
Abstract
OBJECTIVE:
To discuss the role of low-molecular-weight heparins (LMWHs) in the prevention of venous thromboembolism (VTE) in medical and orthopedic surgery patients. VTE prophylaxis trials in these practice settings establishing the current use of LMWHs marketed in the US are included. An overview is also provided of VTE incidence, risk factors, and prophylaxis consensus guidelines.
DATA SOURCES AND STUDY SELECTION:
Clinical trials, review articles, and meta-analyses for Food and Drug Administration–approved LMWHs were identified from a MEDLINE search (1980–March 2002). Search terms included dalteparin, enoxaparin, internal medicine, low-molecular-weight heparin, orthopedic surgery, risk factors, tinzaparin, and venous thromboembolism.
DATA SYNTHESIS:
Consensus guidelines are useful as an initial guide to appropriate VTE prophylaxis; however, a review of the primary literature is needed to identify optimal agents, regimens, or interventions. LMWHs have demonstrated sound efficacy in VTE prevention; however, the quantity and quality of literature are not always comparable for the available agents.
CONCLUSIONS:
Enoxaparin has demonstrated efficacy and safety in VTE prevention in medical patients, whereas information is limited or lacking for dalteparin and tinzaparin. Total hip replacement (THR) trials have been conducted with all US-marketed LMWHs and have demonstrated the efficacy and safety of each agent. Trials specifically establishing the efficacy of an LMWH in total knee replacement surgery (TKR) have been published for enoxaparin. One combination THR and TKR trial has been published for tinzaparin. These trial outcomes have positioned the LMWHs as key alternatives to adjusted-dose warfarin for VTE prophylaxis in orthopedic surgery. Inherent differences between LMWHs prevent the extrapolation of clinical outcomes from 1 trial to another.
Deep-vein thrombosis (DVT) and pulmonary embolism (PE) represent major health problems that cause significant morbidity and mortality in the US. More than 2 million cases of DVT occur in the US each year, with approximately 600 000 cases of PE. 1 Fewer than 50% of patients survive 1 year following a PE. 2 Several groups at higher risk for developing venous thromboembolism (VTE) include those undergoing abdominal, neurologic, or orthopedic surgery; cancer patients; victims of major trauma; and patients with spinal cord injuries. 3 The increased incidence of VTE has also been well recognized for severely ill medical patients with recent myocardial infarction, stroke, or heart failure. In addition, general medical patients are now recognized as a population at risk.
When DVT or PE complicates an existing illness or surgical procedure, there is an increase in the associated mortality and morbidity, as well as an increase in the cost of care. For patients who receive DVT treatment, postthrom-botic syndrome can become a residual medical issue. Up to 29% of patients can develop this condition within 8 years of an initial thrombosis. 4 Postthrombotic syndrome often causes chronic pain accompanied by swelling and skin ulceration in the affected limb. The resulting decrease in mobility and activity can greatly impact the patient's ability to resume a normal lifestyle. 1 Timely VTE prophylaxis is essential for the minimization of these events.
Multiple risk factors for VTE have been identified and are used to stratify both surgical and medical patients according to their risk (Table 1)3,5,6 Patients presenting with several risk factors have a cumulative risk. 3 Some institutions have implemented VTE risk assessment protocols to systematically identify patients who require prophylaxis.7,8 A constant challenge is to ensure that these guidelines become an integral component of day-to-day practice.
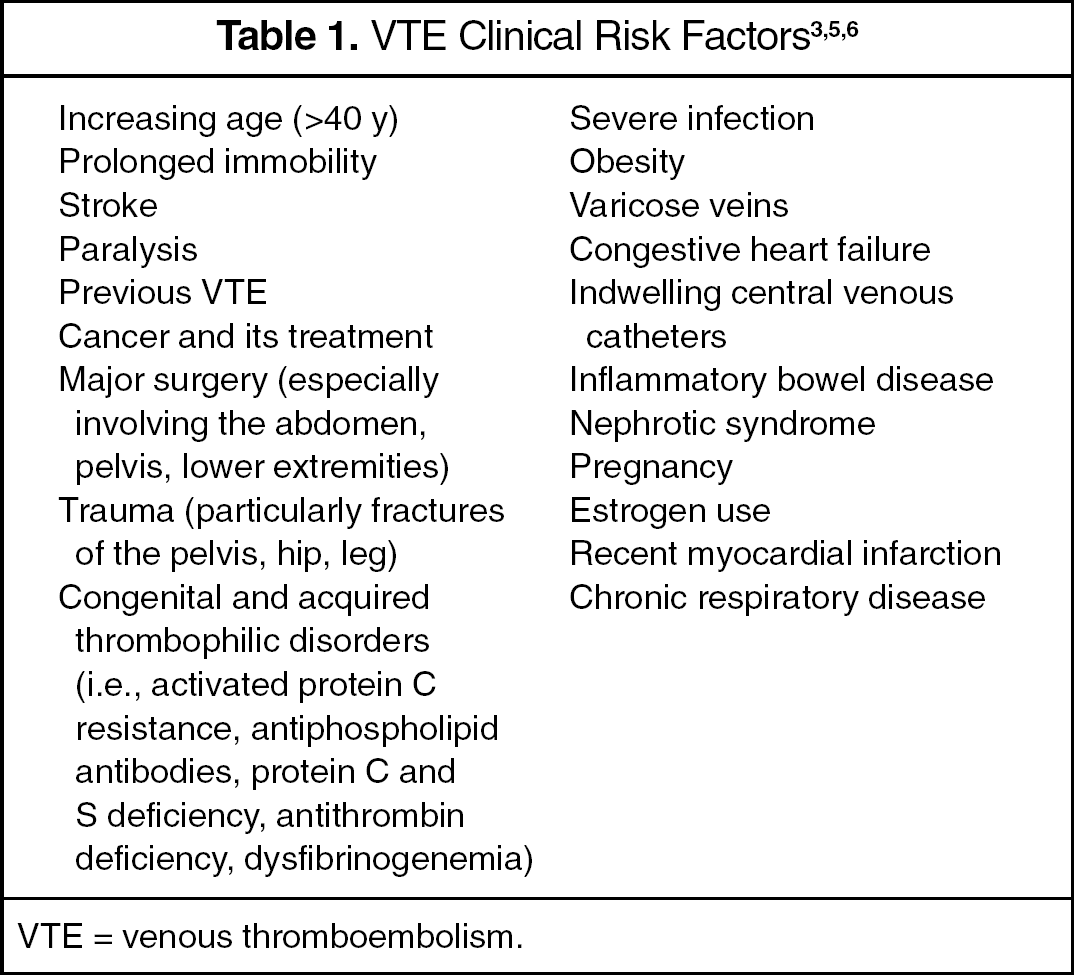
VTE = venous thromboembolism.
