
Abstract
Purpose:
To present a systemic review and meta-analysis investigating the outcomes of endovascular management of arterioenteric fistula (AEF).
Methods:
Literature review on AEF management with endovascular surgery using MEDLINE search, including two cases managed by the authors.
Results:
Fifty-nine patients (50 men; mean age 68 years, range 23–90) were identified. AEF was successfully managed in 55 (93%) patients and 30-day mortality was 8.5% (5/59). During follow-up, 10 (19%) patients developed recurrent bleeding, which occurred more often in AEFs due to cancer. The freedom from recurrence rate at 12 and 24 months was 71.5%. Seventeen (32%) patients developed sepsis, which was managed conservatively in 8 (7 successful). Freedom from sepsis at 12 and 24 months was 64%, while the freedom from combined recurrence and sepsis at 12 and 24 months was 59%. Patients who did not have intestinal repair had a higher rate of combined recurrence and sepsis compared to patients who did; the freedom from combined recurrence and sepsis at 12 months was 52% for patients not having intestinal repair versus 100% in patients who did (p=0.022). Total AEF-related mortality rates at 12 and 24 months were 15% and 19%, respectively, significantly worse when AEF recurred (p=0.001). Overall survival rates at 12 and 24 months were 68% and 52%; prognosis was worse in patients with perioperative sepsis, large bowel fistulization, tube graft placement, no intestinal repair, and recurrent AEF.
Conclusion:
Endovascular management of AEF can achieve satisfactory short and midterm results, better than those historically reported for open surgery, despite the high rate of recurrent bleeding and sepsis. Further investigation of the role played by intestinal repair is warranted.
Keywords
Arterioenteric or aortoenteric fistula (AEF) is a late complication of abdominal aortic aneurysm (AAA) repair; 1 occasionally, it presents as a primary complication of the AAA or arterial invasion by tumors. Even after appropriate surgical intervention, mortality rates average 50%, although there is a trend toward improvement in recent years. 1 This dismal prognosis is associated with advanced age, the presence of comorbidities, hemorrhagic shock and sepsis, and the magnitude of surgery. Although the mortality associated with AEF seems to have decreased over time, this condition continues to be highly lethal, which has prompted the search for a less invasive treatment modality.
Endovascular management of AEF was first performed 11 years ago. 2 This technique has the advantages of being minimally invasive, with low morbidity and mortality 3 ; however, the repair is plagued by high rates of recurrence and sepsis. After a mean of 9.5 months, Danneels et al. 4 documented a 60% rate of recurrence or sepsis in 15 patients with AEF. They suggested that this technique should serve as a bridge to open surgery when possible, providing time to manage shock, local and systemic infection, and comorbidities in order to improve patient fitness and therefore outcome of future open repair. However, many patients with AEF will never become good candidates for elective or semi-elective repair, so these conclusions, based on a relatively small series, are not applicable for all patients. Therefore, a larger series of patients treated with endovascular methods and observed for a longer period is necessary to draw firm conclusions and guide patient care.
The aim of our study was to perform a meta-analysis analyzing the results of endovascular management for AEF, including 2 cases of AEF managed in our institution.
METHODS
A MEDLINE/PubMed search (restricted to full length articles published in the English language, but with no time period limit) was performed in August 2008 (key words: aortoenteric fistula and endovascular) followed by a manual search of the references to identify AEFs that had been treated with endovascular technique, which included 2 published cases managed at the authors' institution. 5 Cases of aortoesophageal fistulas, thought to behave differently, and AEF repair performed as a bridge to open surgery were excluded, but unusual causes of intraabdominal arterial fistulization involving the iliac arteries or due to malignancy were included. Redundant cases from dual/subsequent reports were excluded. The recommendations of the Meta-analysis of Observational Studies in Epidemiology (MOOSE) group were followed throughout. 6
The following information was entered into a database: number of cases (1–2 or >2) reported in each publication; publication year; gender; age; cause (primary, secondary, tumor, other); presence of sepsis; location of AEF; time since original aortic surgery (if applicable); type and size of endovascular graft; adjuvant procedures; persistent, early, and perioperative sepsis; early (30 day or inhospital) mortality and cause; early complications; antibiotic suppression and duration; number of antibiotics and type; AEF recurrence; time to recurrence; management of recurrence; late sepsis; time to late sepsis; management of late sepsis; late mortality due to AEF; time to death due to AEF; total mortality; and time to death.
Statistics
The Shapiro-Wilk test was used to check normality of distribution; nonparametric tests were used for data not normally distributed. Continuous data are presented as means (range) or median (interquartile range) if nonparametric; categorical data are given as counts (percentages). Categorical data were analyzed with the chi-squared or Fisher exact test, where appropriate. Event rates during follow-up were estimated with Kaplan-Meier curves, while the log-rank test was used to compare the event rates of the various subgroups. Cox proportional hazard models were used for multivariate analysis; outcomes are reported as the relative risk (RR) and 95% confidence interval (CI). All data were analyzed with SPSS (version 14 or later) or PASW Statistics (version 18; SPSS Inc, Chicago, IL, USA).
RESULTS
Twenty-seven studies or case reports on 57 patients were identified2–4,7–30; including 2 patients of ours, 5 for a total of 59 patients (Table 1). Approximately half of all patients were reported as case series or case-controlled studies. Most patients were elderly (mean age 68 years, range 23–90) and male (85%). The majority of AEFs (73%) were secondary; 14% were primary, 10% were due to a tumor of the genitourinary system (bladder, ovary, cervix, testicle, or extragonadal germ cells) or rectum (n=2), and 3% were iatrogenic. Sepsis was present preoperatively in 10 (17%) of all cases, and there was no association with baseline characteristics (in 6 cases where the individual patients with sepsis were identified). The abdominal aorta itself was involved in 54 cases, while the remaining AEFs affected the common (n = 1), internal (n = 1), or external (n=3) iliac arteries. In 4 cases, the fistulas involved the rectum and in 1 case the sigmoid colon. In secondary AEFs, median time from aortic surgery was 6.7 years (4–10).
Studies and Patients Included in the Current Meta-Analysis
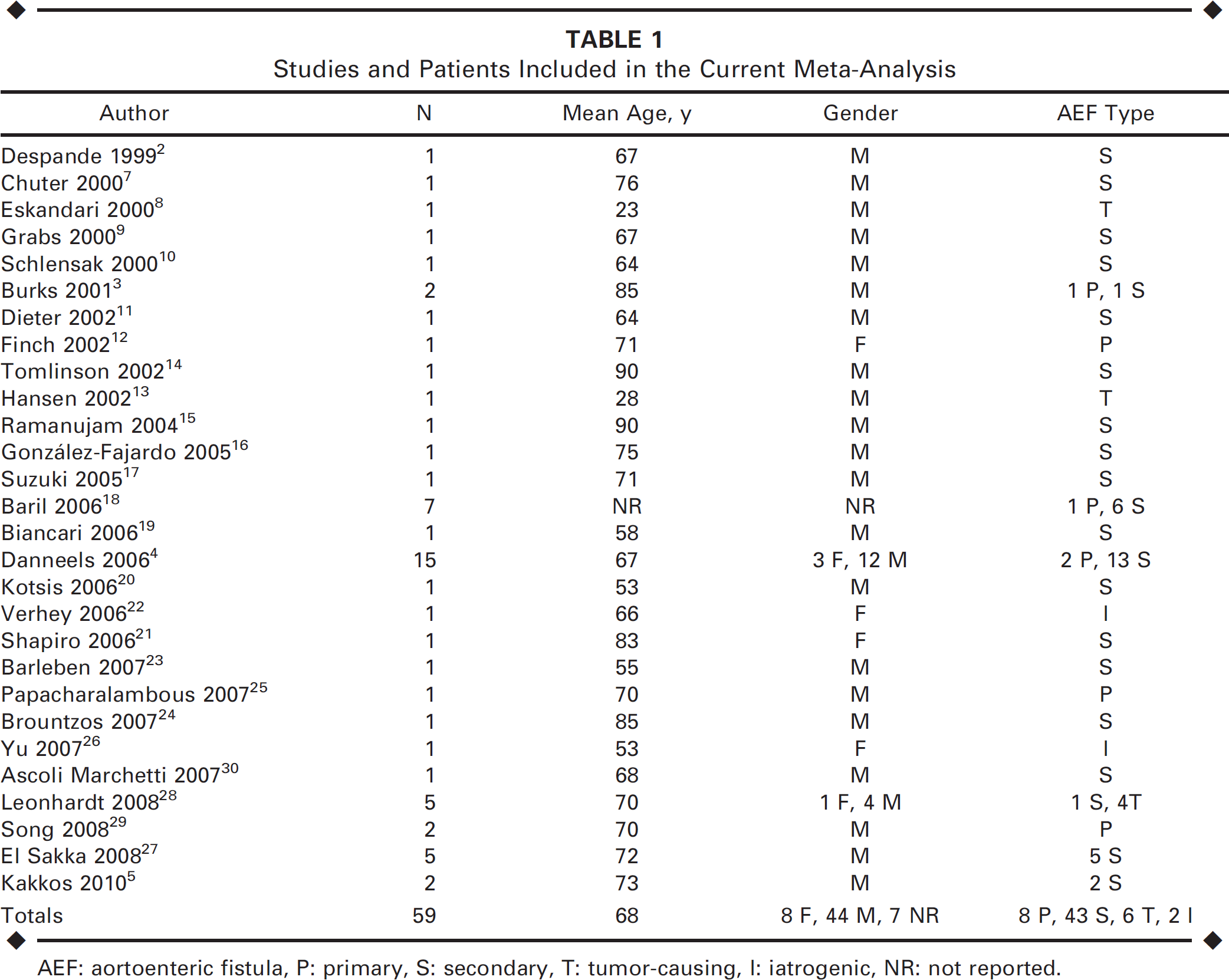
AEF: aortoenteric fistula, P: primary, S: secondary, T: tumor-causing, I: iatrogenic, NR: not reported.
