
Abstract
Purpose:
To evaluate the incidence of clinically evident hemolysis associated with orbital atherectomy used to treat severe peripheral artery disease.
Methods:
The observational CLEAR study enrolled 31 subjects (16 men; mean age 71±10 years, range 44–92) with claudication (58.1%) or critical limb ischemia (38.7%) who underwent orbital atherectomy with the Diamondback 360 system at 4 US centers. The 42 lesions in 31 limbs were located in the superficial femoral (n = 19, 45.2%), popliteal (n=8, 19.0%), and tibial arteries (n = 15, 35.8%). The majority of lesions (34, 81.0%) were de novo; moderate or severe calcification was identified in 90.5% of cases. Lesion and procedural parameters were analyzed at a core laboratory. Blood samples were collected during and post procedure and analyzed for markers of hemolysis. The primary endpoint was the occurrence of clinically significant hemolysis. The secondary endpoints included the occurrence of any clinical symptoms/signs potentially related to hemolysis. Statistical analysis was performed to identify predictors for hemolysis.
Results:
Laboratory evidence of hemolysis was seen in 11 (35.5%) subjects. No one met the clinical event criteria, and so the primary endpoint of the study was not reached. The secondary endpoints were hypertensive crisis (1, 3.2%) and transient hemoglobinuria (3, 9.7%). Lower glomerular filtration rates, calcified plaque, long atherectomy runs, and solid crown selection were independent predictors of hemolysis.
Conclusion:
There was no clinically significant hemolysis after orbital atherectomy. The results of this study will enable users to predict conditions that predispose to high levels of red cell hemolysis following orbital atherectomy and to take appropriate measures to limit its occurrence.
Keywords
A variety of endovascular devices are available to treat peripheral artery occlusive disease (PAOD), with demonstrated success and safety.1,2 Atherectomy, the most recent addition to these endovascular tools, has also shown reasonable efficacy but has occasionally been accompanied by adverse effects, including dissection, perforation, pain, spasm, and slow flow. 1 In particular, the use of a rotational device to perform mechanical atherectomy in coronary and peripheral vessels has frequently been associated with red blood cell hemolysis and hemoglobinuria; however, these laboratory findings have seldom translated into adverse clinical effects.3,4
See commentary on page 64
A newer form of atherectomy that is currently used for the treatment of vascular lesions in the peripheral arteries employs an orbiting crown. Data from the recently published OASIS clinical trial showed that orbital atherectomy is both safe and effective in the treatment of patients who present with severe, mainly infrapopliteal artery disease. 5 While red blood cell hemolysis was not reported in this trial, the potential for its occurrence during this type of atherectomy procedure has not been prospectively evaluated. Furthermore, the occurrence of hemolysis, although unexpected, may be concerning and has the potential to lead to clinically significant adverse events. 6 In view of this, we designed the current study to prospectively evaluate the frequency, extent, and clinical significance of red blood cell hemolysis occurring during the treatment of infrainguinal arterial lesions using orbital atherectomy technology.
METHODS
Study Design
From September 2008 through January 2009, consecutive subjects with symptomatic PAOD who were scheduled to undergo atherectomy in the lower limb with the Diamondback 360 System (DB360; Cardiovascular Systems, Inc., St. Paul, MN, USA) were enrolled in the CLEAR 360° study (Study to Determine the
Atherectomy Procedure
All subjects underwent orbital atherectomy using either a Classic Crown featuring a 30- micron diamond-coated band or a Solid Crown fully coated with 30 or 70 microns of diamonds. The eccentrically mounted crown rotates over a 0.014- or 0.017-inch proprietary ViperWire guidewire (Cardiovascular Systems, Inc.) at speeds of between 60 to 200 krpm at the physician's discretion. During the procedure, orthogonal views of the target vessels were taken, and all angiograms were analyzed using quantitative vascular analysis (QVA) at a core vascular laboratory (Brigham and Women's Hospital, Boston, MA, USA). The core laboratory classified calcification as moderate if radiopacities were noted on one side of the arterial wall but <1 cm in length; severely calcified arteries were identified by opacities on one or both sides of the arterial wall and extending >1 cm.
