
Abstract
OBJECTIVE
To review the pharmacology, pharmacokinetics, clinical efficacy, and safety profile of long-acting (LA) risperidone for the treatment of schizophrenia.
DATA SOURCES
Information was selected from PubMed (1965–July 2004). Applicable scientific posters were also used.
STUDY SELECTION AND DATA EXTRACTION
All published information on risperidone LA was considered. Material providing a comprehensive description was considered.
DATA SYNTHESIS
Risperidone LA is the first long-acting, injectable atypical antipsychotic. It is dosed at 25–50 mg every 2 weeks. Adverse effects are similar to those seen with oral risperidone. A short-term study showed that risperidone LA is better than placebo in reducing the signs and symptoms of schizophrenia, and a long-term trial showed that stable schizophrenic patients can be switched from either oral or other injectable antipsychotic medications to risperidone LA.
CONCLUSIONS
Risperidone LA is efficacious and safe in the treatment of schizophrenia.
Schizophrenia is characterized by periods of remission and relapse for most patients. 1 Five years after the first break, 82% of patients will experience at least one relapse. Unmedicated schizophrenic patients relapse at a rate of approximately 10% per month. 2 The long-term outcome of schizophrenia can be enhanced by improving symptom control, improving relapse prevention, and improving social functioning mediated by facilitating family support and education. 3
Depot medications have been shown to decrease the high percentage of rehospitalization by increasing patient adherence, and they have become the standard of care for the long-term treatment of schizophrenic patients not adherent to oral therapy. 4,5 There are currently 2 typical antipsychotic depot medications available in the US: haloperidol and fluphenazine. These medications offer the benefit of improved adherence, but still produce adverse events such as tardive dyskinesia (TD) and extrapyramidal symptoms (EPS). Recently approved by the Food and Drug Administration, long-acting (LA) risperidone became the first long-acting atypical medication. It offers the benefits of both an atypical antipsychotic with the improved adherence of a long-acting drug.
Pharmacology
Risperidone LA is a formulation for parenteral administration. It is manufactured using a novel drug-delivery system in which the active medication is encapsulated in a Medisorb polymer to form microspheres. The polymer contains the metabolic precursors of 2 naturally occurring compounds, lactic acid and glycolic acid. They are linked together to form chains of varying lengths. Each reconstituted injection of risperidone LA is composed of risperidone microspheres suspended in an aqueous diluent. After each injection, the microspheres break down with the influx of water into the microspheres. The end byproducts of the breakdown of the microspheres are carbon dioxide and water. This gradual breakdown of the microspheres provides a slow and steady release of the risperidone. 6,7
Pharmacokinetics
ABSORPTION AND DISTRIBUTION
After a single intramuscular injection of risperidone LA, there is a small initial release of drug (<1% of the dose), followed by a lag time of 3 weeks. Following continuous exposure to body water for 3 weeks, the main release of the drug starts as the polymer in the microspheres break down naturally. Seven weeks after the intramuscular injection, the release of the medication stops. Oral antipsychotic supplementation should be given during the first 3 weeks of treatment with risperidone LA to maintain therapeutic concentrations until the main release of risperidone from the injection site has begun. 6,7
The combination of the release profile and the dosage regimen (injections every 2 weeks) of risperidone LA results in sustained therapeutic concentrations. Steady-state plasma concentrations are reached after 4 injections and are maintained for 4–6 weeks after the last injection. Plasma concentrations of risperidone, 9-hydroxyrisperidone (the major metabolite), and risperidone plus 9-hydroxyrisperidone are linear over the dosing range of 25–50 mg. 6,7
METABOLISM AND ELIMINATION
The main metabolic pathway of risperidone is through the hydroxylation of risperidone to 9-hydroxyrisperidone by CYP2D6. The rate of metabolism through CYP2D6 is dependent on genetic polymorphism. 8 9-Hydroxyrisperidone has similar pharmacologic activity as risperidone. The clinical effect of the drug results from the combined concentrations of risperidone plus 9-hydroxyrisperidone.
