these cumulative reforms resolves the question of social and health inequities that are intertwined and overlaid with social class, race/ethnicity and gender, nor do they respond to collective health determinants in the region.
Thinking about health systems for the twenty-first century requires transcending these Frankenstein systems, their theory, methodology, Eurocentric policies, and Pan American health doctrine because this framework hides the origins of the dependence and coloniality from long-term imitation of the hierarchical orders and only considers a perspective through the epistemological lens of the Global North. Here, we posit the central question of how to exit this dynamic of reproduction of coloniality and concomitant dependence on its theory, praxis, and policies in the health sector.
This implies a review of specifics and the colonial vestiges in the United States and the Global South as fundamental factors shaping health systems, and we reorient or turn (giro in Spanish) ourselves toward a decolonized vision. 25 We highlight the necessity to decolonize the theories and policies of health systems, which implies interculturalizing, plurinationalizing, and decolonizing structures, concepts, practices and institutions. 26
Injecting complex, decolonial thinking implies a whole other system of knowledge for liberation. In particular, positioning socioculturally determined health as one of the pillars of refounding health systems provides a new point of departure and requires a categorical reframing. 20 This shift is not only a change of language, terminology, the classes of “reforms,” and the concepts of development, Eurocentrism, Pan Americanism or neoliberalism. This rededication looks to propose a new body of categories. 3 The intention from an epistemological and theoretical standpoint is not to be limited by copying classes or concepts, but rather to search for a new body of theories and concepts originating from the South. Hence, the reality of what is perceived in a previous category is not the same in the new frame; thus, the epistemological intention inevitably becomes a transformation of the previous content of the category so that the new content of the concept or category becomes reality in the new approach. This is to say, we create a new categorical system that expresses and materializes critical Latin American thought on health truly constructed from the South.
The territorial architecture of health systems is constructed over a hierarchical and pyramidal base of logic with health establishments such as hospitals, ambulatory clinics, etc., occupying a central focus: the population is an object, there is a distribution of mortality and morbidity, there is widespread homogeneity of medical care, and administrative geographies are made up of jurisdictions for health and social services. In fact, the thesis that underlies Integrated Networks of Health Services 27 implies a functionalism of health services as a focus and a homogeneous, institutionalized amalgam of networks joined together by pyramidal levels of resolution. This logic interweaves the focus of a twentieth century public health workforce as an agent of the State which controls social space with the goal of state-sponsored curative health services, prevention based on individual risk factors, and disease control in populations. We propose Integral Health Care and Well-Living (Cuidado Integral de la Salud y Vivir Bien in Spanish) in the framework of a remade health system, displacing: the existing bureaucratic, institutional geography, which aims to externally control the population apart from society; and the critical social geography of health systems that are produced and constructed as interwoven territories, territorialities, and dynamics of social reproduction at the levels of urban-rural and community-popular. We can reframe health in terms of open, heterogeneous, and symmetrical health networks interwoven with institutionality and territoriality, not only coordinated but embodying strategies of living well and quality of life and health. The molecular expansion of a new institutionality and territoriality, centering the territory where life is developed and collective health is socioculturally produced, will re-dimension the potential shapes and forms acquired by health systems in every country, territory, and context to respond integrally to socially determined health and life—without canned solutions or care-healing packages.
From here we introduce the need to advance an organizing principle of particular importance to rethink and remake health systems: integral care for health and life. Since the decade of the 1970s with the Alma Ata international health conference to assumptions behind integrated and selective primary health care of United Nations Children's Fund (UNICEF) and the Rockefeller Foundation, 28 primary health care became a fetishized framework of discourse about health for the Global South. Nonetheless, during the decade of the 1970s, this conception of primary health care not only was captive of the hegemonic, biomedical model and functionalist public health model, but also it selectively reduced health services to a minimum for the most impoverished populations in societies. Primary care became transformed into a myth and a symbol of seduction of an all-encompassing strategy that claimed to achieve its ends as soon as it was correctly implemented.
