
Abstract
Objective
This study aimed to identify and analyze failure modes associated with the cleaning–disinfection stage of reusable medical devices within the sterilization process in a dental care setting, using the Failure Modes, Effects, and Criticality Analysis (FMECA) method, in order to propose appropriate corrective actions and enhance patient safety.
Methods
A prospective study was conducted at the Dental Consultation and Treatment Center between January and March 2023. The FMECA approach was implemented by a multidisciplinary team to assess the cleaning–disinfection process. The workflow was mapped and broken down into subprocesses and tasks. Failure modes were identified using an Ishikawa diagram based on the 5M (Manpower, Machine, Method, Material, and Environment) approach. Each failure mode was evaluated according to three criteria (severity, occurrence, and detectability), allowing the calculation of a criticality index and the prioritization of risks.
Results and Discussion
A total of 24 failure modes were identified across six process steps. The overall criticality reached a cumulative score of 354, with an average of 14.75 per failure mode. Nine failures (37.5%) were classified as critical, requiring immediate corrective actions, while 37.5% were considered tolerable and 25% acceptable. The preparation of the cleaning system and the cleaning phase were identified as the most critical steps. The relatively high mean severity (2.79), combined with suboptimal detectability (2.29), was identified as the main driver of risk, rather than the frequency of occurrence. Infectious risk predominated (approximately 46%), highlighting its direct impact on patient safety. These findings are consistent with the literature and underscore the need for improved process standardization and enhanced staff training.
Conclusion
The application of the FMECA method enabled the identification of critical control points within the cleaning–disinfection process and the implementation of targeted corrective actions. This approach represents a valuable tool for strengthening risk management and improving the quality of care in dental settings. A post-implementation reassessment is recommended to evaluate the effectiveness of the corrective measures within a continuous improvement framework.
Introduction
Patient care in hospital settings, particularly within dental care centers, is associated with a significant risk of healthcare-associated infections (HAIs). Several studies1, 2 have demonstrated the potential transmission of major viruses, including human immunodeficiency virus (HIV), hepatitis B virus (HBV), and hepatitis C virus (HCV), in the context of dental care. These infections may result from multiple factors, including the healthcare environment, the patient’s health status or underlying pathology, the medical procedures performed, and the devices or instruments used. 3
According to the French National Agency for Medicines and Health Products Safety, a medical device (MD) is defined as “any instrument, apparatus, equipment, material, or product (excluding products of human origin), including accessories and software, intended for medical purposes in humans, whose primary intended action is not achieved by pharmacological, immunological, or metabolic means.” 4 MDs encompass a wide range of products, from single-use consumables such as dressings and compresses to implants such as breast prostheses or cardiac pacemakers, as well as larger medical equipment such as hospital beds.
The processing of MDs depends on their level of infectious risk, which is determined by their intended use and mode of application. Devices are classified into three categories: critical devices, associated with a high risk of transmission, which penetrate sterile tissues, internal cavities, or the vascular system (dental forceps, surgical burs, dental implants); semi-critical devices, presenting a moderate risk, which come into contact with mucous membranes, particularly the oral mucosa, or biological fluids such as saliva (dental probes, cotton pliers, dental handpieces); and non-critical devices, associated with a low risk of transmission, which do not come into direct contact with the patient (operating light, dental control panel). 3 This classification determines the required level of processing (sterilization or high- or low-level disinfection) to ensure patient safety.
Among these devices, some are designed for repeated use (reusable medical devices, RMDs) and require a rigorous sterilization procedure between uses. In the absence of appropriate protocols, these reusable devices may become potential vectors of nosocomial infections. This risk necessitates the implementation of efficient and strictly controlled sterilization systems within healthcare facilities to ensure patient safety. Proper sterilization of RMDs is therefore an essential and effective measure to prevent cross-contamination between patients. 5
Sterilization is a validated process used to obtain a product free of viable microorganisms (ISO/TS 11139:2006). The objective of preparing sterile MDs is to eliminate any risk of infection attributable to them. For a device to be considered “sterile” after the sterilization process, the theoretical probability of the presence of a viable microorganism must be less than or equal to 1 in 1,000,000 (10–6), in accordance with current standards. 6
To ensure the effectiveness of the sterilization workflow for RMDs and to guarantee patient safety within healthcare facilities, it is essential to conduct a risk analysis aimed at identifying potential failures and controlling sources of contamination. According to the French Society of Sterilization Sciences (SF2S), the main risk analysis methods used in healthcare settings include FMECA (Failure Modes, Effects, and Criticality Analysis), HACCP (Hazard Analysis and Critical Control Points), HAZOP (Hazard and Operability Study), and PRA (Preliminary Risk Analysis). 6
The primary objective of this study was to identify failure modes (FMs) likely to occur during the cleaning–disinfection stage of the sterilization process for RMDs using the FMECA method. This approach also aimed to propose corrective and preventive measures to control associated risks. Overall, this analysis contributes to the development of a structured risk management framework for this critical process.