VTE Prophylaxis
The published clinical trials in VTE prophylaxis vary widely in terms of study design (superiority vs. equivalence), dosing strategies, VTE diagnostic methods, bleeding event definitions, reported VTE rates (symptomatic vs. asymptomatic), outpatient follow-up, and applicability to clinical practice. Venography has been used frequently in trials since it is considered the “gold standard” for DVT detection. Its high sensitivity and specificity minimize the rate of false-positive diagnoses, providing an unbiased estimate of the relative treatment effects. 9 However, this method may produce results that are not always applicable to clinical practice, particularly with distal, asymptomatic DVT rates. Some trials have employed a more practical and noninvasive diagnostic method, compression ultrasonography. When combined with venography to confirm positive results, ultrasonography can provide unbiased estimates of relative treatment effects and is more reflective of clinical practice. 9 The definitions for major and minor bleeding events can also vary from study to study. Many trials employ an international classification in which bleeding events, as well as wound hematomas, are categorized according to a descriptive standard. 10 Recent orthopedic trials have employed an additional major bleeding criterion: overt bleeding with a bleeding index ≥2. The bleeding index is calculated as the number of units of packed red blood cells or whole blood transfused plus the prebleeding hemoglobin concentration minus the postbleeding hemoglobin concentration. 11 The applicability of this criterion to clinical practice is unclear.
The American College of Chest Physicians (ACCP) 6th Consensus Conference on Antithrombotic Therapy has published graded recommendations for antithrombotic agents. 12 These recommendations are derived from the methodologic strength of the available evidence, with grade 1A being the most sound and descending incrementally to grade 2C. This review references 1A, 1B, and 2A recommendations (Table 2).3,13–17 A 1A recommendation is based on randomized trials without important limitations that demonstrate a clear risk/benefit ratio for the intervention. Evidence supporting a 1B recommendation provides clear risks and benefits, but the actual trials have important limitations, such as inconsistent results and methodologic flaws. Lastly, a 2A recommendation is given when the trials included are of sound design, but the risks and benefits of the intervention are unclear. The ACCP recommendations include, when appropriate, pharmacologic as well as mechanical device interventions such as intermittent pneumatic compression or elastic stockings. Mechanical devices are particularly useful when the risk of VTE is low, active bleeding is present, or when there is an increased risk of bleeding. The addition of mechanical devices to pharmacologic antithrombotic regimens may provide additional protection in certain high-risk populations. 18
Recommendations for VTE Prophylaxis
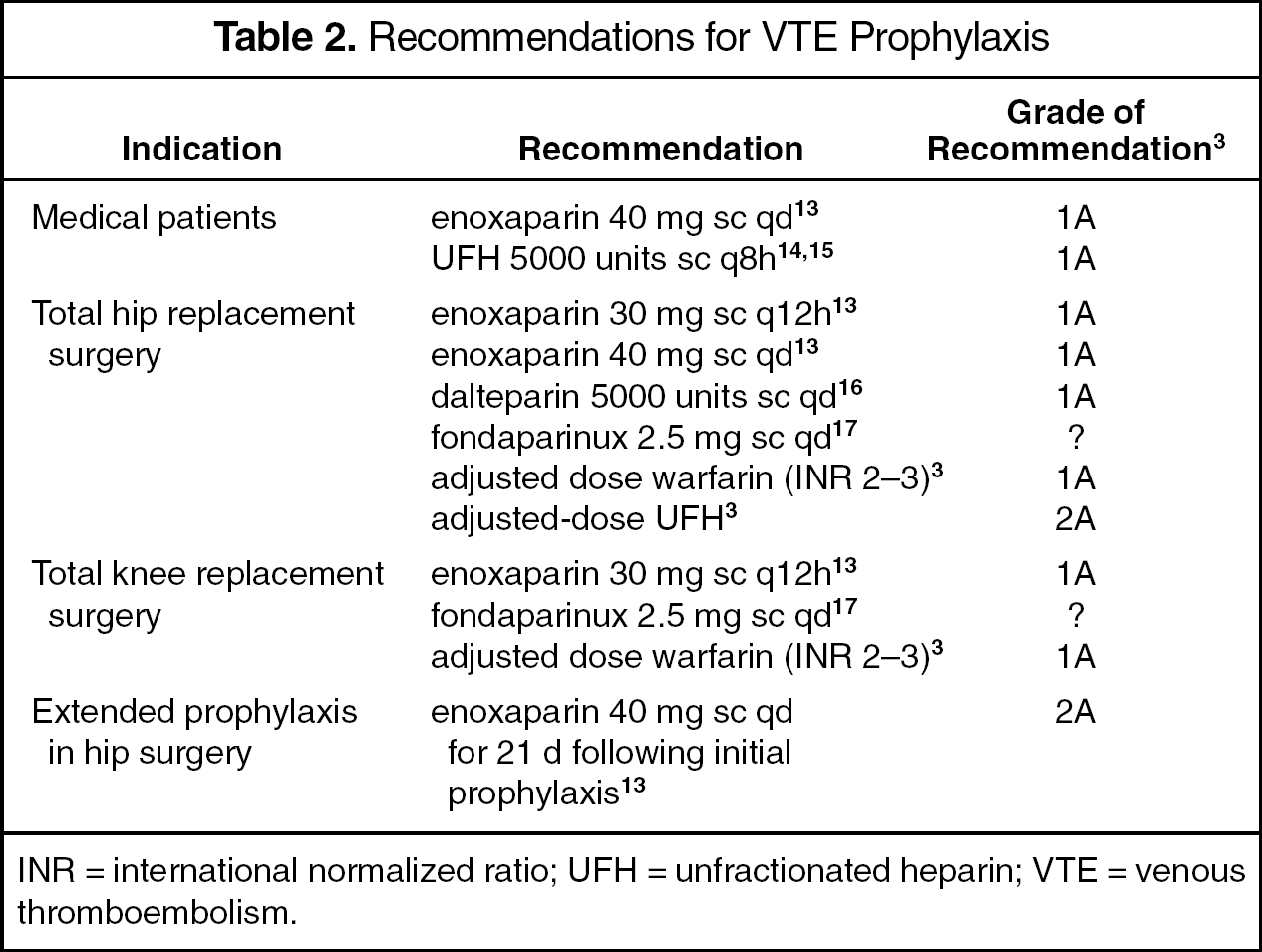
INR = international normalized ratio; UFH = unfractionated heparin; VTE = venous thromboembolism.