Risperidone could be subject to 2 kinds of drug–drug interactions. First, inhibitors of CYP2D6 interfere with the conversion of risperidone to 9-hydroxyrisperidone. The second type of interaction could result from coadministration of risperidone with a known enzyme inducer such as carbamazepine, phenytoin, rifampin, or phenobarbital. This coadministration could result in a decrease in the combined plasma concentrations of risperidone and the metabolite. 7
Risperidone and its metabolites are eliminated via the urine and, to a much lesser extent, via the feces. The apparent half-life of risperidone plus 9-hydroxyrisperidone following intramuscular administration is 3–6 days and is associated with a monoexponential decline in plasma concentrations. This half-life is a result of the breakdown of the microspheres and the subsequent release of risperidone. The elimination phase is complete 7–8 weeks after the last injection. 6
Several recommendations about the use of risperidone LA in special populations have been made; however, patients with either renal or hepatic disease have not been studied using the long-acting formulation. Based on studies with oral risperidone, it is recommended that these patients be carefully titrated on oral risperidone before starting on the long-acting drug. 7 Elderly patients, who can tolerate 2 mg/day, can be started on 25 mg every 2 weeks and maintained on the regular dosing schedule.
Clinical Trials
The efficacy and safety of risperidone LA were evaluated in a 12-week, multicenter, double-blind, randomized study. Patients who met Diagnostic and Statistical Manual (DSM)-IV criteria for schizophrenia, 9 with a baseline Positive and Negative Syndrome Scale (PANSS) total score of 60–120, were randomized to receive injections of risperidone LA (25, 50, or 75 mg) or placebo every 2 weeks. During the first week, previous antipsychotic medications were tapered to discontinuation and oral risperidone was started at 2 mg/day and increased to 4 mg/day for at least 3 days. This oral dose of risperidone was continued for the first 3 weeks of the study. 10 Patients who were taking risperidone 2 mg were started on 25 mg of risperidone LA, 4 mg on 50 mg, and 4 mg on 75 mg, respectively.
Three hundred seventy patients were evaluated in the intent-to-treat population. 10 Clinical improvement (20% reduction in PANSS scores) at endpoint was seen in 17% of the placebo patients, 47% of the 25-mg patients (p = 0.002), 48% of the 50-mg patients (p < 0.001), and 39% of the 75-mg patients (p < 0.001). There were significantly greater improvements seen with the Clinical Global Impressions (CGI) severity scores from baseline to endpoint in the 3 risperidone LA groups than that seen with placebo (p < 0.001 for all doses).
The investigators concluded that risperidone LA was significantly more efficacious than placebo in reducing the signs and symptoms of schizophrenia. 10 For patients who require maintenance therapy for treatment of schizophrenia, 25 mg every 2 weeks appears to offer the best risk/benefit profile, while 75 mg appears to offer no more benefit than 25 or 50 mg.
The long-term safety and efficacy of risperidone LA were evaluated in a 12-month, open-label, international, multicenter trial. 11 Symptomatically stable patients who met the DSM-IV criteria for a diagnosis of schizophrenia and had received a stable dose of antipsychotic for at least 4 weeks preceding the initial screening were eligible for the trial. During the 2-week run-in phase, all patients were switched to receive oral risperidone in a flexible dosage schedule of 1–6 mg/day. The patients were continued on oral risperidone for the first 2 or 3 weeks of the trial. The risperidone LA dose was based on the patients’ oral risperidone dose, and the investigators had the option of adjusting the risperidone LA dose during the trial. Six hundred fifteen patients received at least one injection of risperidone LA. The one-year trial was completed by 65% of the patients. Fifty-eight percent of the patients received 25 injections, 23% of patients received 12–24 injections, and 19% of patients received <12 injections.
Clinical improvement (20% reduction in the total PANSS scores) was seen in 49% of patients: 55% of the 25-mg group, 56% of the 50-mg group, and 40% of the 75-mg group. 11 The proportions of patients who were rated as not ill, very mildly ill, or mildly ill, according to the CGI-S, increased from 58% at baseline to 78% at endpoint in the 25-mg group, from 40% to 65% in the 50-mg group, and from 33% to 44% in the 75-mg group. During the trial, 18% of the patients were rehospitalized compared to the one-year relapse rates for other long-acting depot medications of 27%. 11,12
The investigators concluded that the results of this long-term study show that symptomatically stable schizophrenic patients can be safely switched from both oral antipsychotic medication and conventional depot antipsychotics to injectable risperidone LA. The severity of the patients’ schizophrenia symptoms was also reduced during the trial. The results of this long-term study also suggest that patients in the 75-mg group were less responsive than those in the 25- or 50-mg groups. 11 Some reasons for the lack of response in the 75-mg group could be that this group had a higher percentage of patients with paranoid schizophrenia and had fewer patients with a diagnosis of residual schizophrenia. Also, according to CGI-S, the 75-mg group had an increased percentage of marked to severe illness.
