
Abstract
Purpose
To describe the integration of a medication therapy management (MTM) service in a hospital-based outpatient pharmacy, including adapting Medicare-based screening criteria to target a primarily non-Medicare population, integrating data into the medical center's electronic medical record, and designing a method to track identified drug-related problems (DRPs).
Methods
The hospital-based outpatient pharmacy at the University of Pittsburgh Medical Center (UPMC) established an MTM service to enhance patient medication safety. Identification criteria were developed in accordance with the Medicare Modernization Act of 2003 and institutional practices: older than 65 years, more than 5 chronic medications, more than 3 chronic disease states, presence of diabetes, tobacco use, or possible adverse drug event (ADE). As this was a proof of concept pilot, both Medicare and non-Medicare patients were included. Additionally, an intervention tracking form was developed to use in conjunction with the medical center's electronic medical record.
Results
During an 18-month period, 319 patients met the criteria upon random screening. Sixty-eight patients enrolled in the MTM program, resulting in 234 patient visits. One hundred and seventy DRPs were identified, with 2.5 DRP per patient. The most common problems found were the need for additional drug therapy and nonadherence. The overall physician acceptance rate for recommendations was 69%.
Conclusion
MTM programs are adaptable to a hospital-based outpatient pharmacy utilizing Medicare-based screening criteria in a primarily non-Medicare population resulting in identification of DRPs.
Keywords
The Medicare Modernization Act (MMA) of 2003 established requirements that all Part D prescription drug plans must implement a Medication Therapy Management (MTM) program as a means to improve therapeutic outcomes through improved medication use. 3 However, only general guidelines were provided to identify members who would benefit: multiple chronic diseases, multiple Part D drugs, and an annual drug cost of $4,000. 4 Although, this program targets improving medication use, the scope is limited to those who are Medicare eligible; even then, only 12.9% of the enrolled Medicare population met the criteria as outlined for MTM in 2008. 4 It is evident that medication errors occur in all populations and currently available MTM programs reach only a small percentage of people in need.
A 2006 survey of MTM programs from 70 health plans offering a Medicare Part D plan revealed that only 55% of the programs evaluate for specific drug-related problems (DRPs), 30% offer patient monitoring, and less than 20% contact a patient's provider. 5 In 2009, a review of current MTM programs found that most programs provide interventions to both the provider and beneficiary. However, the nature of these interventions varies greatly regarding the level of interaction or assessment, ranging from passive mailings, refill reminders, and drug interaction screening to face-to-face interactions, case management, and provider consultations. 4 This is in contrast to the core elements of a MTM service model as set forth by the American Pharmacists Association/National Association of Chain Drug Stores (APhA/NACDS). These elements focus on a comprehensive medication review and resolution of identified drug therapy problems, specifically medication therapy review (MTR), personal medication record (PMR), medication-related action plan (MAP), intervention/referral, and documentation and follow-up. 6
The literature shows that pharmacists are established providers of MTM in a variety of settings including community pharmacy, university-based hospital pharmacy, and academic settings.7–11 These programs are often provided to non-Medicare-eligible patients such as employees or Medicaid recipients. The inclusion criteria for these programs vary, however they may be based on the Medicare Part D MTM criteria. Limiting MTM services to only Medicare beneficiaries excludes patients who may be at risk for DRPs and resulting adverse drug events (ADEs). Traditional pharmacy services are changing to avoid these missed opportunities to improve patient care. However, it is not clear how pharmacists can best identify patients in need of MTM.
The hospital-based outpatient pharmacy at the University of Pittsburgh Medical Center (UPMC) established an MTM program to enhance patient medication safety. To target patients who might benefit from MTM, UPMC developed identification criteria in accordance with the MMA.
The purpose of this evaluation is to assess whether MMA-based screening criteria to target primarily non-Medicare patients for MTM correlates to finding a population in need as determined by identification of DRPs.
