
Abstract
The widespread adoption of PCR-based testing for Clostridioides difficile infection (CDI) has replaced enzyme immunoassays (EIA) in the U.S., increasing sensitivity and reported healthcare-onset CDI (HO-CDI) cases. However, concerns about overdiagnosis persist, as PCR may detect asymptomatic colonization. To mitigate this, some institutions use a 2-step algorithm, confirming positive PCR/GDH results with EIA. Our healthcare system, which exclusively reports PCR results, conducted a process improvement (PI) project to evaluate whether incorporating EIA testing could improve hospital reporting and patient safety. We compared our routine PCR testing with 2 commercial EIA platforms to assess sensitivity and specificity and analyzed PCR cycle threshold (Ct) values in relation to EIA results. EIA tests demonstrated less than 30% sensitivity compared to PCR, artificially reducing HO-CDI cases. Few inpatients tested by PCR despite not meeting CDI testing criteria had positive EIA results, indicating true CDI and highlighting the need for better provider education. Lower PCR Ct values, reflecting higher bacterial loads, correlated with EIA positivity, suggesting that EIA requires higher toxin expression for detection. Implementing decision-making alerts in electronic ordering improved diagnostic stewardship. While multi-step testing algorithms may reduce HO-CDI rates, they risk excluding toxin-negative (false-negative) CDI due to EIA’s low sensitivity. This approach offers limited clinical value in CDI management. Instead, reinforcing provider education on appropriate testing criteria is a more effective strategy to reduce unnecessary testing and improve patient care.
Introduction
The Clostridioides difficile infection (CDI) detection enzyme immunoassay (EIA) designed for the detection of toxins A and B produced by Clostridioides difficile, received 510(k) clearance from the FDA in 1997.
1
This marked a paradigm shift in diagnostic medicine, offering improved performance and ease of use compared to the existing gold standard Cell Culture Cytotoxicity Neutralization Assay. For over a decade, it was the preferred method in laboratories for diagnosing CDI.
2
However, in 2008, the FDA approved the first real-time polymerase-chain reaction (PCR)-based diagnostic test developed by BD Diagnostics in Sparks, MD.
3
This innovation ushered in a new era of CDI testing, leading to a rapid proliferation of PCR-based tests in the market. Due to the low sensitivity of toxin detection for CDI, healthcare systems gradually transitioned to more sensitive PCR-based platforms, making them the primary CDI testing method over the past decade.
4
However, it has been debated that molecular assays can detect C. difficile in asymptomatic individuals as well as those without infection (colonization). Our Health Care system currently uses PCR-based direct testing for Clostridioides difficile (C. diff). The aim of this Performance Improvement (PI) project is to investigate whether adopting a 2-step algorithm
5
for C. diff testing would provide any advantages for patient care compared to the current PCR-only approach. The current PCR-based test used in our laboratory, the Xpert C. difficile/Epi Assay, has been validated against the gold-standard cytotoxicity assay. When compared to direct culture with strain typing (the reference standard), the Xpert assay demonstrated a sensitivity of
As the detection threshold has lowered, a higher trend in healthcare facility -onset CDI (HO-CDI) episodes has been observed, often linked to the overuse of antibiotics that artificially increase CDI due to gut microbiota imbalance. 7 .However, recent reports suggest a potential underreporting of PCR positive and toxin negative clinically relevant CDI when using a 2-step algorithm when the toxin assay is the second test in the algorithm . 8 In addition both colonized and symptomatic patients with CDI contribute to transmission in the hospital setting 9 providing a counter point of 2 step testing.
The CDC- NHSN defines 3 main categories of CDI events: Community Onset (CO), Community Onset Healthcare Facility-Associated (CO-HCFA), and Healthcare Facility Onset (HO). 10 Our investigation focused on HO cases, defined as LabID events (positive or negative case definitions that incorporate laboratory based metrics) collected from an inpatient location on or after hospital day 4, with hospital day 1 being the day of admission. 11
Despite a clinical prompt to remind providers of these criteria once an order is placed, our HO-CDI incidence remained relatively high. Addition of EIA testing after a positive PCR result (2-step testing) for CDI has been recommended to help clinical providers distinguish between infection and colonization by improving diagnostic specificity. 12 We are not sure if the rising CDI rates are solely due to highly sensitive diagnostic modalities. This could be due to hypervirulent strains such as ribotype 027 even though they are currently in decline in US. 13
CTVHCS microbiology lab pursued a Process Improvement (PI) project to investigate whether 2-step testing could reduce our HO-CDI rates.