The clinical trials involving approved indications for risperidone LA are summarized in Table 1. 10,11,13,14 Investigators have also looked at using risperidone LA for other off-label indications, such as schizoaffective disorder and bipolar disorder. 15–17
Summary of Risperidone LA Clinical Trials
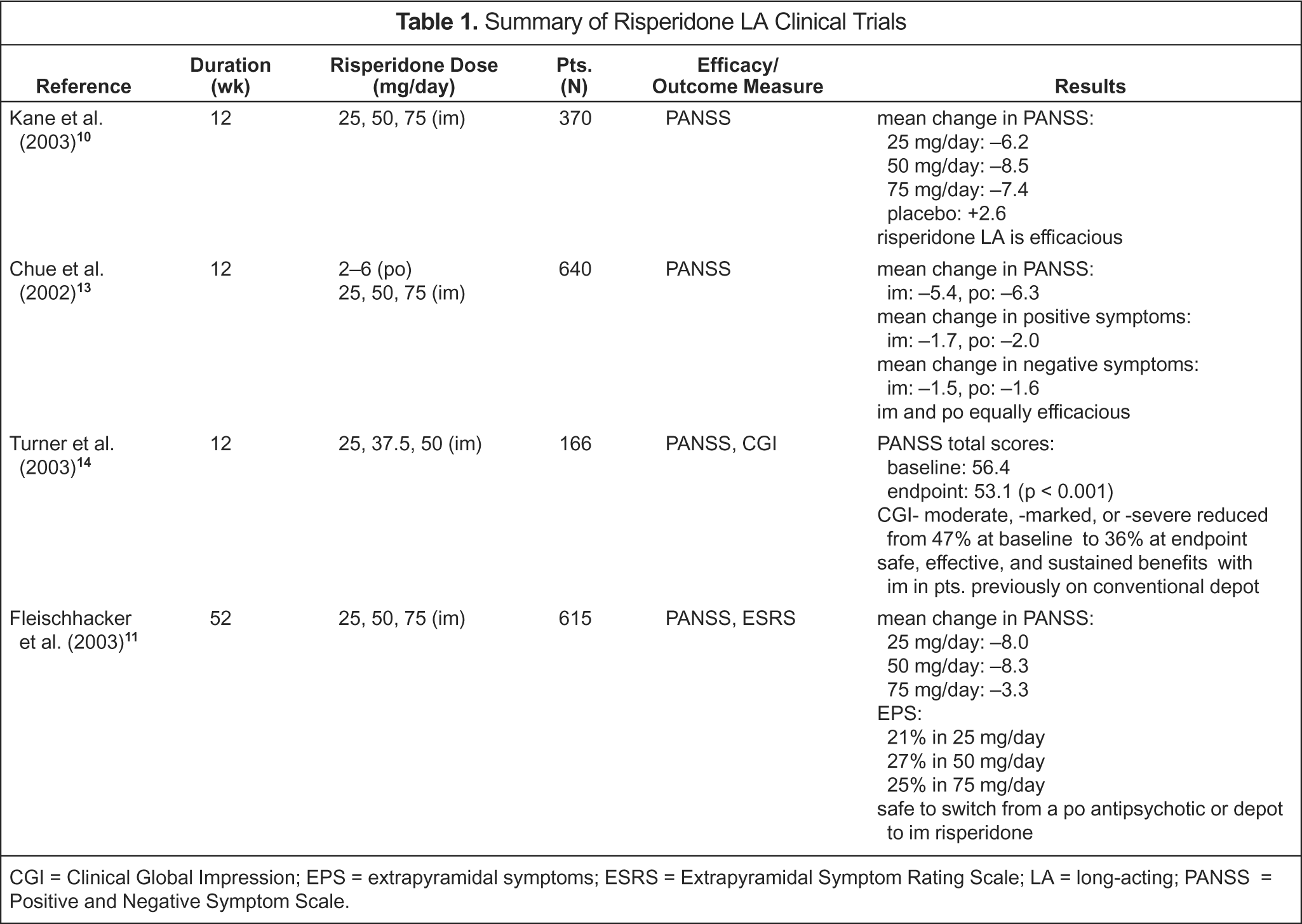
CGI = Clinical Global Impression; EPS = extrapyramidal symptoms; ESRS = Extrapyramidal Symptom Rating Scale; LA= long-acting; PANSS = Positive and Negative Symptom Scale.
Dosage
Risperidone LA is indicated for the treatment of schizophrenia. Patients who have never taken oral risperidone should be given a hypersensitivity challenge with 1–2 mg/day of oral risperidone for 2 consecutive days as a test dose before starting risperidone LA. 7,18
Risperidone LA should be administered every 2 weeks by deep intramuscular gluteal injection. Injections should alternate between the 2 buttocks and should not be administered intravenously. 18 No z-track administration is required. 7 Also, the needle that is provided with the packet is the only needle that should be used when administering the medication.