Moreover, during the last decades of the Cold War (late 1960s to early 1970s), the United States found itself in a crisis of its own world hegemony. It was in this geopolitical context that the concept of primary health care advanced. New proposals for health and development arose as postcolonial theories after 1945. In his 1969 book Health and the Developing World, John Bryant questioned transplanting hospital-based health systems to developing countries and the lack of an emphasis on prevention. 28
These notions of development are based on a theory of stages, which is a huge illusion that normalizes the idea that nation-states and societies exist in development and each will end up more or less the same, except some will advance faster or slower. This is an alibi for self-deception that seriously implicates health systems.
Carl Taylor, founder and director of the Department of International Health at Johns Hopkins University, edited a book that offered rural medicine of India as a general model for other less developed countries of the Global South. Another important influence was that of Kenneth W. Newell, staff member of the World Health Organization since 1967, who compiled and reviewed the experiences of auxiliary rural health workers in countries of Africa, Asia, and Latin America. In 1975, Newell made the argument in Health by the People that “common health problems derive from parts of society itself and that a strict health sectoral approach is ineffective”. 29 , p. x (preface) Moreover, the Canadian Lalonde Report 15 supported the concept of health beyond services. Another important influence for primary health care came from the study of the experiences of barefoot doctors of China and that of Christian missionaries. The Christian Medical Commission, a specialized organization of the World Council of Churches and the Lutheran World Federation, was created in the late 1960s by medical missionaries who worked in developing countries. The organization emphasized the education of rural, lay health workers equipped with essential medicines and simple methods. It deserves mention that both Bryant and Taylor were members of the Christian Medical Commission and in 1974, they formalized a collaboration with the World Health Organization. There were also emerging work from models of social participation in health in which biomedical knowledge was applied to populations by rural health promoters. What was taking shape was the origin of primary health care from an international geopolitical system of cooperation toward development that was imbued with the conception that health and development was based in its own classic principles and body of thinking, including human rights, participation, and traditional intersectorality, among others. In 1973, Halfdan T. Mahler from Denmark was elected director general of the World Health Organization and brought with him this epistemology to the Alma Ata conference. Primary health care is still enshrined today in its all-encompassing thesis—totalizing—and rallying banner that influences global movements and the discussion and policies of big capital, including proposals of the World Bank. They are blind to that which they do not see.
In this brief article, from the standpoint of Latin American critical thought in health, we propose a complete rupture with the myth of primary health care and advocate toward Integrated Care for Health and Well-Living: care instead of treatment; integral instead of primary—and a strategy centered on the territory and territoriality of ways of collective life or the “community” in indigenous nations; and health and well-living with the understanding that health is intertwined with life and nature as central elements.
In regard to territory, 24 understood as the space where life is developed and health is socioenvironmentally constructed, Integrated Care for Health and Well-Living should be the center of a health system that advances policies for the promotion of well-living. In this territory, modes of life and processes that either promote or impair collective health are expressed, and, consequently, they reconfigure the architecture of the system. The health establishments should be territorialized with a population that is aware and actively participates in the design of its policies and strategies directed at holistic health care, not solely the social damage called “disease.” The health care teams in this territory provide community-based encounters of an ecology of knowledge, rather than develop centralized, vertical programs with instrumental community participation, which are tell-tale signs of health colonialism. Hospital establishments will still remain to provide comprehensive (integral in Spanish) responses to situations that merit specialized interventions, but under another management and government of progressive health and life care.
Finally, in this transformation, theorization about universalism in the twenty-first century—not born of Europe—becomes apparent. A critical review of universal and intercultural health systems is implicitly part of constructing new knowledge and action that involves socioculturally determined health and life as the foundation of intercultural, decolonized universalism in the Global South. For Latin America and the Caribbean, this new knowledge and new actions are both a theory and a strategy. The organization of universal systems is more than an end; it is a strategy to confront structural inequities by social class, race/ethnicity, and gender. This begins with the understanding that universalism is not a simple perspective of universalizing biomedical treatment, restorative medical services, nor top-down public health aiming to control populations and their risk factors. Rethinking universal and intercultural health systems as a strategy does not assume a unique and all-encompassing truth for health, but as intercultural, territorial, democratic, and aligned with the local and regional culture. A review of the current experience of the Unified Health System of the Plurinational State of Bolivia is a nucleus of new learnings for theories, policies, and practice about health systems in the Global South.