Materials and Methods
Study Setting
This study did not require ethical approval. It represents a comprehensive assessment of risks associated with the cleaning-disinfection stage within the sterilization process of MDs. It specifically focused on instruments and equipment used at the Dental Consultation and Treatment Center (DCTC). The study was conducted over a 3-month period from January to March 2023, with the aim of rigorously documenting current practices, identifying critical points in the process, and proposing appropriate improvement measures.
Methodological Approach
The methodological tool selected for this study was FMECA. This approach was chosen due to its ability to systematically identify potential FMs occurring during the cleaning–disinfection process, analyze their consequences, and assess their criticality. FMECA not only enables risk identification but also facilitates risk prioritization based on severity (S), occurrence (O), and detectability (D), thereby providing a robust foundation for implementing targeted corrective and preventive actions. Previous studies in stomatology have demonstrated the effectiveness of FMECA in evaluating and improving sterilization systems for RMDs. 7
The overall FMECA process was conducted in nine phases:
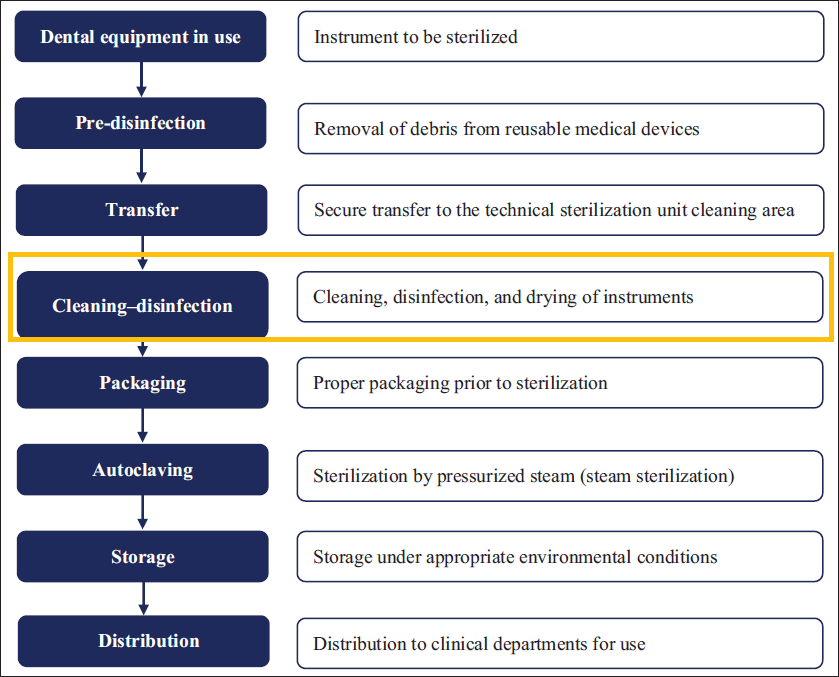
Phase 1—Sterilization workflow: A comprehensive modeling of the RMD sterilization circuit was performed within the DCTC, covering all steps from initial device use to the final distribution of sterilized equipment ready for use (Figure 1).
Phase 2—Scope definition: The study scope was limited to the cleaning-disinfection stages, starting from the reception of pre-disinfected devices from clinical departments and ending with preparation and transfer to the packaging area prior to autoclave sterilization (Figure 1).