Material and Methods
Central Texas VA Health Care System (CTVHCS) provides health care services at 11 locations serving central Texas. Our hospitals are the Olin E. Teague Veterans Medical Center in Temple and the Doris Miller VA Medical Center in Waco. We also operate a stand-alone multispecialty clinic in Austin, and 9 community-based outpatient clinics in various small cities in central Texas locality. We serve approximately 250 000 patients in 39 counties in central Texas. Additionally, our hospital serves a veteran population with an average age range of 25 to 80 years, which provides important demographic context for understanding the patient cohort in this study. Our central lab located in Temple TX, has been performing C. difficile testing based on CDC-NHSN C. difficile LabID Event Reporting, 14 for the entire health care system using the Cepheid® GeneXpert, an automated, multiplex real-time RT-PCR assay for the qualitative detection of C. difficile Toxin B gene from unformed stool.
Decision Support Implementation
To reduce the likelihood of detecting colonization rather than true infection, our hospital adopted stringent testing criteria and implemented decision support alerts within the electronic ordering system in April-May 2024. These alerts were designed to ensure clinical relevance for hospital-onset Clostridioides difficile infection (HO-CDI) testing. The criteria included:
Onset of diarrhea after the first 3 days post-admission
Documentation of significant diarrhea, defined as 3 or more episodes within the 24 hours prior to testing
Exclusion of patients who received laxatives or other diarrhea-inducing medications within the preceding 48 hours
HO-CDI and community-onset CDI (CO-CDI) were defined according to CDC-NHSN guidelines. 11
Sample Collection
Between December 1, 2022, and July 31, 2023, a total of 72 Clostridioides difficile infection (CDI) PCR- positive stool samples were collected and used for this study. These samples had original orders placed for CDI detection from both inpatient and outpatient settings. To maintain patient confidentiality, all samples were de-identified and assigned a chronological number pattern, eliminating the use of patient IDs. Some CDI-positive samples processed by the night shift were inadvertently excluded from the study due to accidental disposal by night shift technicians. Seventy-two CDI-positive samples and 52 CDI-negative unformed stool samples were subjected to comparison using 2 enzyme immunoassay (EIA) testing modalities after PCR test for confirmation. Due to limited reagent availability, only 52 CDI-negative samples were tested for EIA assays during the same period. Starting January 2024, the microbiology lab began collecting data on inpatient CDI orders placed, including the number tested after applying rejection criteria and the number of positive C. difficile LabID Event for comparison.
The Cepheid Xpert C. difficile Assay
This (Xpert CD assay; Cepheid, Sunnyvale, CA, USA) assay is validated to run patient samples in the lab based on manufacturer recommendation with CLIA QA/QC requirements. Briefly, the GeneXpert Dx System automates sample processing, nucleic acid amplification, and target sequence detection using real-time PCR and real time (RT)-PCR assays. It includes an instrument, computer, and preloaded software, and uses single-use cartridges that prevent cross-contamination. The Xpert C. difficile Assay, performed on this system, rapidly detects toxin-producing C. difficile in stool samples by identifying the toxin B gene (tcdB). The assay includes controls to ensure proper sample processing and PCR accuracy.
Tox a/B Quik Chek
This EIA test was run based on manufacturer’s instructions. The TOX A/B QUIK CHEK™ test (TECHLAB, Inc. Blacksburg, VA) 15 detects C. difficile toxins A and B using specific antibodies. The test involves diluting a fecal specimen, adding a conjugate, and allowing it to incubate. Toxins in the sample bind to antibodies and are captured on a membrane. After washing and adding a substrate, the presence of a blue line in the test window indicates a positive result. A control line confirms the test was performed correctly.