Another key component of a new categorical framework 3 is incorporating intersectionality of black and decolonial feminisms, which intertwines class, gender, race/ethnicity, and territory. This avoids making the error of managing each in isolation or as additive effects, which is often how these categories are treated in the fashion of liberal intersectionality. Their intertwining is fundamental to reinforcing the ability to provide complex and transformational explanations of sociocultural and socioenvironmental phenomenon.
Definitively, the effort to construct universal and intercultural health systems in the twenty-first century, which contemplates and acts in the sociocultural production of health, first considers its units of analysis, performance, monitoring, and in the scale of territorialization and intervention. Of course, much uncertainty and discussion leading to resistance or rejection will accompany abandoning the reproduction of models and modeling of treatment-oriented, universal or compartmentalized health systems applied to supposedly homogeneous societies with full employment and standard classifications of the processes that govern disease and death. Moving toward democratizing know-how, decolonizing theory and practice, rethinking health from the territories of putting care above disparate epidemiologic patterns, assuming a strategy of health sovereignty to respond to the needs, problems, and priorities of health all imply autonomy in the periphery. 30 Abandoning Eurocentric thinking and practices in public health and developmental social medicine is not free.
Guided by dynamics of transformation, the new order will be rebuilt taking the old into account and founding principles and institutionality. Refounding strives to be an alternative current to the thinking of the Global North. Refounding includes alternative frameworks that sustain the reinvention of political and health education and critical epidemiology in the Global South. The categories of the refounding and decolonization of health systems are:
Epistemology of health from the South and health sovereignty Universal and intercultural health systems in the twenty-first century Integrated Care for Health and Well-Living Territory and new territorialities; cartographies of systems-networks The public as a sphere and new organizational health architecture to universalize collective goods, with an integrated and interdependent characterization Political economy of health, political ecology,
31
and critical geography
32
Democratization of managing and governing in health Monitoring the intersectionalities and determinants of health
A Transformed and Socially Determined Epidemiology
Breihl in Critical Epidemiology and the People's Health 4 has argued for an epistemological break with classic epidemiology. Critical epidemiology seeks to elevate the determination of health as a different way to view health, which includes society's relationship to nature, the learnings and intercultural and spiritual health episteme of Abya Yala, social reproduction, and the collective modes of life (not lifestyle). This approach gives new meaning to the variables of person, place, and time of classic epidemiology, to produce epistemic and methodological transitions: converting them to social class, decolonized and de-patriarchal gender, ethnicity, and history in the context of health, disease, and health care.
From this critical epidemiology and the social-cultural frame of the South, the determinative process conceives health and disease as the consequence of the social production of health and sociocultural reproduction, which originates at the interior of society as links of many ramifying, complex chains of life. The determinative process considers that health in populations is determined by the material conditions of existence, especially by those processes by which society generates its means of subsistence and the accumulated colonial/geopolitical hierarchical orders determinants of health and life in the South. Health is reproduced as a set of hierarchically ordered conditions that mirror the asymmetries of colonial, racial, gender, and geopolitical power, which are spatially projected throughout the South and which impact health. Through critical epidemiology, health and disease are not considered isolated events, nor biological phenomena, nor a social “health state” in the still-used 1948 definition of the World Health Organization as a “state of complete physical, mental, and social well-being.” 34 On the contrary, we point out that health-disease is a complex and dynamic sociocultural process that forms part of the flow of life, is configured in temporal scales and contexts (society, community, the South), and can only be understood in light of the concrete conditions in which groups of human beings are born, live, and work. This social process encompasses the relations of power and colonization that maintain dynamics of exploitation, exclusion, and asymmetries, which manifest themselves in differential processes of living, working, getting sick, and dying. These conditions and flows of life, which change over history, explain how and why some people, families, groups, and societies experience morbidity, premature aging, premature death, and dysfunctional epidemiologic patterns at the intersection of social class, race/ethnicity, and gender.