Phase 3—Multidisciplinary team: A multidisciplinary team was established, including a professor and head of the pharmacy department, a pharmacy intern, two sterilization technicians, a dental resident, an industrial pharmacy resident, and a pharmacist coordinating the sterilization unit.
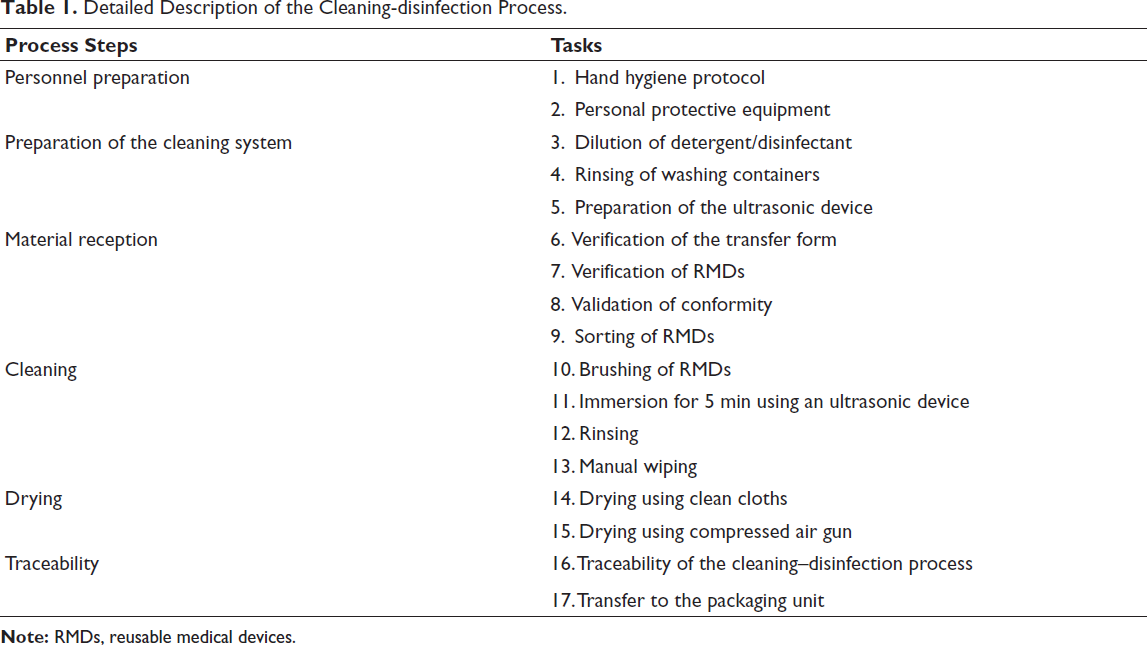
Phase 4—Process description: The team conducted a detailed and systematic observation of each step in the process, complemented by a functional analysis leading to the development of a detailed process map (Table 1).
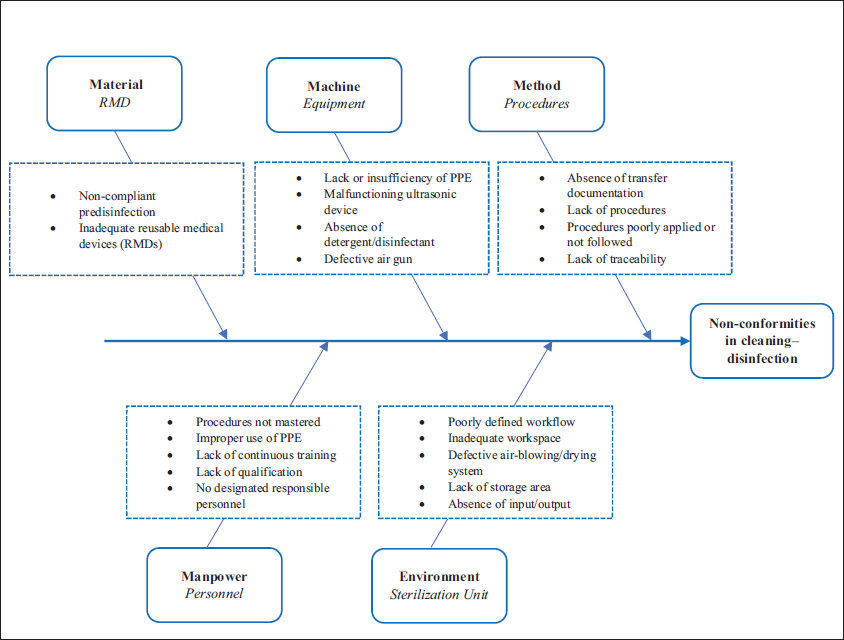
Phase 5—Identification of FMs: FMs were identified using an Ishikawa (fishbone) diagram based on the 5M (Manpower, Machine, Method, Material, and Environment) approach, enabling structured identification of potential causes of dysfunction.