The primary purpose of this article is to evaluate the VTE prophylaxis clinical trials that have established the role of US-marketed low-molecular-weight heparins (LMWHs) in medical and orthopedic surgery practice settings. The focus on medical patients is due to the uncertainty regarding the optimal VTE prophylaxis regimens, as well as the underuse of thromboprophylaxis as a whole in this population. In orthopedic surgery, new anticoagulant agents continue to challenge the standing safety and efficacy of adjusted-dose warfarin therapy for VTE prophylaxis. These agents, as well as the current concept of extended VTE prophylaxis in orthopedic surgery, have prompted the inclusion of this patient population. The ongoing task of bridging evidence to clinical practice is also discussed in terms of current barriers to the provision of timely and optimal VTE prophylaxis regimens, as well as the controversial application of therapeutic interchange within the LMWH pharmacologic class.
Medical Patients: Ensuring Effective Prophylaxis
Without appropriate prophylaxis, a DVT event may occur in up to 1 of 4 hospitalized medical patients. 6 Fatal PE may occur in up to 1 of 20 of these patients who present with numerous issues and severely limited mobility. 5 Evidence from further research suggests that approximately 99% of hospitalized medical patients present with 1 VTE risk factor and at least 80% have ≥3. 19 These findings, in addition to recent trial results demonstrating the significant risk of VTE in moderately ill medical patients, 20 support the need to evaluate the current thrombotic risk for each medical patient upon admission.
The ACCP has given a grade 1A recommendation (Table 2) for the use of both low-dose unfractionated heparin (UFH) and LMWHs in VTE prophylaxis for general medical patients with risk factors. 3 Since these recommendations do not specify individual LMWHs or their regimens, a review of the available evidence is needed to define the efficacy and safety of specific agents.
A limited number of trials have evaluated pharmacologic regimens for VTE prevention in medical patients. The available studies primarily assess the efficacy and safety of LMWHs or low-dose UFH in comparison with placebo or each other. A meta-analysis of randomized VTE prevention trials in medical patients evaluated 8 studies comparing LMWH and UFH, as well as an additional 8 trials comparing heparins with placebo. 21 Although DVT detection methods employed were not consistent among the trials, a homogeneous treatment/control ratio was found. Heparins as a whole compared with placebo demonstrated a 56% risk reduction for lower limb DVT rates, a 52% risk reduction in clinical PE, a nonsignificant increase in major bleeding, and no effect on mortality. Although the power of the meta-analysis was too small to detect a difference in efficacy in the LMWH versus UFH trials, there was a significant reduction in the risk of major bleeding associated with the use of LMWHs (RR 0.48; 95% CI, 0.23 to 1.0; p = 0.049).
VTE prevention trials in medical patients evaluating the LMWHs marketed in the US have focused on the use of enoxaparin. One mortality study was conducted in Germany with dalteparin; however, the English translation is not currently available. 22 Table 314,15,20,23–25 provides specific details for each study presented here.