Management
Bifurcated endografts were placed in 15 (25%) patients, tube grafts in 16 (27%), aortomonoiliac grafts in 11 (19%), and extender cuffs in 6 (10%), while in 1 (2%) patient, the aorta was occluded proximally and distally with aortic occluders that had a gentamycin sponge placed in between. In the remaining 10 (17%) patients, the device type was not reported. Median stent-graft size (reported in 14 cases only) was 25 mm (23.8–28). Stent-graft manufacturers (where reported) included W.L. Gore & Associates (n=8; Flagstaff, AZ, USA), Cook Medical Inc. (n=7; Bloomington, IN, USA), Medtronic (n=6; Minneapolis, MN, USA), Abbott/Jomed (n=5; Abbott Park, IL, USA), MinTec (n = 1; La Ciotat, France), Edwards Lifesciences (n = 1; Irvine, CA, USA), and Boston Scientific Corporation (n=2; Natick, MA, USA).
Adjuvant procedures were performed in 24 (41%), including management of sepsis (percutaneous drainage of 3 abscesses and 1 diversion ileostomy followed by Hartmann's colectomy), intestinal repair (2 preoperative open closures, 1 intraoperative injection of cyanoacrylate glue into the fistula tract, and 3 postoperative open closures), limb revascularization (9 femorofemoral bypasses and 1 axillobifemoral bypass), 2 cases of stenting, 1 common femoral interposition grafting, and removal of loose pedicle screws in 1 case. Interventions for sepsis control, as described above, were necessary in 4/10 (40%) patients with sepsis, while in the remaining 6 patients, no abscess was reported, and sepsis was managed with antibiotics.
Early Complications
Failure to control bleeding. One patient died perioperatively because hemostasis could not be achieved. In 3 additional patients, bleeding recurred; one of them was managed with endovascular means, unsuccessfully, and another one with aorta closure and axillobifemoral bypass. In only 1 patient with a psoas abscess (drained as part of an adjuvant procedure) was sepsis present.
Sepsis. Persistent sepsis developed in 4 patients. Sepsis early in the postoperative period was reported in another 3 patients. In one of them, infection required laparotomy, aortic debridement, bowel resection, and omental wrapping of the prosthesis on postoperative day 7.
Other complications. Multiple organ failure (MOF) developed in 3 patients; in one of them, there was persistent sepsis postoperatively. In 1 patient, the right renal artery was deliberately covered.
Mortality. Thirty-day and in-hospital mortality were both 8.5% (5/59). Combined 30- day/in-hospital mortality was 10.2% (6/59). Causes of death were ongoing (1 perioperative) or recurrent (3 postoperative) bleeding and MOF in 2 patients. There was no association between mortality and sepsis (preoperative or postoperative).
Antibiotic usage. Antibiotics were used in 50 patients who survived the operation. These were given on a short-term (n=8), long-term (>45 days, n=8), or lifelong (n=32) basis; in 2 patients, the duration of antibiotic usage was not reported. Antibiotic type given on the first postoperative day and later during the follow-up period was reported in 44% and 59%, respectively; often these were referred to as being broad spectrum. Mean number (range) of antibiotics given initially was reduced from 1.7 (1–5) to 1.4 (1–2), respectively. Lifelong antibiotics were prescribed in 5 (83%) of the 6 patients presenting with sepsis compared to 15 (41%) of the 37 patients without sepsis (p=0.08, Fisher exact test; where the individual patients with sepsis and antibiotic usage were identified).
Follow-up
AEF recurrence. Ten (19%) of the 53 patients who were discharged alive developed recurrent bleeding at a median 5.6 months (2.9–12) postoperatively, 4 of them with concurrent sepsis. In 7 of these 10 patients, recurrence was managed with graft and/or endograft removal, fistula closure, and revascularization with axillofemoral bypass grafting in 4 (additional staged renal and mesenteric revascularization in 1, co-current sepsis in 2); in situ reconstruction with an antibioticsoaked prosthesis in 2 with co-current sepsis; or closure of the aortic defect using a patch in 1. Two patients with no co-existing sepsis were managed with embolization and placement of a new endoprosthesis, respectively, while in 1 patient, the graft limb was sutured and the jejunum closed. The latter patient developed graft infection a month later, necessitating graft removal, placement of a homograft, and bilateral renal bypass grafting. Median follow-up for patients who did not develop recurrent bleeding was 10.3 months (5.5–20.5). The recurrence-free rate at 12 and 24 months was 71.5%, which included also early postoperative bleeding (Fig. 1).
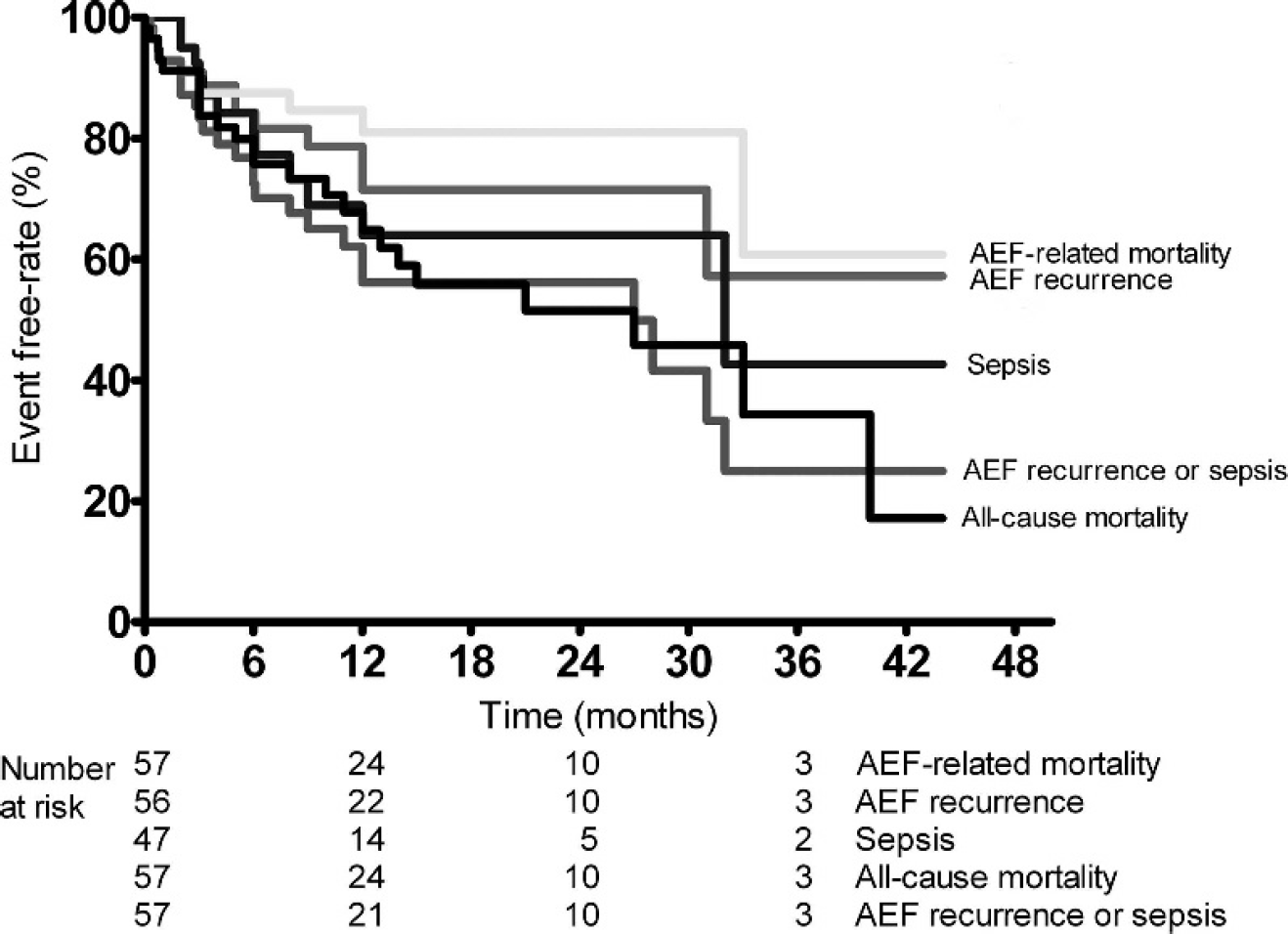
Summary of all major events that occur during follow-up after endovascular management of AEFs, including recurrence, sepsis, combined recurrence and sepsis, AEF-related death, and overall survival. The number of patients at risk at each interval is at the bottom.