Socioculturally determined processes means that health-disease not only concerns biology, individuals, and clinical medicine; nor is it the sum of collective diseases by virtue of an additive logic that turns individuals into so-called populations in which public health operates. Rather, health-disease is the manifestation of concrete social processes crisscrossed by complex dimensions of economics, culture, environment, politics, and biology that are differentially expressed in the range of social classes, race/ethnicity groups, and gender. These form the foundations and signs in societies, or community in the overriding vision of Abya Yala.
All health issues have an unescapable socioenvironmental dimension. Health corresponds to historical conditions and can only be understood if its context and situation can be taken into account (not risk factors alone), including levels of study, understanding, and action overseen by a complex and multidimensional process. 35
The theoretical commitment with the process of socially determined health and disease demands the development of theoretical and methodological focus that allows the systematic study of human groups and reveals its structures, dynamics, and sociocultural processes that act outside the appearance of clinical evidence of biomedicine, or inequalities based on academic criteria driven by funders.
Without doubt, since the 1990s there has been a revitalization of social epidemiology with an Anglo-Saxon trajectory that advocates the collection of empirical data and large databases that fosters a near monopoly of the theme of inequities. We call it modern culture “BINGO”, exemplified in critiques of Oxfam as “Big International Non-Government Organization (BINGO)” that addresses symptoms rather than the underlying causes of health inequities. 33 As well-described by Almeida, 18 modern epidemiological thought is updated over the base of two explanations of the social genesis of health-disease-health care. First, in North America, the concepts of social capital, vulnerability, social risk, and psychosocial stress are employed. Europe uses concepts such as social stratification, social cohesion, and lifestyles. It is worth mentioning that the referential theory of social epidemiology has been and continues to be meager and lacks a theoretical-conceptual view or a complex epistemology. Thus, the dominant perspective of the epistemologies of the Global North, in synthesis, is positioned among the theories of justice of John Rawls 36 and its main derivative by Sen, 37 which reflects a post-World War II theory of human development and social well-being, perhaps better encapsulated as new social welfare theory. The theoretical reflection about economic inequalities and fairness has overtaken the classic research of the social determinants of health in the Global North and wields much influence in the Global South. Eurocentric and Pan American thinking on health migrated from a classic epistemology of economic development (e.g., economic growth and gross domestic product per capita) and, since the 1950s, it has permeated the field of health as it turned toward the epistemology of welfare (human development). Even more contemporary is the movement toward a liberal epistemology of social risk management and resilience. Confronting this thesis of development from the Global North––which imposes determining hierarchical orders, coloniality, and dependence in the reach of global epidemiology to the local—is critical Latin American thought in health. It seeks to make visible and critiques both the fallacy of economic-centric development and social welfare as if it were a type of export industry in which the illusionism of development is constantly updated in the Global South. 38
In contrast to the traditional focus of public health, which analyzes populations as an additive aggregate of individuals or artificial groups according to their morbidities, critical epidemiology recognizes the limitations of statistics in its focus to scientifically quantify and instrumentalize what is actually qualitative. It gives an accounting of essential attributes and the processes of the collective health in a society and considers that both populations and institutions should be regarded as complex social organizations whose attributes are not the summary, but the dynamic result of interactions among individuals in the group—thus, a collective and its forms of producing, reproducing, and living. In other words, in place of considering populations as aggregate statistics of individuals or pathologies, critical epidemiology suggests the focus on human groups as heterogeneous and changing social organizations, with identities, conditioning contexts, cultures, territories, and territorialities in their life histories and situations. This implies, in large measure, an exit from the modern scientific method which reduces the whole to component parts and afterward sums the parts in order to explain the whole.
Undoubtedly, modern scientific thought is the founding basis of the gears between clinical biomedicine, functionalist public health, and the geopolitics of Pan Americanism and liberal global health.
According to critical epidemiology, 35 the material conditions of existence, racialization and social interactions given to a group is what determines the processes in human life that are protective or destructive. For this reason, we emphasize the importance of understanding those historical conditions of social production and sociocultural reproduction, which configure and end in the patterns of health-disease in a population, community, and society. This imposes on researchers the challenge of familiarizing themselves with the theories and methods that come from social sciences, philosophy, and the science of the complex, and that function as other epistemologies dwelling necessarily in an ecology of knowledge.