VTE Prophylaxis: Medical Patients
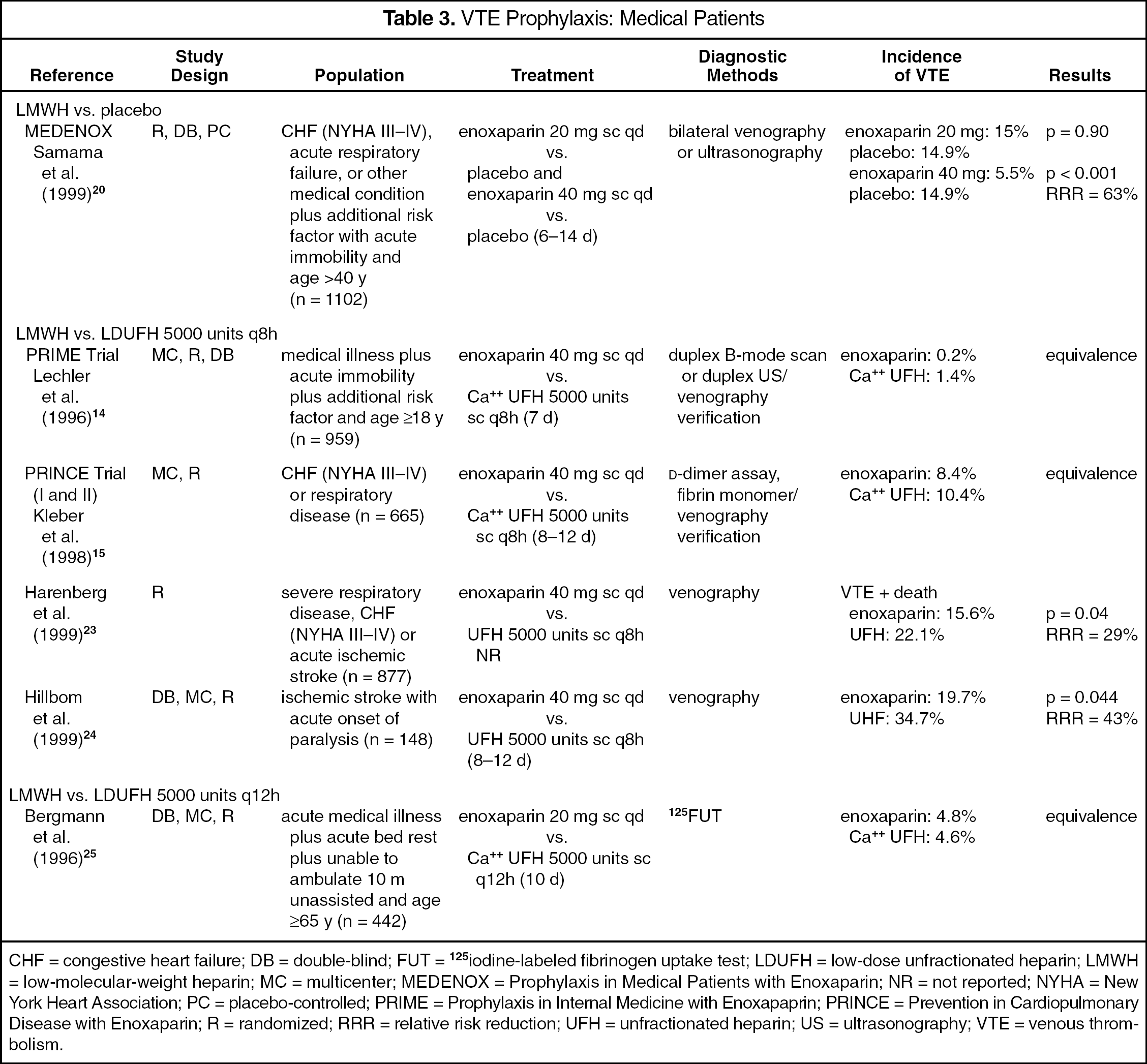
CHF = congestive heart failure; DB = double-blind; FUT = 125iodine-labeled fibrinogen uptake test; LDUFH = low-dose unfractionated heparin; LMWH = low-molecular-weight heparin; MC = multicenter; MEDENOX = Prophylaxis in Medical Patients with Enoxaparin; NR = not reported; NYHA = New York Heart Association; PC = placebo-controlled; PRIME = Prophylaxis in Internal Medicine with Enoxapaprin; PRINCE = Prevention in Cardiopulmonary Disease with Enoxaparin; R = randomized; RRR = relative risk reduction; UFH = unfractionated heparin; US = ultrasonography; VTE = venous thrombolism.
A large placebo-controlled VTE prevention trial randomized moderately ill medical patients to receive either enoxaparin 20 or 40 mg subcutaneously once daily or placebo for 6–14 days. 20 Results demonstrated that enoxaparin 40 mg was clearly superior to placebo for VTE prevention within the first 14 days. This benefit was also maintained at 3 months. The incidence of VTE in the enoxaparin 20-mg arm did not differ significantly from placebo. The actual rate of VTE in the placebo group was 14.9% (˜1 in 6 pts.). This outcome demonstrates the need to provide effective VTE prophylaxis in the studied population. The major bleeding rate among the 3 groups was not significantly different: 1.1% in the placebo group, 0.3% with enoxaparin 20 mg, and 1.7% with enoxaparin 40 mg. Enoxaparin is currently the only LMWH approved by the Food and Drug Administration (FDA) for VTE prophylaxis in acutely ill medical patients. 13
Four key randomized trials have compared subcutaneous enoxaparin 40 mg/d with low-dose UFH 5000 units every 8 hours in medically ill populations. The PRIME (Prophylaxis in Internal Medicine with Enoxaparin) trial, an equivalence study, randomized a nonselect or diverse group of medical patients with limited mobility to 1 of these treatment arms. 14 Reported DVT rates demonstrated that enoxaparin was at least as effective as low-dose UFH. However, the authors noted that, due to the low incidence of thromboembolic events identified, approximately 50% more patients would have been required to determine a significant difference or a lack of equivalence. The 30 documented bleeding events were evenly distributed across the treatment groups, with a trend toward more major bleeds in the low-dose UFH group. Injection-site hematomas also occurred more frequently with low-dose UFH (p < 0.001).