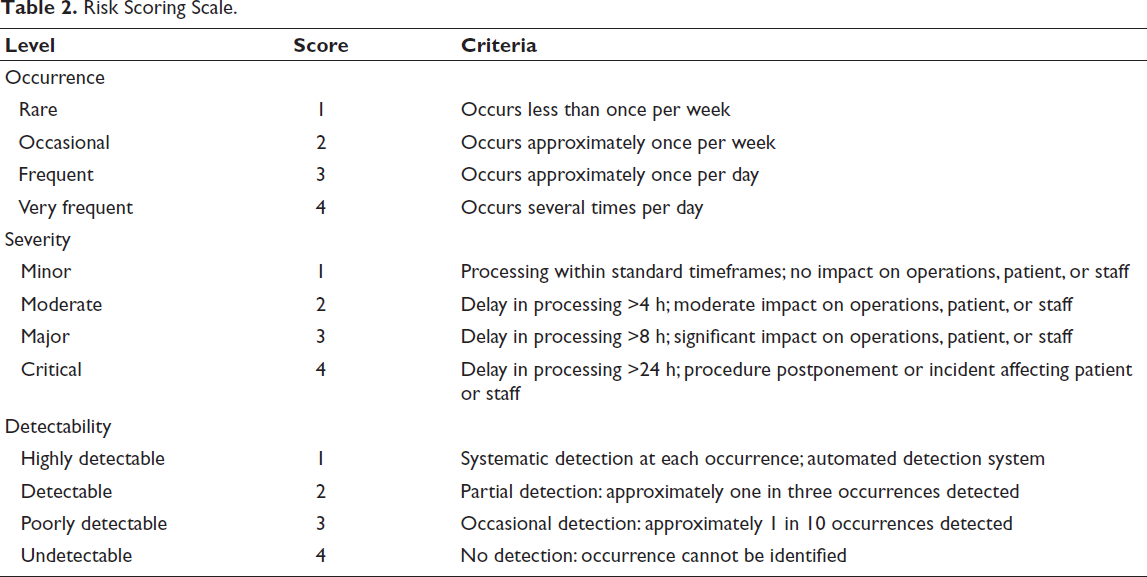
Phase 6—Risk scoring scale: Risks were assessed based on three criteria: occurrence, severity, and detectability. Occurrence reflects the frequency of failures, severity assesses their potential impact, and detectability represents the likelihood of detection (Table 2).
Phase 7—Risk evaluation: Each FM was scored, and its potential consequences on patients, staff, the environment, and system performance were analyzed.
Phase 8—Criticality index (CI) calculation: The CI was calculated using the formula CI = O × D × S. Based on these values, a decision matrix was developed to classify risks according to their criticality level (Table 3), enabling structured prioritization of corrective actions.
Phase 9—Corrective and preventive actions: For risks deemed unacceptable, a corrective and preventive action plan was developed to reduce occurrence, improve detection, or mitigate severity.
Overall Sterilization Workflow of Reusable Medical Devices Within the Dental Consultation and Treatment Center With Delineation of the Study Scope.
Detailed Description of the Cleaning-disinfection Process.
Risk Scoring Scale.
Risk Classification According to Criticality Levels.

Results and Discussion
Observation of activities within the study scope allowed the overall process to be divided into six subprocesses, encompassing a total of seventeen specific tasks (Table 1).
As part of the failure analysis, an Ishikawa diagram (Figure 2) was developed to systematically identify all potential causes leading to non-conformities at each stage of the process.