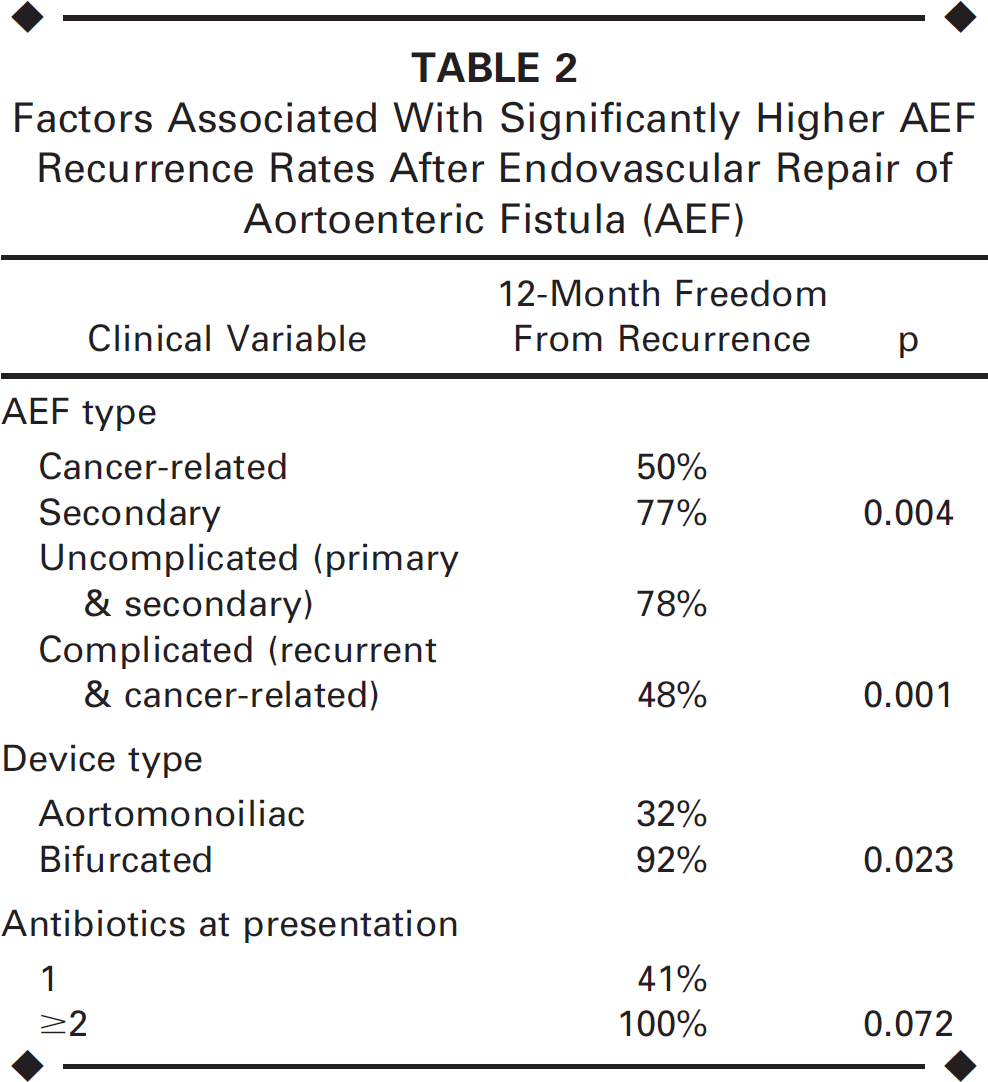
Table 2 shows factors associated with significantly higher AEF recurrence rates. Patients with complicated, cancer-related, and recurrent AEFs demonstrated a higher recurrence rate compared to the common AEF types (Fig. 2). The remaining baseline patient characteristics had no association with AEF recurrence.
