
Abstract
By encouraging doctors and scientists to improve the regulation of births through the observation of natural fertility rhythms, Humanae vitae promoted the development of natural family planning (NFP). The study of NFP has lead to NFP-based methodologies in reproductive healthcare that are promoting advances in treatment of infertility, miscarriage, and a number of reproductive health disorders. In contrast, the contraceptive mentality has stunted the development of reproductive healthcare. Humanae vitae has provided a great gift to science and reproductive healthcare that all Catholics should be proud of.
In 1968 Pope Paul VI issued the encyclical Humanae vitae. He has been hailed as a prophet (Smith 1988; Lagdameo 2008) for accurately predicting some of the negative consequences of widespread use of fertility-control methods (Paul VI 1968, n. 17). 2 In this encyclical Pope Paul VI also noted the licitness of limiting intercourse to only the infertile times of a woman's fertility cycle (n. 16). In this way a couple could space births without interfering with the fertility of any particular conjugal act. Natural family planning (NFP) is the name often given to methods that space births in this manner. 3 As a result, NFP would not be considered a fertility-control method and is in accord with Humanae vitae.
In this paper, I suggest that crediting Humanae vitae for predicting negative consequences of fertility control methods is not going far enough. Humanae vitae should also be praised for promoting what future generations will see as dramatic improvements in reproductive healthcare. These improvements are occurring because (1) Humanae vitae encouraged the development of NFP, and (2) the application of NFP-based approaches has promoted significant developments in reproductive healthcare. In addition, it will also be shown that healthcare based on a contraceptive (that is, fertility-control) mentality 4 has stunted the development of reproductive science. Therefore, Humanae vitae should also be credited for discouraging methodologies rooted in the contraceptive mentality.
So how has Humanae vitae encouraged the development of NFP? At the end of Humanae vitae there are a number of pastoral directives. The one addressed “To Men of Science” states, “It is particularly desirable that … medical science succeed in providing a sufficiently secure basis for a regulation of birth, founded on the observance of natural rhythms” (Paul VI 1968, n. 24). The pastoral directive addressed “To Doctors and Medical Personnel” states, “Let them persevere, therefore, in promoting on every occasion the discovery of solutions inspired by faith and right reason” (Paul VI 1968, n. 27). These directives encouraged doctors and scientists to develop alternatives to fertility control methods that would be based on understanding the natural fertility rhythms. Dr. Thomas Hilgers is an example of a doctor that followed this directive. He specifically cites Humanae vitae as his inspiration for developing the Creighton model of NFP (PPVI 2013) and other developers of NFP have also been inspired by Humanae vitae. 5 Even greater goods have followed from the development of the science of NFP.
According to Catholic teaching, the healthy function of our bodies is a good and noble thing. Number 364 of the Catechism states that “The human body shares in the dignity of ‘the image of God’” (CCC 2011, n. 364). Therefore, doctors who are informed by Catholic teaching, and especially by Humanae vitae, generally see the healthy function of the reproductive system as something good. They will naturally seek to better understand the reproductive system, cooperate with it, and heal its defects. In contrast, a contraceptive approach to the reproductive system sees our fertility as a problem, a disease, and a thing to be suppressed, subverted, overcome, or destroyed.
The practical effects of this distinction may be illustrated with a comparison between a contraceptive approach to infertility and an approach in union with Humanae vitae. A review of some of the details of fertility and the marital act should help bring this distinction into focus. In the womb, a five-month-old female conceptus may have up to seven million of the germ cells that will create her future supply of “eggs” (Carlson 2009, 4–5). By the time she is born, the number of germ cells will have dropped to a mere two million. At puberty only tens of thousands to hundreds of thousands of germ cells remain in the form of oocytes, which are nearly mature “eggs.” Of these thousands of oocytes up to fifty may start to mature during each fertility cycle (Carlson 2009, 13). Each oocyte suppresses the development of the other oocytes in an effort to become the lone dominant oocyte. After a dominant oocyte has been established, it will be released from the ovary during ovulation. The final result over a woman's lifetime is that only a few hundred oocytes (at most) will ever be released, out of a possible seven million germ cells. In other words, only about 1 of 1 percent of the original germ cells ever reach maturity and have an opportunity to be fertilized. Why are so many germ cells created in the first place if such a small number have the opportunity to be used for a new organism? This tremendous level of germ-cell reduction may be a selection process that ensures that only the healthiest of oocytes will eventually be ovulated. In turn, a healthy oocyte increases the probability that a healthy organism will result from fertilization.