A total of 24 FMs were identified across the six stages of the cleaning–disinfection process (Table 4). Their distribution highlights a predominance in the personnel preparation stage and in the preparation of the cleaning system, each accounting for five FMs. The material reception stage included four FMs, while the cleaning phase also comprised five. In contrast, the drying and traceability stages exhibited fewer occurrences, with two and three FMs, respectively. The cumulative CI for all identified FMs reached 354, corresponding to an average value of 14.75 per FM. This level of criticality reflects a non-negligible overall exposure to risk within the studied process, thereby justifying the implementation of targeted and prioritized improvement measures.
FMECA Matrix of the Cleaning–Disinfection Process.
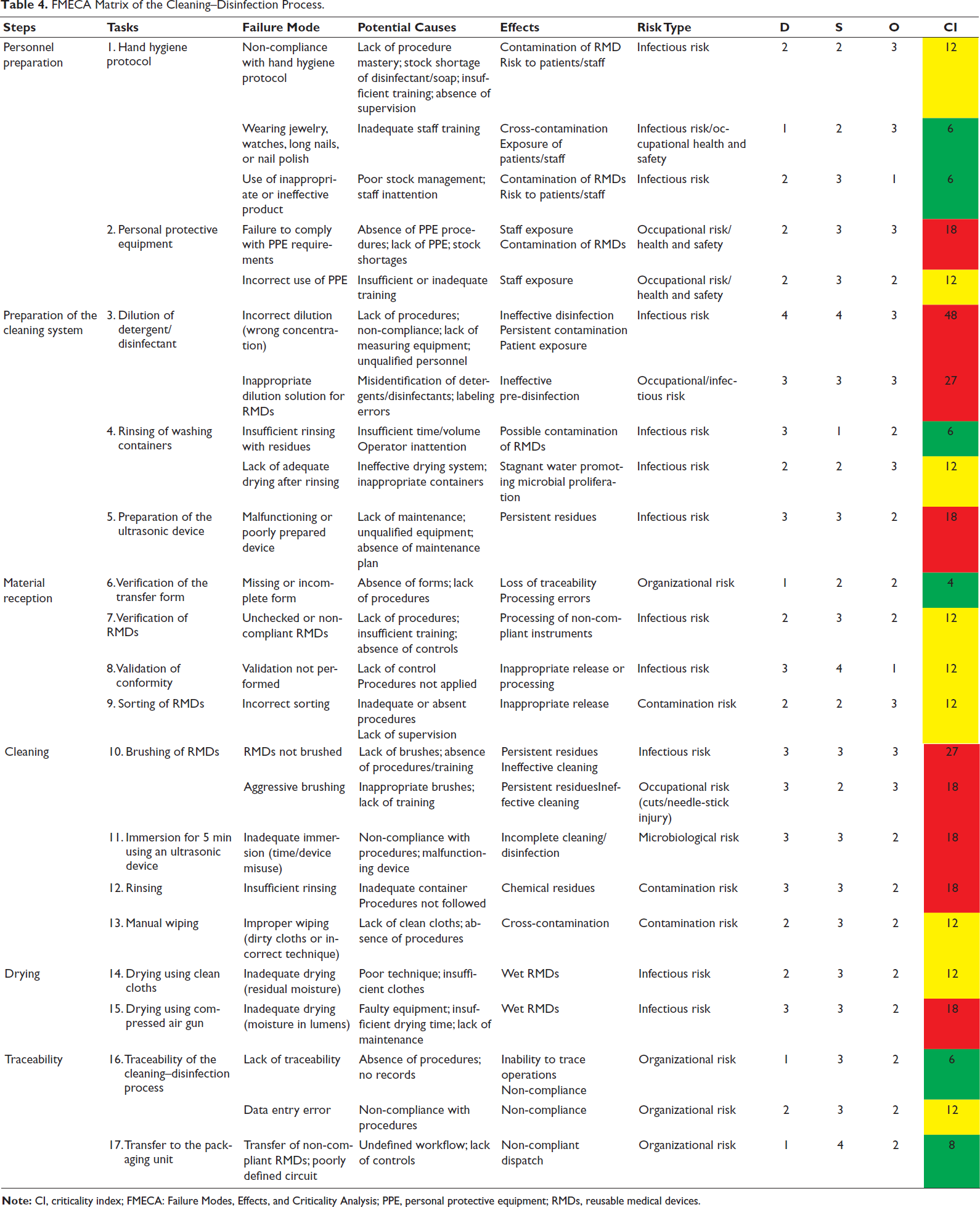
Nine FMs, representing 37.5% of all identified cases, were classified as critical and therefore deemed unacceptable. These failures carry significant consequences, potentially affecting patient safety, staff safety, and overall organizational performance and thus require immediate and prioritized corrective actions. An equivalent proportion (37.5%) was classified as tolerable; although less severe, these failures necessitate continuous monitoring and preventive measures to avoid escalation. Additionally, six FMs (25%) were considered acceptable; however, maintaining this status requires sustained efforts in staff awareness, training, and continuous improvement.