The recommended dose is 25 mg intramuscularly every 2 weeks. The dose for patients not responding can be increased to 37.5 or 50 mg every 2 weeks, but dosage increases should not be made more frequently than every 4 weeks. 7 The clinical effects of the dose adjustment should not be anticipated earlier than 3 weeks after the first injection with the higher dose. The dose should not exceed 50 mg every 2 weeks because there has been no additional benefit observed with a higher dose; the only observed effect is an increase in the number of adverse effects. 7,18 When administering risperidone LA, the doses should not be combined or divided. 7
There are several dosing considerations that clinicians should consider when beginning risperidone LA. When switching patients from other oral antipsychotics, patients should be started on risperidone LA 25 mg every 2 weeks and should continue with their current oral antipsychotic for 3 weeks. For patients who are being switched from other depot conventional antipsychotics to risperidone LA, administration of risperidone LA should occur at the next scheduled injection date instead of the depot conventional antipsychotic. 7,18 No coverage is needed with oral antipsychotic medications because, when patients receive adequate doses of a conventional depot for approximately 6 months, they will maintain an adequate plasma drug concentration for at least 1 or 2 months after their last injection. 18
Storage
Risperidone LA and its diluent should be stored away from light and in a refrigerator at temperatures of 2–8 °C. If the package is left out of the refrigerator at temperatures <25 °C, it is stable for up to 7 days. 7
Administration
Before risperidone LA is administered, the diluent should be brought to room temperature by warming the container with the palms of the hands to reduce the risk of discomfort during injection. The product should be used within 6 hours of reconstitution and must be shaken within 2 minutes before administration. 7
Adverse Effects
Aside from the pain at injection site, the adverse effects from risperidone LA are similar to those of oral risperidone. A summary of the percentages of adverse effects can be found in Table 2. 7
Most Commonly Reported Adverse Effects with Risperidone LA 7
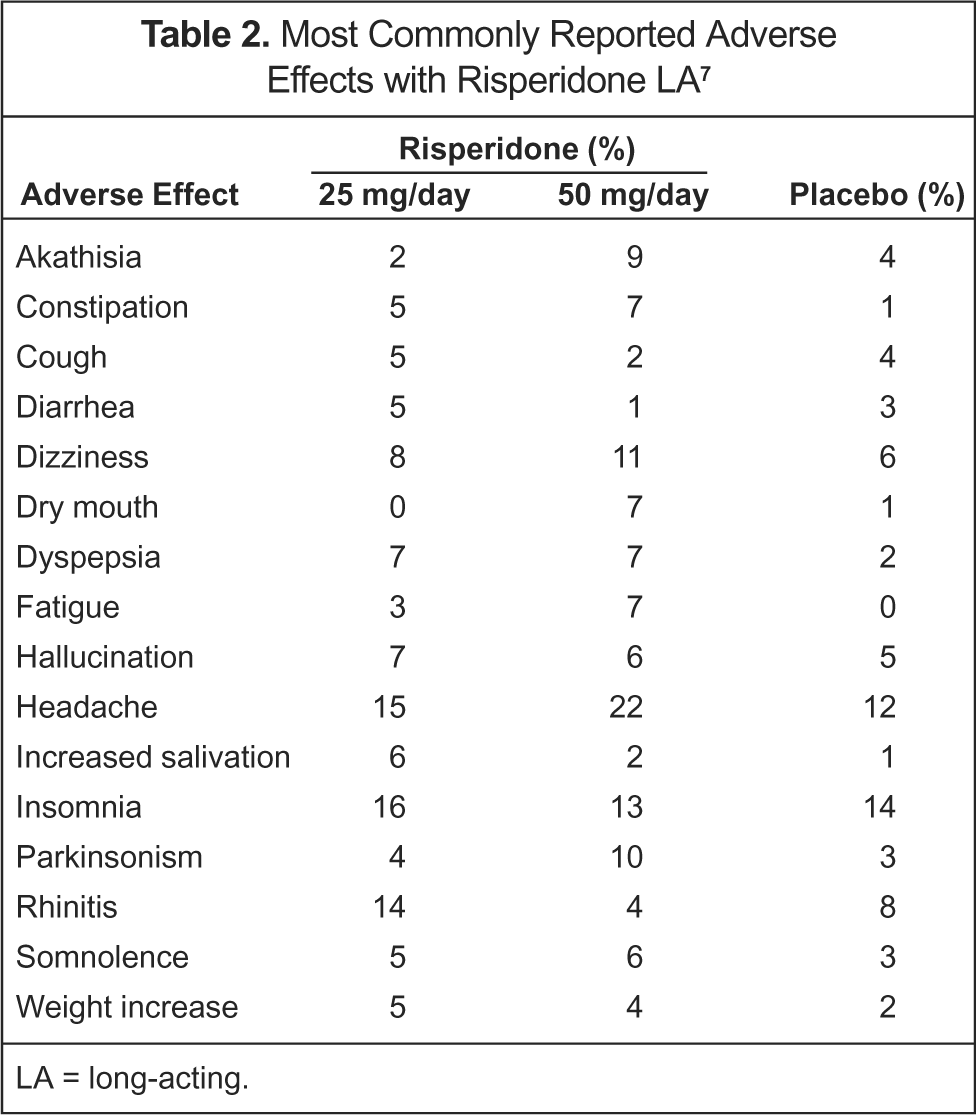
LA= long-acting.