Methods
Program Description
The UPMC Falk Pharmacy is a hospital-based outpatient pharmacy located in a large, urban academic setting and is primarily utilized by health system and university employees; less than 20% of patients are Medicare eligible. The pharmacy averages 800 prescriptions a day, including hospital discharges and specialty medications (such as injectable agents). At the time of this writing, the staff consisted of 5 pharmacist full-time equivalents (FTEs) and 9 technician FTEs. The pharmacy was renovated in 2006, and a patient care room was included for the development of direct patient care programs within the pharmacy, including MTM. To target patients who may benefit from MTM, the pharmacy developed screening criteria based on those set forth by the MMA. It was determined that patients who met at least one of the following would be offered the opportunity to schedule an MTM visit with the pharmacist: over the age of 65 years, more than 5 chronic medications, and more than 3 chronic disease states. Presence of diabetes was also included as screening criteria as it was found to be the most frequent disease state among previous Part D MTM recipients. 4 In addition, 2 criteria were added to meet the goals of the institution: patients experiencing an ADE to target medication safety, and preventive services (smoking cessation, which was an institution-wide sponsored initiative).
A random screening of new prescriptions was reviewed by the pharmacist at order entry to identify patients in need of MTM. Patients meeting at least one of the screening criteria were referred for MTM. Patients were contacted via telephone; during the phone call, the pharmacist explained the program and offered to arrange for an MTM appointment.
At the initial MTM appointment, the pharmacist performed a comprehensive medication review in accordance with the APhA/NACDS Core Elements.
6
Documentation occurred via the electronic patient medical record. The physician was contacted for verbal discussion at the discretion of the MTM pharmacist who felt that the identified problem warranted immediate attention. At the completion of the visit, the pharmacist completed the MTM tracking form (
Program Assessment
At the onset of the program, it was decided that certain process measures and quality indicators would be tracked for departmental reporting purposes and to provide a means for continuous quality improvement. Process measures included number of patients who were identified for MTM, number of patients presenting for MTM, acceptance of patient and physician recommendations, and utilization of the documentation tool. Quality indicators were defined as identification of DRPs. Economic indicators were not assessed at this time.
Development of Intervention Tracking Tool
The documentation within the institution's electronic medical record would not allow for ease of tracking DRPs, so a tracking tool was developed for this purpose. The desired properties of the tracking form was that it was time efficient, did not duplicate the patient information that was within the electronic medical record, and would be able to be quantified. The final product was a check box format that could be translated to a spreadsheet (
Results
Program Outcomes
From January 2007 to July 2008, 319 patients were identified as meeting at least one of the defined criteria during the random prescription screening, thus the total number of patients screened was not documented. The percentage of patients who met each criterion is shown in Table 1. More than 5 chronic medications was the most common criterion at 66%, and 6% had an ADE identified due to the screening process.
Percentage of patients meeting criteria for referral for Medication Therapy Management (MTM) (n=319)
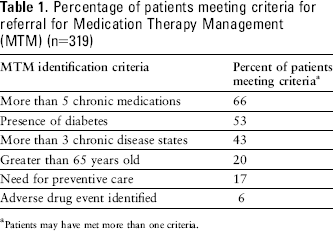
Patients may have met more than one criteria.
Of the 319 patients identified, 68 (21%) agreed to meet with a pharmacist within the MTM program. Sixty-eight percent of the patients were in the 46 to 64 year age range, with an average of 10 chronic medications. Hypertension was found to be the most common disease state. Demographic data are outlined in Table 2.
Demographics of patients receiving Medication Therapy Management
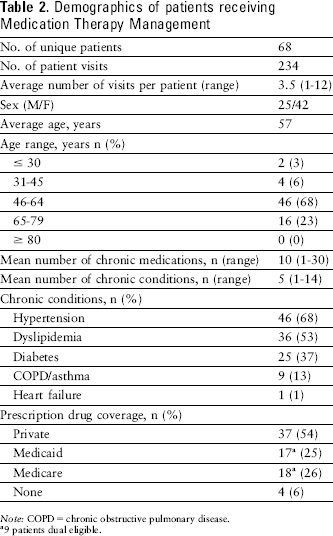
Note: COPD = chronic obstructive pulmonary disease.
9 patients dual eligible.