Clinical Assays
Two sets of blood samples were collected following enrollment. The first set included samples collected at baseline, immediately post intervention and again at 12 and 24 hours, and just prior to discharge. These samples were assayed for lactate dehydrogenase (LDH), plasma free hemoglobin (PfHgb), and serum haptoglobin. The second set of samples was taken during the procedure at the start of atherectomy, immediately following each change in atherectomy speed, and at the end of the procedure. These blood samples were analyzed immediately for PfHgb (HemoCue, Angelholm, Sweden). Urine samples were also collected at baseline, after the procedure, and just prior to discharge. Except as noted, all laboratory tests were performed in the CLIA-certified laboratory at each participating institution. The subjects were monitored for clinical signs of hemolysis and instructed to report any symptoms of chest pain, abdominal pain, or change in the color of the urine.
Patient Sample
The CLEAR study enrolled 31 subjects (16 men; mean age 71±10 years, range 44–92) with claudication (58.1%) or critical limb ischemia (38.7%) related to 42 lesions in 31 limbs (Table 1). The 42 lesions were located in the superficial femoral (n = 19, 45.2%), popliteal (n=8, 19.0%), and tibial arteries (n = 15, 35.8%). The majority of lesions (34, 81.0%) were de novo; there were 2 (4.8%) instent restenoses and 6 (14.3%) post-angioplasty restenoses (Table 2). Moderate or severe calcification was identified by QVA in 90.5% of cases.