Analysis of the criticality parameters revealed a relatively high mean severity score (2.79), a moderate occurrence (2.29), and an intermediate level of detectability (2.29). These findings suggest that the primary driver of risk is not the frequency of occurrence, but rather the relatively high severity combined with suboptimal detectability. This configuration increases overall risk, as potentially severe events may not be detected early or systematically.
The preparation of the cleaning system and the cleaning phase itself emerged as the most critical steps, with the highest proportion of unacceptable FMs. These stages therefore represent key control points requiring enhanced monitoring and process control. This vulnerability can be attributed to the specific design of dental RMDs, which often contain multiple lumens and internal channels. Inadequate preparation or insufficient cleaning may lead to the accumulation of organic residues and contaminants in these hard-to-reach areas, thereby compromising subsequent steps, particularly sterilization, and increasing the risk of microbial persistence.
Consistent with previous studies on RMDs,8, 9 infectious risk was identified as the predominant risk category (approximately 46%), underscoring its direct impact on patient safety and highlighting the critical importance of controlling each stage of the device reprocessing workflow.
In response to the identified critical failures, a structured corrective action plan was developed and implemented (Table 5). This included the revision and updating of existing procedures, as well as the development of additional protocols where necessary to ensure compliance with quality and safety requirements. These measures were complemented by staff training and awareness programs aimed at improving adherence to procedures and harmonizing professional practices. The literature consistently emphasizes the pivotal role of human factors in the effectiveness of sterilization processes in dentistry. 10
Critical Fa ilure Modes and Corrective Actions.
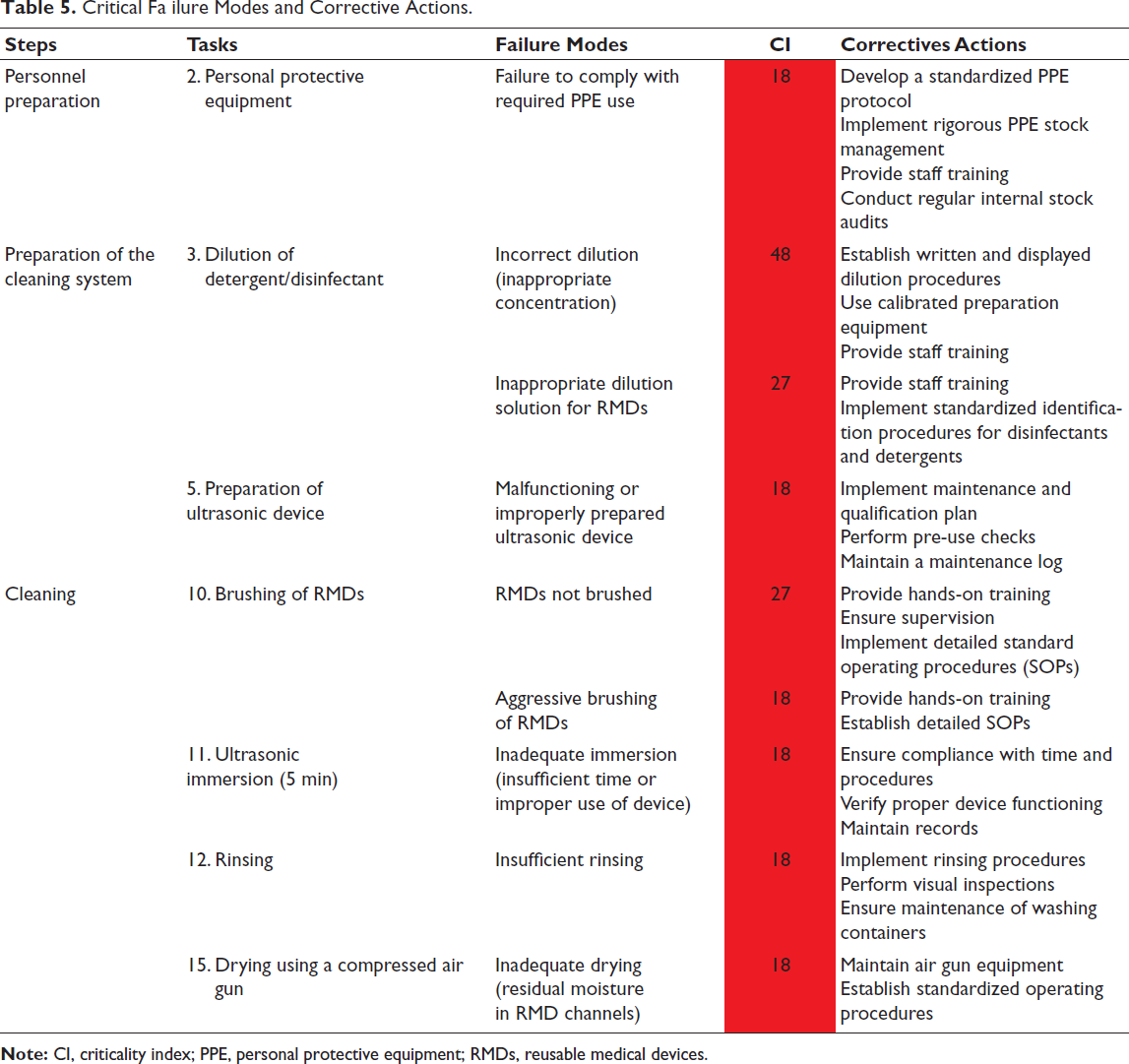
These interventions are aligned with a continuous improvement framework, which is essential for reducing risk and enhancing process reliability. A follow-up FMECA analysis would be valuable to assess the reduction in overall criticality and the effectiveness of implemented actions. Overall, these findings demonstrate the relevance of the FMECA approach for systematically identifying critical points and optimizing cleaning–disinfection processes, thereby contributing to improved safety in dental practice.