The PRINCE (Prevention in Cardiopulmonary Disease with Enoxaparin) trial, also an equivalence study, enrolled a more defined group of high-risk medical patients diagnosed with severe respiratory disease or New York Heart Association (NYHA) class III/IV congestive heart failure (CHF). 15 These patients were randomized to the same enoxaparin and low-dose UFH treatment regimens used in the PRIME trial. Enoxaparin was found to be at least as effective as low-dose UFH. In a subgroup analysis of patients with cardiac insufficiency, enoxaparin was again found to be at least as effective as low-dose UFH in preventing DVT and/or PE (9.7% vs. 16.1%, respectively). 26 A comparison of safety results between enoxaparin and low-dose UFH indicated that bleeding episodes (1.5% and 3.6%, respectively) and injection-site hematomas (7.2% and 12.6%, respectively) were more common in the low-dose UFH group. 15
A superiority trial also enrolled a severely ill group of higher-risk medical patients that were currently diagnosed with severe respiratory disease, CHF (NYHA III/IV), or acute ischemic stroke. 23 This trial, using venography diagnostics, demonstrated that enoxaparin was significantly superior to low-dose UFH at the same dosage regimens studied in the PRINCE and PRIME trials. The largest difference in efficacy (VTE incidence), in favor of enoxaparin compared with low-dose UFH, was seen in stroke patients, 26.5% versus 39.7%, respectively. The authors suggested that the advantage of enoxaparin seemed to increase with the rising VTE risk. Bleeding events were found more frequently with low-dose UFH (3.2%) compared with enoxaparin (1.8%).
Hillbom et al. 24 evaluated VTE prophylaxis regimens in patients who had recently suffered an ischemic stroke with an acute onset of paralysis. The regimen of enoxaparin 40 mg/d was again found to be superior to low-dose UFH administered every 8 hours. For patients with evaluable cerebral computed tomography scans, the results suggested that fewer patients treated with enoxaparin (17.3%) than low-dose UFH (23.3%) had evidence of hemorrhagic infarction. Evidence of intracranial hemorrhage was found in 1 enoxaparin patient; no other major bleeding events were reported.
The use of LMWHs in medical patients has also been compared with low-dose UFH administered every 12 hours for VTE prevention. An equivalence trial found that a lower daily dose of enoxaparin (20 mg) was comparable to UFH 5000 units given every 12 hours in a nonselect group of medical patients with limited mobility. 25 No significant differences were found in terms of bleeding episodes or adverse events. Considering that the efficacy of enoxaparin 20 mg/d in medical patients was found to be comparable to placebo 20 as well as twice-daily low-dose UFH, 25 these study outcomes raise some questions regarding the common practice of prophylaxis for this group with a twice-daily UFH regimen. Currently, this hypothesis remains to be explored in controlled clinical trials.
Two large trials focusing on VTE prophylaxis with LMWHs in medical patients are in progress. EXCLAIM (EXtended CLinical prophylaxis in Acutely Ill Medical patients) is a randomized, double-blind, placebo-controlled trial designed to assess the efficacy and safety of extended enoxaparin VTE prophylaxis in medical patients with prolonged immobilization. 27 Approximately 4000 patients will be enrolled at 450 centers. All patients will initially receive subcutaneous enoxaparin 40 mg/d for 10 days, then undergo randomization to receive either placebo or continued enoxaparin therapy for an additional 28 days. PREVENT (PRospective EValuation of dalteparin Efficacy for prevention of VTE in immobilized patieNts Trial), a randomized, double-blind, placebo-controlled trial, is evaluating medical patients who are at moderate to high risk for VTE to determine the efficacy and safety of dalteparin 5000 anti-factor Xa units subcutaneously daily for up to 14 days. 28 More than 3000 patients are expected to participate. Both EXCLAIM and PREVENT will use compression ultrasonography for DVT diagnosis.
LMWHs in Orthopedic Surgery: Superior Efficacy and Safety
The incidence of DVT, in the absence of prophylaxis, after total hip replacement surgery (THR), total knee replacement surgery (TKR), and hip fracture surgery is 50 – 65% at 7–14 days as detected by venography, with proximal DVT rates reaching 25%. When reviewed individually, the incidence of DVT in patients undergoing TKR is greater than that with THR, with rates approaching 80%. 3
The occurrence of symptomatic DVT in orthopedic surgery patients, as documented in the literature, is relatively infrequent compared with venography-determined endpoints. 3 Thus, a significant number of DVTs that occur dissipate before causing clinical consequences. However, it is difficult to identify the group of orthopedic surgery patients who are at especially high risk for symptomatic DVT and its associated adverse sequelae. As a result, all patients undergoing lower limb orthopedic surgery should be considered for VTE prophylaxis.