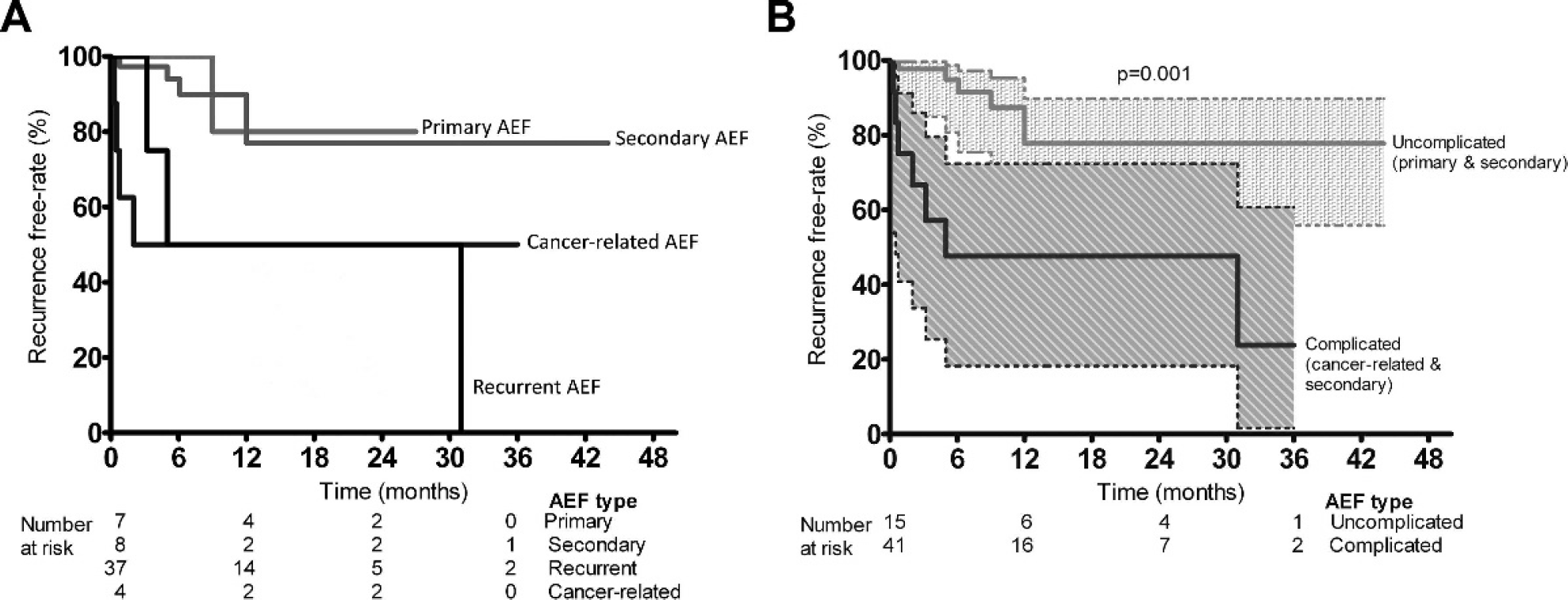
(
Factors Associated With Significantly Higher AEF Recurrence Rates After Endovascular Repair of Aortoenteric Fistula (AEF)
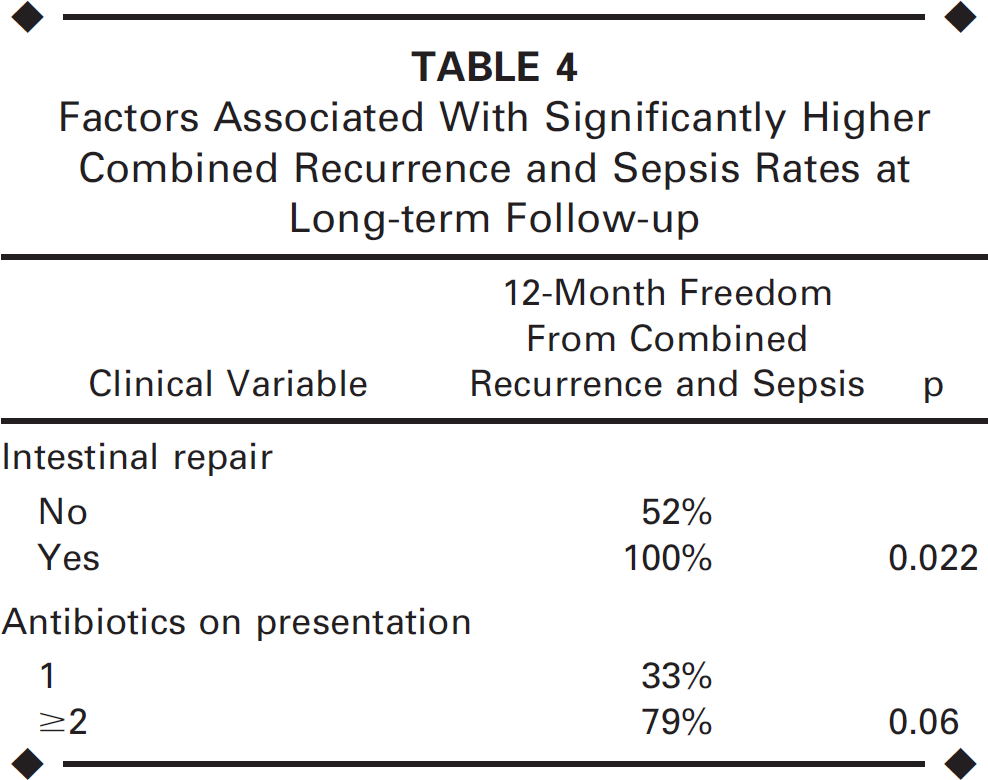
Sepsis. In addition to the 7 patients with perioperative sepsis, 17 (32%) of 53 patients discharged from the hospital developed sepsis at a median of 4 months (2.4–8.5) postoperatively. Although it often recurred, sepsis was managed conservatively in 8 of these patients, successfully in all but 1 patient who developed recurrent bleeding 3 months later. Five patients developed sepsis in association with AEF recurrence, as described above. In 3 of the remaining 4 patients, sepsis was managed with graft removal, fistula closure, and revascularization with axillofemoral bypass grafting in 2 or in situ reconstruction with an antibiotic-soaked prosthesis in the other. The fourth patient, who had an aortomonoiliac device and a femorofemoral bypass to treat a secondary AEF, developed groin sepsis that was managed with drainage and administration of antibiotics. Median follow-up for patients who did not develop sepsis was 8 months (4.5–18.0). The freedom from sepsis at 12 and 24 months was 64% (Fig. 1). Table 3 shows factors associated with significantly higher sepsis rates at long-term follow-up. Freedom from combined recurrence and sepsis at 12 and 24 months was 59% (Fig. 1). Table 4 shows factors associated with significantly greater freedom from combined recurrence and sepsis. Patients who did not have intestinal repair had a higher rate of combined recurrence and sepsis compared to AEF patients who did; freedom from combined recurrence and sepsis at 12 months was 52% in patients without intestinal repair versus 100% in those who had the repair (p=0.022, Fig. 3).
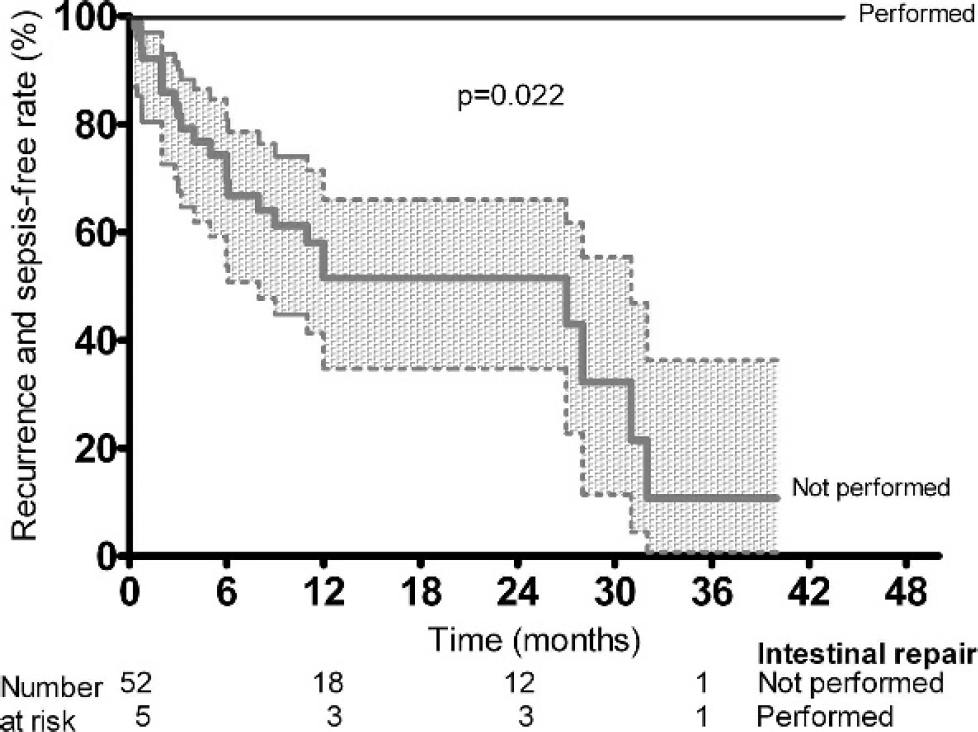
Kaplan-Meier curves with 95% CI (dashed lines) demonstrating combined AEF recurrence and sepsis rates in relation to intestinal repair. Patients who did not have intestinal repair had a higher rate of combined recurrence and sepsis compared to AEF patients who did. The combined recurrence and sepsis-free rates at 12 months were 52% and 100%, respectively (p=0.022).