Baseline Characteristics of the 31 Study Participants
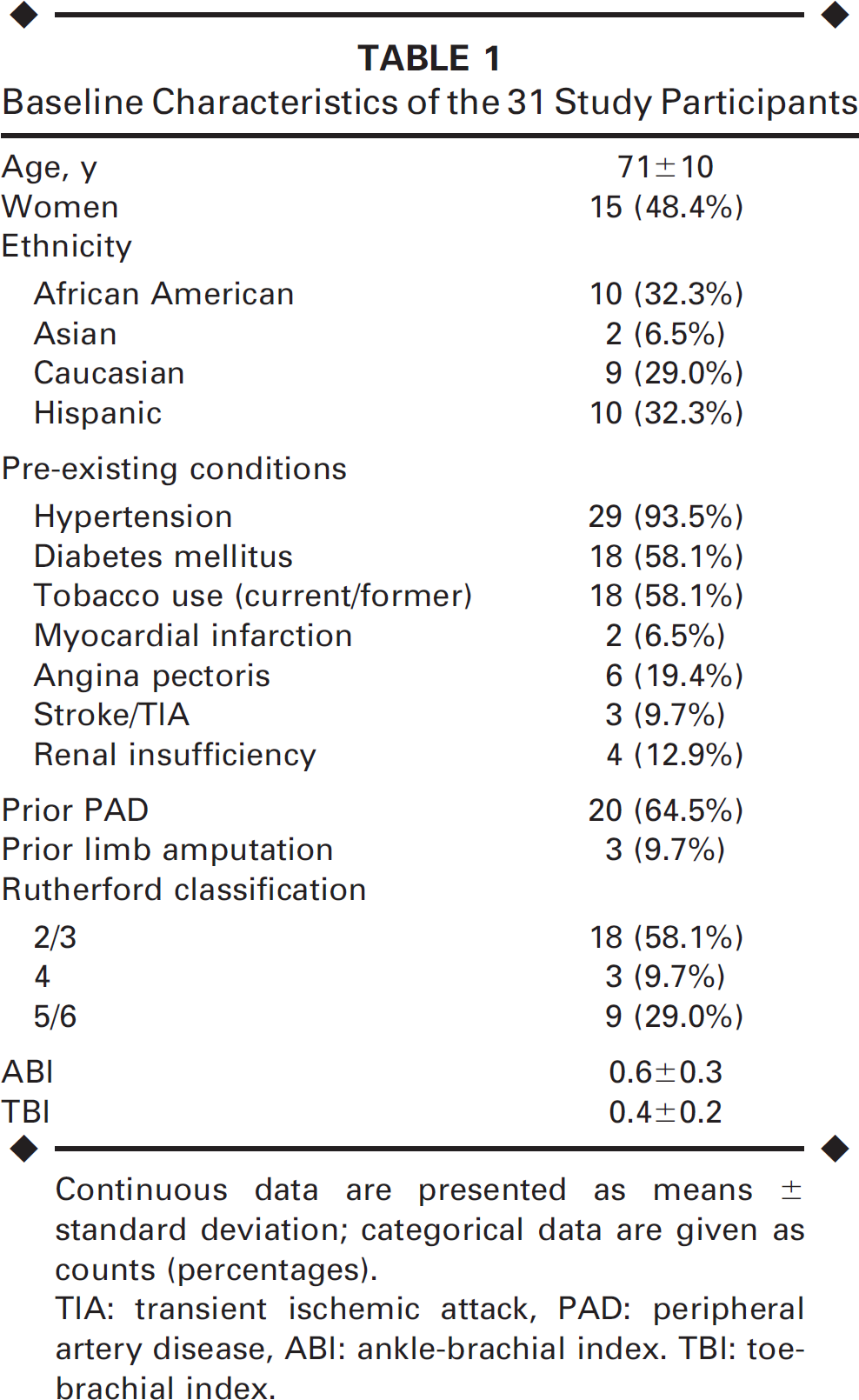
Continuous data are presented as means ± standard deviation; categorical data are given as counts (percentages).
TIA: transient ischemic attack, PAD: peripheral artery disease, ABI: ankle-brachial index. TBI: toebrachial index.
Characteristics of 42 Treated Lesions ∗
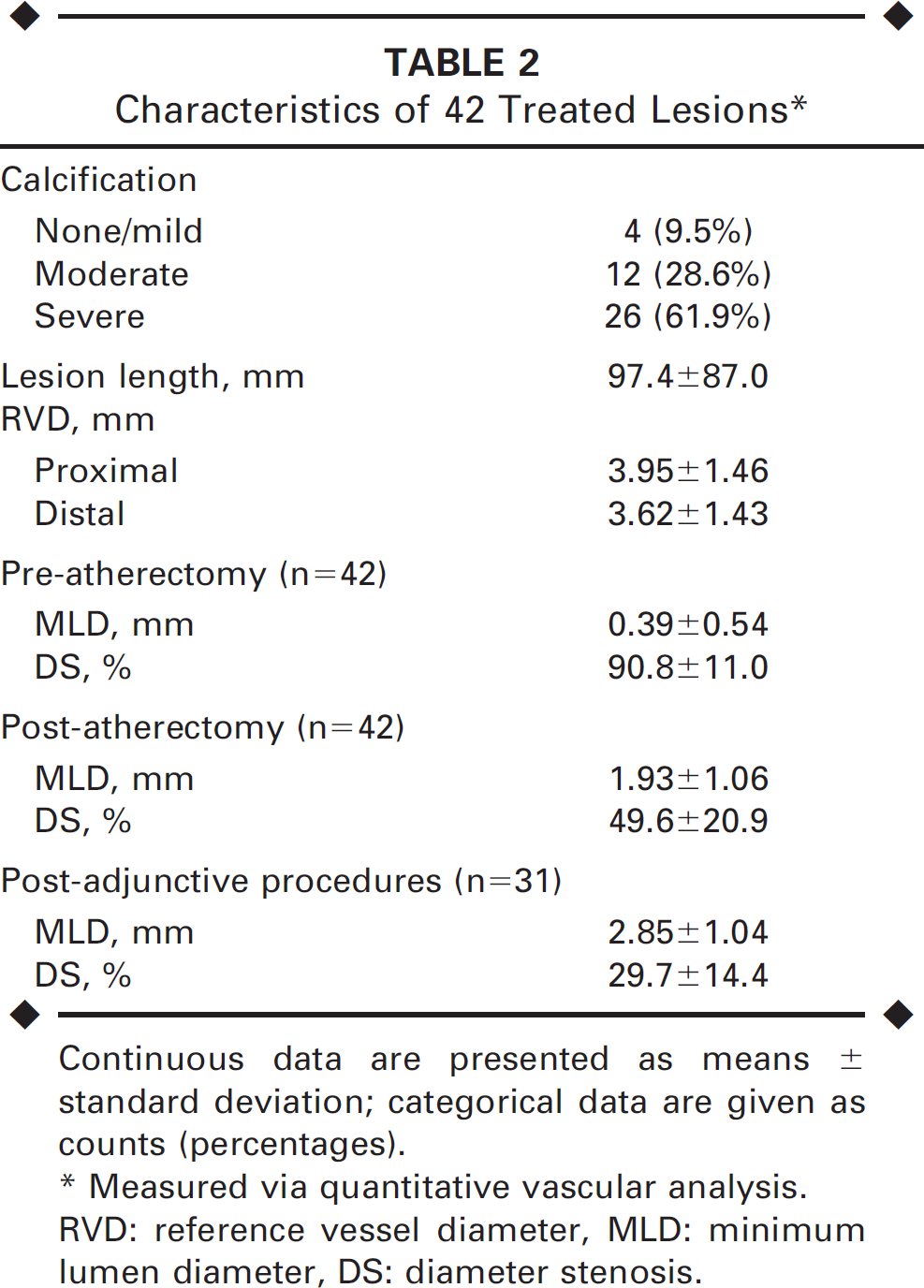
Continuous data are presented as means ± standard deviation; categorical data are given as counts (percentages).
Measured via quantitative vascular analysis.
RVD: reference vessel diameter, MLD: minimum lumen diameter, DS: diameter stenosis.
Endpoints
The primary endpoint was the first occurrence of clinically significant hemolysis either at 24 hours post procedure or prior to discharge as signified by: (1) serum LDH elevated ≤2 times the upper limit of the institution's laboratory normal value anytime after baseline, (2) PfHgb greater than baseline, (3) serum haptoglobin decreased by ≥50% compared with baseline, and (4) any of the following clinical events that were likely caused by hemolysis: acute renal failure requiring dialysis, acute pancreatitis requiring prolonged hospitalization, new anemia requiring blood transfusions, jaundice, acute myocardial infarction, stroke, or death. The first 3 criteria defined objective laboratory evidence of hemolysis and the last criterion their clinical sequelae.
The secondary endpoints included the occurrence of any clinical symptoms/signs potentially related to hemolysis (i.e., chest pain, abdominal pain, severe hypertension, or hemoglobinuria).