In reviewing the orthopedic studies, an important point to consider is the timing of antithrombotic therapy in relation to surgery. It has been suggested that the administration of therapy in close proximity to surgery enhances efficacy. 29 Although early administration appears to be desirable, there may be considerable reluctance by orthopedic surgeons to time therapy in this manner due to anticipated bleeding. Also, in the presence of regional anesthesia, the timing of LMWH administration should adhere to the American Society of Regional Anesthesia (ASRA) recommendations. 30 For example, the ASRA recommends that needle placement for single-injection spinal anesthetic occur at least 10–12 hours after the last preoperative LMWH prophylaxis dose. For single-dose and continuous-catheter techniques, in the presence of adequate hemostasis, the timing of the first postoperative LMWH dose differs between twice-daily and once-daily regimens. The first postoperative dose of a twice-daily LMWH regimen should not occur earlier than 24 hours after surgery. For once-daily LMWH regimens, the first postoperative dose should be administered 6–8 hours after surgery and the second postoperative dose should not occur sooner than 24 hours after the first dose. The ASRA also provides specific recommendations for timing LMWH doses regarding the removal of indwelling catheters.
The safety and efficacy of various pharmacologic prophylaxis regimens in orthopedic surgery have been well documented. Trials have evaluated the use of low-dose UFH, adjusted-dose UFH, adjusted-dose warfarin, LMWHs, hep-arinoids, aspirin, and most recently, a pentasaccharide. Currently, for THR or TKR, the ACCP recommends the use of either LMWH or adjusted-dose warfarin (grade 1A, Table 2). A lower grade recommendation, 1B, has been given for the use of these agents in hip fracture surgery due to the limited amount of available data. The LMWHs enoxaparin and dalteparin are approved by the FDA for VTE prophylaxis in THR; enoxaparin is the only one approved for use in TKR surgery and extended prophylaxis after hip surgery.13,16 Danaparoid, a heparinoid approved for VTE prophylaxis in THR, has been removed from the market due to problems encountered in obtaining raw materials for production. 31
LMWHs have demonstrated superior efficacy over low-dose UFH in orthopedic surgery and are at least as safe.32–35 Adjusted-dose UFH, although found to be highly efficacious in orthopedic surgery, 36 is more difficult to manage than LMWHs and, at this time, is not routinely prescribed. The ACCP has given a grade 2A recommendation for use of adjusted-dose UFH in THR due to the complexity of the regimen (Table 2).
When compared with adjusted-dose warfarin for VTE prevention in THR, LMWHs have shown superiority (Table 4).37,38 In one trial, patients undergoing THR were randomized to receive either postoperative enoxaparin 30 mg every 12 hours or adjusted-dose warfarin. 37 During hospitalization, a significant difference in the incidence of symptomatic, objectively determined VTE for enoxaparin compared with warfarin was 0.3% versus 1.1%. A follow-up evaluation at 3 months found no significant difference between treatment groups for VTE. Major bleeding occurred in 1.2% of the enoxaparin patients and 0.5% of the warfarin patients (p = 0.055). Fourteen of the 18 enoxaparin patients who had a major bleeding event received medication from 0 to 12 hours postoperatively. The current labeling recommends the initiation of therapy 12–24 hours after surgery. 13
VTE Prophylaxis: Orthopedic Surgery
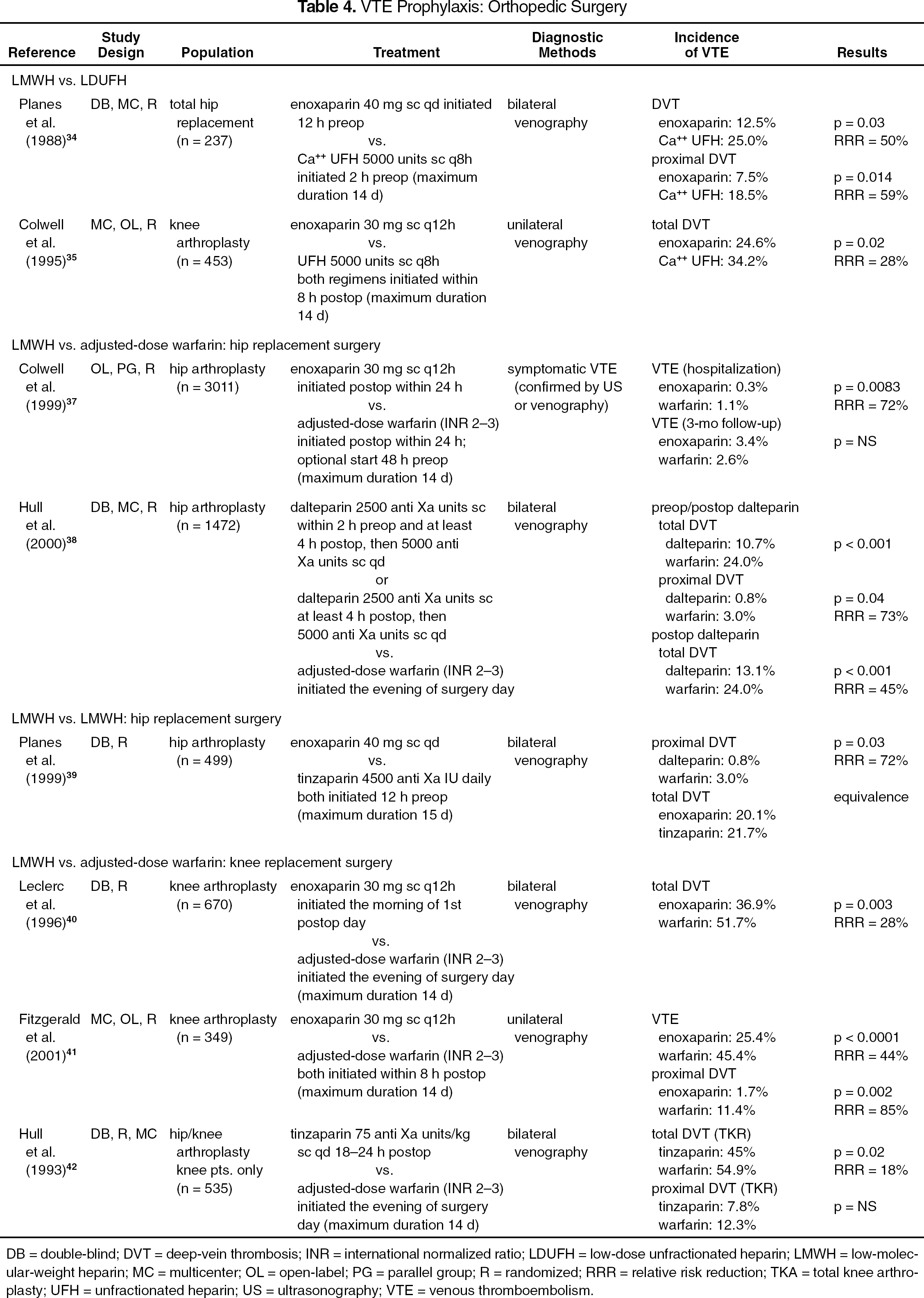
DB = double-blind; DVT = deep-vein thrombosis; INR = international normalized ratio; LDUFH = low-dose unfractionated heparin; LMWH = low-molecular-weight heparin; MC = multicenter; OL = open-label; PG = parallel group; R = randomized; RRR = relative risk reduction; TKA = total knee arthroplasty; UFH = unfractionated heparin; US = ultrasonography; VTE = venous thromboembolism.