VIDAS® C. difficile GDH and C. difficile TOXIN A & B Assay
The VIDAS C. difficile Panel, used on the VIDAS instrument, employs a 2-step algorithm combining the VIDAS C. difficile GDH and VIDAS C. difficile TOXIN A & B CDAB assays (bioMérieux, Inc. Durham, NC) for rapid and accurate detection of C. difficile in stool specimens. The GDH assay, which screens for the C. difficile antigen glutamate dehydrogenase, offers high sensitivity, while the CDAB assay, detecting toxins A and B, provides high specificity. This combination enhances diagnostic sensitivity and specificity compared to using toxin testing alone, allowing for reliable identification of C. difficile infection in patients.
Data Analysis
The performance of the 2 EIA modalities (Tox A&B quick Check and VIDAS® C. difficile GDH and C. difficile TOXIN A & B Assay) was compared with positive and negative PCR results (obtained from the Cepheid Xpert C. difficile Assay to assess sensitivity, specificity, and overall diagnostic accuracy. In addition, CT values from the PCR positive samples were investigated for any correlation with EIA results assigning 1 for positive and zero (0) for negative using Pearson correlation coefficient: GraphPad prism 10.2.3. unpaired 2 tailed t test was used to analyze before and after CDI LabID events reported upon introducing new educational decision support alerts in the electronic order format.
Results
PCR Results Comparison With Toxin Assays
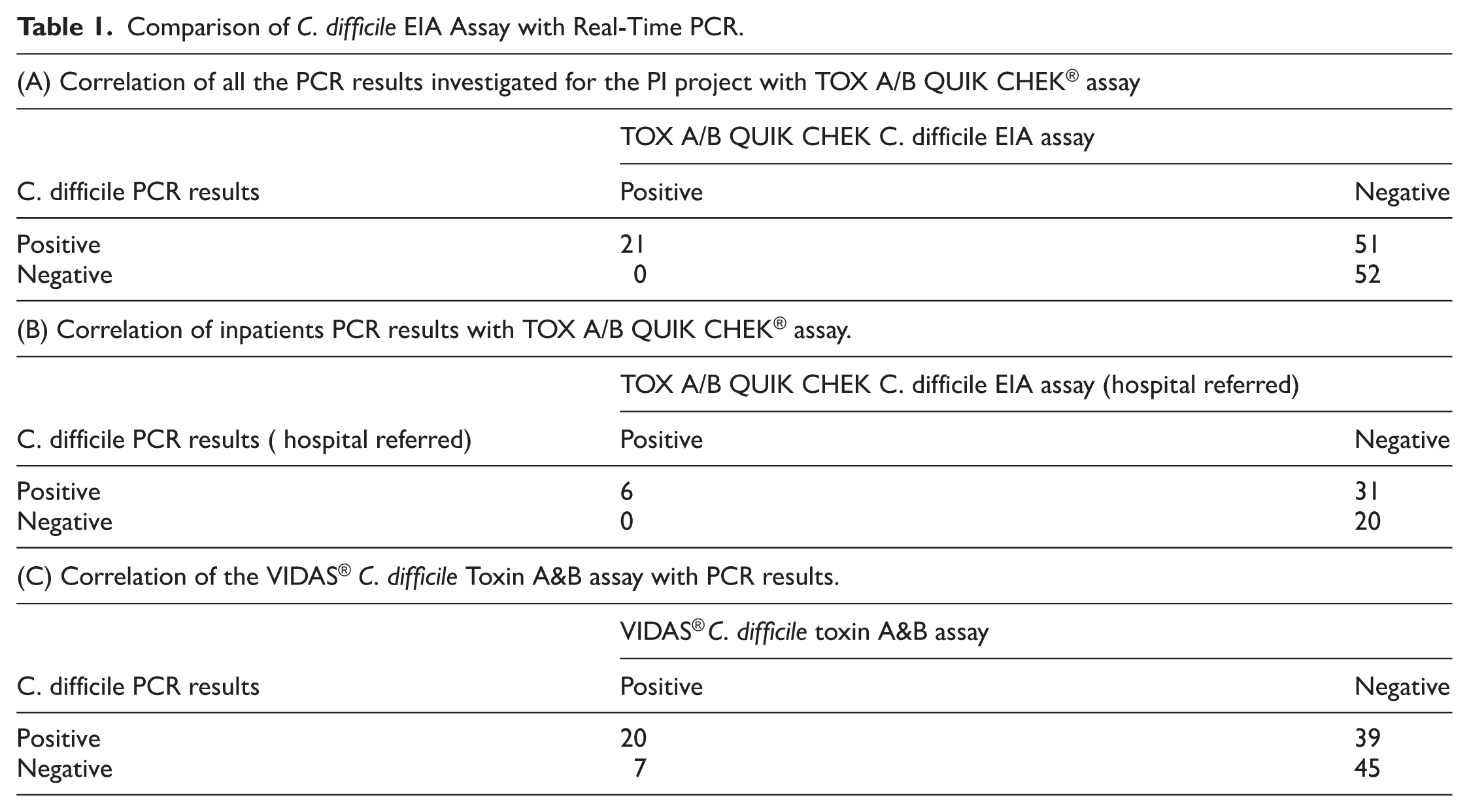
In our process improvement project, we compared 72 PCR-positive and 52 PCR-negative stool samples (Table 1A) with the commonly available toxin assay (TOX A/B QUIK CHEK® TECHLAB Inc.). We found that the toxin assay had only 29% sensitivity and 100% specificity compared to the PCR test. The toxin assay demonstrated a 