Conclusion
The sterilization process, particularly in high-demand environments such as dental care centers, is a critical determinant of patient safety and quality of care. Rigorous control of each stage, from pre-treatment to final sterilization, is essential to prevent cross-contamination and disinfection failure.
In this context, the application of FMECA to the cleaning–disinfection stage enabled the systematic identification of critical FMs and their underlying causes, whether organizational, technical, or human-related. These findings highlight significant vulnerabilities within the process that may directly affect its microbiological effectiveness and reproducibility.
The implementation of targeted corrective actions based on identified criticality levels is therefore essential to strengthen process control and improve the overall safety of RMD reprocessing. However, within a continuous quality improvement framework, these measures must be followed by structured reassessment. A post-implementation FMECA constitutes a key step to objectively evaluate the effectiveness of corrective actions, verify risk reduction, and identify any residual failures. This iterative approach is fully aligned with proactive risk management strategies and ensures the sustainability and robustness of the sterilization process.
Footnotes
Acknowledgment
The authors would like to express their sincere gratitude to all members of the sterilization unit at the Dental Consultation and Treatment Center of Ibn Sina University Hospital in Rabat for their valuable contribution to this work.
Authors’ Contributions
All authors confirm that they meet the current authorship criteria of the International Committee of Medical Journal Editors (ICMJE).
SL conceived, structured, and wrote the review. MC, JKB, SE, NB, NEK, and GM were in a multidisciplinary team. YEA and JEH contributed to critical manuscript review and enhancement of the scientific discussion. MC and SE participated in the language revision and final validation of the content. All authors read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval Institutional Statement
This study did not require ethical approval.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Human and Animal Rights
The authors declare that the work described did not involve experimentation on humans or animals.
Informed Consent
The authors declare that this work did not involve patients or volunteers.