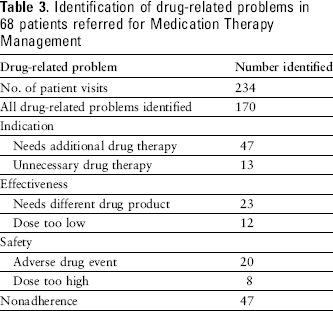
A total of 234 patient visits occurred, resulting in the identification of 170 DRPs. An average of 2.5 DRPs per patient was identified. At least one DRP was identified in 86% of patient visits. The most common problems identified were “needs additional drug therapy” and “nonadherence” with 47 occurrences each (Table 3).
Identification of drug-related problems in 68 patients referred for Medication Therapy Management
Patient encounters were documented either within the patient electronic medical record or via physician letter for 88% of visits. In addition, the pharmacists contacted the physicians via telephone on 37 occasions. When specific recommendations were made to the patient, they were accepted by the patient 96% of the time. Patient recommendations were those that did not require discussion with the physician such as lifestyle modifications (eg, carbohydrate counting for patients with diabetes), education on monitoring (eg, self-monitor blood glucose twice daily), timing of medication doses (eg, to avoid absorption issues), and initiation of over-the-counter medications (eg, use of bowel regimen for chronic opioid use).
The overall acceptance rate for recommendations made to the physician was 69%. When the recommendation was provided in a written note, 51% were accepted; when the recommendation was provided by verbal communication with the physician, 92% were accepted. The acceptance of pharmacist recommendations made to the physician allowed for resolution of certain DRPs, including the need for additional drug therapy (eg, additive benefit from dual antihypertensive therapy), the need for increased dosage (eg, maximization of oral medications for diabetes), and discontinuation of unnecessary drug therapy.
Discussion
MMA-based screening criteria resulted in the identification of 2.5 DRPs per patient in a hospital-based outpatient pharmacy MTM program. This supports using MMA criteria as a guide to identify patients at risk for DRPs in a primarily non-Medicare population. However, using only the MMA criteria may lead to missed opportunities for identifying patients at risk for DRPs. By tailoring the criteria to include diabetes, preventive care, and ADEs, we broadened our patient base to find those in need. Although the current MMA criteria would likely identify patients with diabetes, it is not likely to identify those currently experiencing a medication-related ADE or needing preventive care, such as smoking cessation, both of which would be applicable to the Medicare and non-Medicare populations.
The use of screening criteria offers one method of identifying patents in a systematic fashion. This method matched our pharmacy's need for a process that could be incorporated into a dispensing workflow of a newly renovated pharmacy, with a minimal impact on pharmacy staff time. Due to the high level of preventable medication errors, as outlined by the Institutes of Medicine, the use of differing methods will likely find patients at need as well. 1 The process outlined shows that screening patients at the point of dispensing will result in identifying patients in need of MTM without disrupting the dispensing process.
Our description also reveals a downside of utilizing this process, as indicated by only 21% of the patients identified presenting for at least one MTM visit. The low response rate was primarily attributed to the fact that the patients were contacted via telephone to describe the program and arrange an appointment, rather than engaging them at the point of dispensing, thus providing a passive means of recruitment. Oftentimes, phone contact led to leaving voice messages or being unable to reach the patients, in which case a letter was sent to provide program information. The method was initially utilized due to the needs of the dispensing workflow, training new technicians and cashiers, and frequent workflow changes due to the renovations. A screening can be used in conjunction with actively engaging the patient at the pharmacy counter.
Another limitation of the screening process was that it was a completely random process in that the pharmacists screened incoming prescriptions at their discretion, therefore variations occurred regarding the screening process. Aside from the screening criteria, the pharmacists were provided minimal direction on how or when to perform the screening. For example, most pharmacists screened only new prescriptions, rather than all prescriptions including refills. Also, some pharmacists screened only when they felt they had time, whereas others incorporated it into their workflow on a regular basis. As this was a pilot project, it became apparent that there were different levels of involvement among the pharmacists. This made it difficult to quantify the total number of prescriptions screened as the pharmacists only provided information on patients with identified DRPs and not the total number screened. This was an oversight in the implementation of the program.