A similar process occurs with the sperm from a man. When a husband and wife come together in conjugal union, it is normal for hundreds of millions of sperm to enter the vagina (Carlson 2009, 29). Seminal fluid will protect the sperm from the acidic environment of the vagina for approximately ten minutes. This gives sperm time to make it to the narrow part of the womb called the cervix. Ninety percent of sperm will die in this first step in their journey through the female reproductive system (Carlson 2009, 39). More sperm will be lost as they travel through the womb and the uterine tubes and seek out an oocyte to fertilize. Only hundreds to thousands of sperm will ever make it anywhere near the oocyte (Carlson 2009, 30; Moore, Persaud, and Torchia 2013, 19). This translates into less than 1 of 1 percent of the initial sperm deposited ever making it anywhere near the oocyte. As with the oocyte, this reduction of sperm numbers may be a selection process that ensures that only the healthiest sperm have the opportunity to fertilize the oocyte. In turn, a healthy sperm increases the probability that a healthy organism will result from this fertilization. With these details established, we are now ready to look at potential treatments of infertility.
For many couples struggling with infertility, in vitro fertilization (IVF) will seem like the obvious solution to their problem. The first step in this technique is hyperstimulating the woman's ovaries to promote the production of multiple oocytes. Next, sperm will be collected from the man, usually through masturbation. 6 At this point one sperm may be selected and injected directly into the oocyte in a process call intracytoplasmic sperm injection. Alternatively, a number of sperm may be selected and deposited into an area around the oocyte. After the oocytes are fertilized, the resulting embryos that are to be used for pregnancy will be transferred into the mother's womb. Embryos not used to achieve a pregnancy are typically frozen for potential future use (Carlson 2009, 36–7).
It should be noted that this process promotes reproduction without the use of conjugal union. Using the language found in Humanae vitae, one could say that IVF separates the unitive meaning of conjugal union from the procreative meaning. Humanae vitae teaches that these unitive and procreative meanings are essential aspects of the marital act (Paul VI 1968, n. 12) and that “destroying, even if only partially, its meaning and its purpose is to contradict also the plan of God and His will” (Paul VI 1968, n. 13). By promoting reproduction outside of conjugal union, IVF brings the procreative meaning outside of the conjugal act and thus would be an approach that is not in union with the teachings of Humanae vitae.
Furthermore, the contraceptive mentality present in IVF can also be seen by the contrast between reproduction achieved through conjugal union and the methods used to achieve reproduction in IVF. While healthy function of a woman's reproductive system normally produces one oocyte at a time, IVF hyperstimulates the ovaries to produce multiple oocytes. While conjugal union delivers sperm to the female reproductive tract, IVF delivers sperm to oocytes in a dish. In addition, the sperm used for IVF are normally gathered through masturbation instead of conjugal union. While conjugal union results in selection of sperm by the female reproductive tract, IVF achieves sperm selection through the choices of the IVF practitioner. Each of the IVF practices highlighted here subverts the normal process inherent in the marital act or even goes completely outside of the natural means of the body, thus treating the reproductive system as something to be overcome. Therefore, it is apparent that IVF has a foundation in the contraceptive mentality. One could suggest that IVF is a positive outcome of the contraceptive mentality if one believes that IVF is an advance in reproductive science. However, its success rate suggests otherwise.