50% negative predictive value (Table 1A). Calculation of the positive predictive value was not possible because we lacked an alternative gold standard to determine true positive results. Among these samples, 37 PCR-positive and 20 PCR-negative samples were submitted (Table 1B) after the patients’ admission to the healthcare facility and referred for lab testing to determine healthcare facility-onset C. difficile infection (HO-CDI). Of the 37 PCR-positive samples, only 13 were reported as HO-CDI, while the remaining 24 were categorized as community-acquired. Eight of the 13 reported HO-CDI cases did not meet criteria for testing, but due to the positive PCR test result after the third day of admission were reported as a LabID event and thus as HO-CDI (Figure 1).
Comparison of C. difficile EIA Assay with Real-Time PCR.
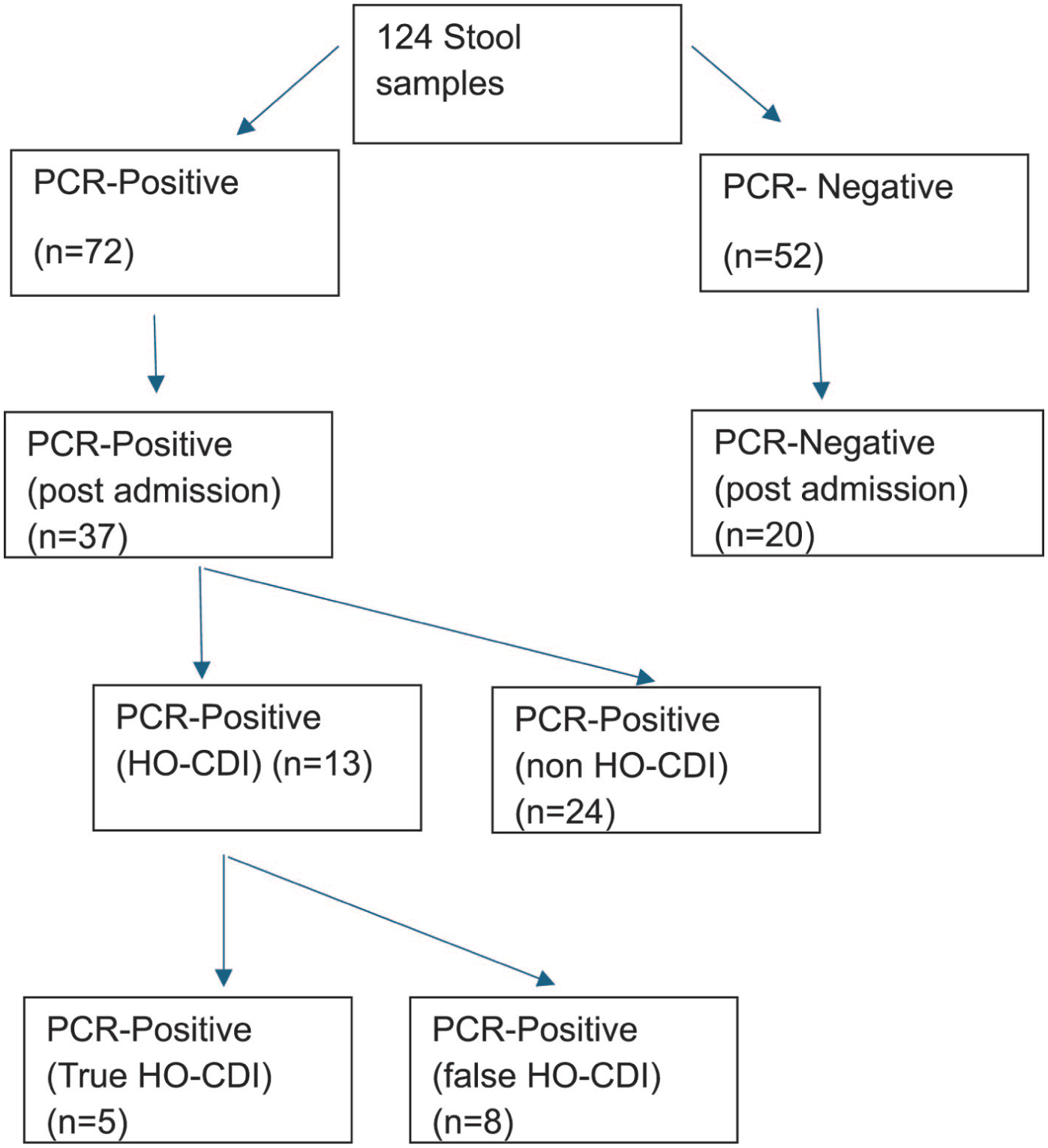
Flowchart showing stool samples tested in the PI project.
To assess whether the Toxin EIA assay could have reduced the number of false HO-CDI cases, we compared these reported samples with EIA toxin assay results (Figure 2). Among the 37 PCR-positive cases only 6 had EIA-positive results (Table 1B) making 21 samples out of testing criteria (Figure 1). Of these, 3 were from the community-onset category (Figure 2) and 3 from the HO-CDI category. Two of the 3 HO-CDI samples with positive EIA were in the group that didn’t meet testing criteria. (Figure 2).

Venn diagram illustrating the comparison between HO-CDI cases reported during the time of PI project versus cases interpreted based in EIA.