This knowledge and these techniques and methods have been excluded in traditional health and health policy education in favor of a positivist, dominant paradigm. In practice, traditional epidemiology has reduced the explanation of processes that produce health or disease to isolated social determinants, which have been incorporated into the normative, functionalist discourse of health as if it were a hashtag repeated over and over again as a listing of risk factors or implementation manual to understand the essential functions of public health.
These restrictive frames of understanding culminate in proposing policies, strategies, and interventions centered on the care of isolated individuals, affected by the damage and their lifestyles at a singular level, and centered on behavior with a hyper-behaviorist logic that transfers responsibility to the subject. Public health programs become the focus of isolated and unmoored social determinants, which are treated as causal risks disconnected and functionally apart from the processes that determined them (e.g., water quality, housing, race, occupation).
Dehumanizing social exclusion, racialization, and increasing ecologic destruction are perhaps the hallmarks of twenty-first century capitalism in its fluid, cognitive, and financial expressions, and serve as the main structural dimension of expanding epidemiological crises. 35 Classic, functionalist public health and epidemiology confuses or oversimplifies the meaning of socially determined health as an explanatory category with social determinants. Classic theories are isolated, unmoored, and outside of sociocultural, situational, geopolitical, colonial, and spatial context.
As a first approximation, socially determined health generates an understanding of the articulation among biological, social, and natural processes. Suppose that the biological, social, or natural are not mutually exclusive nor contradictory dimensions, but rather they join, interlace, and subsume each other. In determining biological from social, or social from natural, a fundamental concept is in play: subsumption. Biology has its own life, laws, and principles, but it is subsumed by the social and natural, which constitute a higher and determining plane. The connection among biological, social, and natural cannot be reduced to an external link, like a factor, or something natural or catastrophic, but rather as an essential, internal nexus. The process of health-disease is thus given in the ways of living and working, with general, particular, and specific determinations, in patterns where the biological is subsumed to the social. 11
The patterns of interaction of humans with nature have varied throughout history. In the cognitive, globalized capitalist world, extractionism converts nature in an accelerated way into commodities and massively extracts common goods that are incorporated into a global market of increasingly rapid financial valuation. That accelerated conversion of nature into commodities disrupts the harmony of ecosystems, a phenomenon that Harvey has called accumulation by dispossession. 39 The subsumption of nature and work by the principles of capitalism, colonialism, modernity, and profit motive disrupts the harmony with nature, and it is strictly related to the creation of socioenvironmental disasters, including pathogenic jumps in epidemics and pandemics, and new patterns of health-disease in the exposed populations. A variety of examples illustrate this process, among them the model of intensive agriculture and open pit mining prevalent in Latin America. Agroindustry promotes crop monocultures and the intensive use of herbicides and pesticides, which convert food production into a business where nutrition ceases to be a necessity of life, but rather is valued for its (foreign) exchange potential—a commodity that is incorporated into the global market as a function of its economic return. An illustrative case of the irrational interaction with the environment is the indiscriminate use of antibiotics in factory farm meat production, which is estimated to consume 50 percent of the world's antibiotics. This carries the risk of ingesting antibiotics in foods and, consequently, facilitates bacterial resistance in the population. 40
The disruption of social metabolism and the nature-society harmony combined with the imposition of unhealthy, inequitable, and hyper-consumerist lifestyles creates a deleterious impact on health and life at a collective level, which is expressed in several ways. One of the most important is the process of epidemiologic accumulation, in which the health of society is threatened by multiple deleterious processes that degrade health and create a pattern that hybridizes health and disease. Even though in Latin America we continue to confront problems rooted in an excess of social precariousness and infections, we also experience the accumulated hazards from historical physical, chemical, and biological exposures as well as new problems associated with new technologies and products. We also face dehumanizing and rapidly accelerating urbanization, robotics, automation, destruction of nutritional sovereignty, irrational exploitation of nature, massive poverty, structural unemployment, marginality and social exclusion, sedentary lifestyles, malnutrition, epidemic of racism, and the work process in the increasingly dehumanizing peripheral dependent upon capitalism and consumption of products that are toxic to health, the ecosystem, and human life.