IVF costs about $13,000 to $16,000 per attempt (Vitek et al. 2013). On average, it results in a 30 percent birth rate per IVF attempt (CDC et al. 2011, 22). The surprising fact is that IVF does not seem to have offered much improvement in overcoming infertility even when compared to treatments available decades ago. A maternity nursing textbook from 1971 suggests that 30 percent of infertile marriages can be rendered fertile (Fitzpatrick, Reeder, and Mastroianni 2009, 62). The first birth resulting from IVF was in 1978. This means that after 30 years of development, IVF may not be much more successful than treatments available 7 years before IVF existed. Studies from 1979 and 1981 of treatments for infertility due to tubal factors, endometriosis, or polycystic ovarian syndrome reported similar or higher treatment rates compared to IVF used today for the same problems (Siegler and Kontopoulos 1979; Adashi et al. 1981; Daniell and Christianson 1981; Kim et al. 2010; CDC et al. 2011, 35). 7 This evidence suggests that the contraceptive mentality, by promoting a focus on IVF, has stunted medical progress and may have even caused it to go backwards.
So how does an approach in union with Humanae vitae fare in comparison? The American College of Obstetricians and Gynecologists (ACOG) has recommended monitoring of menstrual cycles (as is done in NFP) for health reasons (AAP and ACOG 2006). I agree with ACOG that monitoring menstrual cycles through NFP should be an integral part of reproductive healthcare. One of the fundamental health benefits of using NFP-based approaches to overcome infertility is that they promote procreation by improving upon decreased reproductive function. They seek to heal defects of the reproductive system in order to enhance the effectiveness of the marital act. Since NFP-based approaches strengthen the connection between the unitive and procreative meanings of conjugal union, they are in union with the teachings of Humanae vitae. Overall, NFP-based approaches have higher published success rates (61–66%) than IVF (30%) for treating infertility (Stanford, Parnell, and Boyle 2008; CDC et al. 2011, 22; Tham, Schliep, and Stanford 2012). The increased ability to treat infertility remains even when a couple has already tried IVF once and failed (figure 1) or when compared to repeated cycles of IVF (figure 2). 8 The contrast in success can be even more dramatic when treating specific causes of infertility such as endometriosis (Campbell et al. 1995).
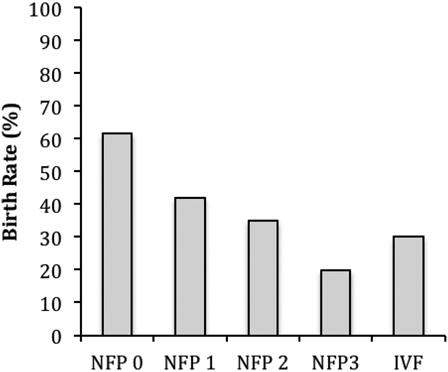
Success rates in treating infertility when an NFP-based approach is used after IVF has previously failed. NFP 0: birth rate using an NFP-based approach if IVF has not been previously attempted. NFP 1: Birth rate using an NFP-based approach if IVF has previously been attempted and failed once. NFP 2: Birth rate using an NFP-based approach if IVF has previously been attempted and failed twice. NFP 3: Birth rate using an NFP-based approach if IVF has previously been attempted and failed three times. IVF: Birth rate per cycle of IVF. This figure is adapted from published data (Stanford, Parnell, and Boyle 2008; CDC et al. 2011, 22).