Factors Associated With Significantly Higher Sepsis Rates at Long-term Follow-up
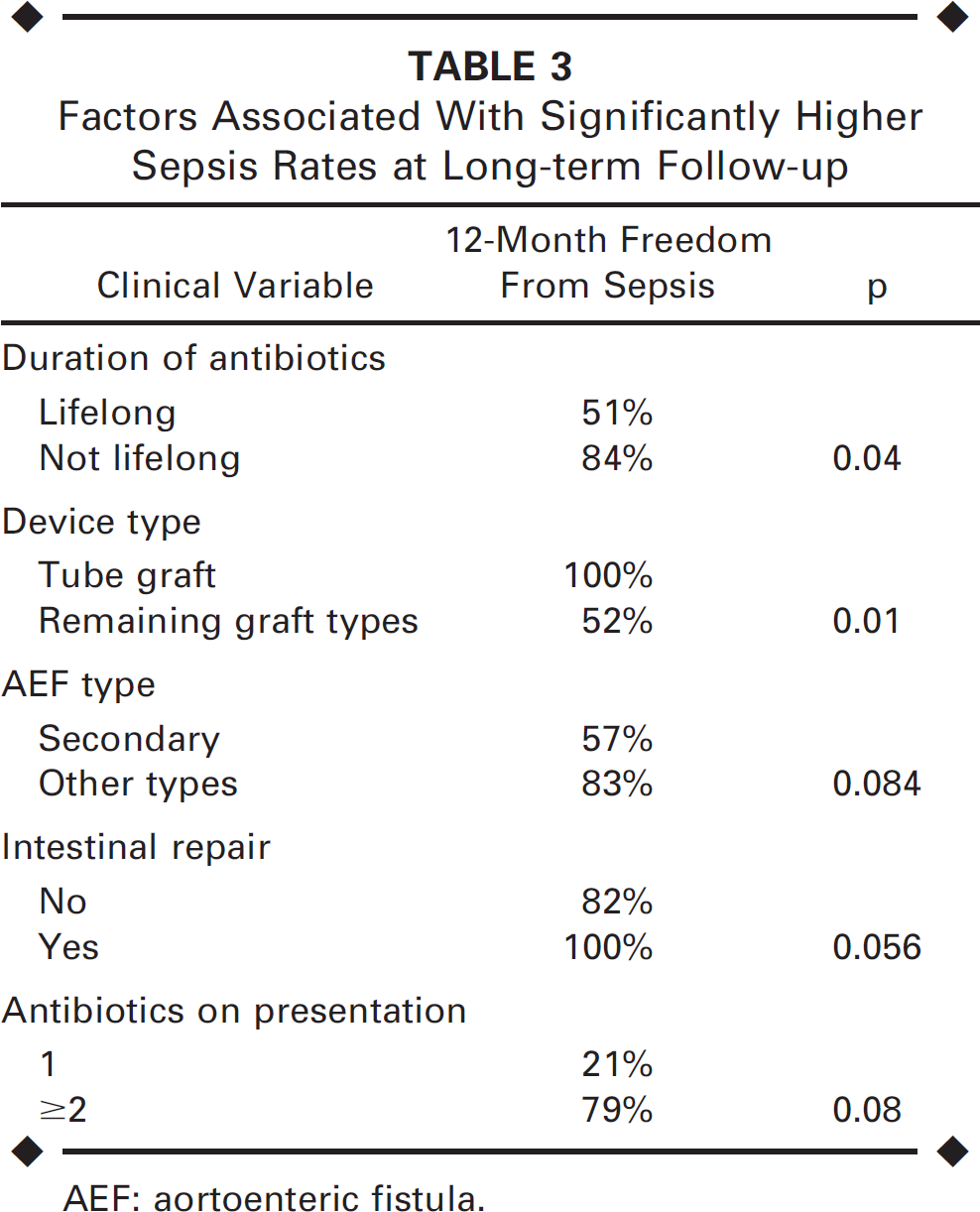
AEF: aortoenteric fistula.
Factors Associated With Significantly Higher Combined Recurrence and Sepsis Rates at Long-term Follow-up
Mortality. Late disease-related mortality was 7.5% (4/53). Causes of death were all complications of surgical management for late AEF sequelae, occurring during the early (n=3) or late (aortic stump blow-out, n = 1) postoperative period of the last open procedure. Total disease-related mortality was 17% (10/59). Total AEF-related mortality rates at 12 and 24 months were 15% and 19% (Fig. 1). Patients who succumbed after AEF repair were not significantly older (median age 73 years) compared to survivors (median age 70 years, p=0.61). AEF recurrence was the single factor associated with worse total AEF-related mortality (Table 5), with 51% survival at 2 years compared to 93% for patients with no recurrence (p=0.001, Fig. 4). Other marginally significant factors are also shown in Table 5.
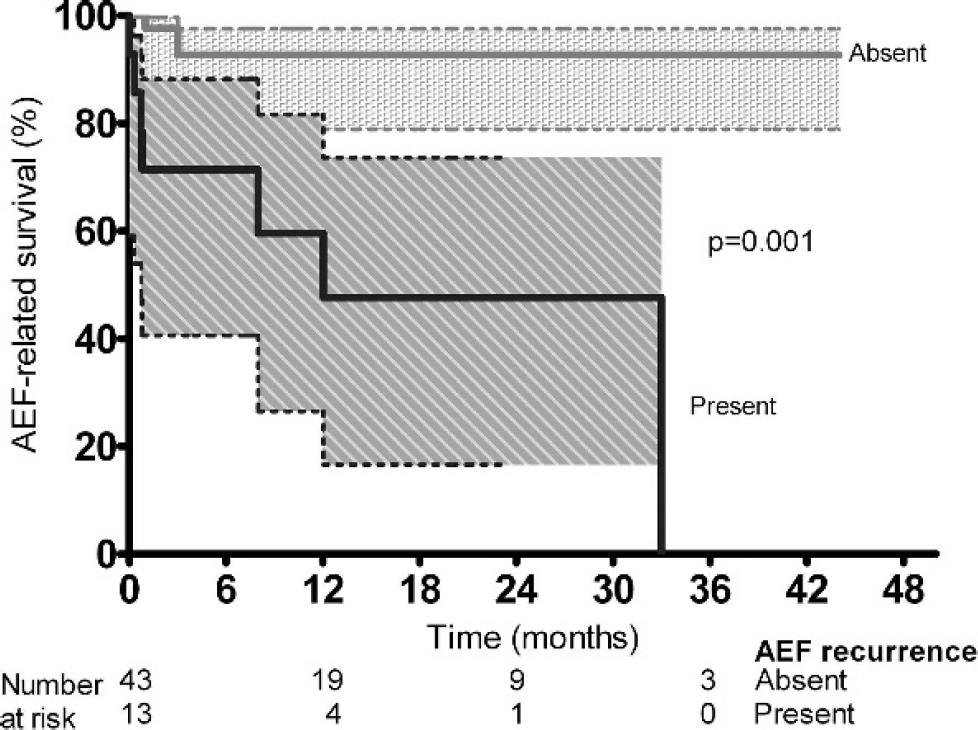
Kaplan-Meier curves with 95% CI (dashed lines) demonstrating that AEF recurrence was the single factor associated with worse total AEF-related mortality, with survival at 2 years just 51% compared to 93% for patients with no recurrence (p=0.001).
Factors Associated With Significantly Higher AEF-Related Mortality
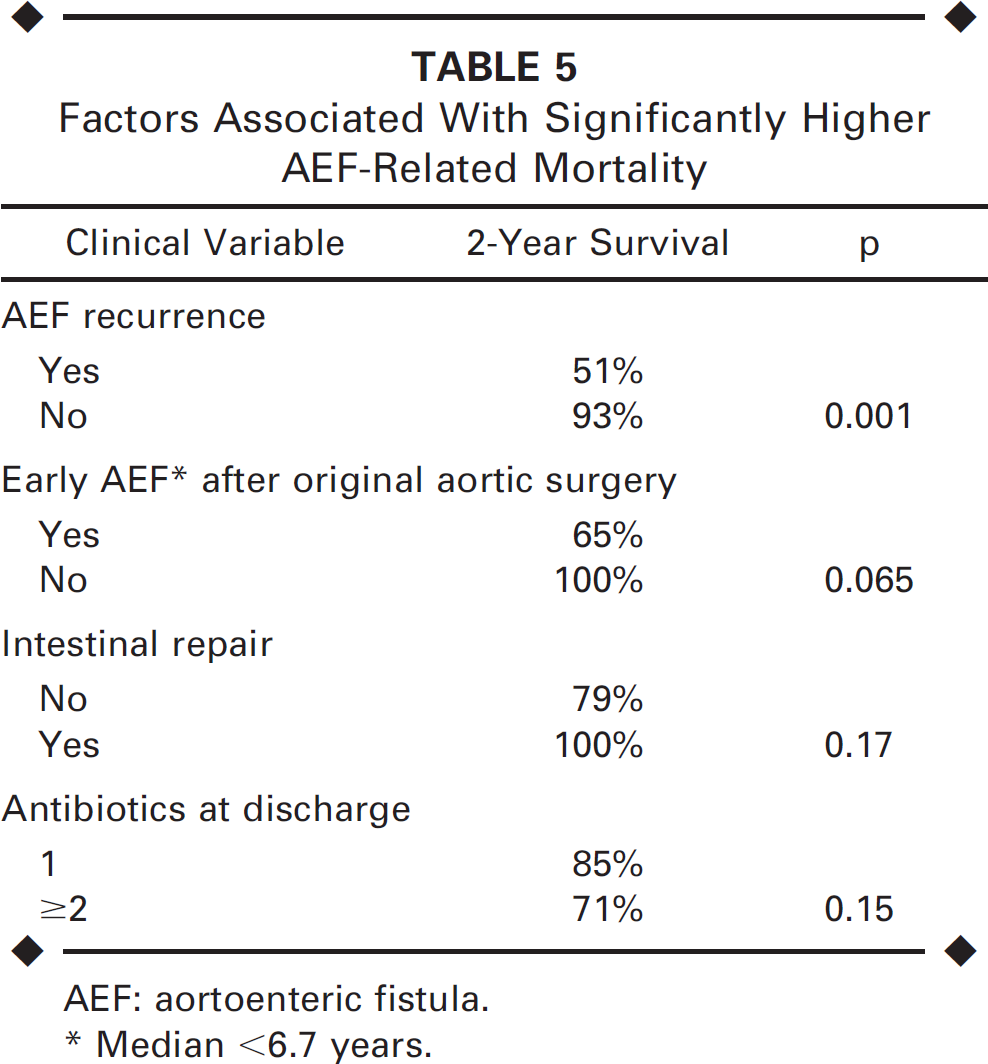
AEF: aortoenteric fistula.