Statistical Analysis
Continuous variables are expressed as the mean ± standard deviation and were compared using the student t test, while categorical variables are expressed as counts (percentages) and were compared with the Fisher exact test. A regression model was built to assess independent predictors for hemolysis; the dependent variable (ΔPfHgb) as a marker for hemolysis was defined as the maximum minus the baseline value. The following variables were tested for their effect on ΔPfHgb: procedural factors (maximum and average speed, total run time, number of passes, maximum straight-line speed); lesion factors (number, length, location, plaque morphology); device type and diameter; smoking status; and medical history (hypertension, myocardial infarction, diabetes, blood pressure). The data were analyzed using SPSS software (10.1 version; SPSS, Chicago, IL, USA); p<0.05 was the threshold of significance.
RESULTS
Table 3 presents relevant procedure and atherectomy data from the 31 cases. The mean number of lesions treated per patient was 1.4 (range 1–4). The mean number of crowns used per lesion was 1.2 (range 1–3). Following atherectomy, adjunctive therapy was used in 31 (73.8%) of the lesions: low-pressure balloon angioplasty in 25 (59.5%) and stenting in 6 (14.2%). The percent diameter stenosis measured via QVA was 91%±11% pre procedure, 50%±21% post orbital atherectomy, and 30%±14 post adjunctive therapy.