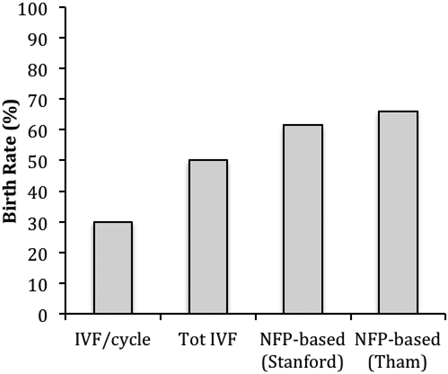
Success rates in treating infertility with IVF or NFP-based approaches. IVF/cycle: Birth rate per cycle of IVF. Tot IVF: Cumulative birth rate when all IVF cycles that a couple has participated in are included. NFP-based (Stanford/Tham): Birth rate of NFP-based based approaches from the respective citations. This figure is adapted from published data (Stanford, Parnell, and Boyle 2008; Moragianni and Penzias 2010; CDC et al. 2011, 22; Tham, Schliep, and Stanford 2012).
In a certain sense, the success rates of IVF are even worse than these results suggest as IVF doesn't actually treat infertility. When IVF-based approaches succeed, a couple has a baby, but is still infertile. This is due to the fact the IVF goes outside of the reproductive system to achieve its effect and does not heal the reproductive system as part of its methodology. In contrast, NFP-based approaches will heal the underlying pathology of the reproductive system that is causing infertility. Therefore, when NFP-based approaches succeed, a couple has a baby and is no longer infertile.
Not only does IVF have a lower success rate in treating infertility compared to NFP-based approaches, but IVF is also accompanied by added complications that are minimal or absent in normal conjugal union. Many of the complications of IVF are strongly linked to the ways in which IVF subverts the normal reproductive process. For example, the condition known as ovarian hyperstimulation syndrome (OHSS) does not arise in the context of normal conjugal union. OHSS is a risk factor of IVF that arises due to the fact that the ovaries are stimulated to produce multiple oocytes (D'Angelo 2010), unlike the situation normally promoted by the reproductive system (i.e., only one oocyte). This can lead to severe pain, blood clots, and even possible kidney failure (Brinsden et al. 1995). While ovulation may be promoted in NFP-based approaches, this stimulation is always targeted toward restoring normal ovulatory function (i.e., promoting ovulation of one oocyte per cycle) and seeks to avoid stimulating the ovaries to function beyond their natural design (Hilgers 2010, 120–1, 217). As a result, OHSS is not a risk of NFP-based approaches (Stanford, Parnell, and Boyle 2008).
In addition to OHSS, IVF also appears to be associated with an increased risk of birth defects compared to normal conjugal union (Hansen et al. 2013). While the precise cause of these birth defects is uncertain (Reefhuis et al. 2009), there is reason to believe that IVF may promote birth defects independent of maternal factors (Kelley-Quon et al. 2013). One potential explanation relates to how the oocytes and sperm are harvested in IVF. As previously noted, the reproductive system has an inherent selection process that results in making only 1 of 1 percent of potential sperm or oocytes available for fertilization. Since IVF goes outside the reproductive system to achieve its ends, this natural selection process is absent. Oocytes that would not normally be released will now be harvested from the hyperstimulated ovary. Even assuming that an IVF practitioner can select the best 1 percent of sperm for fertilization, this still pales in comparison to the natural sperm selection process. The end result is that there is a greater likelihood that sperm and oocytes will be used in IVF that would never have been used in the natural process of reproduction. It would be reasonable to suppose that some of these sperm and oocytes will therefore be less healthy and may promote increased rates of birth defects. Interestingly, infertility treatment techniques that employ the natural selection mechanisms of the reproductive system, such as intrauterine insemination and ovulation induction (without hyperstimulation), may have a lower risk of birth defects than IVF and may not even have an increased risk compared to conjugal union in fertile couples (Olson et al. 2005; Kelly-Quon et al. 2013). In contrast, while there is little published data on the prevalence of birth defects when NFP-based approaches are used, it is reasonable to suppose that these approaches would not promote increased levels of birth defects compared to normal conjugal union since promoting normal conjugal union is how these methods achieve fertility.