When we examined the 37 PCR-positive and 20 PCR-negative samples referred by the hospital, the sensitivity of the toxin assay for this subcategory was 16%, indicating that only 6 out of 37 PCR-positive stool samples were toxin assay-positive (Table 1B). A similar study using the VIDAS® C. difficile Toxin A&B assay mirrored TOX A/B QUIK CHEK® results, showing 33% sensitivity and 86% specificity (Table 1C). Incorporating this into a multistep CDI testing algorithm could significantly reduce the number of reported healthcare facility-onset CDI cases.
Correlation With CT Values and Toxin Assay Results
Based on the data, we observed that 2 variables (CT values of PCR and TOX A/B QUIK CHEK® TECHLAB Inc. toxin positivity) varied together. CT values below 25 were associated with a 69% positivity rate for the toxin EIA assay. We investigated the potential correlation between them and found a significant correlation coefficient (r = −.56, P < .0001), supporting the hypothesis that higher CT values decrease the likelihood of EIA positivity (Table 2). Similar analysis with the VIDAS® C. difficile Toxin A & B Assay yielded CT values below 25 were associated with a 57% positivity.
Evaluation With Positive TOX A/B QUIK CHEK® Assay Based on Ct Value range.

Decision Support Alerts at Ordering Helped Reduce Total CDI LabID Events
We compared LabID CDI reports from the 16 months before and the 12 months after implementing(April-May 2024) decision support alerts; onset of diarrhea after the first 3 days post-admission, significant diarrhea with documentation of 3 or more episodes in the 24 hours prior to testing, and exclusion of laxative or other diarrhea-causing medication use in the past 48 hours in the electronic ordering system used by providers (Figure 3) An unpaired t test showed a significant difference (P = .006). Descriptive statistics from June 2024 to April 2025 show that once the decision support alerts were implemented in May 2024, a gradual reduction in total number of inpatient testing and positive LabID events was shown (Figure 4).