Procedure and Atherectomy Parameters
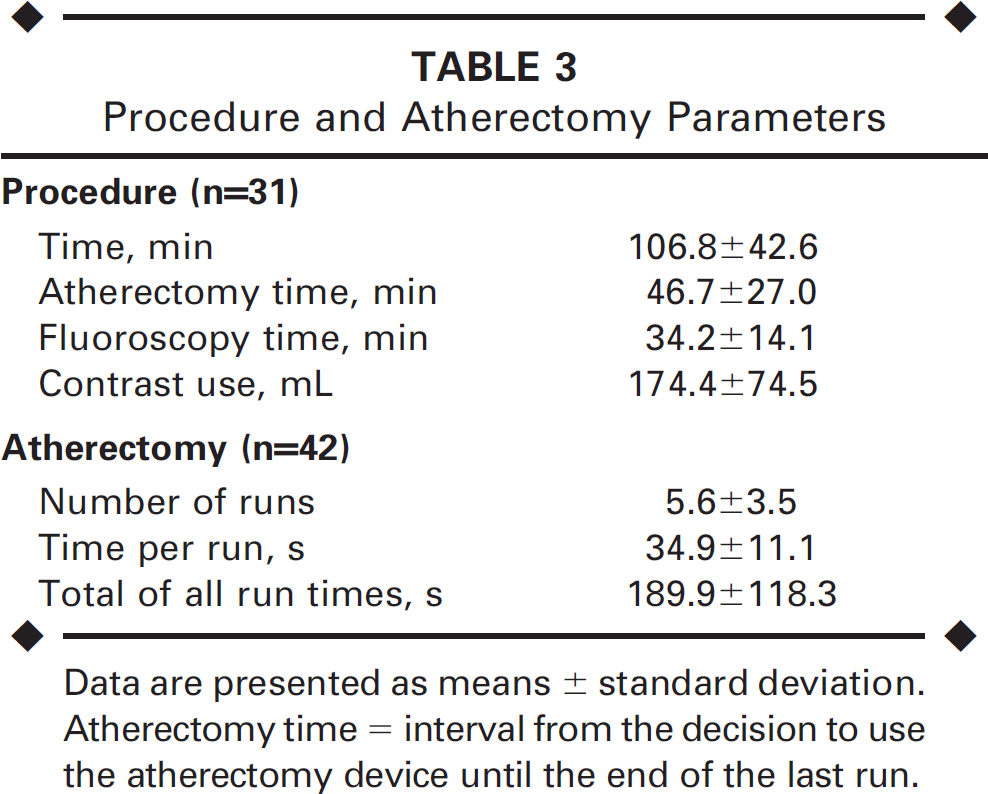
Data are presented as means ± standard deviation. Atherectomy time=interval from the decision to use the atherectomy device until the end of the last run.
Laboratory evidence of hemolysis using study-defined criteria was seen in 11 (35.5%) subjects. The fluctuations in median PfHgb, LDH, and haptoglobin levels during and following orbital atherectomy are depicted in Figure 1. Mean PfHgb was 17.6±24.7 mg/dL at baseline, rising to 169.5±169.7 mg/dL by the completion of atherectomy, and falling to 31.6±22.7 mg/dL by 12 hours post atherectomy. None of the subjects met the clinical event criteria; therefore, the primary endpoint of the study was not reached.