A final complication of IVF is the increased risk of a multiple-conceptus pregnancy (CDC et al. 2011, 25). Since IVF has a relatively low success rate, more than one embryo is usually transferred to the womb (CDC et al. 2011, 47) in order to improve chances of a viable pregnancy. When more than one embryo is transferred to the womb, there is a dramatic increase in the likelihood that multiple embryos will implant (CDC et al. 2011, 49). 9 A multiple-conceptus pregnancy is seen as a disadvantage since it increases the risk of premature birth and low birth weight (Gardner et al. 1995). In contrast, the rate of multiples with NFP-based approaches is very low (Stanford, Parnell, and Boyle 2008; Tham, Schliep, and Stanford 2012). 10 The low multiple rate with NFP-based approaches should not be a surprise since natural reproduction rarely results in the transport of multiple embryos to the womb (Carlson 2009, 54). The common theme in each of these risks is that the subversion of normal reproduction, which causes IVF to conflict with the teachings of Humanae vitae, seems to be promoting negative reproductive-health consequences. In other words, the very things that cause IVF to conflict with Humanae vitae are also resulting in practical detriments. In contrast, the NFP-based approaches do not have these negative consequences since reproduction is achieved in the context of natural conjugal union.
Another dramatic effect of NFP-based approaches is that they are very effective in diagnosing the cause of reproductive pathologies. In multiple studies NFP-based approaches have identified root causes of infertility that had not been previously identified (figure 3). Many of the couples in these studies had already tried IVF without a successful diagnosis of the cause of their infertility. Miscarriage treatments are another dramatic example of the power of NFP-based approaches. The treatments for miscarriage listed on the Mayo Clinic website include expectant management, medications to cause expulsion of the placenta, and dilation and curettage (D&C) (Mayo Clinic 2013, Miscarriage: Treatments and drugs). The medications and D&C remove the remains of the conceptus after the miscarriage has already occurred. Expectant management allows the remains of the conceptus to be expelled naturally. None of these treatments is targeted toward healing the underlying causes of miscarriage or improving the chances that gestation can continue. 11 In fact, the Mayo Clinic website suggests that there is nothing that can generally be done to prevent a miscarriage before it occurs (Mayo Clinic 2013, Miscarriage: Prevention) 12 and does not suggest testing for underlying causes until after multiple miscarriages have already occurred (Mayo Clinic 2013, Miscarriage: Lifestyle and home remedies). 13
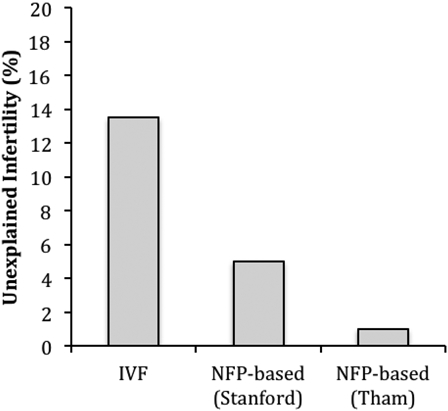
Cases of unexplained infertility after IVF or an NFP-based approach is used to treat infertility. This figure is adapted from published data (Stanford, Parnell, and Boyle 2008; CDC et al. 2011, 34; Tham, Schliep, and Stanford 2012).
In contrast, NFP-based approaches can actually predict the risk of miscarriage before a woman is ever pregnant and then provide treatment to prevent the miscarriage (Hilgers 2010, 259–69). There has been similar success in diagnosing and treating ovarian cysts, endometriosis, premenstrual syndrome (PMS), postpartum depression, and many other conditions (Hilgers 2004). NFP-based approaches are creating dramatic advances in reproductive healthcare even though there are many people, including doctors, who still do not know about them. This is an amazing gift that the Church is giving to the world, and it has been built on the foundation of Humanae vitae. Catholics should be proud of the amazing contributions to reproductive healthcare that the Church has promoted through Pope Paul VI's encyclical.
Footnotes
Derek M. Doroski, PhD is an Assistant Professor of developmental biology at Franciscan University of Steubenville, Steubenville, OH, USA.