Understanding those levels of general, particular, and singular in sociocultural processes of health that are joined and entwined substantially changes the way of thinking and doing in the field of health and care of life. Western positivist science fragments, individualizes, and artificially partitions what it studies. It also focuses its conduct on finding minimalist and reductionist dynamics. 2 Certainly, it is important in this theoretical framework not only to impart the need to go beyond linear thinking and the reduction of health to a set of isolated factors, but to move toward a complex and multidimensional social process, 41 which accomplishes a critical review of biomedicine and public health in order to reframe the categories and conceptual frameworks of Latin American critical thought on health and critical epidemiology.
The last theorical and practice considerations are an exploration of the contributions and approaches of critical epidemiology from Latin America and the Caribbean. These are built on the many contributions of Laurell, 42 Samaja, 43 Almeida Filho, 41 Breihl, 2 and Basile, 23 among others. These theoretical and practice considerations represent expressions that span social medicine and collective health from Brazil of the twentieth century (both also traversed by Eurocentrism and Pan Americanism) toward the new contributions and recasting (ruptura in Spanish) of health from the Global South to the knowledge system of well-living of nations of Abya Yala. Epidemiology is a field in dispute 2 over how to speak and act about health, and this dispute obeys the relationships and geopolitics of power and knowledge, social interests, subordination to linear, positivist science, functionalized to various mandates of the contemporary world system. 7 According to Brielh, “Health comes and goes dialectically among the dimensions of general, particular, and singular: it is reproduced from the general to the particular, and is created from the particular to the general. In the process it experiences forms of subsumption in which the processes of the simplest dimension develop under the subsumption of the more complex. Therefore, it appears that the relationship between the social-natural or the social-biologic occurs as a movement among the parts of a joined whole, which is its essence”. 2 , p. 13 The discourse of traditional, empirical, functional epidemiology operates with the categories of person, place, and time, but reduces persons to the variables of age, sex, and, occasionally, race/ethnicity (only as skin color), and occupation in an additive logic of artificial sums, ignoring the historical context and scales of processes in human groups. The focus of classic epidemiology limits the understanding of time to a chronological series of days, weeks, months, and years, ignoring its context of other temporal scales of disease-health processes. Place is converted to a geographical site based on administrative and bureaucratic boundaries of disease incidence, using the added scales and geopolitical categories of nation, province, department/county/canton, and municipality/city, which hides the complexity and heterogeneity that is nested within social territories and critical geographies with geospatial dimensions and multiscales.
Another foundation of modern epidemiological thought is quantify first, reflect later. Perhaps it should be necessary to first reflect and later investigate what to measure and how to do it. The because and why of knowledge of critical epidemiology reestablishes dynamics where knowledge generates action, and action generates knowledge. Broadening the frameworks of knowledge in considering new units of analysis and scales of epidemiologic observation is to assume different, complex, and contingent truths. 41 Epistemic and methodological leaps give rise to new units of understanding, new observation scales, and new temporal scales.
Another significant phenomenon is the vertiginous increase in the use of maps in functionalist epidemiology. Virtual cartography has become synonymous with managing health knowledge. As Iñiguez Rojas 44 points out, maps do not eliminate but rather they reproduce the deficiencies in health information in its units of analysis, and from biomedicalized data projected to a cartography of health. Maps can be deceptive by presenting an attractive format which glosses over concerns with data quality, they create confusion regarding units of measurement and data collection, have scales that “add and overlap,” and incorporate other deficiencies from poor understanding and incorrect application of methods to map social space and collective health. 45
Critical epidemiology joined with critical geography intends to overcome these limitations and enrich conceptualization, incorporating categories such as social class, race/ethnicity, historicity, and territoriality. Critical epidemiology also intends to focus its main content on these categories, converting each person into an active subject that belongs to a social class, race/ethnicity, gender—not as a superficial, additive sum, but pinned to a moment in history and a place in territory where life, health, and disease are produced. At the same time, critical epidemiology leaves behind the concept of risk factors, centering itself on those dynamic processes that promote and protect or damage and deteriorate health in human groups and collectivities. Moreover, it stresses going beyond the biomedical concept of the natural history of disease and incorporates the concept of the sociocultural history of health (Figure 1).