TD was assessed during the 12-month trial using the Jeste-defined research criteria, 19 the Chouinard Extrapyramidal Symptom Rating Scale, 18 the 7-item dyskinesia movement subscale, and expert care assessment. In the study, 4 patients met the criteria for TD, and the dyskinesia persisted or worsened during the trial. This results in 0.68% of patients who could be classified with persistent emergent TD, which compares with 2.9% that is reported with typical agents. 11
The new aqueous-based formulation of injectable risperidone LA was associated with low patient pain ratings in 2 large multicenter studies. This offers advantages over the oil-based conventional depot preparations. 20
Hyperprolactinemia is listed in the package insert as an infrequent occurrence. In a 12-week study comparing oral risperidone with risperidone LA, the long-acting formulation was associated with a statistically significant reduction in prolactin levels at all doses tested over 12 weeks (p < 0.001). 21 The more stable blood concentrations with the long-acting injectable formulation may contribute to these findings. These results are consistent with the results found in other studies looking at prolactin levels in patients taking risperidone. 22
Hyperglycemia has been reported with the use of atypical antipsychotics, including risperidone. The exact relationship between the use of atypicals and hyperglycemia is not fully understood, and the specific risk estimate for hyperglycemia-related adverse events is not available. 7 Patients being treated with atypical antipsychotics need to be monitored for symptoms of hyperglycemia. In some cases, patients who develop hyperglycemia will have it resolve with the discontinuation of the atypical antipsychotic, while others will continue to require antidiabetic medications.
Cerebrovascular adverse events, including stoke, have been reported in elderly patients (73–97 y) with dementia psychosis who were taking oral risperidone. Risperidone LA is not approved for the treatment of patients with dementia-related psychosis. 7
Place in Therapy
The estimated economic burden of schizophrenia in 1990 was $33 billion in the US. 23 The majority of this cost was due to the consequences of psychotic relapse. To prevent this relapse, maintenance treatment with antipsychotic drugs is required for most patients. In a study comparing risperidone and haloperidol for the prevention of relapse in patients with schizophrenia, the Kaplan–Meier estimate of the risk of relapse at the end of the study was 34% for the risperidone group and 60% for the haloperidol group (p < 0.001). 23 This study also showed that the risperidone group had a greater reduction in both the mean severity of both psychotic symptoms and EPS than those in the haloperidol group.
Risperidone LA has been shown to decrease rehospitalization rates 24 and improve quality of life 25,26 in patients with schizophrenia. While risperidone LA has the potential to reduce the number of relapses and decrease the economic burden of schizophrenia on society, the cost of the medication should also be considered. The average wholesale price of the 25-mg vial is $266.50, the 37.5-mg vial $399.76, and the 50-mg vial $533.00, compared with that of haloperidol 100 mg/mL (5-mL vial) at $247.50 and fluphenazine 25 mg/mL (5-mL vial) at $69.30. 27 Several studies have recently been published investigating the efficacy and safety of risperidone LA with other depot medications and oral conventional antipsychotic medications, but the clinical guidelines do not currently include risperidone LA. 14,28,29
The clinician will need to consider all of the above factors before considering the use of risperidone LA in a patient. The expert consensus guideline series have published a list of patients for whom switching from an oral antipsychotic to a long-acting injectable atypical medication would be appropriate. 26
Summary
Risperidone LA is the first long-acting formulation of an atypical antipsychotic. It offers both the benefits of an atypical antipsychotic together with assured medication delivery. Risperidone LA has been shown to be efficacious, safe, and well tolerated in short- and long-term studies. The use of risperidone LA in patients with schizophrenia has the potential to reduce the number of relapses and decrease the overall economic burden of schizophrenia on society.