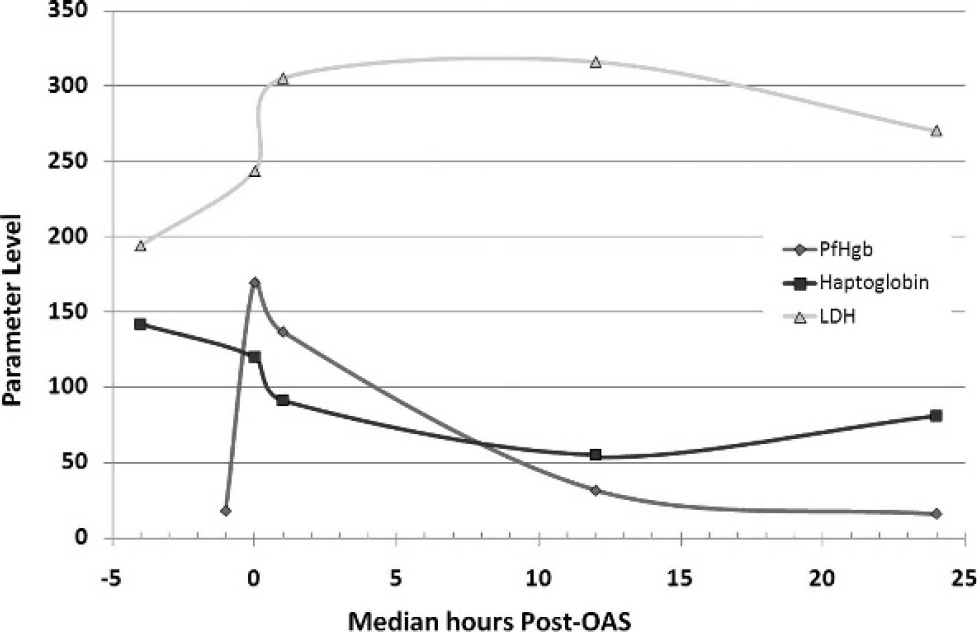
Changes in hemolysis parameter levels during and following the use of the orbital atherectomy system (OAS).
The secondary endpoints related to symptomatic hemolysis showed no new onset of chest (0%) or severe abdominal pain (0%); 1 (3.2%) patient had a hypertensive crisis that responded to medication. Three (9.7%) cases of transient hemoglobinuria were recorded; the mean peak PfHgb levels in these 3 subjects was higher compared to the remaining patients (1121±133 versus 450±68 mg/dL; p<0.01). No other symptoms potentially related to hemolysis occurred.
After multivariate analysis, the following variables were found to have a significant effect on ΔPfHgb: calcified plaque morphology (as opposed to fibrous plaque), use of a solid crown with a 70-micron diamond coating (versus a classic crown), a low baseline glomerular filtration rate, and longer atherectomy run times (Fig. 2).

Multivariate predictors of maximum PfHgb rise following orbital atherectomy. GFR: glomerular filtration rate.
DISCUSSION
When red blood cells are mechanically destroyed within the intravascular space, free hemoglobin is released and is rapidly bound to circulating serum haptoglobin. This complex typically undergoes endocytosis by macrophages and is then degraded. The haptoglobin supply is not endless, so once it is depleted, the surplus of hemoglobin accumulates in the plasma as free hemoglobin, with the potential for clinical sequelae.
A few mechanisms have been postulated linking intravascular hemolysis to its potential clinical consequences, mostly involving the oxidative stress caused by the release of heme protein or nitric oxide scavenging in small vessels. 8 While there are a number of ways the body safeguards against the proin-flammatory effects of these hemoglobin byproducts, marked hemolysis may overwhelm these protective mechanisms. Nitric oxide has been observed to neutralize the oxidative stress imposed by free hemoglobin; however, this scavenging process rapidly depletes nitric oxide, resulting in endothelial dysfunction with consequent vasoconstriction. 6 Nevertheless, this process appears to be shortlived.
There have been case reports of hemolysis occurring following various forms of atherectomy in the lower extremity.9,10 In addition, peripheral treatment with the Rotablator has been associated with a 5% to 13% incidence of hemoglobinuria in subjects undergoing femoropopliteal interventions.11,12 In these studies, the severity of hemolysis correlated with the ablation time, size of the burr, and the length of treated lesion. One potential advantage to the DB360 is its eccentrically-mounted, diamond-coated crown, which may achieve larger luminal gain. Given that the mechanism of plaque debulking with the use of orbital atherectomy is somewhat similar to that of rotational atherectomy, the investigation of potential hemolysis with this device is important.
The main finding of the present study is that while intravascular hemolysis was evident in approximately one third of infrainguinal arterial lesions treated with orbital atherectomy, this did not translate into short-term major clinical events. This important observation reinforces the safety of orbital atherectomy while effectively treating calcified lower extremity lesions.