His email address is
1
This paper was previously presented orally in an abbreviated form as follows. Doroski, D. M. Sept 2013. Response to “Scientific, Spiritual, and Marital Dynamics of Natural Family Planning.” Oral Presentation. “Humanae vitae at 45: Life, Liberty, and the Pursuit of Holiness.” Franciscan University of Steubenville, Steubenville, OH.
2
In this paper I use the term “fertility control” to refer to methods of spacing pregnancy that are designed to render infertile conjugal acts that could otherwise result in pregnancy. For example, condoms, hormonal birth control, and sterilization would be fertility-control methods.
3
“Fertility awareness method” is sometimes used synonymously with NFP although the terms can have different connotations.
4
“Fertility control” and “contraceptive” are not necessarily synonymous terms, as a fertility control method could use a method of action other than a contraceptive one (i.e., contragestive or interceptive). However “contraceptive mentality” is a term that is likely to be widely understood by readers of this journal, and its use does not change the main points of this paper in a significant way. Therefore, for ease of use, the term “contraceptive” will be used synonymously with “fertility control” in later sections of this paper. This is not intended to limit the definition of “contraception” in this paper to fertility-control methods that have a contraceptive method of action. Contragestives and interceptives would be “contraceptive” under the usage in this paper.
5
The developers of the Marquette model of NFP have mentioned their inspiration from Humanae vitae in conversations with the author.
6
Sperm could licitly be obtained through use of a perforated condom employed during normal intercourse. However, this method is rarely used in IVF. Even if sperm are licitly obtained, other steps used in the process of IVF would remain illicit.
7
Live-birth rate after tubal factor infertility was 28% in 1979 (Adashi 1979) vs. 32% for IVF in 2009 (CDC et al. 2011, 35). Live birth rate after endometriosis was 50% in 1981 (Daniel and Christianson 1981) vs. 35.3% for IVF in 2009 (CDC et al. 2011, 35). Rates of conception after treatment for polycystic ovarian syndrome was 73% in 1981 (Adashi et al. 1981) vs. 26–34% for IVF in 2010 (Kim et al. 2010). It should be noted that these comparisons do not meet the highest level of evidence (i.e., randomized controlled trials). However, it would be difficult, if not impossible, to make comparisons of this type across time with a randomized controlled trial. Comparison of similar studies is the best available evidence that we have at this point. Therefore, given the available evidence, it would seem reasonable to conclude that IVF has not resulted in much historical success.
8
It should be noted that some of these comparisons do not meet the highest level of evidence (i.e., randomized controlled trials). In some cases, comparisons of similar studies are the best available evidence that we have at this point. This evidence points to the superiority of NFP-based approaches for treating infertility compared to IVF. Another important factor to consider is that it would be illicit to do a randomized control trial that included IVF. This limits the ability of promoters of NFP-based approaches to definitively show that these approaches are superior to IVF.
9
There is a 1.9% chance of multiples when one embryo is transferred. This rate is greater than 25% (as high as 34.7%) when two or more embryos are transferred.
10
Stanford, Parnell, and Boyle (2008) reported a multiple rate of 4.5% and Tham, Schliep, and Stanford (2012) reported no cases of multiples (0%).
11
While the site does suggest avoiding known risk factors such as smoking and drinking, it offers little in terms of identifying a miscarriage risk in the general population before a miscarriage occurs.
12
The term “threatened miscarriage” is used to refer to a point at which the conceptus is alive, but in danger of miscarriage. Therefore, it could be reasonable to assume that a search for the term “threatened miscarriage” might provide information on preventing miscarriage. However, a search for “threatened miscarriage” does not bring up any further results.
13
The exact wording is as follows “If you experience multiple miscarriages, generally more than three in a row, consider testing to identify any underlying causes.” It goes on to say, “In some cases your healthcare provider might suggest testing after two consecutive losses.”