A trial conducted by the North American Fragmin Trial Investigators (NAFT) compared the safety and efficacy of 2 dalteparin regimens to adjusted-dose warfarin in THR. 38 Dalteparin was administered at half the high-risk dose either 2 hours prior to surgery and/or at least 4 hours postoperatively, then continued at the usual high-risk dose daily for both groups. Each dalteparin regimen demonstrated superiority to warfarin in preventing total DVTs and proximal DVTs. In terms of major bleeding events, both dalteparin regimens resulted in a greater frequency compared with warfarin; however, the difference was significant only with the dalteparin regimen including a preoperative dose (p = 0.01).
Subcutaneous enoxaparin 40 mg/d was compared head-to-head in an equivalence trial with tinzaparin 4500 anti-Xa units/d for VTE prevention in patients undergoing THR. 39 Both regimens were initiated prior to surgery and then continued daily for a maximum of 15 days. Equivalence between the regimens for efficacy and safety was demonstrated based on total DVT rates and bleeding events. For TKR, postoperative enoxaparin 30 mg subcutaneously every 12 hours was determined to be superior to adjusted-dose warfarin when investigated by Leclerc et al. 40 and Fitzgerald et al. 41 Although the major bleeding episodes were somewhat higher in the enoxaparin groups, the differences did not reach statistical significance. Major bleeding events reported for enoxaparin and warfarin were 2.1% versus 1.8% (p > 0.2) 40 and 5.2% versus 2.3% (p = 0.17). 41 Differences in important operative site bleeding rates reported by Fitzgerald et al. 41 also did not reach statistical significance (6.9% for enoxaparin, 3.4% for warfarin).
Tinzaparin was compared with warfarin in a combination THR/TKR trial. 42 Although tinzaparin demonstrated a limited DVT risk reduction of approximately 10%, there was a significant increase in the number of major bleeding events (p = 0.04) and wound hematomas (p = 0.01) found with this therapy.
It has been common practice to terminate VTE prophylaxis when patients are discharged after orthopedic surgery. However, due to the emphasis on a shorter length of stay, patient discharge may occur at a time when the VTE risk is still high. A review of selected studies on extended prophylaxis in THR demonstrated that 10–20% of the patients who were sent home without continued prophylaxis had new indications of DVT within 4–5 weeks after hospital discharge as determined by venography. 3
A randomized trial using 179 THR patients demonstrated the benefit of continued enoxaparin prophylaxis for an additional 21 days after discharge compared with patients who received no further enoxaparin prophylaxis (total DVT; p = 0.018). 43 All patients received enoxaparin 30 mg subcutaneously twice daily for 13–15 days during hospitalization. Results from another extended prophylaxis trial after THR substantiated the superiority of continued dalteparin for an overall total of 35 days when compared with a group of patients who received adjusted-dose warfarin therapy for 6 days during hospitalization (total DVT; p < 0.001). 44 At this time, enoxaparin is the only LMWH approved by the FDA for this indication.