Median <6.7 years.
During follow-up, 16 additional patients died due to myocardial infarction (n=6), cancer (n=6), stroke (n = 1), pulmonary embolism (n = 1), trauma complications (n = 1), and undetermined causes (n = 1, possibly due to cancer). Therefore, total all-cause mortality was 44% (26/59). Patients who died late after AEF repair were older (median age 73 years) compared to those who survived to the last follow-up (median age 67.5 years, p=0.057). Survival rates at 12 and 24 months were 68% and 52% (Fig. 1). Perioperative sepsis, among other factors (Table 6), was associated with worse all-cause mortality (Fig. 5). On multivariate analysis that included publication type, study period, age, gender, cause of AEF (secondary versus other types), intestinal repair, perioperative sepsis, late sepsis, and AEF recurrence, only perioperative sepsis and AEF recurrence were significantly associated with worse outcome [4.7 RR, 95% CI 1.7 to 12.7, (p=0.002) and 3.5 RR, 95% CI 1.4 to 8.6 (p=0.006), respectively].
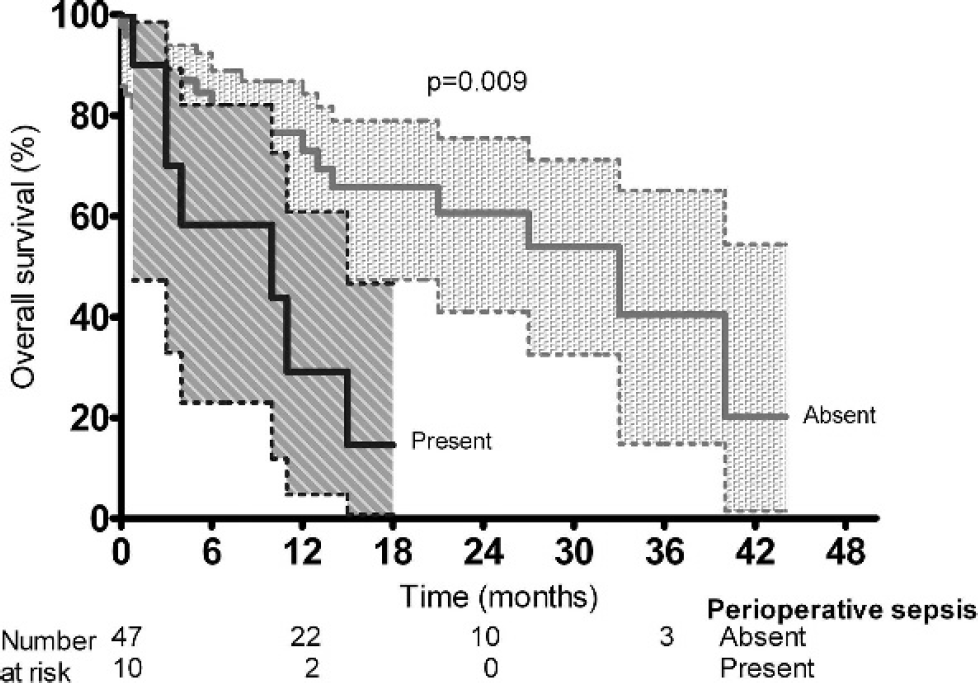
Kaplan-Meier curves with 95% CI (dashed lines) demonstrating that overall survival was worse at 2 years in patients with perioperative sepsis (15% at 18 months) compared to those who did not have sepsis (66%, p=0.009).
Factors Associated With Significantly Higher All-Cause Mortality
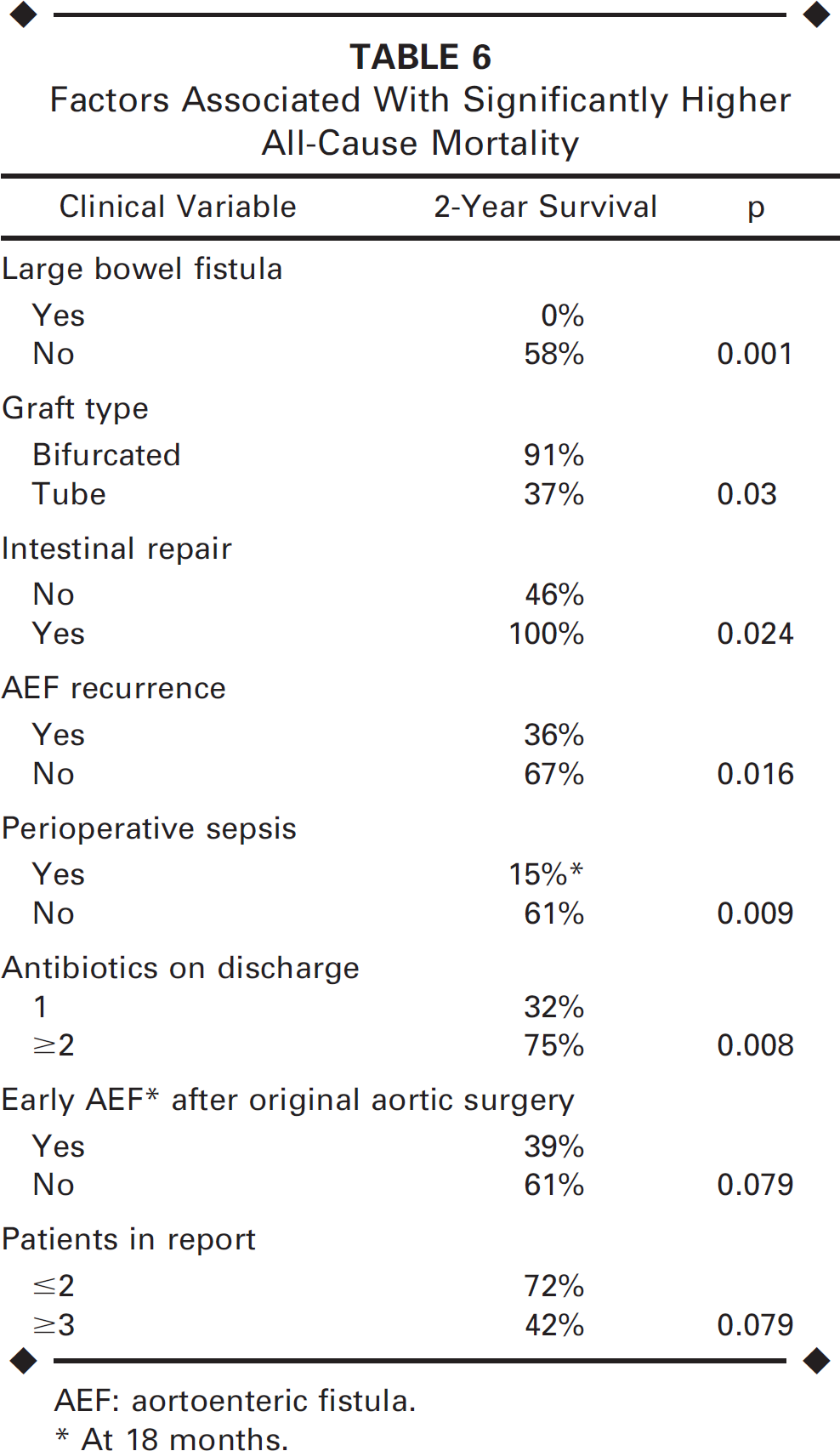
AEF: aortoenteric fistula.