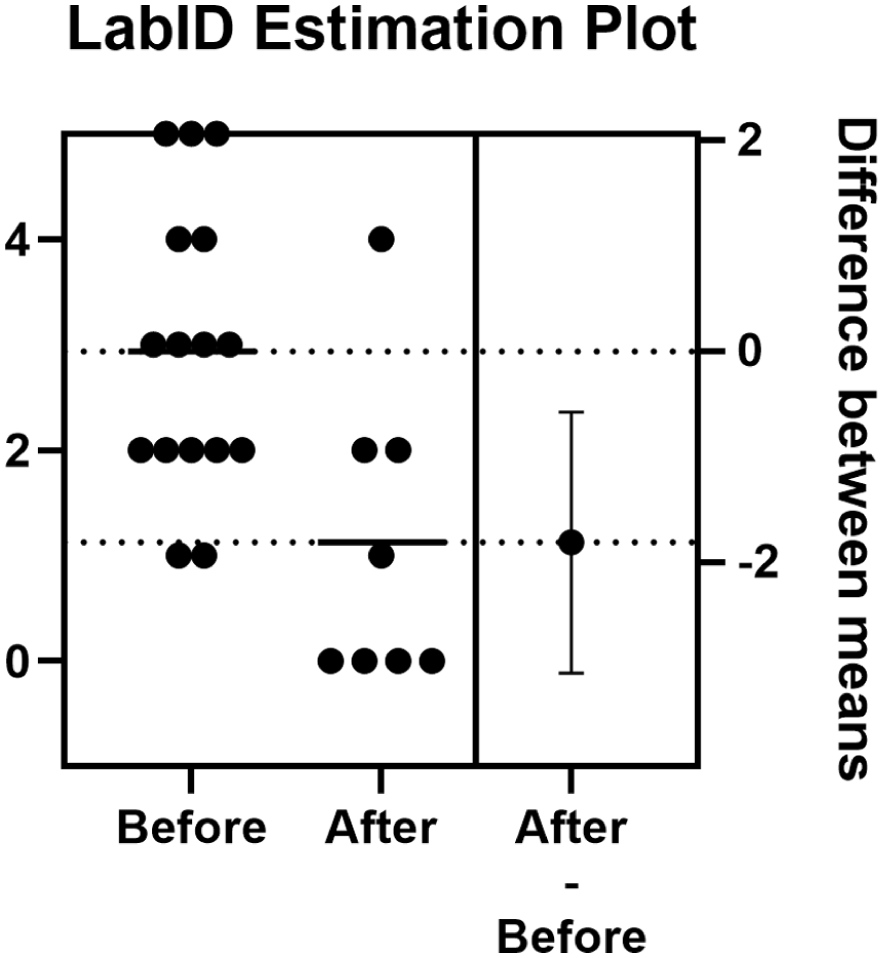
Estimation plot of 16 months upstream and 8 moths downstream upon introducing decision support alerts at the electronic ordering system.
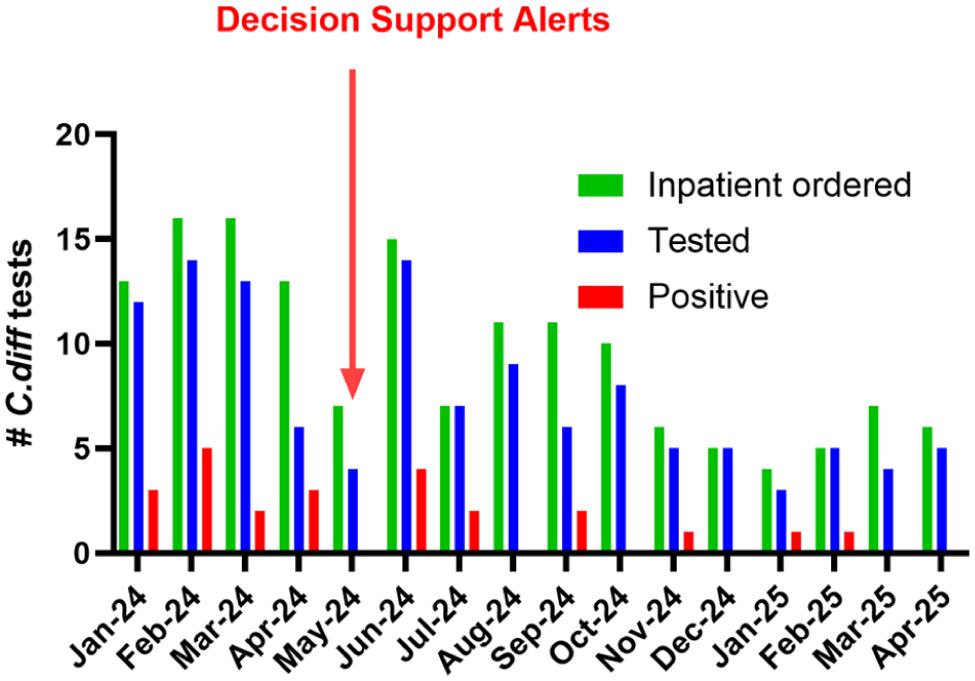
The bar chart depicts the total number of hospital inpatient orders placed for C. difficile testing and the number of tests performed after applying rejection criteria, along with the number of positive samples.