In a recent review of extended LMWH prophylaxis trials for THR, the authors concluded that the available evidence demonstrates the consistent efficacy and safety of this intervention. 45 The reviewers found a reduced frequency of symptomatic, objectively documented DVTs in patients receiving extended LMWH prophylaxis. Based on readmissions to the hospital because of DVTs, the authors suggested that an extended outpatient VTE prophylaxis period of 19–28 days is reasonable for patients undergoing elective hip surgery. Additional trials are required to further define whether all or only select higher-risk patients require this intervention. The ACCP gives an intermediate-strength recommendation (grade 2A) to these extended regimens, since the available trials are unable to clearly define the benefit or justify the cost (Table 2). 3
The newest agent to be approved by the FDA for VTE prevention in orthopedic surgery is fondaparinux sodium, a synthetic pentasaccharide. This selective anti-Xa inhibitor is rapidly absorbed by the subcutaneous route, exhibiting 100% bioavailability. Its terminal half-life is 17–21 hours, allowing for once-daily dosing. 46 Currently, the anticoagulation effects of fondaparinux are not reversible; however, factor VII is being investigated as a possible antidote. The FDA has approved this agent for DVT prophylaxis in patients undergoing THR, TKR, and hip fracture surgery. 17 Four pivotal Phase III trials in orthopedic surgery compared the safety and efficacy of subcutaneous fondaparinux sodium 2.5 mg/d initiated 6 ± 2 hours postoperatively with either subcutaneous enoxaparin 30 mg every 12 hours starting 12–24 hours postoperatively or enoxaparin 40 mg/d beginning 12 hours before surgery and continuing daily postoperatively. The primary efficacy outcome was the incidence of VTE as determined by bilateral venography performed between days 5 and 11 and, if warranted, a lung scan, pulmonary angiography, or helical computed tomography. Two trials were completed in THR and 1 each in TKR and in hip fracture surgery.47–49
A combined relative risk reduction of 50% in favor of fondaparinux can be derived from the results of these trials. 51 The fondaparinux product labeling reports the efficacy results as demonstrated under the conditions of the trials. 17 Regarding antithrombotic dose-timing and dose omission, certain trial conditions are to be considered in the interpretation of these results. The majority of the fondaparinux patients in the 4 orthopedic trials were administered the first postoperative dose at a mean of 6 – 6.5 hours after surgery. The majority of the enoxaparin patients in the combined trials received the first postoperative dose at a mean of 13–21 hours after surgery.47–50 In addition, for the 2 orthopedic trials that compared fondaparinux with the once daily enoxaparin regimen, the required preoperative enoxaparin dose was omitted in approximately 74% and 22% of the patients.48,49 For major bleeding events, there is a trend in the combined fondaparinux groups suggesting an increased incidence, particularly when considering the results for overt bleeding with a bleeding index ≥2.47,49,50 The difference in major bleeding rates was significant in the TKR trial, PEN-TAMAK (Pentasaccharide in Major Knee Surgery Study) (fondaparinux 2.1% vs. enoxaparin 0.2%; p = 0.006). 47 The approved labeling for fondaparinux cautions its use in the elderly and includes contraindications for its use in patients with severe renal impairment (creatinine clearance <30 mL/min) and those weighing <50 kg due to increased bleeding risks. 17 As greater experience is gained with fondaparinux, its place in therapy will become further defined among the available antithrombotic agents and those currently in the pipeline, such as the direct thrombin inhibitors melagatran and ximelagatran.
BRIDGING EVIDENCE TO PRACTICE
Although current research provides improved methods for identifying and stratifying populations at risk for VTE, a large number of preventable events continues to occur. 52 Barriers preventing the initiation of appropriate VTE prevention include the failure to evaluate patients in a systematic and timely manner, inconsistencies in the literature regarding optimal VTE prophylaxis regimens, concerns related to potential bleeding complications, and cost. These barriers can lead to an underestimation of the true VTE risk and the resulting failure to initiate appropriate prophylaxis. In terms of optimal prophylaxis regimens, the ACCP provides graded recommendations for patient populations at risk. However, the pharmacologic recommendations list agents in a general format or by class. As a result, clinicians refer to these recommendations as an excellent initial guide, but then must review and evaluate the available clinical evidence to identify the optimal regimen for a given population.
Of the LMWHs available in the US, enoxaparin has been the most frequently studied for VTE prophylaxis in medical patients and is currently the only LMWH approved for this indication. Efficacy outcomes have demonstrated the superiority of enoxaparin over placebo and superiority or equivalence to low-dose UFH given every 8 hours. A trend toward an overall improved safety profile is seen with daily enoxaparin dosing compared with this UFH regimen. Similar safety results were also found for LMWHs compared with low-dose UFH in a meta-analysis that evaluated VTE prevention trials in medical patients. 21 In addition, LMWHs demonstrate an improved pharmacokinetic profile over UFH, including increased bioavailability and a longer half-life. LMWHs are also associated with a significantly lower incidence of heparin-induced thrombocytopenia. 53 Lastly, the administration of a once-daily LMWH regimen is more convenient and less labor-intensive.
For orthopedic surgery, the ACCP currently recommends at least 7–10 days of anticoagulation therapy after THR or TKR. In addition, due to the positive outcomes reported for extended DVT prophylaxis with LMWHs in THR, the ACCP recognizes the use of this intervention for at least high-risk patients. Clinical trials have demonstrated the efficacy and safety of dalteparin, enoxaparin, and tinzaparin for VTE prophylaxis in THR. In the US, enoxaparin has been the most thoroughly evaluated LMWH in TKR and is approved for this indication. Enoxaparin and dalteparin are effective and safe for extended prophylaxis in THR, with enoxaparin currently having FDA approval. Finally, as more evidence becomes available, new agents, such as fondaparinux, may provide additional options for the prevention of VTE in orthopedic surgery.
Summary
A detailed review of the LMWH literature is particularly important in today's environment, as current LMWH acquisition costs are forcing many institutions to consider the application of a therapeutic interchange program to this pharmacologic class. However, as evident from the information provided here on medical patients and orthopedic surgery, the published LMWH trials are not equally distributed among the agents within this class. Also, head-to-head trials comparing the efficacy and safety of LMWHs in these patient populations are lacking. As a result, it is not appropriate to assume that 1 LMWH agent can be used in a safe and effective manner for a given indication based on experience with another. Therefore, the application of a therapeutic interchange program to this pharmacologic class is not advisable. 54