At 18 months.
DISCUSSION
Our meta-analysis showed that endovascular management of AEF can accomplish acceptable short and midterm survival. Although plagued by a high rate of recurrent bleeding and sepsis, the overall results are better than those reported for open surgery.
Sepsis, an important determinant of patient outcome, 31 was present preoperatively in 17% of all cases, significantly lower than the 26% to 36% range reported by large metaanalyses of patients managed operatively.1,32 In 7% of all patients in the current meta-analysis, an abscess was drained, either percutaneously in 3 cases (large perigraft collection in a patient with persistent sepsis, psoas abscess associated with raised inflammatory markers, and aneurysm sac demonstrating air and fluid on imaging)3,18,28 or with an open procedure (retroperitoneal abscess in a patient with an aortosigmoid fistula necessitating also a diverting ileostomy completed with a Hartmann procedure). 18 Patients in a meta-analysis of open management 1 were on average 5 years younger than our patients. Similarly, the median interval from the original surgery was longer in the endovascular series, 6.7 years, compared to the 2 to 5 years in open series.1,32 This implies a process of patient selection in the open series, which could be the result of selecting patients fit for surgery.33,34
Endovascular management of AEF was successful in short-term sealing of the aorta in 93%. Although it failed in 4 patients, the procedure was a bridge to open surgery in only one of these 4 patients with early recurrent bleeding. Combined 30-day/in-hospital mortality (due to bleeding or MOF) was only 10% compared with the 52% mortality rate of open management. 1 The minimally invasive nature of endovascular repair, associated with less reperfusion injury, in compromised elderly patients with bleeding, often in shock and sepsis, is probably one of the reasons for the reduced mortality. Prolonged cross clamping is not well tolerated, and patients fare better (mortality 26%) if leg revascularization is performed prior to fistula management than vice versa (mortality 48%). 1
Antibiotics are an important part of adjunctive treatment, since most patients received them on a lifelong basis, presumably because it was thought that the presence of a foreign body would prevent infection eradication. Interestingly, lifelong antibiotics were prescribed more often in patients presenting with sepsis compared to those without, which could be the reason their use was associated with worse prognosis.
Poor Prognostic Factors Associated With Complications and Mortality Following Endovascular Repair of Aortoenteric Fistula (AEF)
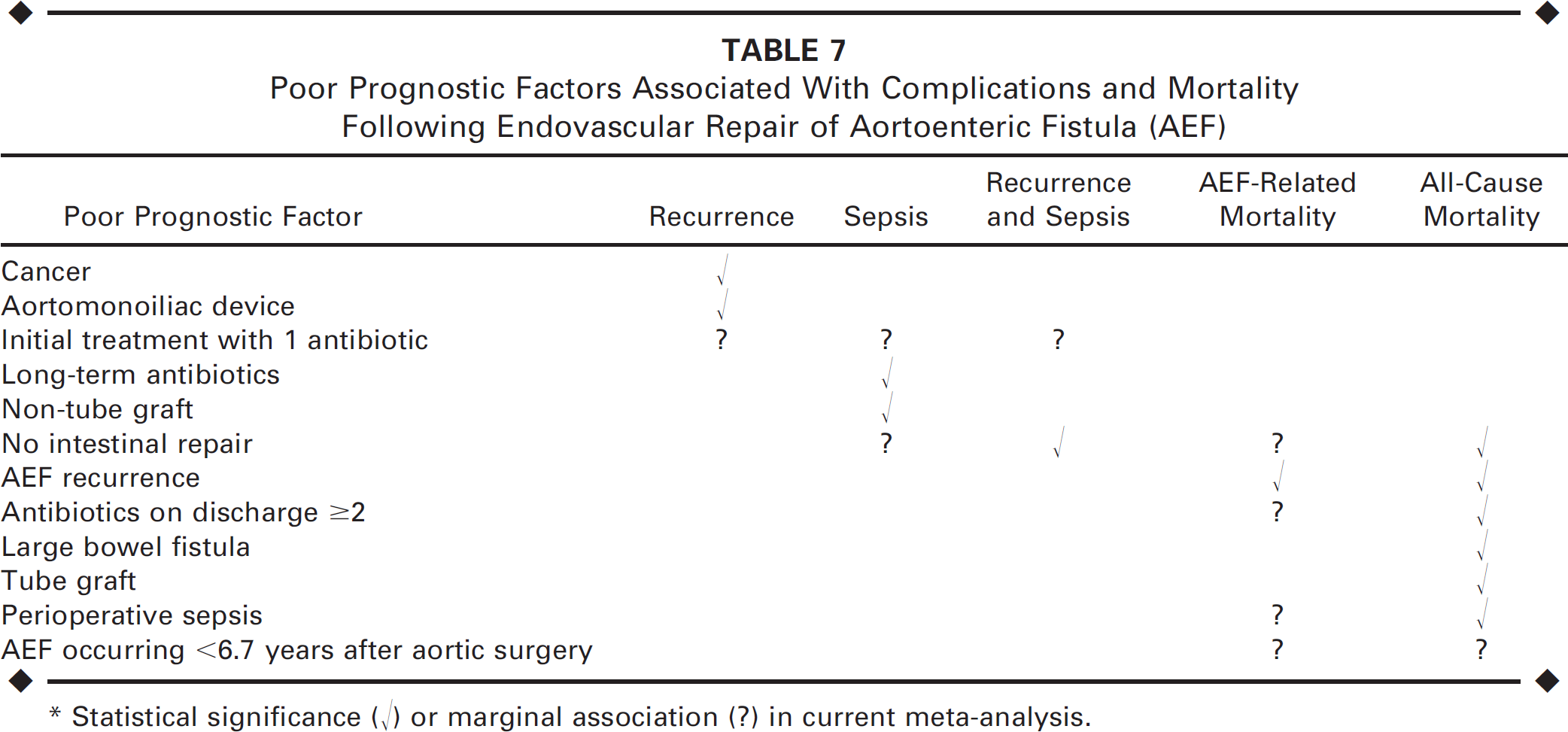
Statistical significance (√) or marginal association (?) in current meta-analysis.
Recurrent bleeding, which developed in a fifth of the patients who survived hospitalization, was mainly managed surgically. Cancer was associated with a higher risk of recurrence, perhaps because tumors can advance and cause instability of the endograft or because the site of fistulization was more often the large bowel. Recurrent AEFs followed a similar pattern, with recurrence being more common, perhaps the result of untreated infection. Similarly, patients who had an aortomonoiliac device placed had a higher rate of recurrence compared to those who received a bifurcated device. The exact reason remains unclear, but it is most likely related to the formation of a short, incomplete sealing zone or no sealing in cases of AEFs involving the distal anastomosis; for this reason, some surgeons routinely use bifurcated endografts to manage AEFs. 27
We showed that patients with secondary AEFs had a higher rate of sepsis compared to patients with AEFs due to other causes. This worse outcome could be due to the presence of graft material in secondary fistulas, which is not removed with endovascular management. Patients who did not have intestinal repair had a higher rate of sepsis than patients who did, which is expected since ongoing contamination can prevent sterilization of the graft and/or endograft. Patients who initially received one antibiotic had a higher rate of sepsis compared to those who received ≥2, which indicates that broader spectrum antibiotics are more effective in local infection control.