In this report, the levels of PfHgb, the gold standard for measuring intravascular hemolysis, increased progressively in nearly all subjects throughout the procedure and peaked following the last atherectomy run; these levels fell sharply as soon as the atherectomy ended. During the next 12-hour period, the continued depletion of haptoglobin followed a parallel downward course with the reduction in PfHgb, after which haptoglobin levels began to rise. Perhaps this explains the paucity of clinical signs and symptoms seen in this study, in that the magnitude of hemolysis resulting from orbital atherectomy did not overwhelm the protective free hemoglobin scavenging mechanisms. Ultimately, PfHgb levels returned to their baseline values at 24 hours following atherectomy. Nevertheless, the long-term outcome of subjects who experience intravascular hemolysis is unknown.
Based upon the multivariate analysis, severely calcified plaque, reduced renal function, larger crown size, and longer atherectomy run times were independent predictors of a maximal increase in PfHgb following atherectomy. With regards to the extensively calcified plaque, one may hypothesize the presence of higher shear stresses during atherectomy resulting in higher degrees of red blood cell fragmentation. Decreases in the glomerular filtration rate may limit the absolute amount of free hemoglobin that is filtered through the glomerulus. Under these circumstances, it seems to follow that less aggressive atherectomy, including the use of smaller crown sizes and shorter total spin times, may limit the degree of hemolysis.
In terms of the secondary endpoints, transient hemoglobinuria was noted in 3 subjects. The occurrence of hemoglobinuria was presumably related to higher levels of free hemoglobin release, as the peak PfHgb levels in the 3 subjects was higher compared to the remaining subjects. Once the haptoglobin has been saturated, the excess free hemoglobin is filtered freely by the glomerulus. Severe hypertension seen in 1 patient was the only clinical event associated with hemolysis. While the peak PfHgb level for the individual who developed a hypertensive response was 406 mg/dL, this event could have been either related to the vasculotoxic effect of this molecule or just due to chance.
In addition, while measurement of changes in renal function was not a planned endpoint of this study, post-hoc analysis showed no significant change in pre- versus post-atherectomy serum creatinine in these patients, and there was no relationship between the level of PfHgb and change in creatinine. Nevertheless, the renal function was assessed only at 24 hours after exposure to contrast, and potential cases of contrast-induced nephropathy could have been missed.
The results of this study establish the safety of orbital atherectomy in terms of hemolytic risk and also highlight the need to employ best practices for device utilization to limit the potential impact of PfHgb elevation and to prevent other procedural events. Based on the authors' experience, the technique used in the present study, and the results achieved, the following practice standards are advised:
♦ The device should be started at a low speed and advanced slowly, at a rate of ∼1 cm/s.
♦ A total atherectomy time <5 minutes per patient is recommended, while individual intervals should be kept to <30 seconds.
♦ Liberal doses of vasodilators, such as 200 to 400 μg of nitroglycerin at baseline and between device intervals, will assist in preventing spasm and slow flow.
♦ The saline flush with device lubricant that runs continuously with device operation can also be administered between device intervals to facilitate flow of plaque particulate and hemolyzed red blood cells.
♦ Finally, implementing aggressive intravenous hydration protocols should limit the potential clinical consequences of intravascular hemolysis.
Limitations
The study was performed in a selected group of patients without evidence of severe renal disease who were intensively monitored before, during, and after atherectomy for hemolysis and for potential adverse clinical events. Importantly, this study, while observational, was prospectively designed to reflect “real-world” conditions of patient treatment through the recruitment of patients from several centers, treatment of a variety of lesion types and complexities, and the use of a range of crown sizes, shapes, and rotation speeds.
Conclusion
The results of this study, although based on a relatively small group of patients, will enable the users of the Diamondback 360 to predict conditions that predispose to high levels of red cell destruction. The potential hemolysis can be readily managed by currently employed standard supportive measures, such as attention to patient hydration, vital signs, renal output, and device selection. Furthermore, proper technique when using the Diamondback 360 device will yield optimal procedural success and facilitate safe and effective treatment of patients with peripheral artery disease.