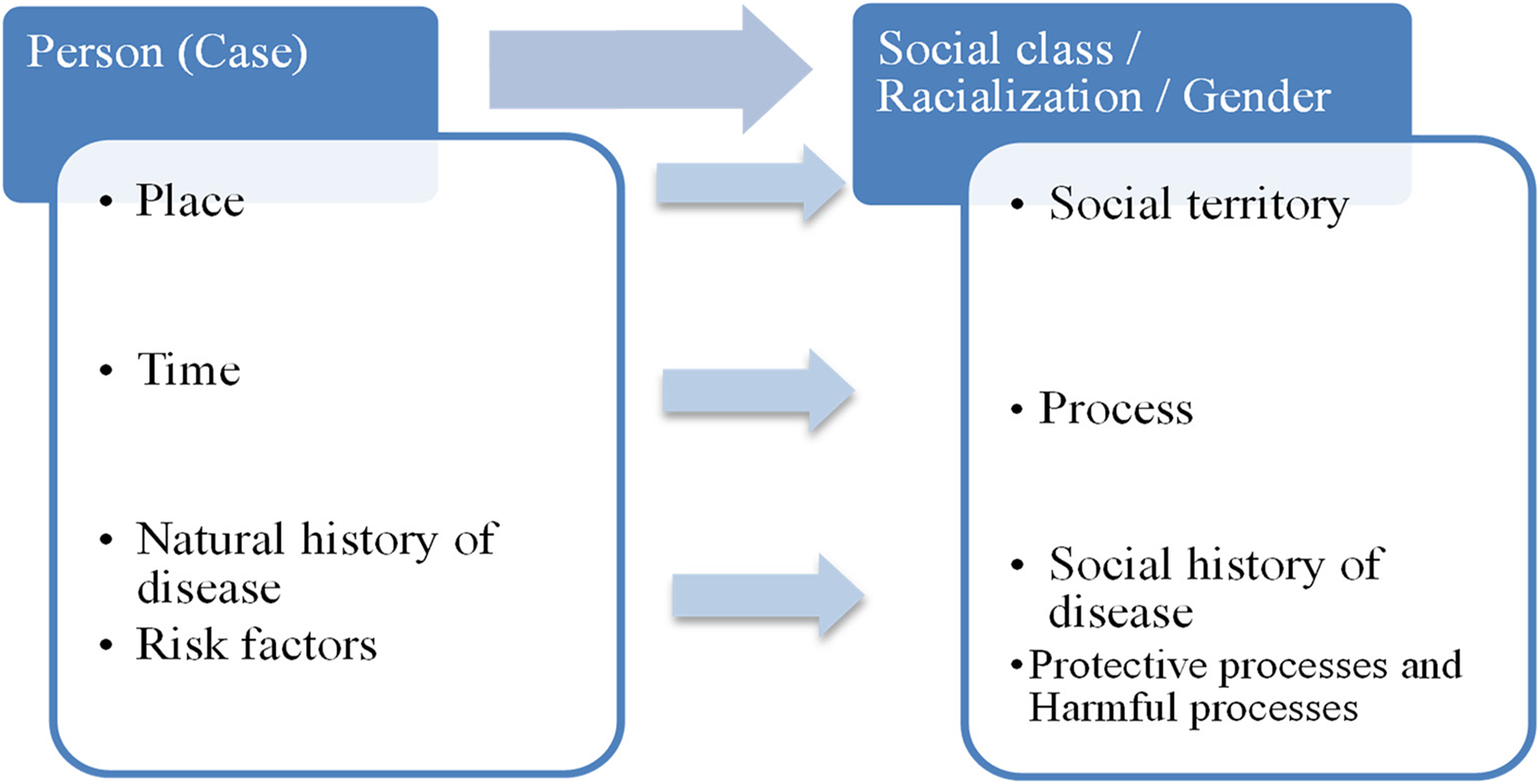
Transformation of the axes of analysis from classic to critical epidemiology.