Since sepsis and AEF recurrence can be associated, we calculated the freedom from combined recurrence and sepsis; outcome was better in patients who had intestinal repair or received ≥2 antibiotics as initial treatment, which indicates the important role of treating the source of contamination. Interestingly, intestinal repair was not performed to manage sepsis per se; instead, this procedure was performed in conjunction with direct repair of the aortic defect to achieve hemodynamic stability in 3 of 6 cases,4,19,26 while an additional patient had glue injected into the fistula tract. 12
Also there was no association of intestinal repair with preoperative variables, apart from a marginal association with cancer (p=0.04) and placement of tube grafts (p=0.04). More investigation into the role of fistula management, preferably once the patient is stabilized, is warranted. This repair could be justified in high-risk patients who can tolerate an upper gastrointestinal procedure but not major open surgery.
Half of the total disease-related mortality in our analysis was related to late complications, exclusively to surgery or, most likely, disease severity necessitating surgery. AEF-related mortality actuarial rates at 12 and 24 months were 15% and 19%, respectively. Although longer follow-up results are necessary, these rates compare favorably to those achieved with traditional surgery. 1 In contrast, the all-cause mortality of 44% sounds high and, similarly, the actuarial survival rates of 68% and 52% at 12 and 24 months, respectively, relatively low; this high mortality is probably indicative of a group of older, compromised patients. Perioperative sepsis was associated with worse survival in our meta-analysis; similar results have been reported by others in aortoenteric and aortoesophageal fistulas. 31 For the sake of homogeneity, the latter were not included in our review.
A distinctive pattern of endovascular management of AEFs is the frequent use of straight stent-grafts (in the form of tube or aortomonoiliac grafts or extender cuffs). This may be due to the favorable anatomy resulting from the previous open aneurysm repair, which provides a long and uniform distal landing zone for deployment of a tube graft or extender cuffs. It may also be indicative of patient instability, which would necessitate using an aortomonoiliac graft. Additionally, the size of most aortic grafts fits the size of the commercially available endografts. We could not determine the optimum graft type to be used for AEF repair. Aortomonoiliac devices were associated with a higher AEF recurrence rate, perhaps because these cannot establish a long sealing zone. Tube grafts outperformed their non-tube counterparts in preventing sepsis, perhaps because they establish a better sealing zone.
An additional distinctive pattern of endovascular management for AEF is the use of adjuvant procedures, performed often for the management of sepsis or the fistula itself. Obviously, sepsis in the presence of an aortic graft predicts worse outcome, 31 and it is not surprising that attempts to address it were made by abscess drainage or intestine repair. This is known to be the rationale for open surgery, with sepsis and need to perform a complex duodenum repair being predictors of poor outcome.35,36
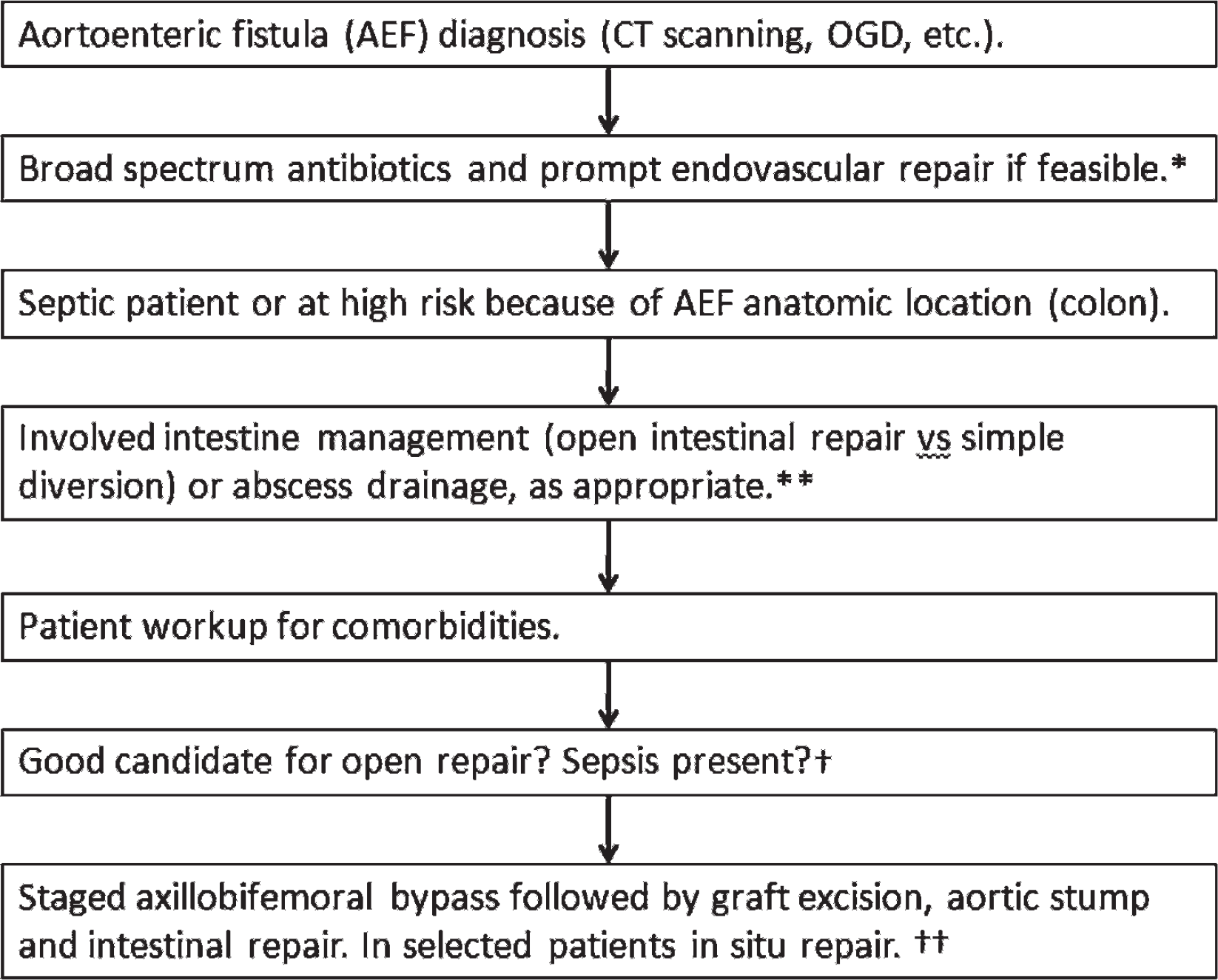
The small number of patients with AEF seen in each center would make it very difficult to recruit patients for a randomized study comparing open with endovascular management. Until then, valuable information can be obtained from meta-analyses or multicenter series, 1 the latter being necessary to avoid publication bias by reporting only positive outcomes of single case reports, an inherent problem of our study, too. Because of the high risk for recurrence, this approach has been suggested as a bridge to open surgery 4 ; however, some patients with comorbidities cannot undergo open surgery even after they are stabilized with endovascular management. Also, the timing of open surgery in this case can be difficult to determine when a satisfactory steady state with conservative treatment has been achieved. 34 Similarly, in patients who present with sepsis and have comorbidities (contraindications for immediate open repair), endovascular management is a one-way ticket. Many patients may heal their AEFs with endovascular repair coupled with antibiotic therapy, mostly those with secondary infrarenal AEFs who present without evidence of sepsis. 18 Patients with AEFs involving the colon who undergo endovascular repair should have additional procedures, such as open intestinal repair or simple diversion, in most cases to decrease the risk of persistent sepsis. 18 Similarly, patients with a co-existing abscess should have percutaneous or open drainage. Finally, for patients who may be medically optimized, endovascular repair may serve as a bridging therapy to open repair,4,37 particularly in patients with perioperative sepsis. 31 A summary of our recommendations is illustrated in Figure 6.
Limitations
Study limitations included a lack of a control surgical group and the fact that the AEFs analyzed were not consecutive patients; it is therefore possible that some publication bias does exist in the sense that bad results of AEF repair might not have been published, so the overall results of the published cases look better than what they should be. Nevertheless, in our meta-analysis, there was no difference in presentation and outcome between reports of 1 to 2 cases and case series reporting ≥3 cases.
Conclusion
Endovascular management of AEF can achieve satisfactory short-term results, better than those reported for open surgery. There is, however, a high rate of recurrent bleeding and sepsis. Future research toward fistula management as an adjuvant procedure is warranted. Longer follow-up to determine the durability of endovascular management of AEFs is warranted.