Based on these findings and the acknowledgment of the benefit of face-to-face interactions, the pharmacy manager decided to change the workflow to arrange for a pharmacist to be available at the pharmacy counter at all times for the purpose of providing counseling on medications and brief interventions and to be the point of entry to arrange for MTM visits. Patients were also identified and scheduled for MTM appointments during education events led by pharmacy students, such as blood pressure screenings and medication disposal sessions, as well as during influenza vaccination clinics.
This description also outlines the tracking process for DRPs. In an institutional setting, it is important for pharmacist-provided patient care programs to be documented within the patient's medical record, inpatient or outpatient, in the same fashion as the other health care providers within the institution. First, this provides consistent communication with other providers; second, it allows the pharmacist to be recognized as part of the health care team; and third, it provides a method of patient care documentation not possible through a pharmacy dispensing system. Thus, it was decided to utilize the institution's electronic medical record, rather than one of the commercially available pharmacist-specific MTM documentation systems. It was recognized, however, that one of the functionality losses would be the ability to quantify identified DRPs. This is a decision that does not need to be made within community pharmacies, which will benefit from MTM-specific documentation systems, as there are no pre-established means to communicate patient care activities with other health care providers.
The development of a tracking form for DRPs had benefits and drawbacks. It allowed for standardization of data collection, and data were easily collated by utilizing a check box fashion. However, some pharmacists felt the form asked for duplication of information in the inclusion of a free text subjective and objective data field. It was realized that this was not needed as the purpose of the form was strictly for data collection, not patient care documentation, thus revisions of the form do not include those fields. The intent is to continue to revise the form and explore transforming it into an electronic data collection tool that could be utilized from a computer or hand-held device.
Although the purpose of this article is to describe our experience, it is important to point out limitations in data that were collected that may be rectified in evaluations going forward. This evaluation tracked only if recommendations were accepted by the physician and patient and not the impact on clinical and patient outcomes. In 47% of patients, nonadherence was found as a DRP. It would have been beneficial to collect the reasons for nonadherence (ie, forgetfulness, cost, misunderstanding). This information would assist in targeting areas for patient education programs at the pharmacy. Although we reported that 96% of patients accepted a pharmacist recommendation, this was based on the agreement of the patient at the time the recommendation was made. It would be interesting to track how many patients implemented and sustained the recommended lifestyle or medication change. In addition, this evaluation did not track patient acceptance of recommendations that needed physician approval, thus it could not be reported if a patient implemented a change to which the physician agreed. Also, the implementation of the electronic medical record did not occur until 2 months after the initiation of the MTM program. Patient encounters during that time were written on paper and faxed to the physician, thus reflecting the 88% of encounters within the electronic medical records. This identifies the importance of having all program components in place before implementation.
Another important finding was the improvement in recommendation acceptance rates by physicians when the pharmacists contacted the physicians via phone or in person versus a written note to discuss DRPs (92% and 51%, respectively). This highlights the importance of the interprofessional approach to patient care and the need to work as a team to improve outcomes.
The greatest limitation is the lack of reimbursement structure. As this was designed as a proof of concept project to evaluate whether the implementation of a primarily community-based program in a hospital-based pharmacy could function structurally, reimbursement for service was not established prior to its implementation. At the time of this writing, current reimbursable avenues for MTM services have been established with nationally available systems (Mirixa and Outcomes), and local strategies for payment opportunities are being investigated.
Conclusion
Traditional dispensing models allow for missed opportunities for pharmacists to identify and resolve DRPs. MTM programs are adaptable to a hospital-based outpatient pharmacy utilizing Medicare-based screening criteria in a primarily non-Medicare population, resulting in the identification of DRPs. Applying this type of patient-centered approach in the traditional dispensing model may build a foundation for improved communication between providers and improve patient outcomes.
Footnotes
Acknowledgments
We would like to acknowledge Rafael Saenz, PharmD, Maria Yaramus, PharmD, and Janet St. Denis, RPh, for their dedication to the creation and implementation of the UPMC Falk Pharmacy MTM Service, and Melissa Somma McGivney, PharmD, for her assistance in the development of the MTM program and DRP tracking form.