This article introduces the need and urgency to dismantle the system of categories that are nested and reproduced in the epistemologies of the Global North without disowning the critical European tradition while seeking to substitute them with categories that express epistemologies from the Global South.
Questioning the ways in which researchers, managers, technicians, and professionals engaged in epidemiology and health go about their work is not a call to decolonize the academies nor the technical practices of the Global North. That is an exercise and effort that does not concern the South. Rather, for ourselves, we advocate for: formulating and contextualizing problems; reinventing and radicalizing the questions of research; creating methodologic focus and interpreting new findings; reviewing, understanding, and elevating alternative systems of knowledge, producing theory and policy from innovation and audacity. This also serves as self-criticism and interpellation which engages our academic practice in the South.
As the International Health and Sanitary Sovereignty Working Group of CLACSO (Latin American Council of Social Sciences) expresses in documents, these marketing movements of decolonizing global health only express a health coloniality in the twenty-first century where the Global North and its academies will explain to us how to decolonize.
In synthesis, it would appear to be necessary to review from a critical perspective in health the logic of living in a world of undisputed, monocultural, and all-encompassing scientific certainties impregnated with racialization and white supremacy as a repetitive cut-and-paste process.
A reconfiguration of knowing how we know theory, action, and policies about epidemiology, public health, and health systems in the twenty-first century is an invitation to suspend our routines of certainties, dilemmas, flowing slogans, and hashtags in order to return to the potentiality of producing alternatives of knowing-acting from the South. 20
It would appear to be necessary from critical health theory from Latin America and the Caribbean to liberate ourselves from paralysis and fears of criticizing the modern, universal, institutionalized scientific order. This entails a reconfiguration of knowing as we understand the fields of health and epidemiology in the twenty-first century. The basis of conventional knowledge with its biomedical, empirical, functionalist, and health professional-oriented characteristics has always been tied to rules of a logic of reasoning that manifests itself in a dynamic of colonial hegemony throughout the entire 20th and part of the twenty-first century in Latin America and the Caribbean. 46 It is necessary to have a strategic distance from this Eurocentric thought, including from critical Eurocentric epistemologies in order to frame and give them context. Establishing a distance is an a priori condition in order to carry out the most fundamental task of our time: think the unthinkable and expect the unexpected as an integral part of our (a) work in its epistemological, geopolitical, and methodological dimensions, and (b) ability to create critical and emancipating knowledge in the Global South. 8 From the epistemological threads among critical Latin American and Caribbean thought, we express a new current of health from the South, 38 an ecology of knowledge and systems of knowledge of Abya Yala, which offers a choice with ethical, political and epistemological characteristics to construct a critical health science for the twenty-first century from the Global South. Identifying the key points for the dynamics of reproduction from frameworks already in effect and engaging the dynamics of transformation allows us to exit from the thesis of paralysis of thinking that nothing can be done; from the dichotomy of act first, think later versus think first, act later; from the reproduction of an all-ology that describes everything, but itself is fragmented in pieces, from an immobilizing determinism, 47 from a belief in a increasing professional vanguard that aspires to a personalized monopoly of political and academic activism opposed to the complexity and polyphonics of thinking-doing health from the Global South.
Transformation also means breaking the metamorphosis of modern, abyss-creating thought (pensamiento abismal in Spanish) which involves actors, expressions, and currents within the field of critical theory of health in the territories of Abya Yala. As described by Ramón Grosfoguel, 48 abyss-creating thought concedes a universal monopoly to modern science of what is true or false, and inherently divides into dilemmas of two universes: this side of the line, and the other side of the line.
This article attempts to disseminate the processes of intersections and an ecology of knowledge among the epistemologies of health from the South from indigenous nations, social movements, governmental leaders in the periphery, and health academics of the rearguard who now seek to create new Latin American and Caribbean platforms for health sovereignty in the twenty-first century. We seek to propel a reinvention of education of health based on critical epidemiology and a refounding of health systems in a framework of epistemology of health from the South and a decolonial turn. This movement arises from necessities of theory, methods, and praxis in order to confront the intersections and bifurcations in the production of territories and territorialities of health sovereignty of Latin America and the Caribbean. These are the horizons of reconstruction of hope in the South.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.