Discussion
Adding a toxin assay to PCR (2 step testing) could have reduced the number of HO-CDI cases reported by our institution. Instead of reporting 13 HO-CDI, we would have reported only 3 HO-CDI cases. However, Figure 1 shows that 5 out of 6 EIA positive patients were either not HO-CDI and or should not have been considered for testing for HO-CDI. The question arises whether this would be beneficial for patient care, as most toxin-negative patients are likely to still require CDI treatment.8,16 As mentioned in the results, submission of inappropriate specimens—those meeting laboratory rejection criteria—compromises data integrity and limits the interpretation of diagnostic accuracy. Consequently, an absolute correlation between testing results and CDI status cannot be established. CDI should, therefore, be a clinical diagnosis based on multiple factors, with diagnostic testing serving as 1 piece of the puzzle. We emphasize the limitations of a multi-step algorithm, aligning with the rationale that clinical assessment should play a more significant role in establishing CDI. 12 .
Our study investigating the correlation between PCR cycle threshold (CT) values and toxin assay results reveals a clear association: higher expression of the toxin B gene correlates with a higher likelihood of a positive toxin assay. This finding prompts 2 important questions. First, could the observed correlation be due to the enzyme immunoassay (EIA) for toxins being less sensitive and only detecting toxin levels above a certain threshold? In this scenario, only samples with a high toxin presence—reflected by lower CT values indicating higher gene expression—would yield positive EIA results. Alternatively, could it be that lower CT values are directly associated with the actual presence of toxin, rather than merely its detection by EIA? The second question, while intriguing, requires further investigation. Previous studies have reported findings consistent with our own, 17 but they also fell short of providing conclusive evidence to fully address these questions. Thus, a more comprehensive study will be necessary to explore the relationship between CT values, toxin presence, and the sensitivity of toxin detection assays. Some studies indicate that organism burden does not consistently correlate with clinical symptoms.18,19
A major criticism of PCR testing is that it cannot differentiate between C. difficile colonization and active infection. The rate of asymptomatic colonization in non-hospitalized adults is estimated to be between 2% to as high as 20% with healthcare exposure. 20 Another study suggests that asymptomatic C. difficile colonization among elderly in long term care facilities can be up to 51%. 21 A recent study by Pollock et al showed that toxin levels do not differentiate patients with C. difficile colonization from those with CDI. 16 Thus, adding EIA to PCR testing, while it may improve the number of LabID events reported, does not assist the clinician in differentiating C. difficile colonization from infection.
Several peer-reviewed publications and the CDC website highlight the low sensitivity of the toxin assay for CDI. 18 The toxin stability is controversial due to conflicting reports. A recent paper reported that the toxin degrades rapidly. 22 But its citations lack direct studies to support this except showing data for less sensitivity in Toxin EIA assays.23,24 other studies showed that the toxin is not unstable with refrigeration 25 and EIA for detection of CDI is considered less sensitive testing compared to culture and NAAT. 18 Several recent studies have questioned the validity of adding a low-sensitivity test to improve epidemiology, arguing that patient safety should take precedence.8,16,26,27 The common argument of all these publications is its validity on clinical decision making, as there is no difference between Toxin positive and Toxin negative CDI patients with regard to symptoms and complications. Concerns for patient safety have also been cited in an editorial commentary 26 recommending labs should report PCR+/Tox- results with the comment “likely represents colonization,” providing clinicians additional information to consider when evaluating the patient for treatment.
However, the 2-step algorithm helps antibiotic stewardship programs based on the current NHSN lab-based definition of CDI. Professional recommendations are in the process of transitioning to a treatment-based definition. 28 In order to support clinical decision making, a recent presentation proposed to replace the current NHSN CDI guideline on LabID events with “ Any positive test in the algorithm is reported to NHSN regardless of the order of testing” and “Additionally, treatment for C. difficile initiated within 2 calendar days of the test results will meet the definition of a positive C. difficile case.” 29
Even though it’s a small number, our own data showed that when we examined individual patient outcomes, few tested patients who could not have tested for possible HO-CDI still became EIA Toxin positive. It’s another limitation of communication and educational outreach to providers as it seems that the decision support alters were ignored on some occasions. However, when we compared before and after LabID CDI events, we noticed a significant reduction of total CDI reported by the lab indicating this educational effort is making progress. While inpatient-only CDI orders placed are shown over time, data on the number of tests performed after applying rejection criteria and corresponding positive results were only collected starting in January 2024. Due to lack of stratified data prior to Jan 2024, the number of cases in the category before May 2024 was limited, which restricts the ability to make a robust comparison. This represents a limitation in interpreting trends in test level positivity and even attribution over the full time shown in Figure 3. Another multicenter study found that 95% of patients with NAAT+ stools had diarrhea, and more than 70% of the patients with NAAT+/Tox- results received CDI treatment after clinical assessment. 8 Thus, a NAAT+/Tox- result most likely represents CDI, not colonization. There was no difference between NAAT+/Tox+ and NAAT+/Tox- patients in the incidence of severe CDI, ICU admission, pseudomembranous colitis, toxic megacolon/ileus, or colectomy. Hecker et al, in an independent study reported similar results. 27 Nicholson and Donskey in a diagnostic test interpretation commentary explained that patients with NAAT+/Tox- results may still warrant treatment. 24 A recent meta-analysis of 46 studies reported that patients who test positive by NAAT but negative by EIA have comparable risks of mortality and CDI-related complications to those who are positive by both NAAT and EIA. Furthermore, most individuals in the NAAT-positive/EIA-negative group still receive treatment for CDI. 30
These data question whether HO- CDI rates remain a useful indicator of infection control effectiveness. Rates of HO- CDI have declined following the widespread implementation of control measures, 31 and many cases of CDI now occur in patients already colonized with toxigenic C. difficile rather than from de novo acquisition. 32 Preventing CDI in this setting may require screening, proper use of broad-spectrum antibiotics, or possibly prophylaxis, but it will not be preventable by isolation and contact precautions. Using an insensitive testing method merely to improve an institution’s apparent CDI rate seems like a stewardship intervention that does not actually reduce the true burden of disease. For a small hospital setting, introducing a low-sensitivity EIA (Enzyme Immunoassay) test for C. difficile detection would not enhance quality patient care. The data shows that EIA has poor sensitivity (16%-29%) and low negative predictive value (50%), which risks underdiagnosis and inaccurate reporting. Instead, maintaining the use of highly sensitive PCR testing, combined with robust clinical decision support alerts integrated into the electronic ordering system, ensures that testing is clinically relevant and reduces inappropriate orders. This approach aligns better with patient safety, accurate diagnosis, and quality care standards.
Footnotes
Acknowledgements
No direct funding was provided for this study, and his material is the result of work supported with resources and the use of facilities at the at department of Pathology and lab. Medicine, central Texas veterans’ Health care system, Temple Texas76504.
Author Note
The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the CTVHCS, Department of Veterans Affairs or the United States government.
Ethical Considerations
This study received an exemption from ethics approval as it was conducted as a Performance Improvement (PI) project, which does not require Institutional Review Board (IRB) or ethics committee review. The project involved retrospective data analysis and did not include any patient identifiers or data that would violate HIPAA regulations. The submission was reviewed and approved by the Chief of Research at Central Texas Veterans Health Care System (CTVHCS),
Consent to Participate
No written consent is required from the patient as there is no patient identifiable data included in this article.
Author Contributions
All authors contributed to the study conception and design. Patient data and clinical description were collected by DN , JL and LW. PCR and EIA tests were performed by LW, MRSA and AB and analyzed by DN and LC. The first draft of the paper was written by DN and edited by LC. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data supporting the findings of this study are presented within the figures and tables of the manuscript. No additional data is available.